
Abstract
Study Design:
Retrospective case-control study.
Objectives:
Vertebral end plate (EP) lesions include Modic changes, Schmorl’s nodes, EP erosion, EP sclerosis, and so on. While previous studies have mostly focused on the association between vertebral EP lesions and low back pain, few studies evaluated the influence of vertebral EP lesions on the radiological outcomes in lumbar interbody fusion.
Methods:
This study included a total of 125 operated disc levels from 86 consecutive patients who underwent a 1- or 2-level oblique lateral interbody fusion (OLIF) and had more than 1-year regular follow-up. The presence of vertebral EP lesions, changes in disc heights/angle, cage subsidence, and fusion grade were examined. The associations between vertebral EP lesions and radiological parameters were analyzed.
Result:
The presence of Modic changes, Schmorl’s node, EP cartilage erosion, and EP sclerosis were found in 72 (57.6%), 26 (20.8%), 31 (24.8%), and 44 (35.2%) disc levels, respectively. The mean anterior disc height increased from 6.9 ± 3.8 mm to 13.1 ± 2.7 mm (P < .001) and the mean segmental angle increased from 2.9° ± 5.8° to 9.2° ± 4.8° (P < .001) at the last follow-up. The overall fusion rate was 98.4% (123/125) and cage subsidence rate was 7.2% (9/125). All radiological parameters and cage subsidence rate were not different regardless of vertebral EP lesions.
Conclusions:
Vertebral EP lesions did not affect the overall radiological outcome in 1- or 2-level OLIF. These results come from the stable contact between lateral cage and peripheral rim of vertebral EP.
Keywords
Introduction
Vertebral end plate (EP) provides nutritional transport between vertebral capillaries and nucleus pulposus by diffusion. 1 This physiological function explains its fragile structure of a thin cartilage layer with a porous subchondral trabecular bone. However, vertebral EP sustains considerable amount of compressive loads and distribute the intradiscal pressure onto the adjacent vertebrae. 2 This conflicting mechanical function makes the vertebral EP vulnerable to external stress.
Vertebral EP lesions have been hypothesized as a cause of discogenic back pain because the subchondral trabecular bone has rich vascularity and innervation in contrast to the avascular and aneural intervertebral disc.2,3 Vertebral EP lesions include bone marrow lesions (Modic changes), intravertebral disc protrusion (Schmorl’s nodes), EP cartilage erosion, and EP sclerosis (Figure 1).4-10 Although numerous studies investigated the association between vertebral EP lesions and low back pain, this still remains controversial.3,7,11,12
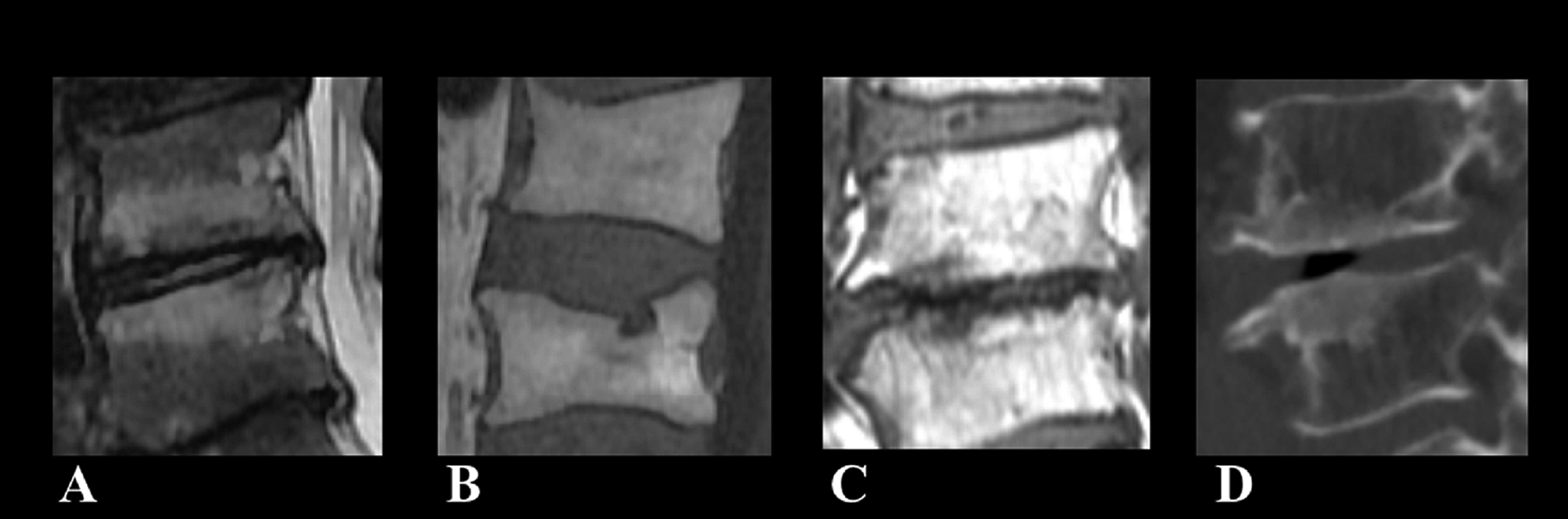
Vertebral end plate (EP) lesions: (A) Modic changes, (B) Schmorl’s nodes, (C) EP cartilage erosion, and (D) EP sclerosis.
In lumbar interbody fusion, adequate manipulation of vertebral EP and proper placement of intervertebral graft are essential. The graft should distract the intervertebral space to restore the canal space and the neural foramen. Compression force is then applied on the graft-subchondral trabecular bone interface to provide initial stability and to promote the graft incorporation. If the subchondral trabecular bone fails to resist the compressive load, complications including graft subsidence, loss of disc space restoration, nonunion, or graft failure may occur. Vertebral EP lesions may affect the mechanical and biological property of graft incorporation on the subchondral trabecular bone during lumbar interbody fusion.9,13 In the current study, we aimed to examine whether vertebral EP lesions are risk factors for unfavorable radiological outcomes in oblique lateral interbody fusion (OLIF).
Methods
Patients
This study involved a retrospective analysis of 125 operated disc levels from 86 consecutive patients who underwent a 1- or 2-level OLIF for lumbar degenerative disease and had more than 1-year regular follow-up. Informed consent was obtained from each subject. All patients underwent routine preoperative standing anteroposterior (AP)/lateral radiography of the lumbar spine, computed tomography (CT), and magnetic resonance (MR) imaging. OLIF procedures were performed by a single spine surgeon (N.C.) using the original Hynes’s technique (Figure 2). 14 Briefly, each patient was placed in the 90° right lateral decubitus position on a Jackson spinal surgery table (Mizuho OSI) under general anesthesia. The exact lateral position was confirmed by AP/lateral C-arm fluoroscopic images. For L2-3 to L4-5 level, an anterior retroperitoneal approach was made between the psoas muscle and abdominal aorta, and the OLIF 25 tubular retractor system (Medtronic Inc) was set. For L5-S1 level, OLIF 51 retractor system (Medtronic Inc) was applied to expose the L5-S1 disc space between the bifurcations of iliac vessels. The disc and cartilage EPs were then prepared for interbody fusion. A lateral polyetheretherketone (PEEK) cage (Clydesdale; Medtronic Inc) filled with autologous iliac crest bone graft and demineralized bone matrix was used at the L2-3 to L4-5 level. An anterior PEEK cage (Perimeter; Medtronic Inc) was used at the L5-S1 level. On completion of the anterior procedure, supplemental posterior pedicle screw instrumentation was performed with either open or percutaneous technique. Data on the patients’ sex, age, preoperative diagnosis, body mass index (BMI), bone mineral density (BMD), smoking, operative time, estimated blood loss, and cage parameters (cage height, width, and lordotic angle) was obtained from their medical records. The hospital’s ethics committee reviewed and approved the present study.
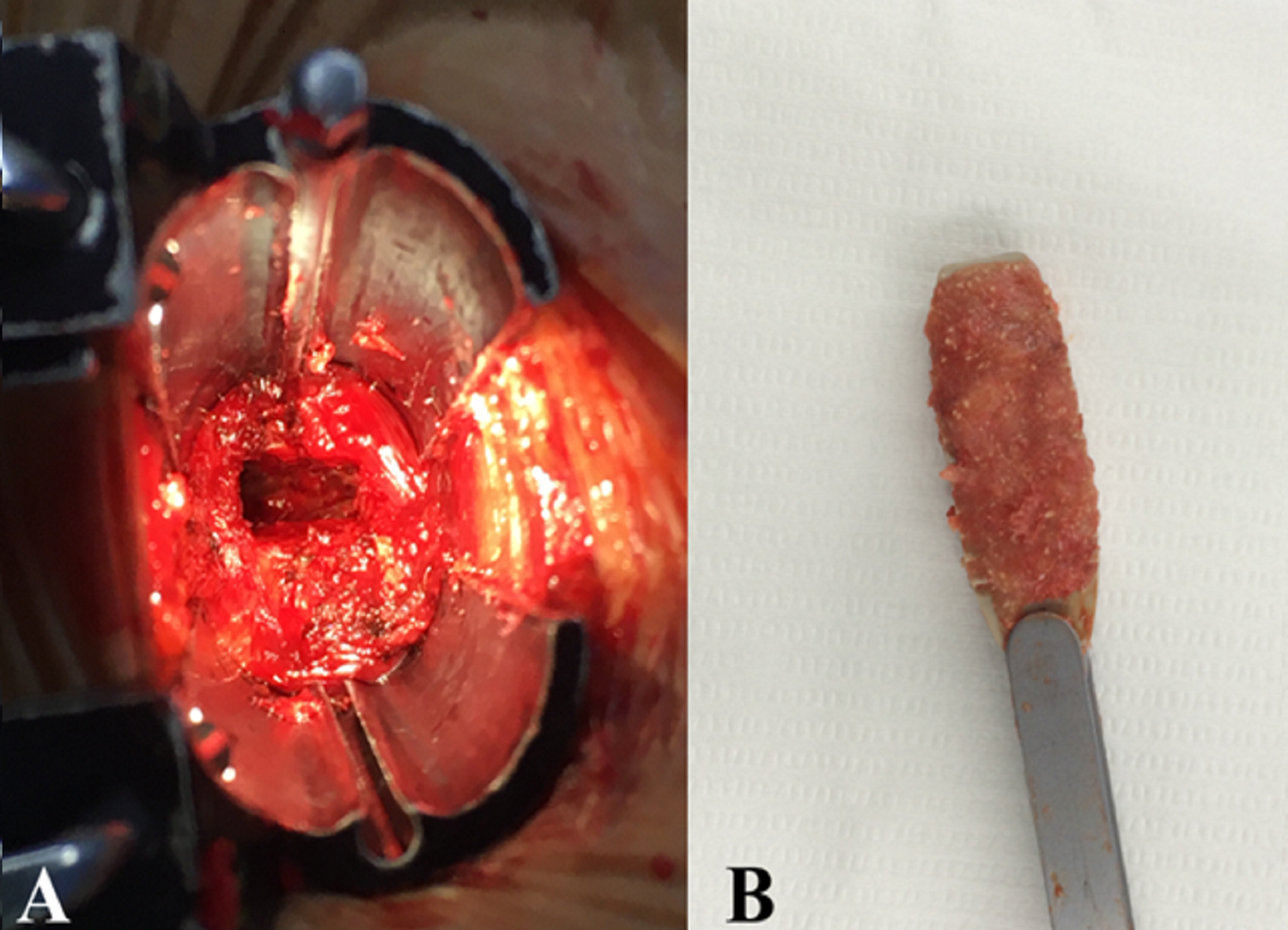
Oblique lateral interbody fusion (OLIF) procedures. (A) Discectomy and cartilaginous end plate (EP) removal was performed through OLIF 25 tubular retractor system. (B) Lateral cage was filled with autologous iliac crest bone graft and demineralized bone matrix.
Evaluation of Vertebral EP Lesions
Using the T1- and T2-weighted sagittal MR images, the presence and type of Modic changes, Schmorl’s node, and EP cartilage erosion (EP cartilage defect >1 cm) were examined. Using CT images of the lumbar spine, the presence of EP sclerosis was examined. Two independent observers (2 spine surgeons) evaluated the vertebral EP lesions twice, with an interval of 1 week. Disagreements were resolved through discussion until a consensus opinion was reached.
Radiological Outcome of OLIF
Radiological measurements included anterior/posterior disc heights, segmental angle, cage subsidence, and fusion grade. The anterior/posterior disc heights and segmental angle were measured on the preoperative and on the last follow-up standing lateral radiograph of the lumbar spine. Fusion grade was evaluated on the postoperative 1-year CT images based on the criteria established by Bridwell et al. 15 Briefly, fusion was categorized as follows: (1) grade 1, fused with remodeling and trabeculae present; (2) grade 2, graft intact, not fully remodeled and incorporated, but no lucency present; (3) grade 3, graft intact, potential lucency present at top and bottom of graft; and (4) grade 4, fusion absent, collapse or resorption of the graft. Grade 1 and 2 were considered as a successful fusion. Cage subsidence was evaluated using postoperative and serial follow-up standing lateral radiographs, and was defined as present if a cage was observed to sink into an adjacent vertebral body by >2 mm, based on comparisons with previous radiographs. 16 The radiological measurements were performed by a single spinal surgeon using a picture archiving and communication system (PiViewerSTAR; INFINITT) equipped with an integrated digital measurement feature.
Statistical Analysis
The preoperative anterior/posterior disc heights and segmental angle were compared with those on the last follow-up radiographs using a paired t test. The associations between the radiological parameters and patients’ demographics, cage parameters, or vertebral EP lesions were analyzed using one-way analysis of variance test, chi-square test, or Pearson’s correlation test. Inter- and intraobserver reliabilities for the categorization of the vertebral EP lesions were estimated using kappa values. Agreement was rated as fair, moderate, substantial, or excellent with respective kappa values of 0.21 to 0.4, 0.41 to 0.60, 0.61 to 0.8, or >0.81. Statistical analysis was carried out using SPSS for Windows software (version 19.0; IBM Corp). In all analyses, P < .05 was taken to indicate statistical significance.
Results
Subject Characteristics
The study population consisted of 32 men and 54 women with a mean age of 64.7 ± 9.1 years (range, 37-80 years). The mean follow-up duration was 28.6 ± 12.1 months (range, 12-61 months). The mean BMI was 25.8 ± 3.9 m/kg2 (range, 18.2-36.5 months), and the mean T score of the spine BMD was −1.2 ± 1.2 (range, −3.5 to 2.2). The diagnosis was degenerative spondylolisthesis in 46 (36.8%) patients, spinal stenosis in 32 (25.6%), degenerative disc disease in 26 (20.8%), and spondylolytic spondylolisthesis in 21 (16.8%). The number of current smokers was 27 (21.6%). Among the 125 operated levels, 4 (3.2%) were located at L2-3 level, 28 (22.4%) at L3-4 level, 64 (51.2%) at L4-5 level, and 29 (23.2%) at L5-S1 level. Single-level OLIFs were performed in 47 (54.7%) patients, while 2-level OLIFs in 39 (45.3%). The size of cages was 14 mm height in 33 (26.4%) cases, 12 mm in 72 (57.6%), 10 mm in 17 (13.6%), and 8 mm in 3 (2.4%). The lordotic angle of cages was 18° in 2 (1.6%) cases, 12° in 71 (56.8%), 8° in 4 (3.2%), and 6° in 48 (38.4%).
Vertebral EP Lesions
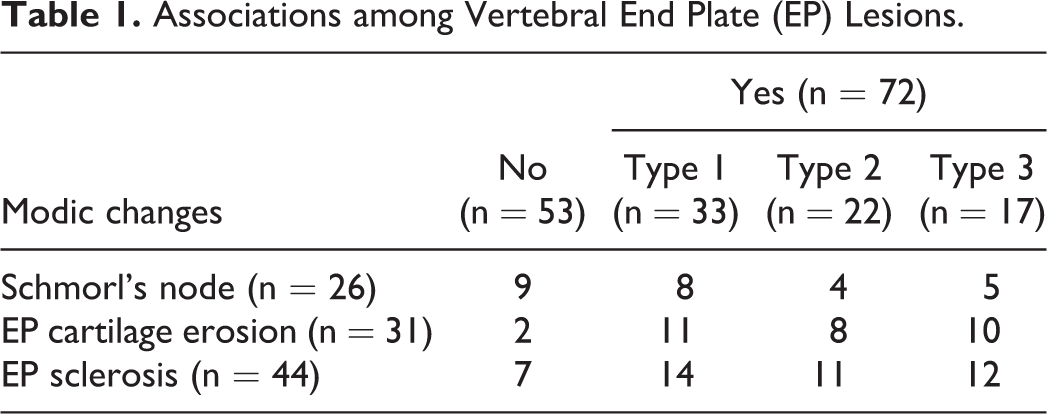
Among the 125 operated levels, Modic changes were observed in 72 (57.6%) levels; type 1 was 33 (26.4%) levels, type 2 was 22 (17.6%), and type 3 was 17 (13.6%). Schmorl’s node, EP cartilage erosion, and EP sclerosis were found in 26 (20.8%) levels, 31 (24.8%), and 44 (35.2%), respectively. There was no difference in the occurrence of Schmorl’s node, EP cartilage erosion, and EP sclerosis among the 3 types of Modic changes (all Ps > .05). The associations among vertebral EP lesions are illustrated in Table 1.
Associations among Vertebral End Plate (EP) Lesions.
Radiological Outcomes and Associated Factors
Of the 125 operated levels, the mean anterior disc height increased from 6.9 ± 3.8 mm to 13.1 ± 2.7 mm (mean increase of 6.2 ± 3.8 mm, P < .001) at the last follow-up. The mean posterior disc height increased from 4.9 ± 2.1 mm to 6.9 ± 2.3 mm (mean increase of 2.0 ± 2.3 mm, P < .001). The mean segmental angle increased from 2.9° ± 5.8° to 9.2° ± 4.8° (mean increase of 6.3° ± 6.2°, P < .001). The overall fusion rate was 98.4% (123/125) and the cage subsidence rate was 7.2% (9/125). Among the patient’s demographics, age (68.9 ± 5.8 years vs 63.5 ± 10.1 years, P = 0.044) and BMI (28.0 ± 3.3 kg/m2 vs 25.3 ± 3.9 kg/m2, P = .011) were significantly higher in patients with cage subsidence. There was no association between other radiological parameters and sex, BMD, smoking, operative time, estimated blood loss, or operated level (all Ps > .05). Among the cage parameters, cage angle was associated with the segmental angle at the last follow-up (R = 0.488, P < .000). No association was found between other radiological parameters and cage height or cage width (all Ps > .05). Table 2 summarizes the association between vertebral EP lesions and radiological parameters.
Vertebral End Plate (EP) Lesions and Radiological Outcomes.a
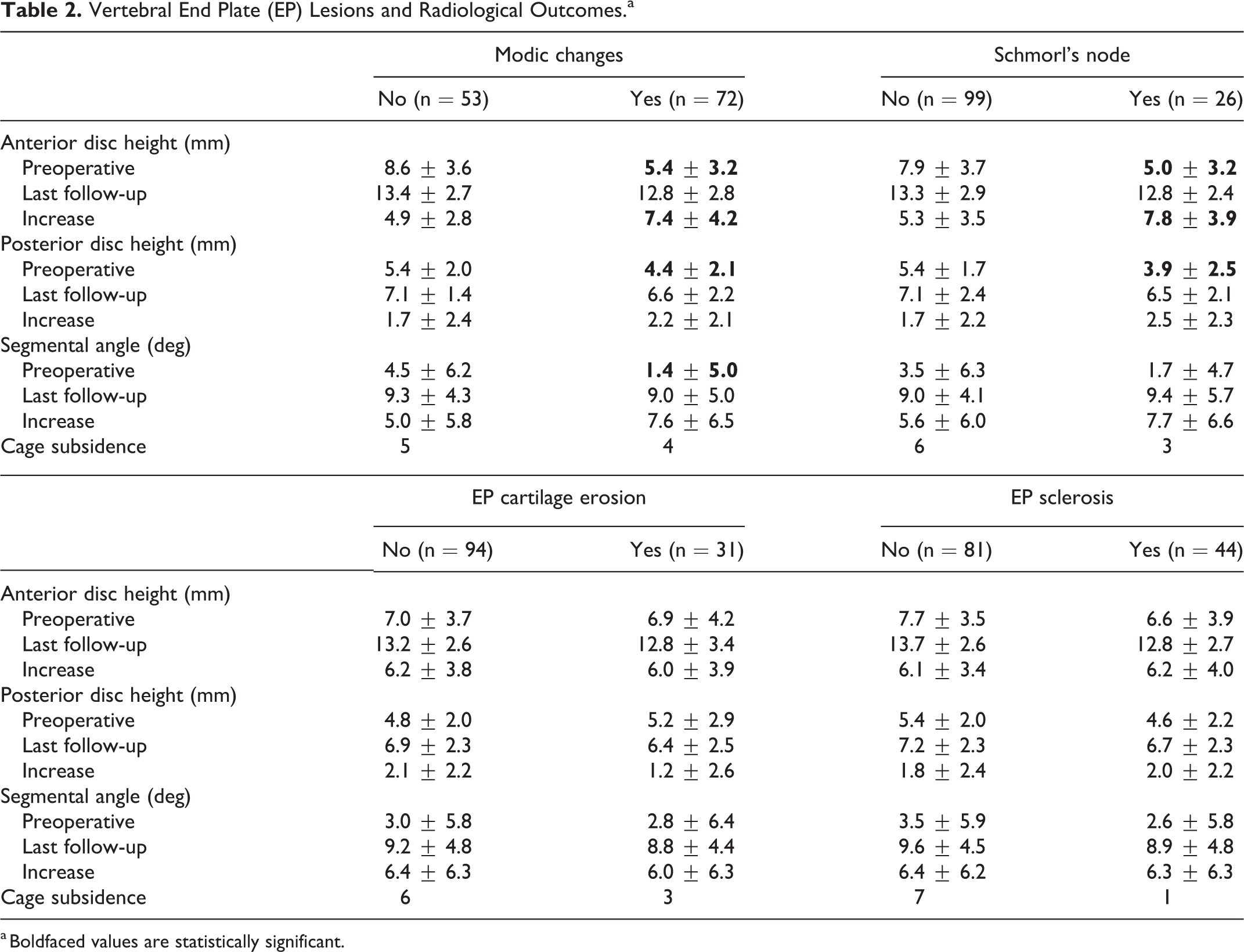
a Boldfaced values are statistically significant.
Intra- and Interobserver Reliabilities for the Interpretation of Vertebral EP Lesions
The intraobserver kappa values for vertebral EP lesions were 0.776 to 0.921 (substantial to excellent agreement), while the interobserver kappa values for the type of EP cartilage were 0.714 to 0.795 (substantial agreement).
Discussion
Lumbar interbody fusion aims to provide segmental stability by solid bone bridging, neural decompression by disc height elevation, and alignment correction by segmental lordosis restoration. To achieve a successful lumbar interbody fusion, the EP cartilage should be clearly removed from the surface without injury to the subchondral trabecular bone. If the subchondral trabecular bone fails to support the compressive load between the intervertebral graft and vertebrae during the graft incorporation, loss of the disc space restoration or graft subsidence/nonunion/failure may occur.
Vertebral EP defect or erosions can affect the stable contact between the intervertebral graft and the subchondral trabecular bone during lumbar interbody fusion. EP Sclerosis may change the microstructure of the subchondral trabecular bone. A recent micro-CT analysis found a drastic loss of rod-like trabeculae and thickening of plate-like trabeculae in the subchondral sclerosis of a knee osteoarthritis model. 17 A molecular study of Modic changes showed an inflammatory dysmyelopoiesis with fibrogenic changes and upregulation of neurotrophic receptors in the bone marrow, 18 which also may change the biology of subchondral trabecular bone.
In the current study, we hypothesized that vertebral EP lesions may lessen the mechanical strength or biological property of the subchondral trabecular bone, and subsequently affect the radiological outcome in lumbar interbody fusion. As expected, the levels with vertebral EP lesions were more degenerated and thus had smaller preoperative radiological parameters. However, most of the radiological parameters at the last follow-up and the cage subsidence rate were not different regardless of vertebral EP lesions as there were more increases at the level with vertebral EP lesions (Table 2). The cage subsidence rates after lateral lumbar interbody fusion were reported as 0 to 17.3%, 19 and our cage subsidence rate was 7.2% (9/125). Although the amount of disc height distraction was known to be a risk factor for cage subsidence, 16 the more increased disc height in vertebral EP lesions of our study did not increase the cage subsidence rate. Therefore, we concluded that vertebral EP lesions are not risk factors for unfavorable radiological outcome in 1- or 2-level OLIF.
The negative results of our study were primarily due to the technical advantage of a lateral cage, which is implanted on the peripheral dense EP rather than on the central weaker portion of the EP (Figure 3). Second, we used autogenous iliac bone graft in all cases; hence, it could promote earlier bone graft incorporation. Third, the bone quantity of our study subjects was favorable; the mean T score of the spine BMD was −1.2 ± 1.2. Finally, we tried to make extreme effort to avoid the vertebral EP injury. Sateke et al 20 reported that the predisposing factors of EP injury were reduced BMD and cage height regardless of the amount of distraction.
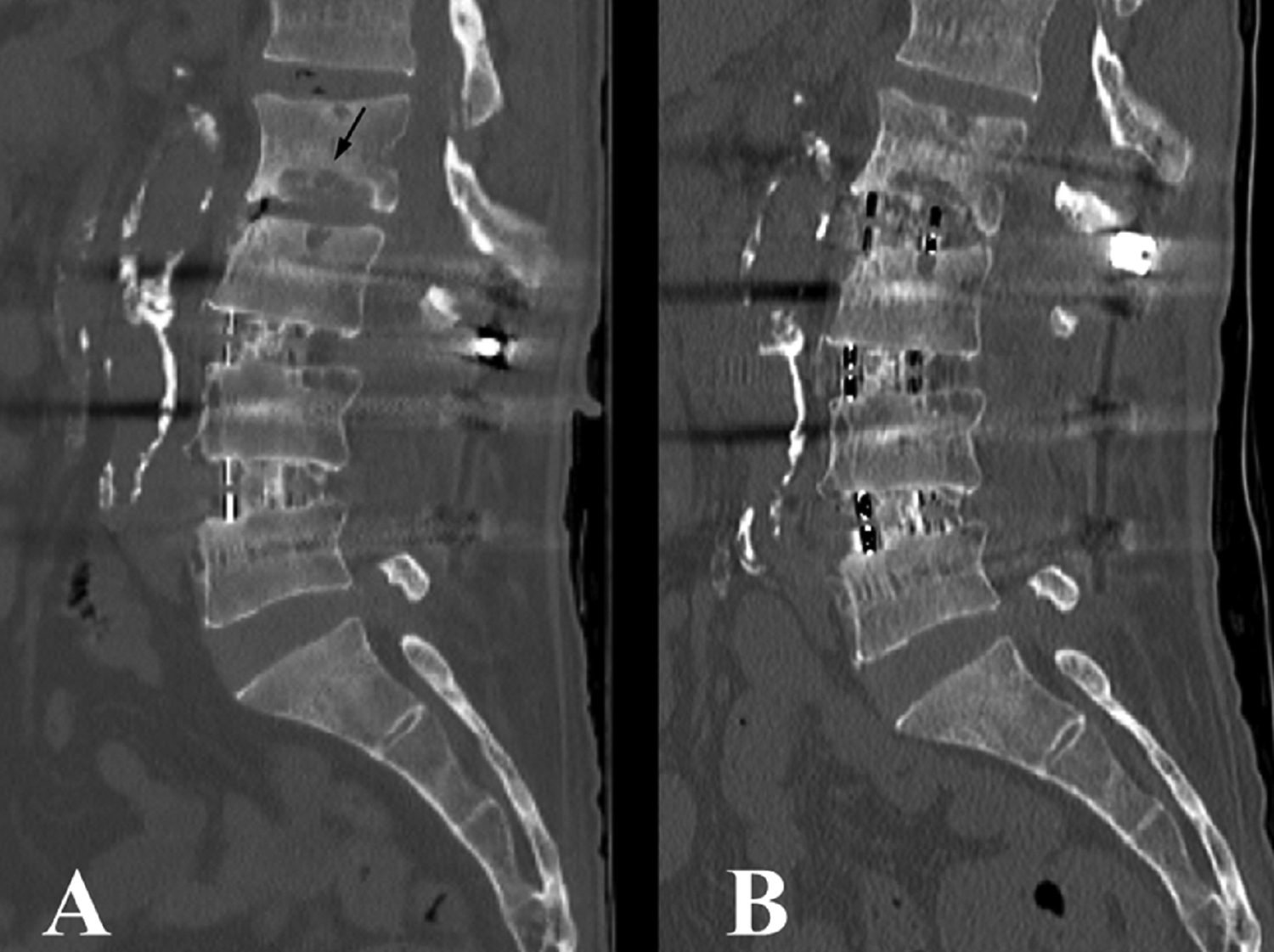
An illustration of oblique lateral interbody fusion (OLIF) case at vertebral end plate (EP) lesion. (A) A 63-year-old male patient presented with adjacent segment pathology at the L2-3 level. He had undergone OLIF at the L3-4-5 levels 3 years before the presentation. Black arrow indicates a huge vertebral EP lesion. (B) Additional OLIF was performed at the L2-3 level. Despite the huge EP lesion, a successful fusion was observed.
The main limitation of our study is the lack of universal MR classification for vertebral EP lesions. Various descriptions of vertebral EP lesions have been reported for the analysis of symptomatic disc degeneration. Modic et al 21 described the signal change of vertebral EP/bone marrow but did not involve the morphology of vertebral EP. Rajasekaran et al 5 reported a classification and scoring system according to the severity of vertebral EP lesions on T1-weighted MR images. Samartzis et al 10 also classified vertebral EP lesions using 6 domains of Schmorl’s node on MR images. Brayda-Bruno et al 8 categorized vertebral EP lesions as wavy/irregular, notched, Schmorl’s node, and fracture based on T2-weighted MR images. In this study, we simply defined 4 types of vertebral EP lesions as Modic changes, Schmorl’s node, EP cartilage erosion, and EP sclerosis. The intra- and interobserver reliabilities of vertebral EP determination in this study were substantial to excellent agreement. However, the small sample size of the type of EP cartilage and other subgroups likely affected the strength of the statistical analysis of the association with the radiological parameters. Second limitation was the lack of analysis among the types of Modic changes. Each type of Modic changes may have different mechanical and biological property of the subchondral trabecular bone and bone marrow. However, subgroup analysis among the types of Modic changes could not be performed due to the small sample size. Third, only OLIF technique was used in this study. OLIF has advantages in that a larger lateral cage can achieve greater restoration of the disc height, indirect decompression, and coronal correction. 22 In addition, the lateral cage can be implanted more securely on the peripheral dense EP instead of the central weaker portions of the EP.23,24 Additional studies with larger samples, long-term follow-up, and other lumbar interbody fusion techniques are warranted to further determine whether vertebral EP lesions can influence the radiological outcomes in lumbar interbody fusion.
Conclusions
In this study, the overall radiological outcome in 1- or 2-level OLIF was not affected by vertebral EP lesions. Careful removal of vertebral EP cartilage and lateral interbody fusion are useful options that can provide favorable radiological outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.