
Abstract
Study Design:
Retrospective cohort study
Objectives:
The study aims to evaluate anterior cervical discectomy and fusion (ACDF) in the treatment of patients with ossification of the anterior longitudinal ligament (OALL).
Methods:
We retrospectively reviewed cases performed at our institution between January 2015 and December 2018; adult (age ≥18 years) patients who underwent anterior cervical decompression and fusion in the presence of dysphagia and OALL. Ten patients (9 male, 1 female, mean age 64.4 years) with OALL who underwent ACDF were included. Charts were reviewed for demographics and comorbidities. Primary outcomes assessed were intra- and postoperative complications. Secondary outcomes were fusion rates, instrumentation failure, postsurgical instability/deformity, and readmission rates.
Results:
The average duration of symptoms prior to surgery was 12.3 months. All patients presented with dysphagia (mean Bazaz score 2.0). The average number of levels with OALL was 4.7 (±1.67). All patients underwent ACDF and 3 patients underwent additional posterior cervical fusion for kyphotic deformity correction or when extensive laminectomy was required. We did not encounter any intraoperative complications. Eight patients (72%) had solid fusion demonstrated on the lateral x-rays and no evidence of progressive kyphotic deformity. We did not encounter any instrumentation failure or loosening. Two patients developed recurrence of dysphagia (Bazaz scores 2 and 3 respectively).
Conclusion:
ACDF for OALL with dysphagia and concomitant myelopathy in our small series of 10 patients demonstrate good fusion and clinical outcomes. Larger studies will be necessary to determine the optimal treatment for patients with dysphagia due to OALL.
Introduction
Diffuse idiopathic skeletal hyperostosis (DISH) may present with the development of prominent anterior cervical osteophytes in a majority of patients with degenerative spine disease. DISH, a condition, which was first described as senile ankylosing hyperostosis by Forestier in 1950, is characterized by ossification of entheses and spinal ligaments. It was then referred to as Forestier’s disease until Resnick et al. coined the term diffuse idiopathic skeletal hyperostosis. 1,2 The diagnosis of DISH is established when soft tissues of the anterolateral spine are ossified over at least four contiguous segments, with relative preservation of the height of the intervertebral disc in the affected areas and without obvious signs of intervertebral or apophyseal degenerative changes. 3 Ossification of thoracic and lumbar spinal longitudinal ligaments may lead to a variety of sequelae, including myelopathy, radiculopathy, and unstable fractures after low-energy trauma. 1,2,4 In the cervical spine, DISH might be accompanied by large ossifications of the anterior longitudinal ligament (OALL), which is associated with the formation of anterior cervical osteophytes. Although most cases of OALL are asymptomatic, when symptoms do occur, they are typically caused by ventral displacement of the pharynx, larynx, trachea, and esophagus. Again it is important to note that OALL is the spinal form of DISH. The most common symptoms of OALL are dysphagia, dyspnea, dysphonia, foreign body sensation, hoarseness, stridor, spinal rigidity of variable degrees, acute or chronic cervical pain and also neurologic signs due to medullar compression. 5 However, because many physicians are not familiar with the clinical or radiologic features of DISH, the causal relationship between dysphagia and/or airway obstruction caused by anterior osteophytes and DISH may pass unnoticed. Management of those ossifications is tailored to the degree of symptoms. Treatment options range from conservative measures including dietary modifications and pain medications to surgical resection. 5,6
The aim of the present study is to evaluate anterior cervical discectomy and fusion (ACDF) in the treatment of patients with DISH and resulting OALL and myelopathy/radiculopathy. Primary outcomes are intra- and postoperative complications. Secondary outcomes are fusion rates, instrumentation failure, postsurgical instability/deformity and readmission rates.
Methods
This study is a retrospective chart review from a database of all spine Between January 2015 and December 2018 who were treated for OALL. Inclusion criteria were (1) presence of OALL seen on imaging of the cervical spine, (2) Resnick’s diagnostic criteria met for DISH, (3) presence of dysphagia, and (4) presence of myelopathy or radiculopathy. 7 Of the 24 patients who had OALL, 10 patients met inclusion criteria.
Clinical characteristics were collected, including complaints of dysphagia, respiratory symptoms and neurological deficits. The grade of dysphagia was assessed using the Bazaz dysphagia score. 8 Surgical characteristics including surgical approach, levels addressed, blood loss, and complications were collected. Preoperative computed tomography (CT) scans of the cervical spine were assessed, including the levels affected, the level with the most severe OALL, thickness of the OALL, and kyphosis, which was measured using the Cobb method. 9 We classified the OALL according to Song et al 10 using axial CT scans and lateral x rays using the classification according to Mizuno et al. 11 Postoperative cervical x-rays were examined for fusion and recurrence of OALL. Our institutional review board did not require any approval for retrospective chart reviews. The study has been performed according to the Declaration of Helsinki.
Results
Ten patients met the inclusion criteria, which included 9 (90%) males and 1 (10%) females with mean age of 64.4 years (±10.54) (Tables 1 and 2) and mean follow-up of 11.7 months. One patient was out of network and did not follow up with our clinic. The average body mass index was 30.0 kg/m2 (±6.85) and 8 patients (80%) suffered from diabetes mellitus. The average duration of symptoms prior to surgery was 12.3 months. All patients in our cohort presented with dysphagia (mean Bazaz score is 2.0), four (36.4%) of whom additionally complained of hoarseness and 1 patient who suffered from breathing difficulty. Several patients experienced detrimental effects from the dysphagia including 1 patient with weight loss and another who required had gastrostomy placement for nutrition. Two patients experienced recurrent aspiration pneumonia due to dysphagia. Additionally, 10 patients presented with myelopathy.
Clinical and Radiographic Findings.
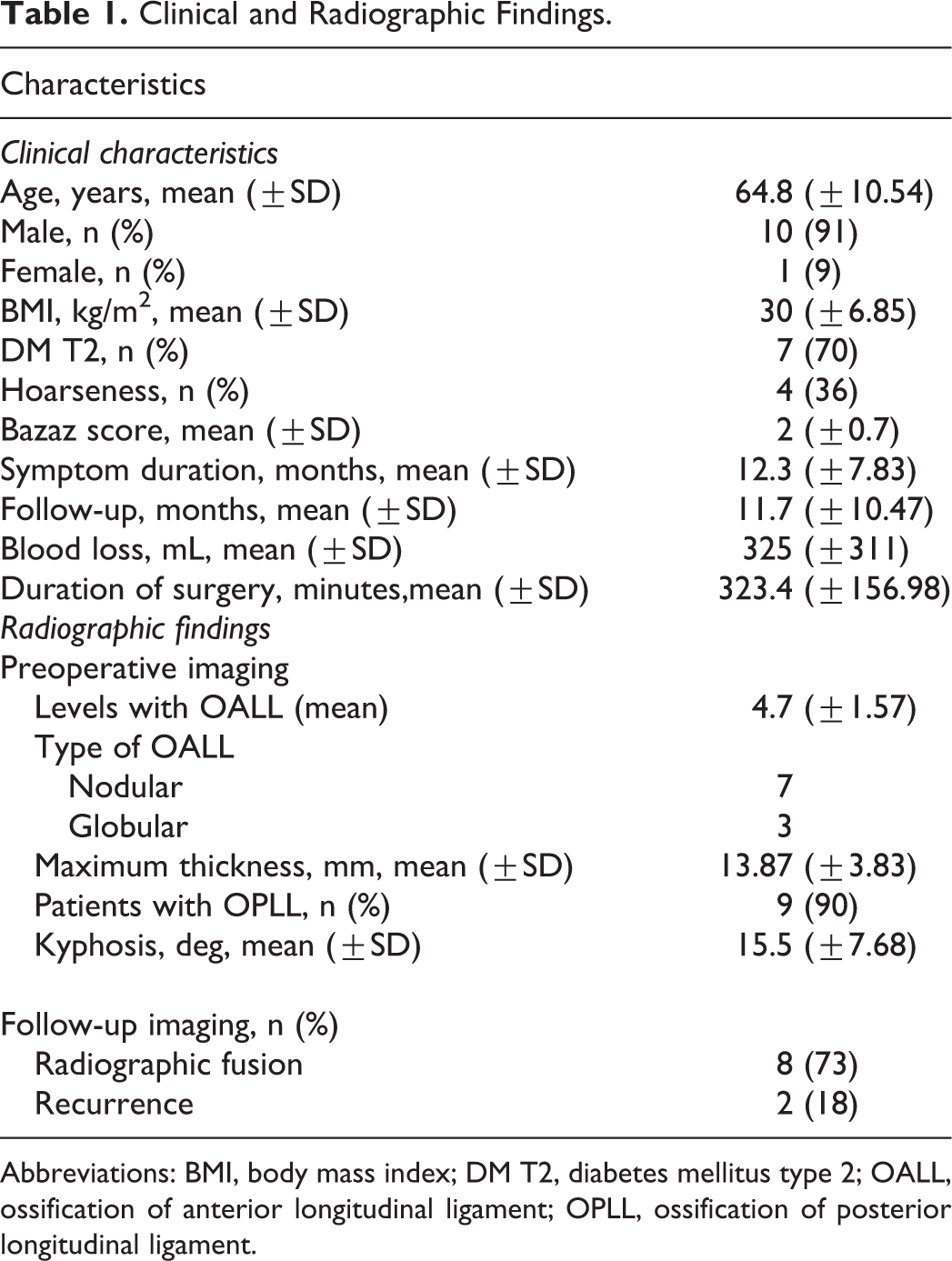
Abbreviations: BMI, body mass index; DM T2, diabetes mellitus type 2; OALL, ossification of anterior longitudinal ligament; OPLL, ossification of posterior longitudinal ligament.
Clinical and Radiographic Characteristics.
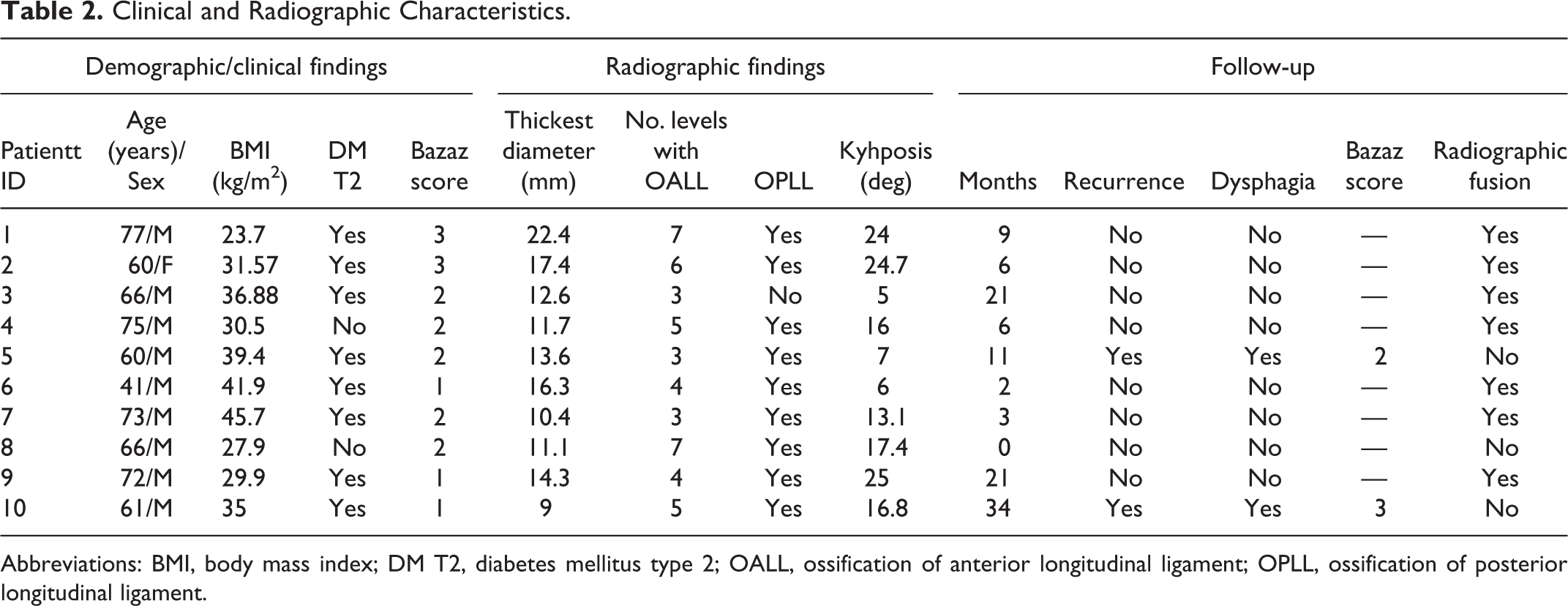
Abbreviations: BMI, body mass index; DM T2, diabetes mellitus type 2; OALL, ossification of anterior longitudinal ligament; OPLL, ossification of posterior longitudinal ligament.
The average number of levels with OALL was 4.7 (±1.67). On examination of the lateral films, the segmental type was most common, while on axial CT the nodular type was most frequently seen. The most prominent level of ossification was in the subaxial cervical spine in all cases, with C4/C5 being the most common level. The average maximal thickness of OALL was 13.87 mm (±3.83). Nine patients had concomitant ossification of the posterior longitudinal ligament (OPLL; Tables 1 and 2).
Ten patients underwent total resection of the anterior cervical osteophytes while 1 patient underwent limited resection of the OALL. All patients underwent ACDF and 3 patients underwent additional posterior cervical fusion for kyphotic deformity correction or when extensive laminectomy was required (Table 3). The average number of levels fused from anterior approach was two levels. One patient underwent a C6 corpectomy and 3 other patients underwent partial vertebrectomies for large ossifications (Table 3). The average estimated blood loss was 325 mL. We did not encounter any intraoperative complications.
Details of Surgery Performed.
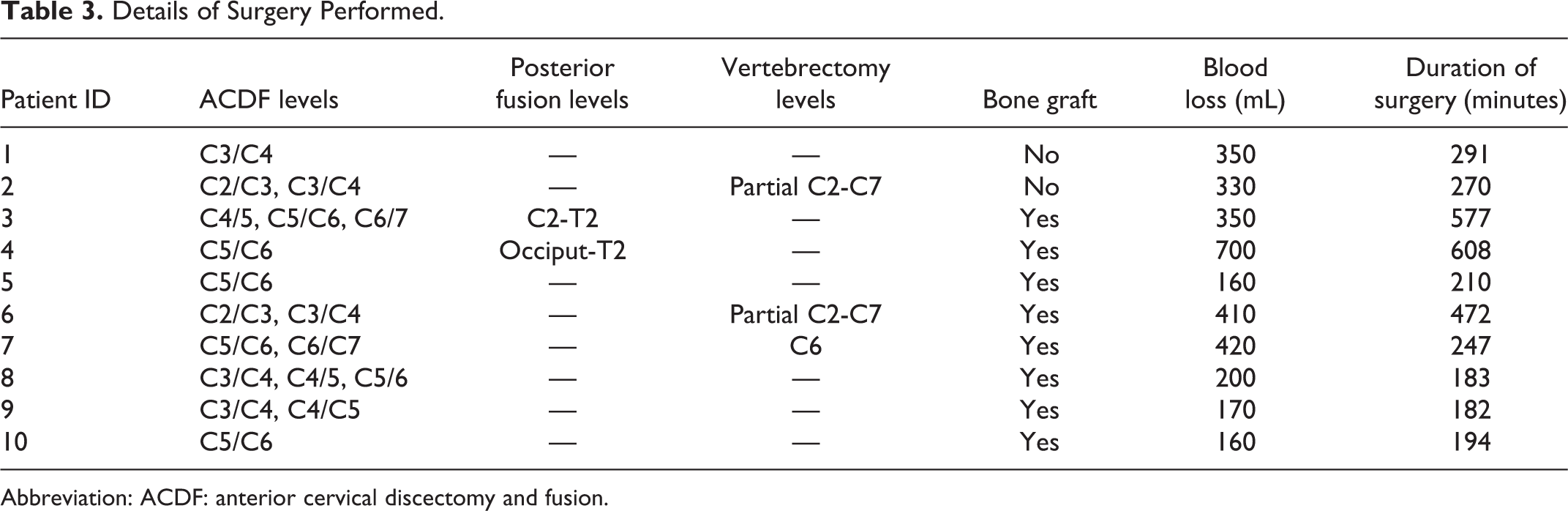
Abbreviation: ACDF: anterior cervical discectomy and fusion.
One patient was readmitted and underwent revision surgery for a cervical pseudomeningocele. Eight patients (72%) had solid fusion noted in the lateral radiographs and there was no evidence of progressive kyphotic deformity. We did not encounter any instrumentation failure or loosening. At the final follow-up, the radiographic examinations showed 2 cases with pathological regrowth, which both reported recurrence of dysphagia (Bazaz scores 2 and 3, respectively) (Table 2).
Preoperative CT cervical spine with sagittal (left) and axial (right) (Figure 1) views of patient X with OALL spanning from C2 to superior portion of C6, with a prominent osteophyte at C3/C4. Figure 2 shows impaired swallowing on barium swallow study in patient X. Furthermore, postoperative anterior/posterior and lateral films of the cervical spine after patient X underwent C3-C4 ACDF and osteophyte resection can be seen in Figure 3. Finally, pre- and postoperative lateral films of the cervical spine after patient 3 underwent resection of osteophytes and C4-C7 ACDF and posterior cervical decompression and fusion C2-T2 is demonstrated in Figure 4.
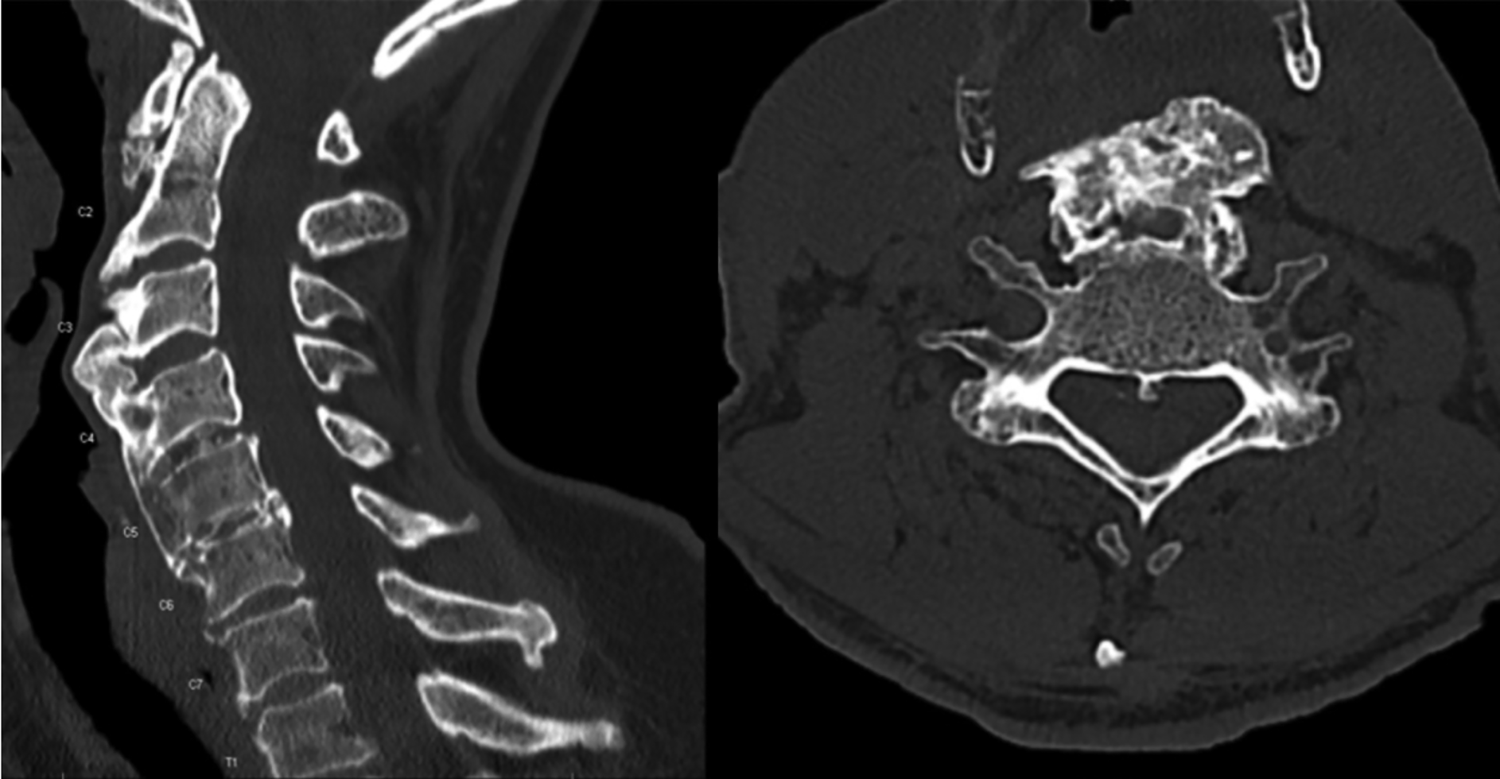
Patient 1: Computed tomography (CT) cervical spine, sagittal (left) and axial views. Ossification of the anterior longitudinal ligament (OALL) spanning from C2 to superior portion of C6, with a prominent osteophyte at C3/C4.

Patient 1: Barium swallow study showing impaired swallowing at level of C3-C4.
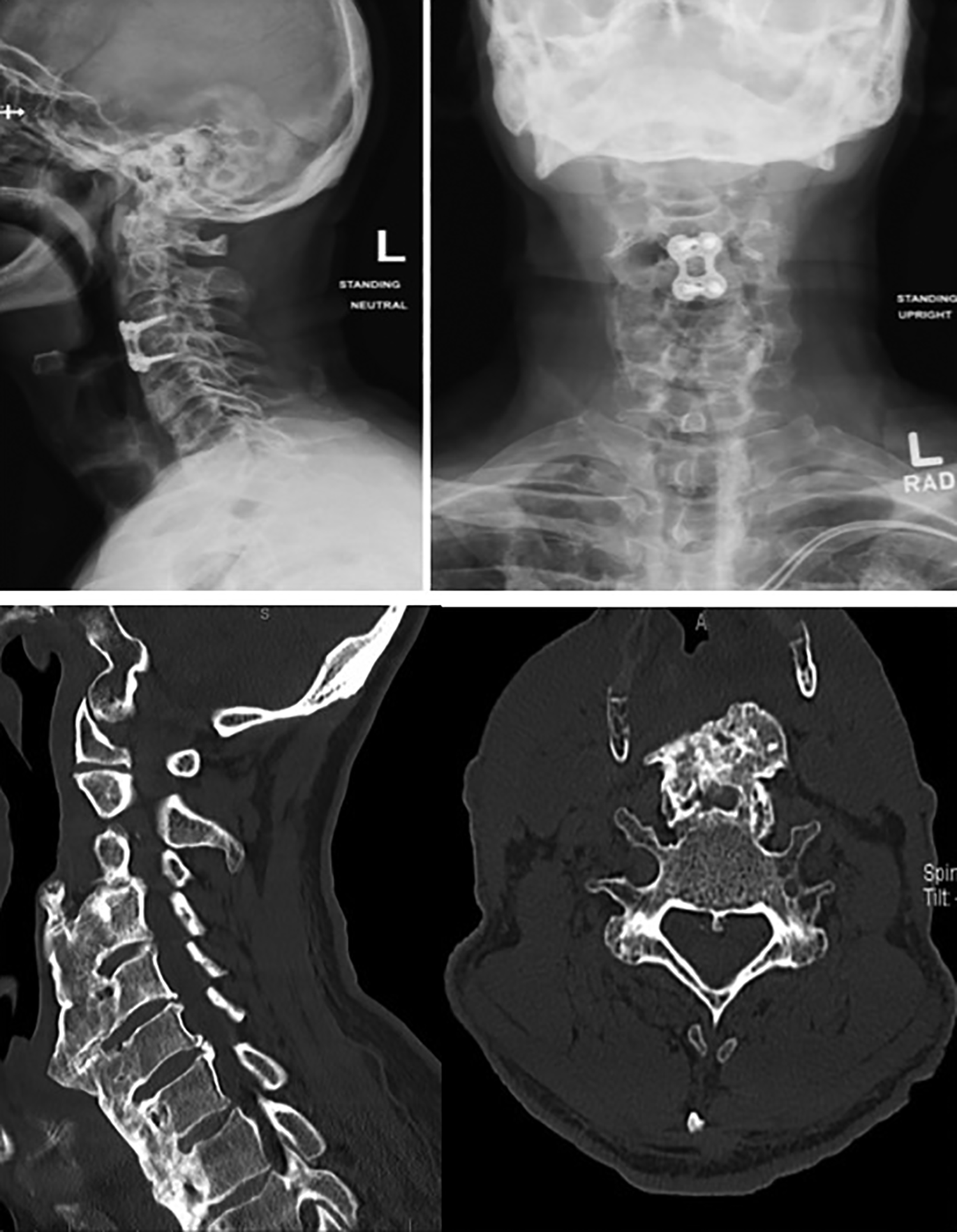
Patient 1: Lateral and anterior/posterior upright cervical X-ray after resection of OALL and C3/C4 ACDF. Preoperative computed tomography (CT; sagittal and axial views) of patient X with ossification of the anterior longitudinal ligament (OALL) (bottom).

Pre- and postoperative lateral cervical radiographs of patient 3 with ossification of the anterior longitudinal ligament (OALL) after resection of osteophytes and anterior cervical discectomy and fusion (ACDF) C4-C7 with posterior cervical decompression and fusion C2-T2.
Discussion
Symptomatic OALL of the cervical spine is uncommon, and the management remains controversial. 11,12 Less than 10% of patients experience dysphagia that is severe enough to require surgery. 13 To our knowledge, this is the largest cohort of patients undergoing ACDF for symptomatic OALL with myelopathy. In our cohort, we had minimal complications, with no intraoperative complications and only 1 patient who required revision surgery. Additionally, we had a reasonable fusion rate (80%).
The average age seen in our cohort (64.8 years) was similar to those previously reported (68.9 years). 5 While previous studies have reported a male predominance ranging from 2:1 to 6:1 male to female ratio, the male predominance was more pronounced in the present cohort (9:1 males: females). 3,5 As expected, there was a high incidence of diabetes mellitus (70%) and high mean body mass index (30.0 kg/m2), both of which are risk factors for development and progression of DISH. We found that maximal thickness was most commonly found at the C4/C5 level, which is consistent with previous literature. This may be explained by the anatomical relationship of this level to the esophagus. 13
The clinical symptoms from DISH are caused by altered skeletal biomechanics, which lead to a decreased range of motion and painful stiffness of the axial and peripheral locomotor apparatus. 4 Several previous case series in which patients with OALL were treated with resection of the osteophyte without fusion. However, the patients in both Miyamoto et al 14 (7 patients) and Mattioli et al 6 (21 patients) had chief complaints of dysphagia without neurological deficits. This is in contrast to our cohort in which, as determined by our inclusion criteria, all patients presented with neurologic deficits in addition to dysphagia. The neurological deficits in our cohort were largely due to OPLL which was present in the majority of the patients (90%). Our cohort was unique to prior studies in that patients had kyphotic deformity and spondylosis causing myelopathy, and therefore fusion was performed in addition to resection of the osteophytes. Due to the predominance of OALL and presenting symptoms of neurological deficits such as myelopathy in our cohort, surgical resection of the anterior cervical osteophytes alone has the potential to create further instability, this may be avoided with an ACDF—our preferred surgical treatment. In addition to ACDF, three of the patients underwent posterior laminectomy and fusion when further deformity correction was required (Figure 4). We found in our cohort the blood loss of the ACDF (range 160-700 mL) which includes the cases that required a posterior cervical surgery for kyphotic deformity correction and stabilization. The operative time was recorded (range 182-608 minutes) for the surgical procedures in our clinical cohort. The trend of increased blood loss and greater length of time of the procedure was related to patients who underwent both ACDF and posterior cervical fusion.
Nevertheless, in our cohort our complication rate (1 revision for pseudomeningocele, 9%) was comparable to rates reported for less invasive osteophyte resection (0%-14%). 6,11,14 Additionally, although previous series have reported 57.1% tracheostomy for postoperative swelling and bleeding, none of our patients required tracheostomy postoperatively. 6
One patient who had a single level ACDF at C5/C6 with subtotal resection of the OALL developed a kyphotic deformity at C4/C5. The patient was autofused from C2-C6 and C6-C7. When the C5/C6 osteophyte was resected, a lever arm was created with motion stress focused at C5-C6. This phenomenon is similar to that occurring in adjacent segment disease in that the level adjacent to the previously fused segments degenerates. 15 In our cohort the kyphotic deformity did not have any clinical significance and the patient declined any further surgery in order to prevent a progression of the deformity.
We had an OALL recurrence rate of 20%. One patient underwent a single level C5/C6 ACDF with a zero-profile spacer for OALL, cervical myelopathy, and dysphagia. They continued to have persistent dysphagia postprocedure (Table 2, Figure 5). OALL recurrence occurred due to large anterior osteophytes that was not addressed at a higher level during the index surgery. A study by Miyamoto et al 14 reported a regrowth rate of osteophytes of 1 mm per year after the surgical resection alone of 20 segments with OALL in 7 patients with DISH. They found that there was a significantly higher rate of osteophyte recurrence in segments with mobility (P = .0013). 14 Therefore fusion may help prevent recurrence of osteophytes given that instability may be contributing to regrowth. Another case series by Suzuki et al, 16 which included 11 patients with OALL had continued growth of osteophytes at levels with mobility while there was no growth at levels with no motion. Furthermore, in a case series that included 6 patients with DISH with severe dysphagia due to OALL, patients underwent ACDF with complete resolution of symptoms. 17 While in our cohort fusion was indicated for neurological symptoms, it is possible that fusion may also be necessary to prevent recurrence of osteophytes.

Patient 5 underwent C5 – C6 ACDF with zero-profile spacer for ossification of the anterior longitudinal ligament (OALL) and myelopathy and continued to have persistent dysphagia postprocedure. Pre- and postoperative lateral cervical radiographs (left and right respectively).
There is a continued global increase in patients with risk factors for DISH, including obesity, diabetes mellitus, metabolic syndrome, and prolonged life expectancy. Research to better define treatment modalities for OALL and DISH will be increasingly necessary given the expected increase in prevalence of DISH in the coming decades. 18,19
Limitations
Longer follow-up will be necessary to obtain accurate recurrence rates after ACDF for OALL. Recent studies indicate that ossifications may reoccur several years after successful initial surgical resection. 14 While Miyamoto et al 14 describe an average follow-up period of 9 years, 2 patients presented recurrence after 10 respective 11 years postsurgery. Additionally, our sample size was small, and larger studies will be necessary to determine the best mode of treatment for symptomatic OALL of the cervical spine.
Conclusion
ACDF for OALL with dysphagia and concomitant myelopathy in our small series of ten patients demonstrate good fusion and clinical outcomes. Larger studies will be necessary to determine the optimal treatment for patients with dysphagia due to OALL.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.