
Abstract
Study Design:
In vitro biomechanical study.
Objective:
The strength of the alar ligament has been described inconsistently, possibly because of the nonphysiological biomechanical testing models, and the inability to test the ligament with both attachments simultaneously. The purpose of this biomechanical model was to reevaluate the alar ligament’s tensile strength with both bony attachments, while also keeping the transverse ligament intact, all in a more physiological biomechanical model that mimics the mechanism of traumatic injury closely.
Methods:
Eleven fresh-frozen occipito-atlanto-axial (C0-C1-C2) specimens were harvested from individuals whose mean age at death was 77.4 years (range 46-97 years). Only the alar and transverse ligaments were preserved, and the bony C0-C1-C2 complex was left intact. Axial tension was exerted on the dens to displace it posteriorly, while the occipito-axial complex was fixed anteriorly. A device that applies controlled increasing force was used to test the tensile strength (M2-200, Mark-10 Corporation).
Results:
The mean force required for the alar ligament to fail was 394 ± 52 N (range 317-503 N). However, both the right and left alar ligaments ruptured simultaneously in 10 specimens. The ligament failed most often at the dens (n = 10), followed by occipital condyle rupture (n = 1). The transverse ligament remained intact in all specimens.
Conclusions:
When both the right and left alar ligament were included, the total alar ligament failure occurred at an average force of 394 N. The alar ligament failed before the transverse ligament.
Introduction
The first part of this study highlights the transverse ligament’s biomechanics and its tensile properties as a major stabilizer of the craniocervical junction (CCJ). The alar ligaments are thick cords that join the dens of C2 to the occipital condyles and limit C0-C2 extension, axial rotation, and lateral bending. Indeed, the landmark studies Dvorak and Panjabi 1 carried out formed the foundation for the understanding of, as well as future research on, the CCJ’s major ligaments. However, the recent literature has reported varied and inconsistent results that make reevaluation necessary. The landmark studies on the alar ligaments involved removal of the transverse ligament, which, while necessary for an accurate measure of the ligament’s tensile properties, may not be the most specific when considering the physiological in vivo mechanisms of CCJ trauma in which all major stabilizing ligaments are intact. Because the alar ligaments’ tensile strength has been explored well in isolation, the second installment of this study is designed to describe the ligaments’ biomechanics in a more physiological model of CCJ trauma by preserving the state of the transverse ligament during loading, while testing the rupture of the left and right alar ligaments simultaneously.
Material and Methods
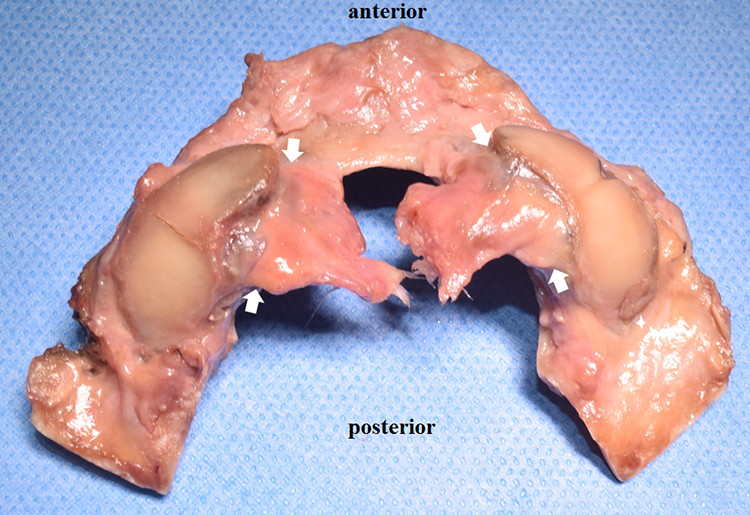
A total of eleven occipito-atlanto-axial (C0-C1-C2) specimens was harvested from 9 male and 2 female fresh-frozen Caucasian (n = 10) and Hispanic (n = 1) cadavers with a mean age of 77.4 years (range 46-97 years). After all muscles were removed, the cadavers were assessed for pathologic changes, such as previous trauma, malformations, tumors, and other abnormalities. After extracting the C0-C1-C2 complex, the dura mater, spinal cord, lateral and oblique atlanto-occipital ligament, atlanto-dental ligament, anterior longitudinal ligament, tectorial membrane, superior and inferior longitudinal bands of the cruciform ligament, and C1-C2 joint capsules were removed. Furthermore, the apical ligament was cut due to the fact that this ligament represents a remnant of the notochord (rudimentary nucleus pulposus) without adding biomechanical stability to the CCJ. 2 To support stabilization of the anterior C0-C1 complex, the anterior atlanto-occipital membrane was left intact. The alar and transverse ligaments were preserved (Figure 1). Radiographic imaging was not available.
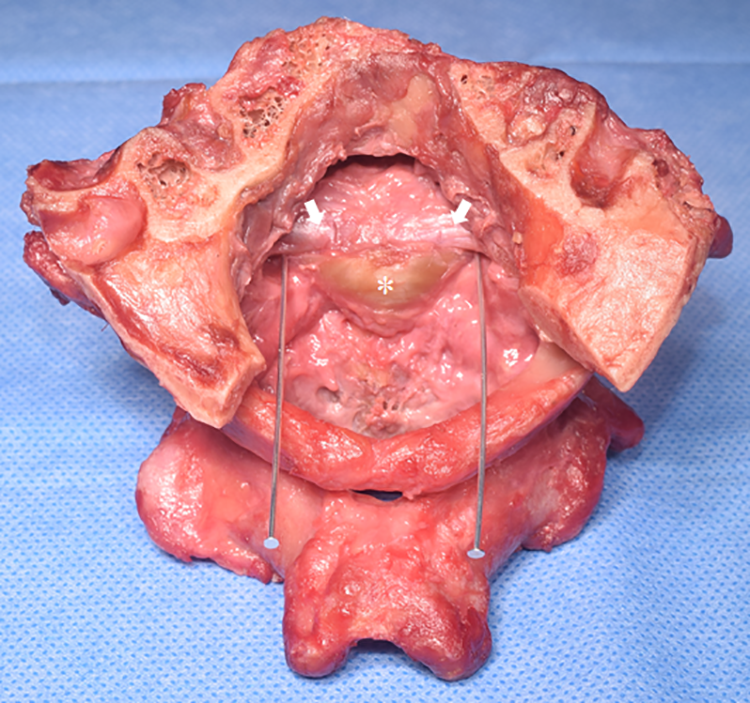
Posterior view of the harvested occipito-atlanto-axial complex. A small part of the posterior occiput was cut. Two metal pins were placed between the alar ligament (arrows) and transverse ligament (*).
The C0-C1-C2 specimens were then secured in a strength testing device (M2-200, Mark-10 Corporation). A bony clamp was fixed circumferentially around the dens from the posterior between the alar and transverse ligaments. To verify correct clamp position anteriorly, one-third of the anterior atlas and a small part of the occiput was removed (Figure 2).
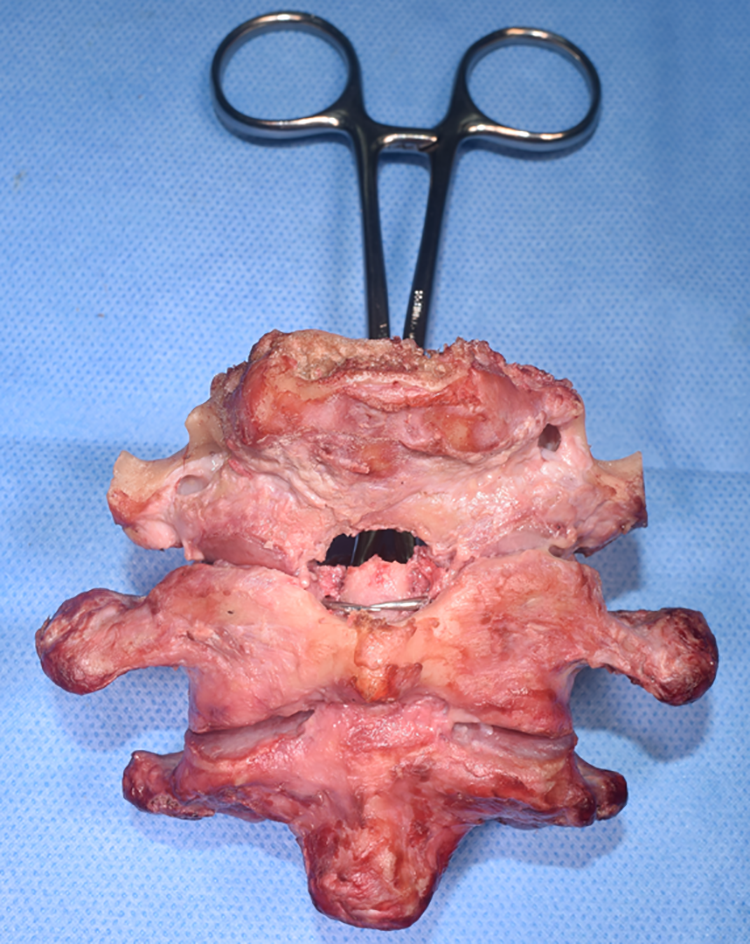
Anterior view of the occipito-atlanto-axial complex. A bone clamp was placed between the alar and transverse ligament from posterior. To ensure correct placement of the clamp, one-third of the anterior arch of the atlas was drilled out.
Two bony clamps were used to fix the C0-C1 complex from the anterior (Figure 3A). Once the entire complex was secured with the clamps, horizontally controlled increasing force was applied (Figure 3B). The anterior C0-C1 complex was displaced anteriorly (Farch), while axial tension was exerted on the dens (Fdens) to displace it posteriorly (Figure 4). The peak force (N) was recorded at the first ligament’s (always the alar ligament) point of failure. Failure was defined as the alar ligament’s complete rupture on both sides. We categorized the rupture locations as condylar or dens rupture. After the testing, the dens was split in half along its sagittal axis to identify any cysts or hidden pathologies that may have influenced the integrity of the alar ligament’s attachment to the dens.
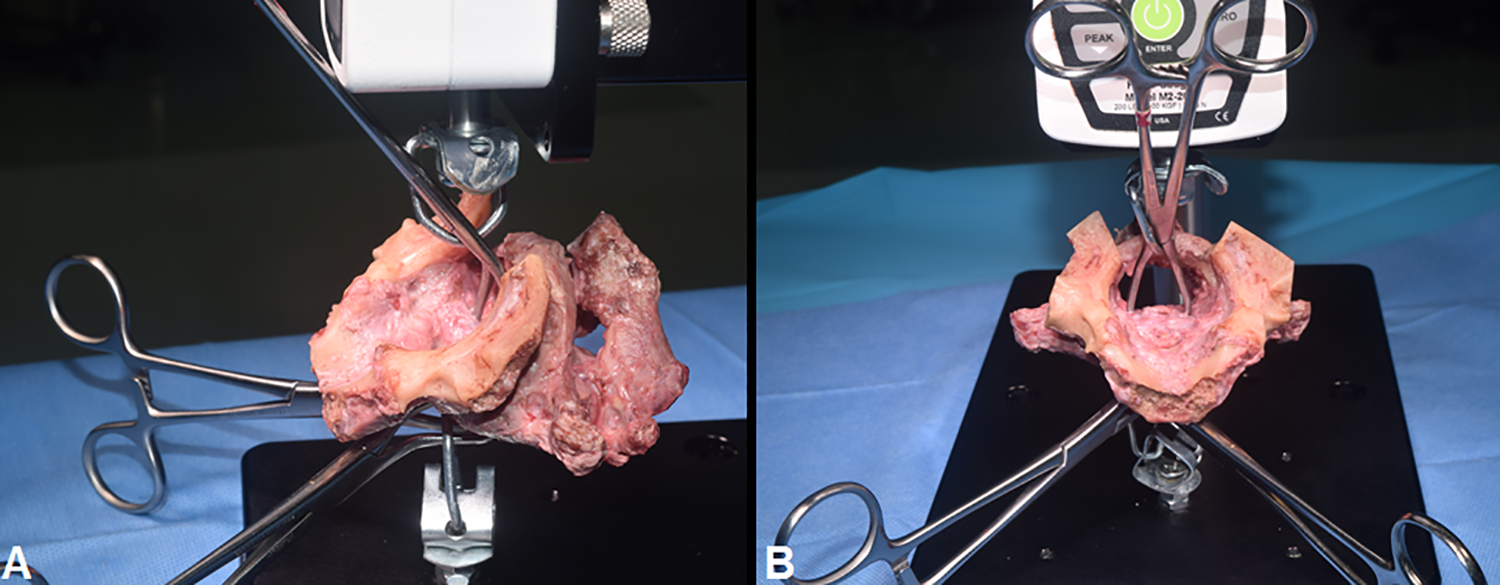
Lateral (A) and superior (B) view of the harvested specimen secured in the testing machine. Two bony clamps fix the occipito-atlantal complex, one of which is placed around the dens from the posterior to apply horizontally controlled increasing force.
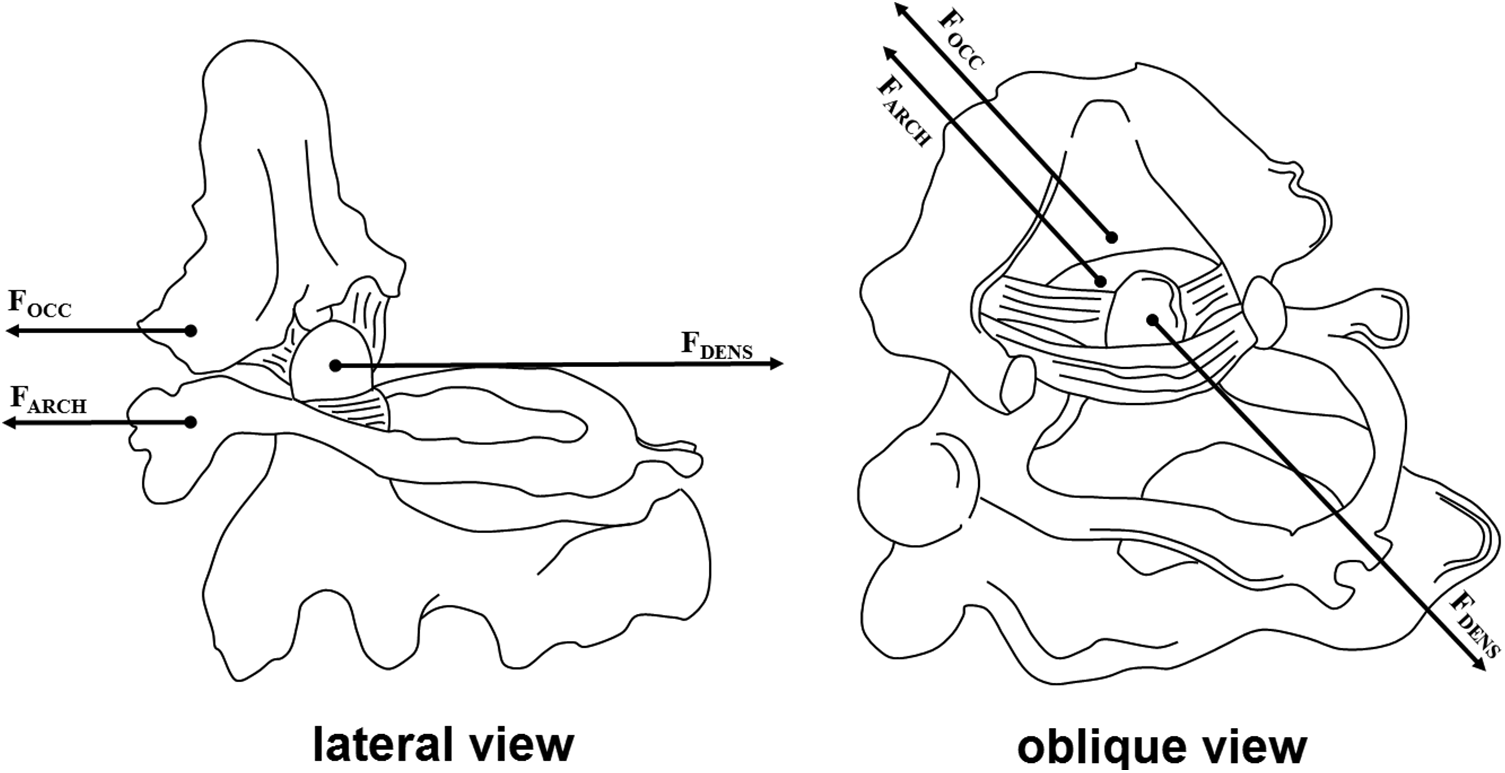
Forces on occipito-atlanto-axial complex (lateral and oblique view) during testing process.
The differences in the failure force between sex and age groups were compared. To assess the relationship between failure force and age we divided the specimens into 2 different age groups: group I (<80 years old) and group II (>80 years old). A Student’s t test was used, and a P value of <.05 was considered to indicate a significant relation. SPSS v. 22 (IBM Corp) was used for statistical analysis. The Anatomical Quality Assurance checklist (AQUA) also was used in this cadaveric study. 3,4 Institutional review board approval is not required at our institution for a cadaveric study, and the work was performed in accordance with the 1964 Helsinki Declaration and its later amendments.
Results
The alar ligaments’ mean force at failure on both sides was 394.5 ± 52 N (range 317-503 N). In 1 male specimen, the ligament did not rupture simultaneously on both sides, and therefore, additional force was applied to cause complete rupture (Table 1). In this specimen, the alar ligament ruptured on the right and in part on the left side after 296 N with an additional force of 207 N required to cause a complete rupture. As there were only 2 female specimens, it was not possible to make statistically reliable statements with regard to force and gender. In group I, the mean failure force was 395.3 N (±26.9) and in group II, it was 393 N (±76.9). There was no significant difference between the groups (P > .05). The alar ligament failed at the dens in most specimens (n = 10; Figure 5), although rupture occurred at the occipital condyles in 1 specimen. Interestingly, the alar ligament that ruptured at the occipital condyles required the lowest failure force (317 N). The transverse ligament remained intact during all testing. No signs of fractures, malformations, congenital abnormalities, tumors, or other pathologies were found in any specimen before or after testing.
Characteristics and Results of the Tested Specimens.
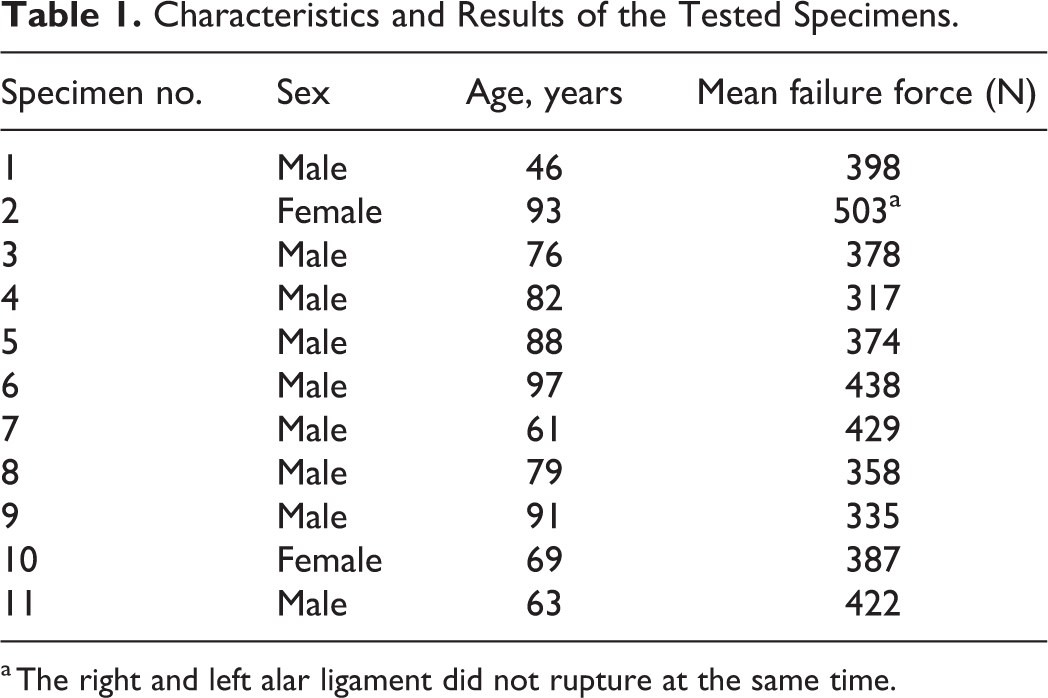
a The right and left alar ligament did not rupture at the same time.
Inferior view of the alar ligament attachment (arrow) into the anterior two-thirds of the occipital condyles after rupture from the dens.
Discussion
History of the Anatomical Understanding of the Alar Ligaments
Historically, there has been confusion with regard to the alar ligaments’ exact embryology, anatomy, and morphology. 5,6 Previously, it was believed that the alar ligaments conveyed a single occipital-odontoid attachment from the occipital condyles spanning inferomedially to the lateral surfaces of the dens’ apex. Dvorak et al 1 described a discrete atlantal portion of the alar ligament, approximately 3 mm in length, in 12 of 19 specimens that connected the alar ligaments’ inferior fibers to the atlas’s lateral masses. This second portion of the alar ligaments may offer additional resistance to the anterior translation of C1 over C2, together with the remarkable transverse atlantal ligament, albeit there is a lack of evidence of this atlantal portion in the literature from the work of Dvorak and Panjabi 1 to the present. Recent cadaveric studies performed by Cattrysse et al, 7 Osmotherly et al, 8 and Iwanaga et al 9 and the magnetic resonance imaging (MRI) study by Krakenes et al 10 revealed no evidence of the atlantal portion described previously. These observations of the atlantal portion of the alar ligament likely are anatomical variations or soft tissue/vascular artifacts. 8
In major medical texts, the alar ligaments are illustrated as more vertical and V-shaped; however, recent studies have provided conclusive support that, in fact, the ligaments are oriented horizontally more commonly. 9,11 For example, Osmotherly et al 8 reported that 63.6% of cadaveric ligaments were horizontal (n = 11). These findings are consistent with the alar ligaments’ known role in limiting atlanto-axial rotation. Dvorak and Panjabi 1 studied the alar ligaments’ functional anatomy through computed tomography (CT), and reported that 12 of 19 ligaments were “almost” parallel to the dens and occipital condyle, while 7 of 19 were flat (150°170°). Iwanaga et al 12 reported that the angle both alar ligaments formed was 149° ± 24.19° (range 105°-180°) in their study of 22 alar ligaments. Knowledge of these ligaments’ biomechanics derives currently from the pioneering anatomical studies performed several decades ago, and recently, by Iwanaga et al 9,12 and Osmotherly et al. 8
Biomechanical Studies
The precedent biomechanical study by Dvorak et al 13 of the alar ligaments used seven fresh-frozen cadavers. After harvesting the occipito-atlanto-axial complex and cutting the posterior arch of the atlas, the alar and transverse ligaments were carefully dissected. The anterior arch was cut along the midline, and then the specimens were mounted on the testing device. Three specimens were excluded from testing due to damage and anatomical circumstances during preparation and mounting. The spinous process of C2 was clamped to a support plate, a steel bar fixed the body, and a cable secured the anterior tubercle. The C2 body and dens were fixed and rotated 90° on their sagittal axis; therefore, the fragment of occipital bone is pulled superiorly to apply tension to the alar ligament. Axial load was applied to the ligaments at 1.5 mm/s. The alar ligaments’ mean tensile strength was found to be 212 ± 81 N (left) and 216 ± 60 N (right).
Although the methodology of Dvorak et al 13 does apply strain to the ligament adequate to cause rupture, we question whether or not this strain could be followed more physiologically. In many studies, bone-ligament-bone preparations involve a significant amount of bone removal to fixate portions of the occipito-atlanto-axial complex, and may influence the results of tensile strength testing. Removal of bony fragments may affect the bone-ligament-bone preparations’ integrity and the way forces are transmitted along the trabecular bone as tension is applied to the ligament.
Panjabi et al 14 published another important study of the alar ligaments, the results of which may be applicable to low- and high-energy trauma to the CCJ. In their study, a total of 19 unilateral alar ligaments was harvested from 11 fresh-frozen human cadavers aged 37 to 53 years. Each ligament was dissected carefully, and the dens was detached from the C2 body. After harvesting the alar ligaments’ occipital attachments via cutting out 1 cm bone cubes, a left and right alar ligament, as well as the dens were anchored in blocks with polyester resin. Each ligament underwent prestretching to a sub-injurious load until failure. 13 During slow testing, 14 unilateral alar ligaments sustained irreversible damage, and therefore, only five could be tested at a fast extension rate (920 mm/s) by fixing these in an apparatus the authors designed that included a pneumatic cylinder. The mean strain when the alar ligament failed was 3%, the mean energy absorbed was 122.6 N mm, and the failure load was 367 ± 83.2 N.
The removal of bone may have been a limitation in the work of Panjabi et al. 14 Further methodological errors may stem from drilling into the trabecular bone, which causes alterations that would not be present in vivo otherwise. Moreover, testing up to a predetermined sub-injurious load may cause microtears in the alar ligaments’ fiber bundles that result in a lower failure force. This may explain why our study demonstrates higher mean failure force values (394 ± 52 N), as the methodology did not cause any tissue deformation prior to testing. They mention further that all but 5 unilateral alar ligament specimens showed sudden minor drops in load during the slow extension rate testing, indicating that the ligament might have been in the process of rupturing. The motivation for slow testing of the ligaments to a subinjurious load without failure is questionable, as it has no immediate clinical relevance.
Iwanaga et al 12 published the most recent biomechanical study. After removing the occipito-atlanto-axial complex en bloc, all soft tissue and ligaments were stripped to expose the alar ligament with its bony attachments. The base of the dens and occipital condyles then were fixed vertically via bony clamps to a tensile strength testing device. Each side of the alar ligament was tested individually by using slow extension rates. All ligaments’ failure force ranged between 87 and 346 N, with a mean of 186.9 ± 69.7 N. Unlike previous works, Iwanaga et al 12 noted that there was a significant difference in failure force between males and females (215.8 ± 70.8 vs 137.3 ± 29.3 N). Much like previous tests on the ligament, this study had some limitations, in that the entire C0-C1-C2 complex was not left intact and both ligaments were not tested simultaneously.
This cadaveric study is the first to (1) test failure of the right and left alar ligament simultaneously and (2) test the strength of alar ligaments with an intact transverse ligament. Furthermore, this study obtained similar values, while also keeping both ligaments, their attachments, and the occipito-atlanto-axial complex intact. This relation may validate the more natural physiological mechanism by which the ligaments were tested in the study and may therefore led to a higher tensile strength of the alar ligament as compared with Panjabi et al 14 and Iwanaga et al. 12
Clinical Implication
Considering the alar ligament’s anatomical characteristics and biomechanical properties, the authors hypothesize that rupture of the alar ligament, without involvement of the transverse ligament, most probably occurs when the head is subjected to sudden movement in rotation and hyperflexion. In this scenario, the abrupt forces needed to rupture the alar ligament are not enough to cause transverse ligament failure. Therefore, special attention to the alar ligament should be given when evaluating the CCJ after an adequate trauma. In difficulties to interpret signal intensity of the alar ligament in MRI, guided cervical spine flexion-extension radiographs can be useful.
Limitations
One major limitation is the relatively small number of cadaveric specimens tested. More specimens would refine the alar ligament’s strength threshold value. Furthermore, the ligament’s biomechanical properties may differ in younger patients, and although we used fresh-frozen specimens, the differences between cadaveric and live tissue’s properties must be considered as well. Another limitation results from the fact that the dimensions of the alar ligament were not studied. We also applied horizontally controlled increasing force due to the fact that we could not find another adequate biomechanical testing model in which we could fix the occipito-atlanto-axial complex to test other biomechanical testing modalities, for example, rotation to simulate neck torsion. Despite these limitations, we believe this cadaveric study presents the most accurate data on the alar ligament’s strength in a more physiological setting.
Conclusion
The mean force required to cause the alar ligament to fail was 394 ± 52 N and ranged from 317 to 503 N. The alar ligament failed before transverse ligament rupture occurred. Further biomechanical studies will be needed to determine the alar ligament’s strength within other stabilizing ligaments of the CCJ and to evaluate the forces when rotation and lateral bending are applied.
Footnotes
Acknowledgments
We thank the donors and their families for their gifts, which definitely advanced our knowledge of the transverse ligament’s strength.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.