
Abstract
Study Design:
Retrospective cohort study.
Objectives:
Studies in the lumbar spine suggest a correlation between sarcopenia and worse patient outcomes. The purpose of this study was to determine whether paraspinal Goutalier grade of fat degeneration is associated with patient-reported outcomes in patients undergoing anterior cervical discectomy and fusion (ACDF).
Methods:
We performed a retrospective review of a prospective cohort of patients undergoing 1- to 3-level ACDF at a single institution between the years 2011-2014. We utilized preoperative magnetic resonance images to classify patients into Goutalier grades. Patient-reported outcomes, including Neck Disability Index (NDI), RAND score, and EQ-5D score were collected and analyzed according to patients’ Goutalier grade.
Results:
We identified 69 patients for inclusion. A total of 29 patients were classified as Goutalier 0-1 (group 1), 29 were Goutalier 1.5-2 (group 2), and 11 were Goutalier 2.5-4.0 (group 3). All Goutalier groups experienced significant improvement in all 3 outcome scores. Average postoperative NDI scores were 25.3 in group 1, 13.9 in group 2, and 25.1 in group 3 (P = .02). The percentage of patients in each group reporting worse disability after surgery was 17.2%, 3.3%, and 9.1%, respectively (P = .05). No statistically significant difference was seen between groups in postoperative EQ-5D (P = .07) or RAND scores (P > .05).
Conclusions:
The present study is the first to assess the association between cervical paraspinal muscle Goutalier grade and patient-reported outcomes following ACDF. Based on our study, patients with worse cervical paraspinal degeneration may benefit from improved symptom relief in comparison to patients with a lesser degree of degeneration undergoing ACDF.
Introduction
Sarcopenia is the progressive loss of muscle mass and strength and is a manifestation of musculoskeletal frailty. 1,2 Decreased muscle mass has been associated with several detrimental health effects including increased fall risk, osteoporosis, and increased mortality. 3 -5 Furthermore, sarcopenia is an independent marker of overall frailty, 6 and indicates an increased probability of adverse events in the perioperative period. 7 -10 As such, the past decade has witnessed increasing interest in the impact of paraspinal sarcopenia on clinical outcomes following spine surgery.
A number of studies have investigated the relationship between paraspinal sarcopenia and postoperative outcomes following lumbar spine surgery and, considered collectively, suggest a possible correlation between sarcopenia and worse patient outcomes. 11 -17 At present, only 1 study has investigated the relationship between sarcopenia and outcomes following cervical laminoplasty, but this study classified patients as sarcopenic based on appendicular skeletal muscle. 18 Though paraspinal muscle degeneration can be assumed using proxy measurements of peripheral strength such as the timed-up-and-go (TUG) test and hand grip strength, more precise characterization of paraspinal degeneration is quantified by measuring cross-sectional surface area (CSA) and degree of fat infiltration on advanced imaging. 3,11 -14,19 To our knowledge, no studies have investigated whether an association exists between fatty degeneration of the cervical paraspinal musculature and cervical disability in the perioperative period. The purpose of the present study was to determine whether paraspinal Goutalier grade of fat degeneration is associated with patient-reported outcomes in patients undergoing anterior cervical discectomy and fusion (ACDF).
Methods
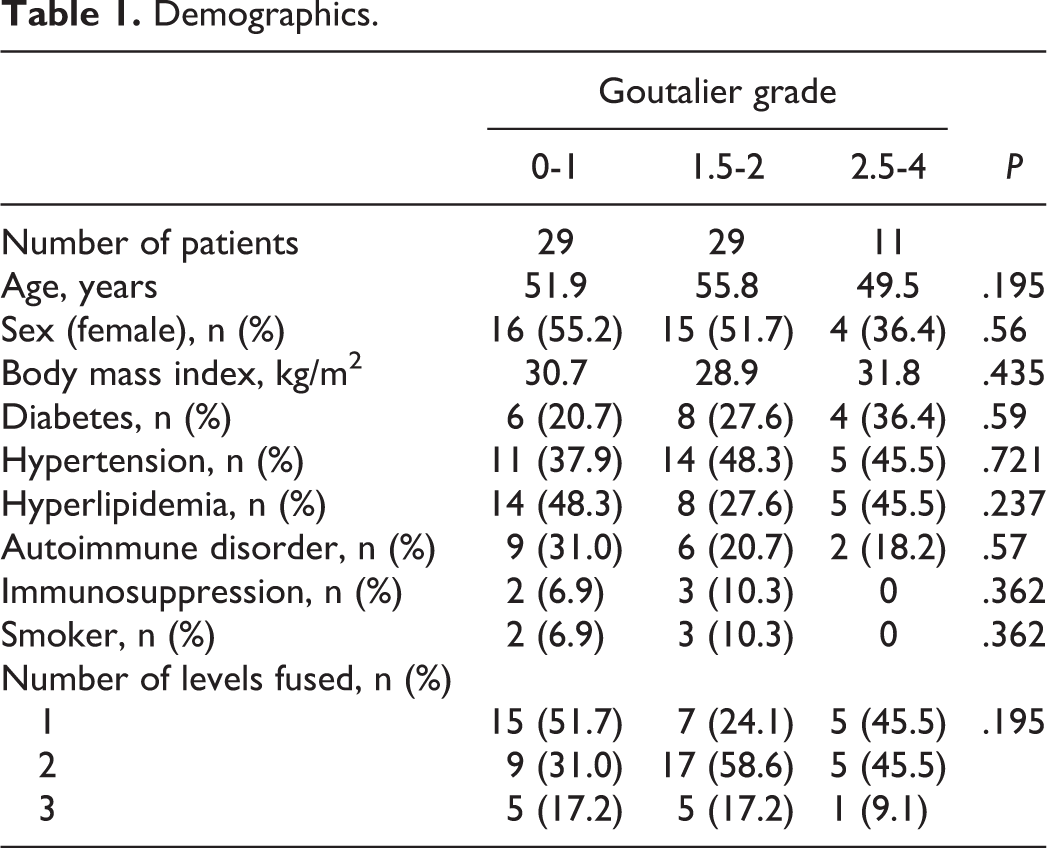
After obtaining approval from the institutional review board, we performed a retrospective review of a prospective cohort of patients undergoing 1- to 3-level ACDF at a single institution between the years 2011 and 2014. Patients were included if they underwent a 1- to 3-level ACDF; had both pre- and postoperative Neck Disability Index (NDI) scores, RAND scores, and EQ-5D scores; underwent preoperative magnetic resonance imaging (MRI) within 6 months prior to the index operation; and authorized use of their medical information for research. We collected demographic information, including age, sex, body mass index, pertinent comorbidities, and number of levels fused (Table 1). Clinical outcome scores were collected both preoperatively and postoperatively at a minimum 1-year follow-up and compared, including NDI, RAND score, and EQ-5D score. Two independent reviewers who were blinded to the clinical outcome scores utilized axial cuts of T2 MRI scans to perform Goutalier classification of the right- and left-sided paraspinal muscle complexes at the C5-6 level in order to capture the muscle belly of the multifidus in mid-course and ensure consistency of measurements (Figure 1). The 2 sides were then averaged for final Goutalier classification. Patients were classified as Goutalier 0 if there were no visible fat streaks in the muscle, Goutalier 1 if there were minimal fatty streaks in the muscle, Goutalier 2 if there was more muscle present than fat, Goutalier 3 if fat and muscle were present in equal quantity, and Goutalier 4 if more fat was present than muscle (Figure 2). We utilized Student’s t test and analysis of variance to compare all means between groups. The mid-P exact test was used to compare proportional differences between groups.
Demographics.
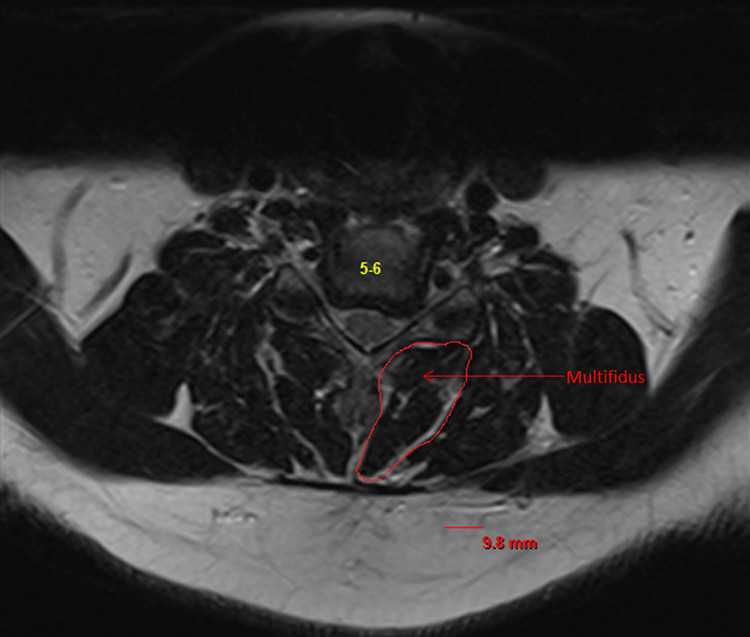
Axial T2 magnetic resonance imaging cut at C5/6 with the multfidus outlined.

Demonstrative axial T2 magnetic resonance imaging cuts at C5/6 (left to right): Goutalier 0, Goutalier 1, Goutalier 2, Goutalier 3, Goutalier 4.
Results
We identified 69 patients for inclusion. The cohort was 50.7% male. A total of 29 patients were classified as goutalier 0-1 (group 1), 29 were Goutalier 1.5-2 (group 2), and 11 were Goutalier 2.5-4.0 (group 3). Determination of Goutalier grade by the 2 reviewers resulted in 82.8% agreement with correlation coefficient of 0.69 (Pearson, r 2 ), demonstrating moderate interrater reliability. For the entire cohort of 69 patients, there was a significant improvement in NDI, RAND, and EQ-5D scores after ACDF (P < .0001). All Goutalier groups experienced significant overall improvement from preoperative to postoperative in all 3 outcome scores, though a subset of patients within each group reported worse outcome scores postoperatively and varying amounts of improvement were seen based on stratification into Goutalier grade (Tables 2, 3, and 4).
Relationship between Goutalier grade and NDI.
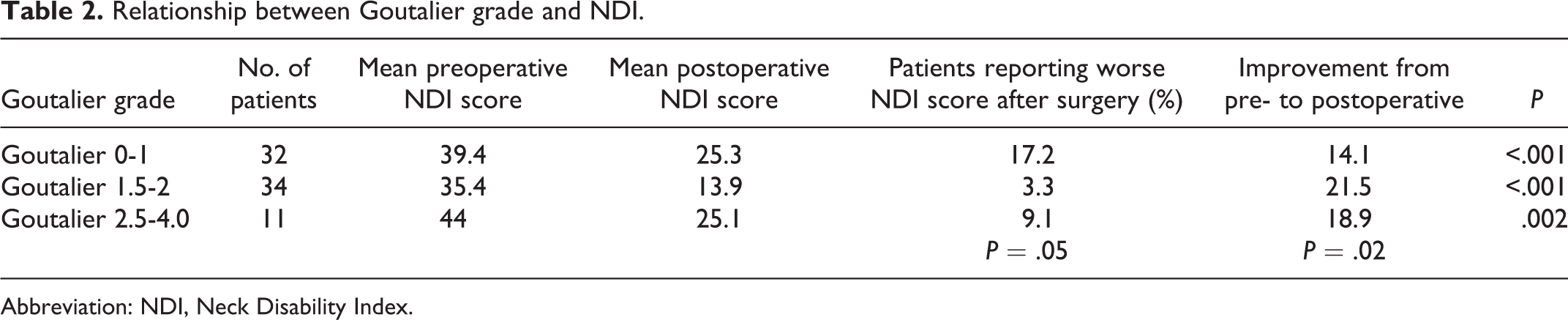
Abbreviation: NDI, Neck Disability Index.
Relationship between Goutalier grade and EQ-5D.

Relationship between Goutalier grade and RAND score.

NDI Scores
Mean preoperative NDI scores were 39.4, 35.4, and 44.0, respectively, which were not statistically significantly different between groups (P > .05). Average postoperative NDI scores were 25.3, 13.9, and 25.1, respectively, which represented a statistically significant difference (P = .02). The percentage of patients in each group reporting worse disability after surgery was 17.2%, 3.3%, and 9.1%, respectively (P = .05) (Table 2).
EQ-5D Scores
Mean preoperative EQ-5D scores were 10.9, 10.8, and 11.6, respectively, which were not statistically significantly different between groups (P > .05). Average postoperative EQ-5D scores were 8.9, 7.3, and 9.2, respectively, which did not represent a statistically significant difference between Goutalier grades (P > .05). The percentage of patients in each group with worse EQ-5D scores after surgery was 20.1%, 6.7%, and 9.1%, respectively (P = .07) (Table 3).
RAND Scores
Mean preoperative RAND scores were 1955.2, 1969.5, and 1991.1, respectively, which were not statistically significantly different between groups (P > .05). Average postoperative RAND scores were 2344.9, 2750.0, and 2371.6, respectively, which did not represent a statistically significant difference between Goutalier grades (P > .05). The percentage of patients in each group with worse RAND scores after surgery was 27.6%, 10.0%, and 27.3%, respectively (P > .05) (Table 4).
Discussion
The present study is the first to investigate whether an association exists between cervical paraspinal degeneration assessed on advanced imaging and patient-reported outcomes following cervical spine surgery. In our cohort, all patients experienced a significant improvement in their NDI, EQ-5D, and RAND scores following ACDF. However, patients with less fatty degeneration of the cervical paraspinal muscles were significantly more likely to experience less improvement in NDI score after ACDF. Furthermore, patients with less paraspinal degeneration were more likely to experience relative worsening of their NDI after surgery than patients with higher Goutalier grade. Though it did not reach the level of statistical significance, patients with less fatty degeneration of the cervical paraspinal muscles also reported relative worsening of their EQ-5D scores from preoperative to postoperative with greater frequency. These results suggest that patients with worse paraspinal degeneration may experience superior symptom relief compared to patients with only mild muscle degeneration undergoing ACDF. It is also important to note that RAND scores were not different between patients based on their Goutalier grade, suggesting that cervical paraspinal degeneration impacts neck disability without a downstream effect on healthy utility and quality of life.
The impact of sarcopenia on thoracolumbar spine biomechanics and clinical outcomes following lumbar spine surgery has been well studied. In a recent biomechanical study, Ignasiak et al 20 demonstrated that severe lumbar paraspinal sarcopenia was associated with substantial increases in compression at the levels of the upper thoracic spine (T1/T2-T5/T6) and shear loading along the whole thoracolumbar spine (T1/T2-L4/L5). A subsequent radiographic study by Ohyama et al 16 found that among patients with spinopelvic mismatch, the subgroup of patients with sarcopenia had a significantly larger sagittal vertebral axis (SVA) (115.7 mm vs 58.7 mm, P < .01) and thoracic kyphosis (TK) (36.6° vs 21.3°, P < .01). Furthermore, sarcopenia was found to be independently related to a significant increase in SVA and TK (P < .01) after adjusting for age. Bokshan et al 11 retrospectively reviewed 55 patients who underwent thoracolumbar spine surgery for a variety of spinal pathologies and found that patients with sarcopenia had a significantly increased length of hospital stay (8.1 vs 4.7 days, P = .02), rate of in-hospital complications (1.2 vs 0.4, P = .02), and need for discharge to a rehabilitation or nursing facility (81.2% vs 43.3%, P = .006). Though other studies have provided contradictory evidence, 13,14 the current literature suggests that sarcopenia both portends a greater likelihood of degenerative spinal pathology and has a negative effect on clinical outcomes following lumbar spine surgery. 21
Though the impact of sarcopenia has been extensively investigated in the lumbar spine, there is a dearth of literature investigating its effect on patient-reported outcomes following cervical spine surgery. In the only clinical study currently published, Koshimizu et al 18 performed a prospective follow-up study of 171 patients who underwent cervical laminoplasty, 48 of whom were diagnosed with sarcopenia based solely on appendicular skeletal muscle mass. They found that patients with sarcopenia had a significantly higher C2-C7 SVA, lower SF-36 (Short Form–36) scores, and lower Japanese Orthopedic Association (JOA) scores at all time points measured. These results are contradicted by the present study, in which we found that patients with severe cervical paraspinal degeneration experienced superior symptom relief to their mildly sarcopenic counterparts undergoing ACDF. One possible explanation for our findings is that patients with more severe cervical paraspinal degeneration have less muscular support of their cervical spine and, therefore, experience greater benefit from the enhanced structural support provided by the interbody and subsequent fusion mass. Alternatively, patients with less sarcopenia may experience more muscular pain following ACDF due to increased disc height and resultant ligamentotaxis. Further biomechanical studies are needed to investigate the relationship between the cervical paraspinal muscles and overall cervical biomechanics.
Our study has a few limitations. First, our study is retrospective in nature. Second, our study includes only 69 patients. Third, there are a disproportionate number of patients in group 2 that underwent multilevel ACDF, raising the possibility that the improvement in patient-reported outcomes in this subset of patients is most influenced by interbody insertion, not cervical sarcopenia. Further studies are needed that are prospective, randomized, and report results at long-term follow-up.
Conclusions
The present study is the first to assess the association between cervical paraspinal muscle Goutalier grade and patient reported outcomes following ACDF. Based on our study, patients with worse cervical paraspinal degeneration may benefit from improved symptom relief in comparison to patients with a lesser degree of degeneration undergoing ACDF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.