
Abstract
Study Design
Systematic review and meta-analysis.
Objectives
Perioperative interventions in Enhanced recovery after surgery (ERAS) protocols for managing adult spinal deformity (ASD) patients vary widely across institutions without widespread standardization. This study aims to evaluate the various interventions performed in ERAS protocols and the impact of these protocols on postoperative outcomes following ASD surgery.
Methods
A comprehensive systematic review was conducted following PRISMA guidelines. Studies that addressed the implementation of ERAS protocol for thoraco-lumbar corrective surgery were included. We conducted a meta-analysis on postoperative outcomes, where possible, calculating the pooled standardized mean difference between conventional care (pre-ERAS) and ERAS pathways (post-ERAS).
Results
Out of 63 articles, 8 were included in the systematic review. Common interventions in the ERAS protocols included: (1) preoperative anesthesia-related risk assessment and multidisciplinary assessment, (2) intraoperative tranexamic acid (TXA) administration and continuous monitoring of lab data, and (3) postoperative early mobilization and early nutritional support. Multimodal analgesia plans were commonly observed in many of the ERAS protocols. Although meta-analysis demonstrated no significant difference in length of stay (LOS) between the groups, the post-ERAS group generally tended to exhibit lower rates of readmission and medical complications, and reductions in total opioid consumption.
Conclusions
The goals of ERAS protocols for ASD surgery often address preoperative optimization, intraoperative stress minimization, and postoperative recovery facilitation. While the implementation of the ERAS protocol has shown improvements in postoperative outcomes, further studies are required to standardize the ERAS protocol for ASD surgery and enhance the impact on multiple postoperative outcomes.
Keywords
Introduction
Adult spinal deformity (ASD) is one of the most challenging spinal disorders, encompassing a heterogeneous group of spinal diseases that present in adulthood including adult scoliosis, degenerative scoliosis, sagittal and coronal imbalance, and iatrogenic deformity. 1 With an expanding aging population, the global prevalence of ASD has been reported to range from 30% to 68% in the elderly population. 2 Although there has been significant improvement observed in surgical techniques and diagnostic tools to address ASD, this patient population places an increasing burden on healthcare systems due to more frequent surgical interventions and ASD-specific challenges such as prolonged recovery times, high complication rates, and perioperative pain management. Thus, it is essential to establish protocols that improve patient care without creating additional financial burden on healthcare systems. 3
Enhanced recovery after surgery (ERAS) protocols are a set of interventions which are carried out in the perioperative period to improve patient outcomes and to accelerate recovery from surgery. 4 The concepts of ERAS were first defined 30 years ago in colorectal surgery with multiple surgical specialties quickly adopting the principles of ERAS shortly thereafter. 5 Since complex spinal reconstruction procedures for ASD are associated with the risk of surgical complications and frequency of readmissions, a comprehensive perioperative care is required. Early standardized, multidisciplinary approaches to complex spine surgery, such as the Seattle Spine Team Protocol, demonstrated reduced perioperative complications in complex spinal deformity procedures through a systematic multidisciplinary risk-factor optimization program. 6 Subsequent studies have confirmed that ERAS protocols can be beneficial in managing patients who have undergone ASD surgery by reducing length of stay (LOS).7-9 However, the evidence of the impact of ERAS protocols on postoperative outcomes in patients with ASD has not yet been obtained.
The primary aim of this study is to perform a systematic review of ERAS protocols designed for ASD surgical episodes of care, and to evaluate the impact of these protocols on postoperative outcomes. Although systematic reviews on ERAS within spine surgery have been conducted, they have focused on the broad spectrum of spine pathology and interventions. However, no systematic reviews have focused directly on patients undergoing surgical intervention for ASD, arguably the most complicated patient population and perioperative management amongst spinal patients. Given the distinctive characteristics of ASD surgeries, which involve increased complexity, extended duration, and prolonged recovery and hospitalization periods, the applicability of conclusions drawn from case series’ is challenging. Therefore, a systematic review and meta-analysis are critical to improve care models for ASD patients undergoing spinal reconstruction procedures.
Methods
Search Strategy
A comprehensive systematic review was conducted in accordance with the standard recommendations of the Primary Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.10,11 We reviewed the literature in January 2025 using 2 electronic databases, PubMed and Embase. The following keywords were used: (1) Search terms for ERAS: “ERAS,” “enhanced recovery,” “enhanced recovery protocol,” “enhanced recovery pathway,” and “perioperative optimization.” (2) Search terms for ASD: “ASD,” “adult spine deformity,” “complex spine surgery,” and “complex spinal surgery.” Results were restricted to studies written in English and full text articles. An updated search was conducted before data analyses with the same screening and selection process as the initial search. Institutional Review Board approval and informed consent were not applicable due to the nature of systematic review of available research.
Selection Criteria and Study Collection
In the current study, we included articles regarding implementation of ERAS protocols for adults with spine deformities that underwent thoraco-lumbar corrective surgery. Studies that include minimally invasive surgery (MIS), decompression-only procedures or cervical deformity were excluded. Reviews, case reports, abstracts for conferences, and editorial letters were also excluded. Using Covidence software, abstracts and full texts of retrieved studies were reviewed independently by 3 authors (RK, PL and TF) to identify studies that potentially met the inclusion criteria. When disagreements occurred regarding study eligibility, a final decision was made using a predefined decision rule to include only studies that compared groups treated with conventional care pathways vs ERAS pathways. Finally, a data extraction sheet was created, outlining the variables to be collected.
Meta-Analysis
We conducted a meta-analysis in postoperative outcomes, calculating the pooled standardized mean difference between the group treated with conventional care pathways (pre-ERAS) and treated with ERAS pathways (post-ERAS). This analysis was performed using R Studio 2023.06.1 Build 524 and the meta for package.
Risk of Bias and Quality of Evidence
The risk of bias of the included articles was evaluated independently by 2 authors (PL and TF) using the Risk of Bias In Nonrandomized Studies-of Exposure (ROBINS-E) tool. 12 A visualization tool (Robvis) was used to visualize the risk of bias assessment in this systematic review. 13 The ROBINS-E tool includes 7 domains of bias, including bias due to confounding, bias arising from measurement of the exposure, bias in selection of participants into the study, bias due to post-exposure interventions, bias due to missing data, bias arising from measurement of the outcome, and bias in selection of the reported result. In cases of discrepancies in risk of bias assessments among the reviewers, a consensus was decided between the 2 reviewers.
Results
Search and Selection
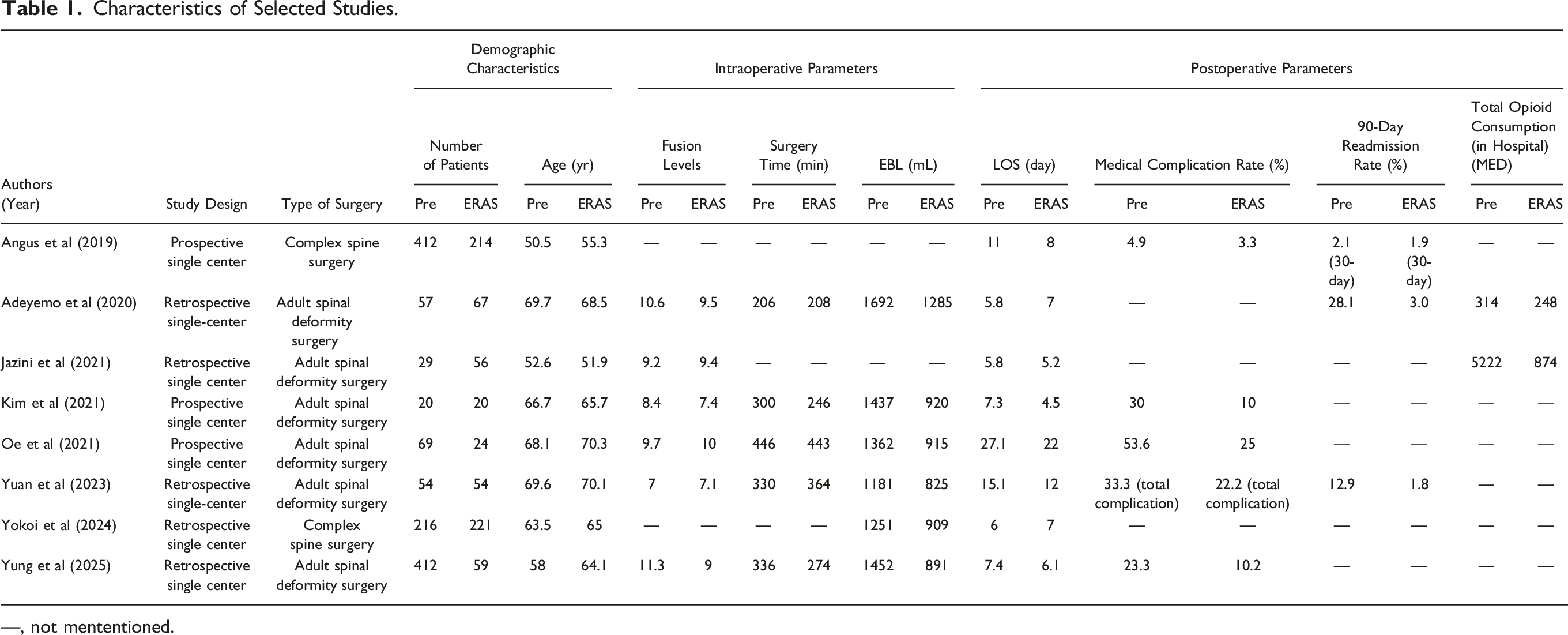
Our search identified 63 studies, with 33 from PubMed and 30 from Embase. Using Covidence software, we identified and removed 5 duplicate studies. Among the remaining studies, 37 were excluded for not being relevant to ERAS and spine surgery, 4 were excluded because they were abstracts, 5 did not measure proper outcomes, and 4 did not use a compatible study design. The final systematic review included 8 studies that ranged in publication date from 2019 to 2025, totaling 1984 patients (1269 Pre-ERAS and 715 Post-ERAS).7,8,14-19 The selection process was detailed in the PRISMA chart (Figure 1). Table 1 illustrated various study specific details, including: study design, surgical techniques/approaches, demographic characteristics, intraoperative factors, and postoperative outcomes in the included studies, comparing the pre-ERAS group and post-ERAS group. PRISMA chart for ERAS protocols in ASD. This chart outlines the study selection process for the systematic review and meta-analysis. It details the number of studies identified, screened, assessed for eligibility, and included in the final analysis, highlighting reasons for exclusions at each stage. Characteristics of Selected Studies. —, not mententioned.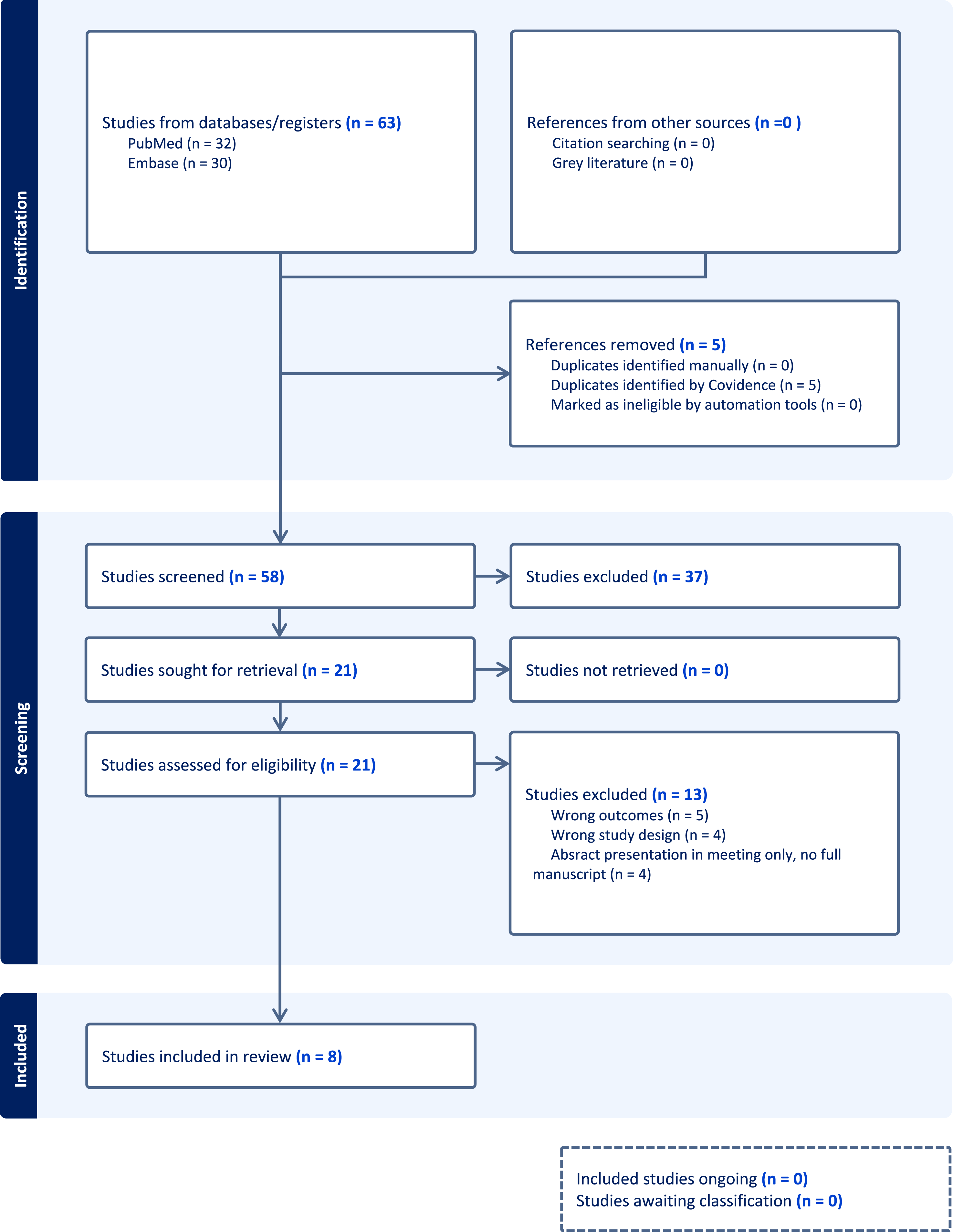
Interventions in ERAS Protocol
Interventions in ERAS Protocol.
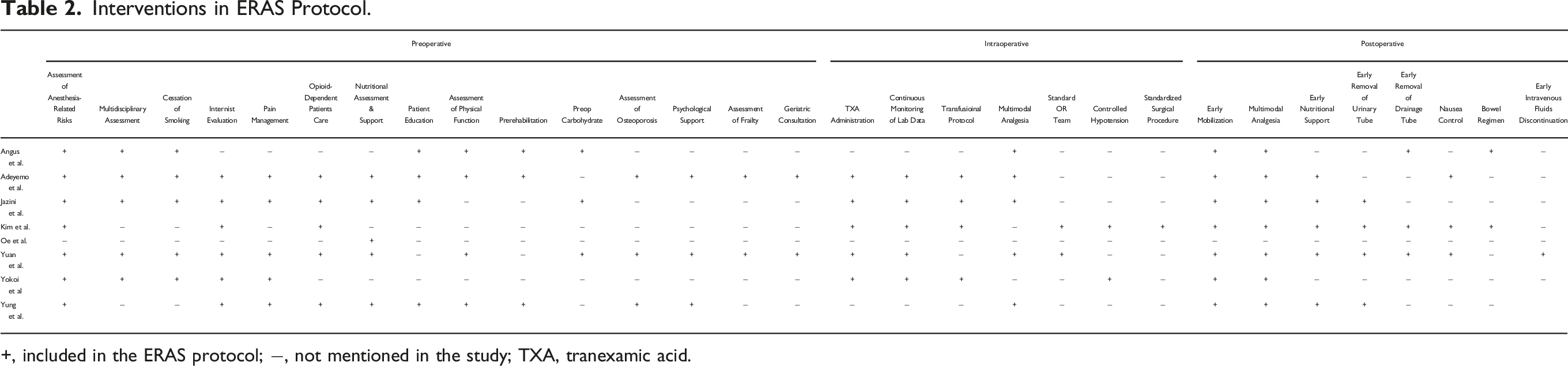
+, included in the ERAS protocol; −, not mentioned in the study; TXA, tranexamic acid.
Postoperative Outcomes
Out of 8 studies included in this systematic review, 5 studies reported medical complication rates, ranging from 4.9% to 70.6% for pre-ERAS group and from 3.3% to 50.8% for post-ERAS group.7,8,14,17,19 Although medical complication rates including deep venous thrombosis, pneumonia, and hematoma were comparable between the pre-ERAS and post-ERAS group in 3 studies (Angus et al; 4.9% (20/412 patients) vs 3.3% (7/214 patients), P = .25, Kim et al; 30% (6/20) vs 10% (2/20), P = .235, Yuan et al (total complication); 33.3% (18/54) vs 22.2% (12/54), P = .198),7,8,14 2 studies demonstrated significantly lower rate of medical complications, such as delirium and surgical site infection, in post-ERAS group (Oe et al; 53.6% (37/69 patients) vs 25% (6/24 patients) P = .015, Yung et al; 23.3% (96/412) vs 10.2% (6/59), P = .02).17,19
The 90-day readmission rate was evaluated in 3 studies,7,14,15 showing significant reduction in ERAS groups compared to pre-ERAS groups in 2 studies (Yuan et al; 12.9% (7/54 patients) vs 1.8% (1/54 patients), P = .027, Adeyemo et al; 28.1% (16/57) vs 3.0% (2/67), P = .0001). In the study of Adeyemo et al, a total of 16 patients were readmitted for the pre-ERAS group, and the reason for readmission for 15 of those patients was pain control. 15 A study from the United Kingdom (Angus et al) demonstrated that the 30-day readmissions have decreased from 2.1% to 1.9%, though this reduction was not statistically significant. 14
Two studies compared opioid consumption in the groups.15,16 Jazini E et al demonstrated that the implementation of ERAS was associated with a significant decrease in both in-hospital and 90-day global MMEs (P = .000 and P = .034) in multivariable regression analysis. 16 Similarly, Adeyemo et al showed that ERAS patients had a significantly lower rate of postoperative supplemental opioid consumption in hospital (248.05 vs 314.05 MED, P = .04). 15 Those studies indicated that the ERAS pathway independently reduced total opioid consumption while in the hospital.
Meta-Analysis of LOS
LOS measured in days was evaluated in all studies included in this study.7,8,14-19 We conducted a meta-analysis of the LOS, since the data on complication rate, readmission rate, and opioid consumption were insufficient for pooling data for meta-analysis. Out of the 8 included studies, 4 studies showed a significant reduction in LOS.7,8,14,19 Conversely, there was a significant increase in LOS in 2 studies.15,18 The overall result was a standardized mean difference of −.27, 95% CI (−.55, .01). Since the confidence interval included 0, the overall analysis indicated no significant difference in LOS between the pre-ERAS and post-ERAS groups, however, the observed difference was nearly significant. (Figure 2). Forest plot showing the meta-analysis for length of stay (days). This plot illustrates the standardized mean differences in LOS between pre-ERAS and post-ERAS groups across the included studies. Each study is represented by a square, with the size indicating the weight of the study in the meta-analysis, and a horizontal line representing the 95% confidence interval. The pooled estimate is shown as a diamond at the bottom, with a summary of the overall effect and confidence interval.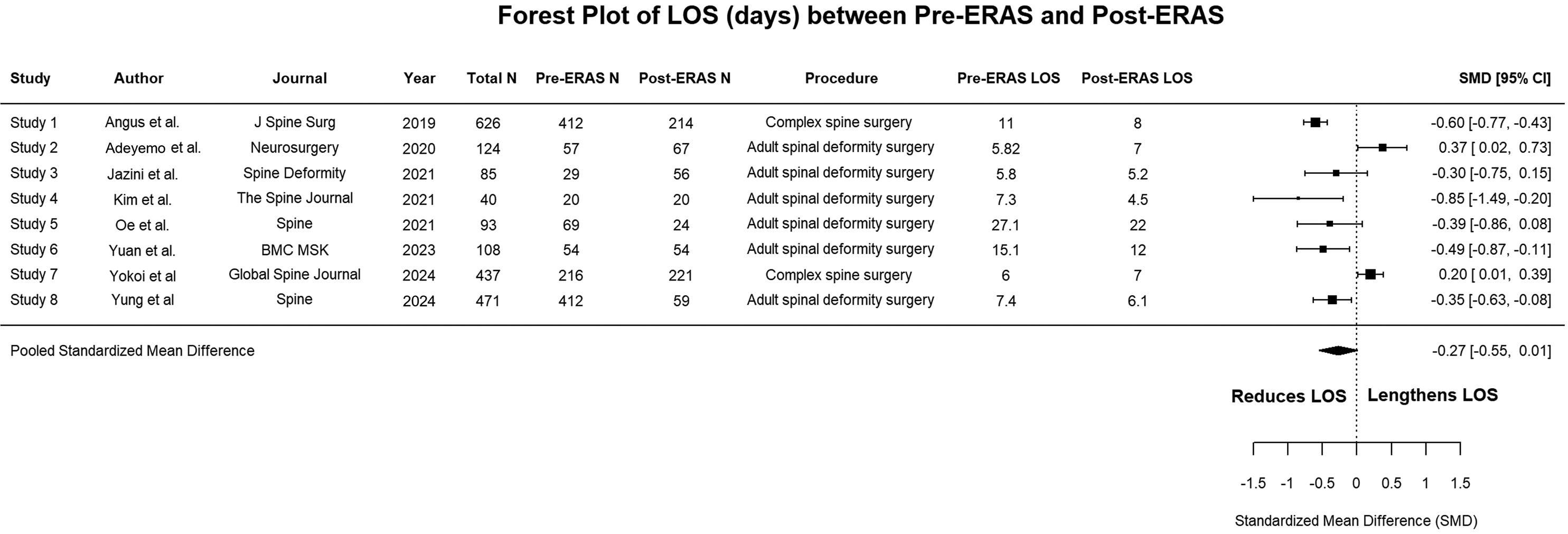
Risk of Bias Assessment
A risk of bias assessment was performed for each included study. (Figure 3) 4 of the 8 studies were judged to hold “some concerns,” while other 4 studies demonstrated high risk of bias. Since most of the studies were retrospective, their biases were primarily due to confounding factors. The overall risk of bias in the study set was some concerns or greater when considering all 7 domains together, likely influenced by the inclusion of nonrandomized studies. Risk of bias assessment using the ROBINS-E tool. The assessments of the risk of bias assessment for each of the included studies in this systematic review are broken down into 7 different domains to yield an overall risk of bias.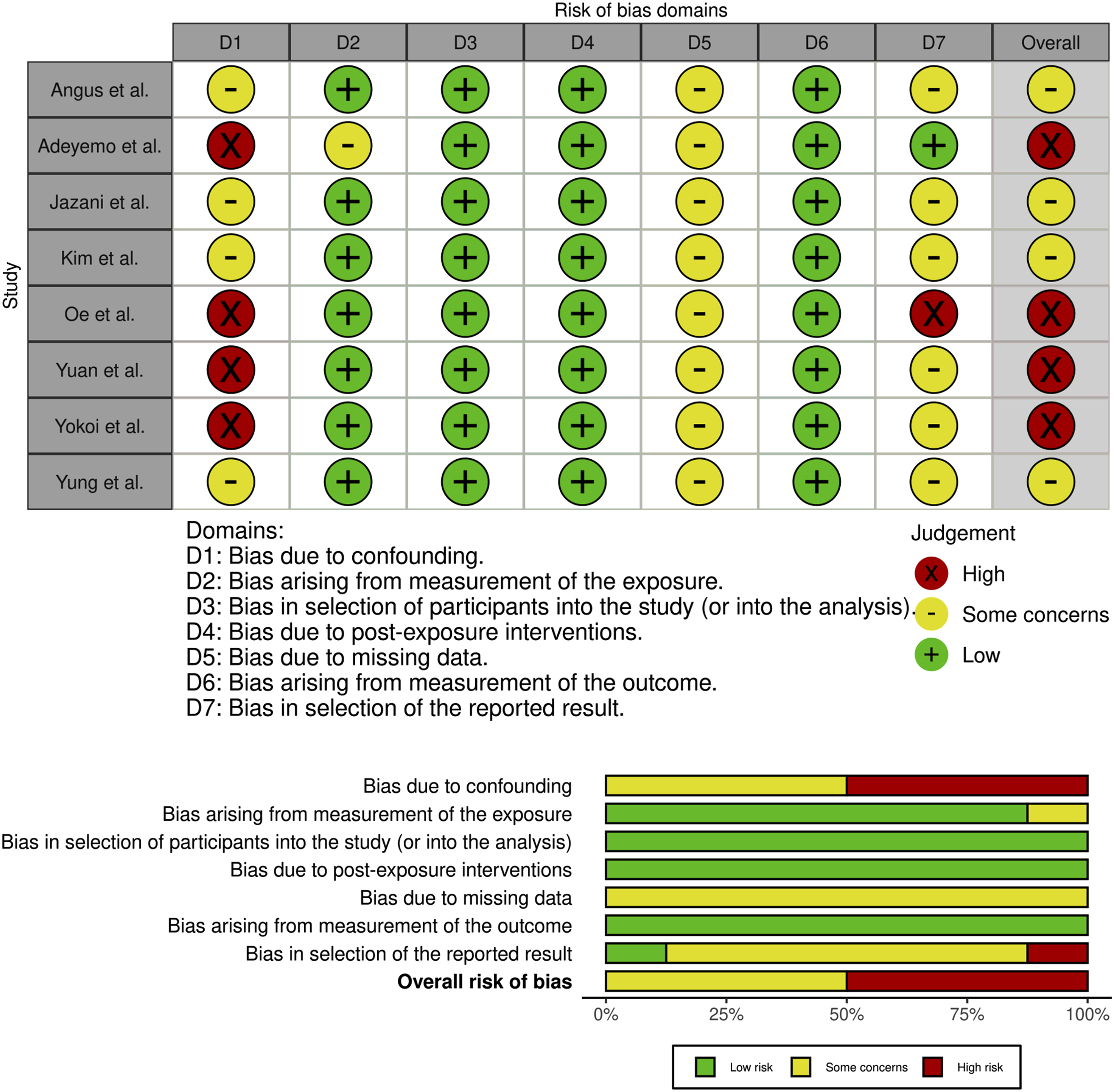
Discussion
Surgical management of ASD is associated with high rates of intraoperative and postoperative complications, with a substantial risk of operative mortality ranging from 1.0% to 3.5%.20,21 A comprehensive perioperative team approach, such as The Seattle Spine Team Protocol, has been reported, showing that multidisciplinary team care reduced perioperative complication rates and enhanced patient safety in patients undergoing complex spinal reconstructions for adult spinal deformity.
6
ERAS pathways for ASD surgery focus heavily on postoperative pain control, ambulation, and nutrition. However, the specific components of the protocols vary widely between studies. Thus, we conducted a systematic review and meta-analysis to evaluate the interventions within ERAS protocols and their impact on postoperative outcomes following ASD surgery. Nevertheless, the meta-analysis results showed no significant difference in LOS between the pre-ERAS and post-ERAS groups. The ERAS protocols for ASD surgery generally consisted of 3 main components: preoperative optimization, intraoperative stress minimization, and postoperative recovery facilitation. The overall interventions encompassed within ERAS protocols were demonstrated in Figure 4. Despite the spectrum of interventions, there were common components in the preoperative, intraoperative, and postoperative phases. Overall flow of the ERAS protocols for ASD surgery. ERAS protocols for ASD surgery consists of 3 main components: preoperative optimization, intraoperative stress minimization, and postoperative recovery facilitation. Components marked in gray are common interventions included in the studies.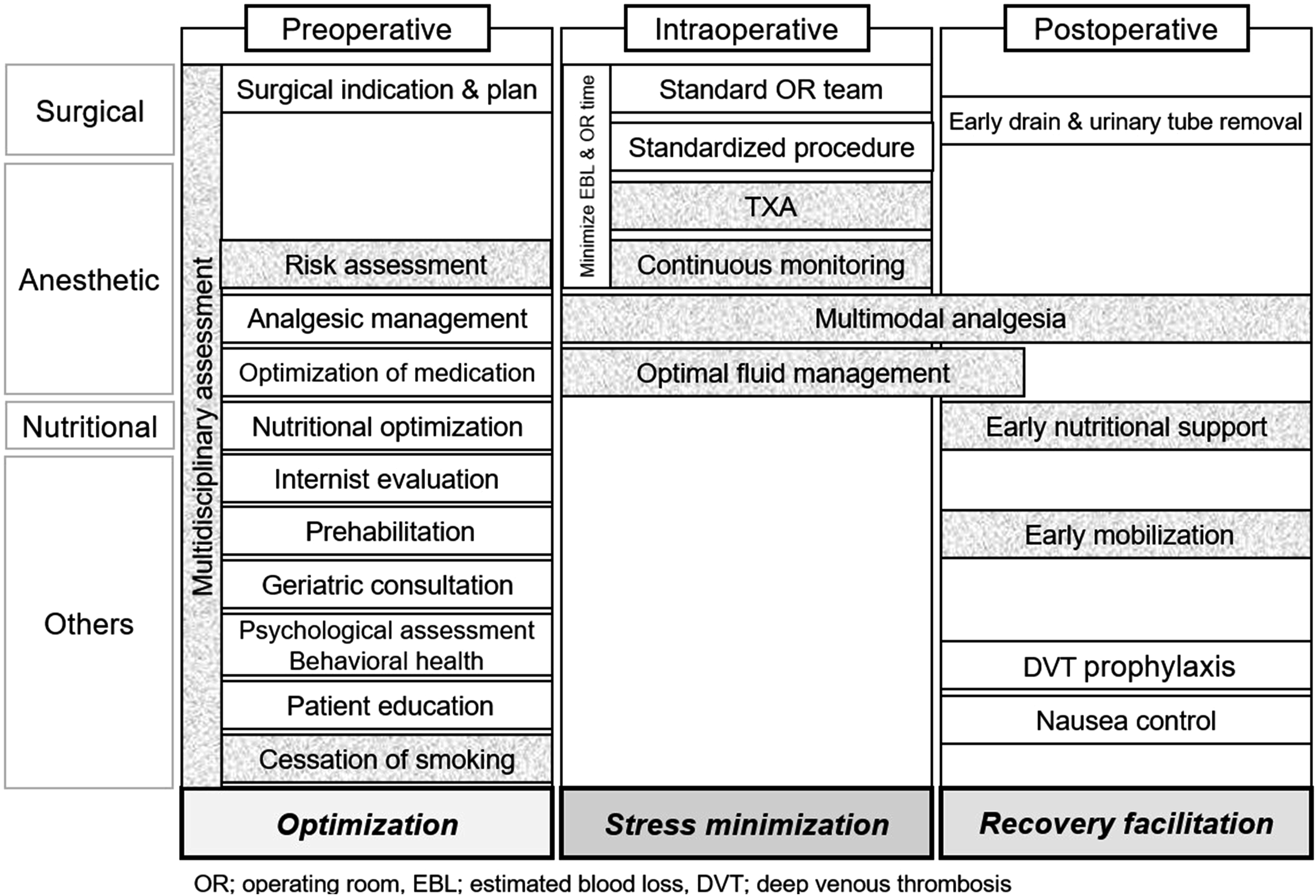
Preoperative components within the ERAS protocols included in this review often aimed to identify the risk factors for perioperative complications and to optimize the patient medical status to minimize complications associated with ASD surgery. Major interventions for patient optimization described in this review were (1) anesthesia-related risk assessment and (2) multidisciplinary assessment. These assessments provide an opportunity to select a surgical candidate and improve preoperative health status by optimizing potentially modifiable factors, such as frailty and diabetes. 22 Other varying interventions, such as cessation of smoking, internist evaluation, and assessment of nutrition, physical function, and mental health, have been incorporated into ERAS protocols to achieve this goal. Identification of risk factors for perioperative complications through the multidisciplinary team approach is a priority for empowering informed choices for patients and surgeons and managing patient expectations in ASD surgery. 23 Multidisciplinary team care is crucial for optimizing spinal deformity patients in the preoperative period within ERAS protocols, as research has demonstrated that it enhances quality of care by improving outcomes, reducing complications, and lowering costs.21,24,25 Examples of preoperative optimization criteria by the multidisciplinary care in this review included a hemoglobin of 13 g/dL, 18 a hemoglobin A1c <7% or 8%,8,19 BMI <30, 19 controlled hypertension, and normal thyroid levels. 8 Smoking cessation was strictly enforced in almost all included studies, requiring the patients to be nicotine-free for a month to 6 weeks before their planned surgery.7,14,16,18 While current literature suggested that smoking does not significantly affect 30-day readmission rates and mortality, previous studies indicated that smoking is associated with long-term skeletal complications due to reduction of bone density leading to decreased healing capacity. 26 Therefore, smoking cessation should be a key component of surgical optimization.1,27,28 Multiple studies in this review also recommended a preoperative nutritional intervention, as part of ERAS protocols.7,15-19 Oe et al demonstrated that nutritional intervention with guidance and supplements reduced postoperative medical complications in malnourished patients. 17 Prehabilitation, which is the use of therapeutic exercise including physical exercise, nutrition supplementation, and behavioral health assessment, was recommended in 3 studies in this review.14,15,19 While past studies reported the benefits of prehabilitation in improving preoperative disability and reducing LOS in spine surgery, evidence does not yet support its widespread implementation in ASD patients.29-32 Pain management was common among the included studies to minimize opioid use and improve pain control, including multimodal analgesia plans and the preoperative administration of analgesics or nerve blocks. A recent article evaluating the evidence for proposed risk factors associated with perioperative complications following ASD surgery found good evidence supporting frailty as a significant risk factor. In the study, smoking, hyperglycemia, nutritional status, renal disease, cardiovascular disease, pulmonary disease, bone quality, and immunosuppression/steroid use had a fair level of evidence. 23 Given that frailty assessment was described in only 2 studies reviewed, it could be considered for integration as an additional intervention in ERAS protocols.7,15 For older patients, geriatric consultation for optimizing pain medication regimens to mitigate postoperative delirium and demotivation was recommended in 2 studies included in this review.7,15
Intraoperative interventions included in most of the studies were strategies to minimize blood loss and operative time, standard operating room team, and multimodal analgesia. Due to the elevated blood loss and transfusion rates in ASD surgeries, the ERAS protocols in this review have been centered around decreasing both of these parameters, as they have been shown to be correlated with increased risk of morbidity and mortality and postoperative complications.33,34 Major strategies to minimize blood loss described in these studies included: (1) infusion of tranexamic acid (TXA), (2) continuous monitoring of laboratory data, (3) standardized surgical procedure to minimize operative time. The use of tranexamic acid (TXA) given as an initial bolus dose and maintenance dose was present in the majority of papers included in this review. TXA has been shown to significantly decrease intraoperative and postoperative blood loss, as well as transfusion rates.33,35-37 Studies have demonstrated no increase in thromboembolic risks including DVT/PE/MI/CVA with their use in appropriate patient populations as well as TXA use in high risk thromboembolic patients.36,38 Other varying strategies have been integrated into ERAS protocols to achieve this goal, such as the standardization of staff and operating room protocols, use of hemostatic agents and antifibrinolytics, and reduced transfusion. Anesthesia protocols and continuous monitoring of laboratory data have been used to help limit intraoperative blood loss, specifically with applications of transfusion guidelines, fibrinolysis administration, goal directed fluid therapy, and a variety of intraoperative pain modalities. Adeyemo et al set intraoperative transfusion rates for hemoglobin at 10 g/dL with FFP given in a 1:3 ratio to pRBCs and platelets in a 1:5 ratio, 15 while Yokoi et al set their threshold at 8 g/dL with both papers showing a decrease in measured EBL. 18 Kim et al set exposure goals less than 400 cc estimated blood loss (EBL), procedural time less than 4.5 h, total EBL less than 1200 cc, with a result of a decrease in LOS and EBL. 8 Intraoperative transfusion protocol to manage coagulopathy, such as an international normalized ratio (INR), hematocrit, and platelet, can be one of the options to reduce perioperative complications, as previously reported. 6
Multiple studies in this review recommended a consistent operating room team that ultimately serves as a cornerstone for the application of intraoperative protocols. The data clearly demonstrated that staff who were experienced with complex spine surgical procedures and the attending surgeons’ workflow could reproducibly decrease operating room time.7,8 Intraoperative protocols combined with a dual attending surgeon approach in the operating room and patient clearance by a multidisciplinary team has demonstrated a decrease in EBL, major complications and return to operating room.6,21,39 Multimodal analgesia varied among authors with some using epidural catheters, 14 intraoperative infusions of lidocaine and ketamine14,16 and the use of transverse abdominis plane (TAP) blocks on anterior approach cases. 16 Common among studies was the use of non-opioid medications and treatments as shorter acting agents, such as lidocaine and ketamine, were preferred to promote early ambulation postoperatively.
Postoperative interventions included in this review aimed to facilitate postoperative recovery after ASD surgery. Common interventions to enhance recovery were (1) early mobilization/ambulation, (2) early nutritional support, and (3) multimodal analgesics. Early mobilization aims to reduce skeletal muscle loss and improve respiratory function and oxygen delivery to tissues. 40 In most of the studies in this review, patients were asked to start physical exercise from POD 0-1. Patients were encouraged to ambulate POD0 in 4 studies,7,8,16,19 and those on ERAS protocols ambulated significantly earlier than conventional pathways. In the study conducted by Kim HJ et al, many patients were not seen by physical therapy on POD0 despite setting a goal within the ERAS protocol that PT performs an initial evaluation and mobilization on POD 0. 8 However, almost all patients received the standardized multimodal regimen, and as a result, patients in the ERAS cohort were mobilized earlier than the historical cohort, and there was a trend toward an increased rate of home discharges. Jazini et al demonstrated patients on ERAS ambulated earlier (.6 days vs 1.1, P = .028) and had their urinary catheter removed earlier (2.7 vs 3.9 days, P = .006) compared to patients in conventional pathway, however, despite of mobilization 3 times a day, LOS in post-ERAS group was similar to pre-ERAS group. They noted that frequent ambulation on POD 0 by PT and consuming meals out of bed in a chair beginning on the day of surgery could facilitate early mobilization. 16 According to past studies, it is recommended for patients to sit out of bed for 2 h on the day of surgery and 6 h a day until discharge.41,42 Although there were few literatures examining the specific role of early mobilization in ASD surgery, early commencement of physical therapy in spine surgery patients has been shown to facilitate early return to functional activity in RCT. 29 Postoperative nutritional support, such as early oral fluid intake and protein shakes to supplement diet, were involved in most of the studies in this review. While there is no postoperative standardized nutritional protocol, previous studies have demonstrated reduction of postoperative complications by implementation of nutritional support and early rehabilitation.43,44 Acute postoperative pain management was clearly an important are of focus within ERAS protocols for ASD patients. Postoperative optimum pain relief has shown to facilitate early mobilization, early feeding and reduces stress related complications. 45 Conversely, inadequate acute pain control is associated with the development of chronic pain and significant systemic inflammatory response leading to organ dysfunction and pain. 46 While no studies have incorporated standardized multimodal analgesic pathways in ASD patients, several RCTs investigated multimodal opioid-sparing techniques for postoperative analgesia, including acetaminophen, NSAIDs, gabapentin, a2-agonists, S-ketamine, magnesium sulfate, high-dose steroids, and local anesthetic infusion or intravenous patient-controlled analgesia (PCA) with morphine.46-51 Most of the studies in this review used combinations of these drugs with PCA for breakthrough pain to minimize opioid use. With regard to postoperative oral medication, Alboog et al. looked into several commonly used medications in adult patients undergoing complex spine surgery, finding that pregabalin or gabapentin reduced postoperative opioid consumption and opioid-related side effects. 52 When developing a multimodal pain management plan, multiple factors, including patients’ medical history and comorbidities, type of surgery and anticipated postoperative pain, emotional and psychological status, baseline pain tolerance, and the risk-benefit of the various medications, are considered. 42 Therefore, collaboration with the pain management specialists is essential for postoperative multimodal analgesia. 6 Other common interventions to reduce complications in this review included deep venous thrombosis prophylaxis with compression stockings placement, nausea control, and early intravenous fluids discontinuation.
With regard to postoperative outcomes, the majority of studies reported significant improvements associated with implementation of ERAS protocol, including reduction in readmission rates and opioid consumption. Although medical complication rates were comparable between the pre-ERAS and post-ERAS group in 3 of 5 studies,7,8,14 the post-ERAS group generally tended to exhibit lower complication rates. Notably, 2 studies demonstrated a significantly reduced rate of medical complications in the post-ERAS group.17,19 In terms of LOS, while 4 studies showed a significant reduction in LOS,7,8,14,19 2 studies reported an increase.15,18 Although the meta-analysis indicated no significant difference in LOS between the pre-ERAS and post-ERAS groups, the observed difference was nearly significant. Focusing on the components of ERAS protocol, there was no relationship between LOS and the number of interventions implemented. Adeyemo et al discussed that the increase in LOS might be attributed to an emphasis on patient preparation prior to discharge under the ERAS protocol, such as education on the nutrition and rehabilitation services, and the use of electronic patient communication portal, and therefore, the lower rate of 90-day readmission was seen in the ERAS group.
15
Achieving postoperative objectives across multiple departments required substantial time and resources. Establishing a well-organized collaborative team can also take several years. Of note, studies showing an increase in LOS evaluated outcomes only 1 to 2 years after the implementation of ERAS protocols,15,18 whereas studies with reduction in LOS observed these effects over several years.7,8,14,19 Potential reasons for the lack of significant difference in LOS between the groups included (1) heterogeneity of the primary goals of the ERAS protocols, (2) relatively short-term outcomes, (3) small sample size, (4) moderate to high risk of bias in included studies due to retrospective study. LOS may have been influenced by the duration of implementation of ERAS protocol, the specific qualities and goals of each component, and confounding factors such as selection bias. Although LOS is certainly an important surrogate of acute post-operative outcomes in ASD care, different hospital systems may prioritize other factors when designing their ERAS protocols. Moreover, in the setting of the episode of care for ASD patients undergoing spinal reconstructive procedures, there may be several factors outside of the ERAS protocol itself that may be directly associated with LOS, such as social support.
53
As ERAS began as a patient-centered science, LOS may be secondary outcome related to pathophysiological principles such as complications, readmissions, and pain management, requiring additional time and effort to achieve multiple goals (Figure 5). The controversial impact of ERAS protocols on postoperative outcomes in ASD surgery.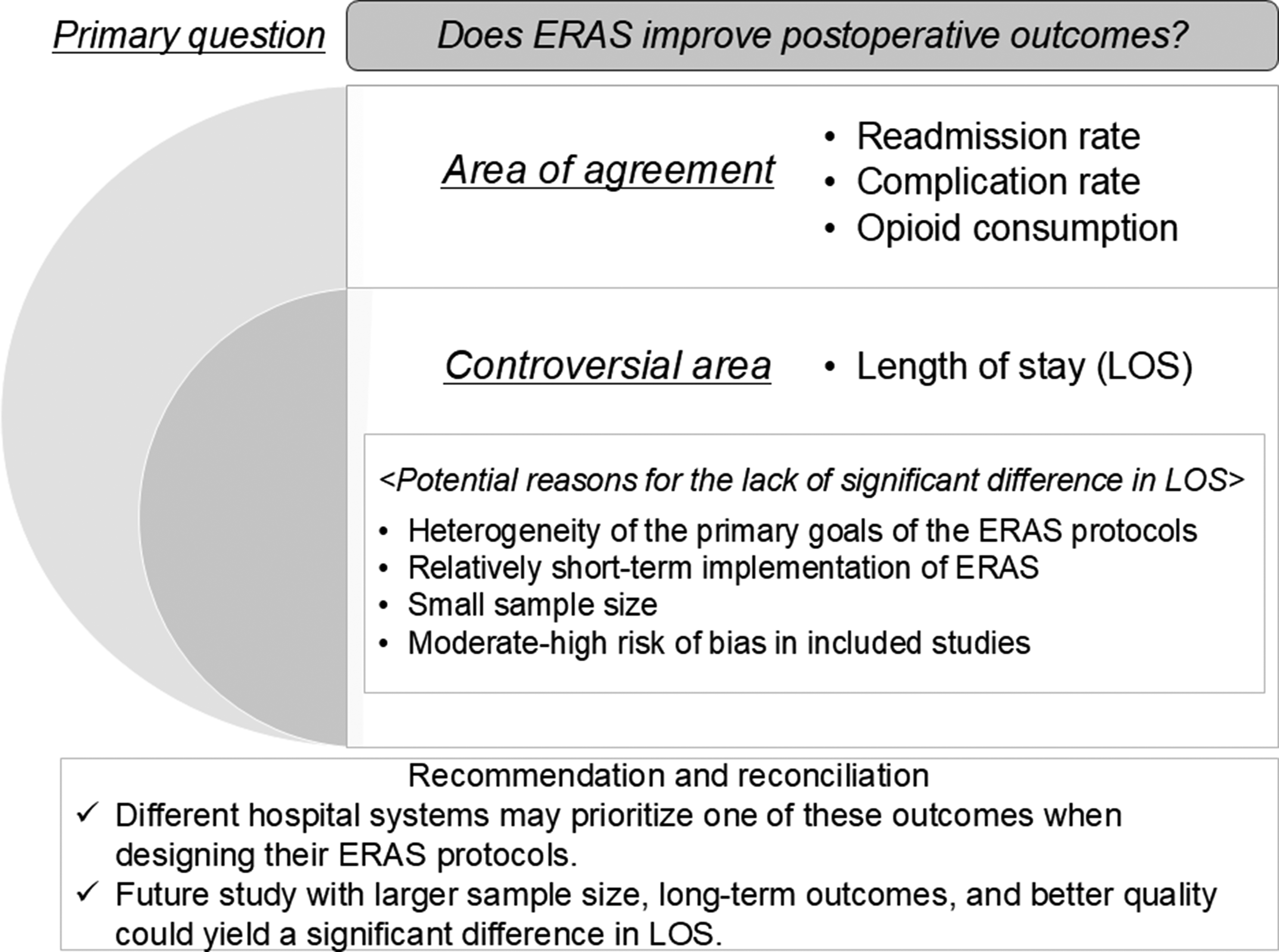
Limitations
There are several limitations of the current study. Due to the multifactorial nature of ERAS protocols, each study focused on different primary target of outcomes. Given the limited number of studies and insufficient outcome measures, we were unable to conduct a meta-analysis for overall complication rates, 90-day readmission rates, and opioid consumption, as the data was inadequate for pooling across multiple studies. Although The ERAS Society published a consensus statement for perioperative care in lumbar spinal fusion in 2021, 54 a consensus on ERAS protocol for ASD surgery is still lacking and studies evaluating the impact of ERAS on ASD surgery remain scarce. Specifically, evidence on effectiveness of mobilization on POD0, the frequency of ambulation, specific materials to support postoperative nutrition, and multimodal analgesics protocol has yet to be developed. Successful implementation of ERAS protocols requires collaboration, teamwork and patient understanding throughout the 3 different perioperative periods to facilitate the pathway. Despite the benefits of ERAS programs as effective and economically viable, challenges may arise when introducing into routine practice, including patient-related, staff-related and practice-related factors. Further studies are required to gain the consensus of each intervention to standardize the ERAS protocol for patients undergoing ASD surgery.
Conclusion
ERAS protocols for ASD surgery consist of preoperative optimization, intraoperative stress minimization, and postoperative recovery facilitation. Common interventions included: (1) preoperative anesthesia-related risk assessment, multidisciplinary assessment, and cessation of smoking, (2) intraoperative TXA administration and continuous monitoring of lab data, and (3) postoperative early mobilization and early nutritional support. Additionally, pain management through multimodal analgesia is essential throughout the entire episode of care. Although meta-analysis demonstrated no significant difference in LOS between the groups and postoperative outcomes varied across studies, the majority of studies reported improvements associated with implementation of ERAS protocol, including reduction in readmission rates, medical complications, opioid consumption, and LOS. LOS may be secondary outcome related to pathophysiological principles, requiring additional time and effort. Further studies are required to standardize the ERAS protocol for ASD surgery and enhance the impact on multiple postoperative outcomes.
Footnotes
Author Contributions
Takeshi Fujii, MD, PhD (Study design, data collection, manuscript preparation). Rakesh Kumar MD (Study design, data collection, manuscript preparation). Patricia Lipson, BS (Study design, data collection, manuscript preparation). Kellen Nold, PA-C (Study design, results review, manuscript preparation). Aiyush Bansal, MD (Study design, statistical analysis, risk of bias assessment, manuscript preparation). Murad Alostaz, BS (Study design, data collection, manuscript preparation). Philip K. Louie MD (Study design, results review, manuscript preparation). Rajiv K. Sethi MD, PhD (Study design, results review, manuscript preparation).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
A list of include studies and the search strategy have been provided in the manuscript and table.