
Abstract
Study Design:
Observational study.
Objective:
To investigate whether the progression of anterior longitudinal ligament ossification varies by age among patients with diffuse idiopathic skeletal hyperostosis (DISH).
Methods:
Of the patients who underwent computed tomography (CT) of the thoracic to pelvic region at least twice from 2009 to 2018, 191 who underwent CT at an interval of 5 years and 0 months to 5 years and 2 months were enrolled (87 men and 104 women). Sex, age at the time of the first CT scan, the presence/absence of DISH, level of complete vertebral body fusion associated with DISH, and extent of ligament ossification using the modified Mata scoring system were investigated.
Results:
DISHs were detected in 53 (27.7%) of 191 patients. The score of ligament ossification increased over time in 35 (66%) of 53 patients; 93 intervertebral spaces were affected. The percentage of completely fused intervertebral spaces increased by 6.7% from 31.3% to 38.0% over time. The increase in score for all intervertebral spaces in individual patients was significantly greater in the ≤70 years old group (2.7 ± 2.8 points, n = 28) than in the ≥71 years old group (1.2 ± 1.4 points; n = 25; P = .028). The mean age of patients with a recorded score that increased by ≥1 point was 67.4 years and that of patients without any change in the score was 73.3 years (P = .036). Thus, patients with recorded changes in the score were younger.
Conclusion:
During the approximately 5-year period, ossification progressed more in younger patients than in older patients.
Keywords
Introduction
Diffuse idiopathic skeletal hyperostosis (DISH) is a condition characterized by progressive ossification of systemic ligaments. In the spine, spinal ankylosis is caused by ossification of the anterior longitudinal ligament. This disease was first reported in 1950 by Forestier and colleagues and then described as DISH by Resnick et al. 1,2 According to these authors, a diagnosis of DISH is made in cases where (1) there is a presence of flowing ossification along the anterolateral aspects of at least 4 contiguous vertebral bodies, (2) relative preservation of the intervertebral disc height, and (3) the absence of sacroiliac joint ankylosis. 1,2 If spinal ankylosis develops, clinical symptoms such as back pain, restricted range of motion, reduced vital capacity, dysphagia, and airway obstruction arise. 1 -6 Vertebral body fracture can be caused by even minimal injury, with the risk of such fracture reported to be 2 to 5 times higher than in patients without ankylosis. 7 -9 In cases of spinal fracture accompanied by DISH, the spine assumes the form of a long lever arm, resulting in concentration of stress at the fractured site. In such cases, conservative treatment may lead to nonunion and delayed-onset paralysis. 10,11 This has been also reported as a factor responsible for poor outcome of spinal fixation surgery or surgical decomposition, 12 -14 and other diseases of the spine can be affected in various manners, depending on the presence/absence of DISH and the severity of intervertebral body ligament ossification.
The prevalence of DISH among adults in general has been reported to be 2.9% to 27.2%. 10,15 -18 Its high prevalence has been reported particularly among elderly men. Factors reported to be associated with ligament ossification include metabolic factors (eg, diabetes mellitus), 19 -22 genetic factors (eg, COL6A1), 23 endocrine factors (eg, growth hormone), 24 vitamin A, 25 and signal transduction, 26 but the exact etiology remains unclear.
The risk of fracture and degenerative disease can vary depending on the severity of ossification. In cases of vertebral body fracture, the presence/absence of DISH can affect the indications for surgery or the selection of operative procedure, and surgery is sometimes recommended. 7,27 However, details about the timing of onset of ligament ossification or the natural course of ossification are unknown, and few reports about these topics are available. Therefore, the present study aimed to investigate the natural course of ligament ossification and the progression of ossification by age among patients with DISH who underwent computed tomography (CT) of the thoracic to pelvic region at least twice.
Materials and Methods
Study Design and Population
Of 8216 patients who underwent CT of the thoracic to pelvic region at least twice in our hospital from 2009 to 2018 regardless of the underlying disease, 191 patients who underwent CT at an interval of 5 years and 0 months to 5 years and 2 months were enrolled in this study (87 men and 34 women; mean age = 69.4 years; range = 51-88 years). Based on the diagnostic criteria of Resnick et al, 1 the diagnosis of DISH was made in cases where the sagittal and coronal CT images satisfied all the following requirements: (1) presence of osseous bridging anterior or lateral to the vertebral body for 4 or more consecutive vertebral bodies; (2) relatively good preservation of the intervertebral disc space; and (3) sacroiliac joint being free of ankylosis. This study was approved by the institutional review board of the author’s affiliated institutions, and informed, written consent was taken from all patients in the study.
Data Collection and Analysis
First, the 191 patients were divided into the DISH group and non-DISH group, and age at first CT scan and male/female ratio were compared between the groups. Then, the extent of ligament ossification was evaluated in the DISH group using the modified Mata scoring system 28 (Table 1; score 0: ossification is absent; 1: half or less ossification of the intervertebral space height; 2: more than half ossification of the intervertebral height but absence of complete ossification; 3: presence of complete ossification; Figure 1). Scoring of all intervertebral spaces (T1/2 to L5/S) was performed, and the association of changes in the score during the 5 years with age was analyzed.
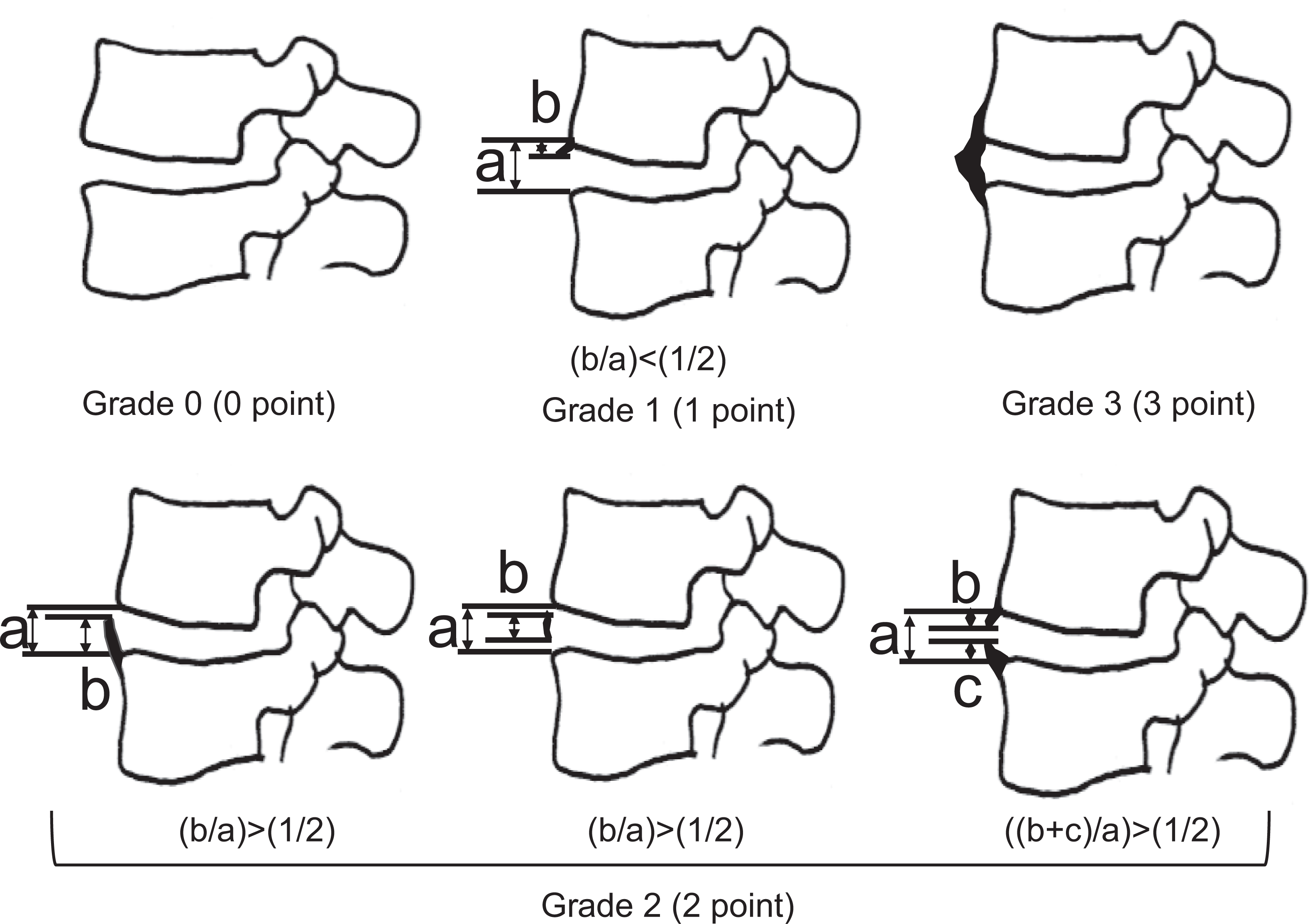
Modified Mata's score. Grade 0 (0 points), absence of ossification in the anterior longitudinal ligament; grade 1 (1 point), total ossification height less than 1/2 of the vertebral body height; grade 2 (2 points), total ossification height 1/2 or more of the vertebral body weight; and grade 3 (3 points), complete ossification of the anterior longitudinal ligament.
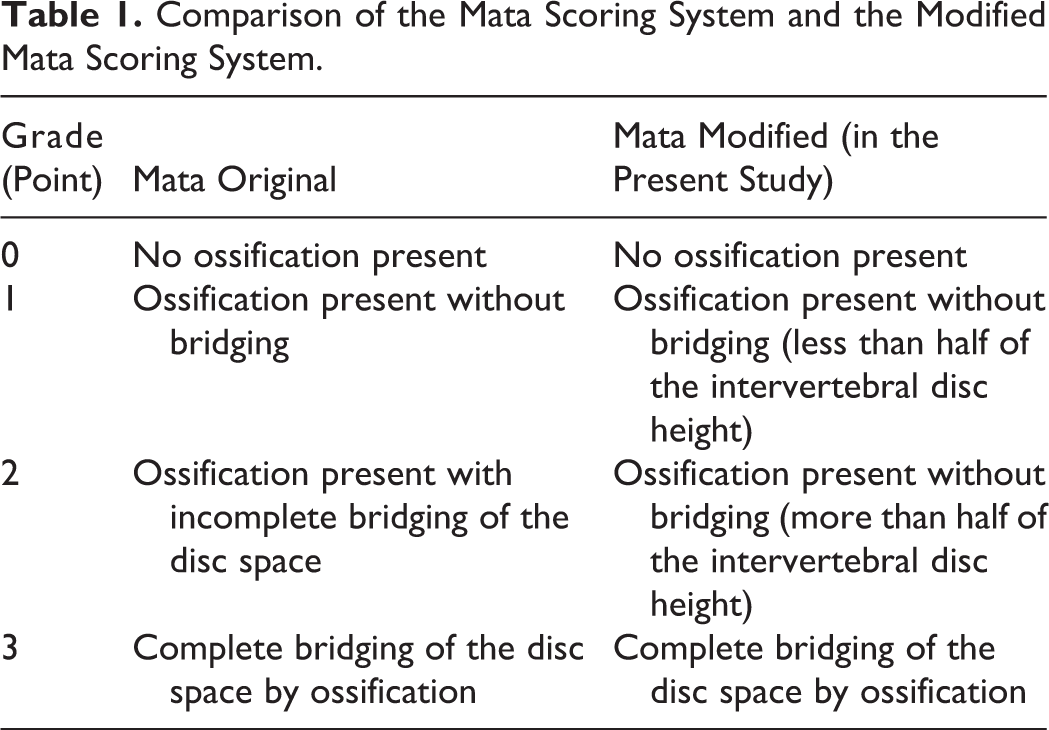
Comparison of the Mata Scoring System and the Modified Mata Scoring System.
Statistical Analysis
For statistical analysis, the χ2 test was used to analyze categorical variables, and the Mann-Whitney U test was used to analyze age. The Spearman correlation coefficient was calculated in analysis of the association of age with increase in the modified Mata score. A P value <.05 was regarded as statistically significant. The software used to perform statistical analyses was JMP version 14.2 for Macintosh (SAS Institute, Inc).
Results
Based on CT findings, 53 (27.7%) of the 191 patients were diagnosed with DISH. The prevalence of patients diagnosed with DISH was significantly higher among men (39.0%, 34/87) than among women (17.4%, 19/104; P = .025). Mean age was significantly higher in the DISH group (69.7 years; 70.0 years for men and 69.1 years for women) than in the non-DISH group (58.7 years; 61.0 years for men and 57.3 for women; P < .001; Table 2).
Number of Cases, Age, and Male/Female Ratio in the DISH and Non-DISH Groups.
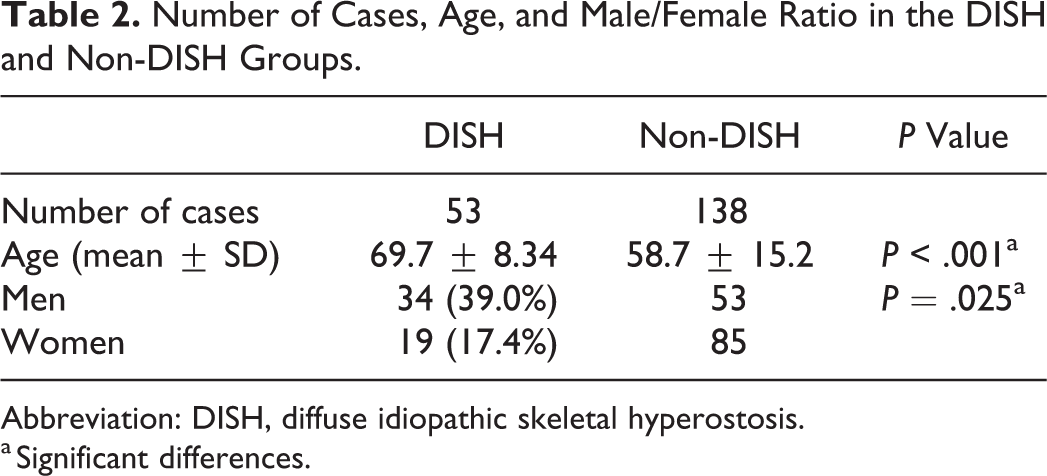
Abbreviation: DISH, diffuse idiopathic skeletal hyperostosis.
a Significant differences.
In analysis of the modified Mata score data, the score increased during the 5-year period in 35 (66%) of 53 patients or 93 (10.3%) of 901 intervertebral spaces, with the magnitude of increase being 0 to 1 in 10 intervertebral spaces, 1 to 2 in 18 spaces, 2 to 3 in 55 spaces, 0 to 2 in 5 spaces, 1 to 3 in 3 spaces, and 0 to 3 in 2 spaces (Figure 2). The percentage of completely fused intervertebral spaces increased by 6.7% from 31.3% (282/901 intervertebral spaces) to 38.0% (342/901 intervertebral spaces; Figure 3). Thus, the mean number of intervertebral spaces that underwent complete ossification during the 5-year period was 1.14 per patient. The total increase in the score for all intervertebral spaces per patient was significantly greater in the ≤70 years old group (2.7 ± 2.8 points) than in the ≥70 years old group (1.2 ± 1.4 points; P = .028; Table 3). The mean age of patients with an increase in the score by 1 point or more was 67.4 years (n = 35), which was significantly lower than that of patients with no change recorded in the score (73.3, n = 18; P = .036; Table 4). A weak negative correlation was noted between age and the increased score (r = −0.325, P = .018; Figure 4).
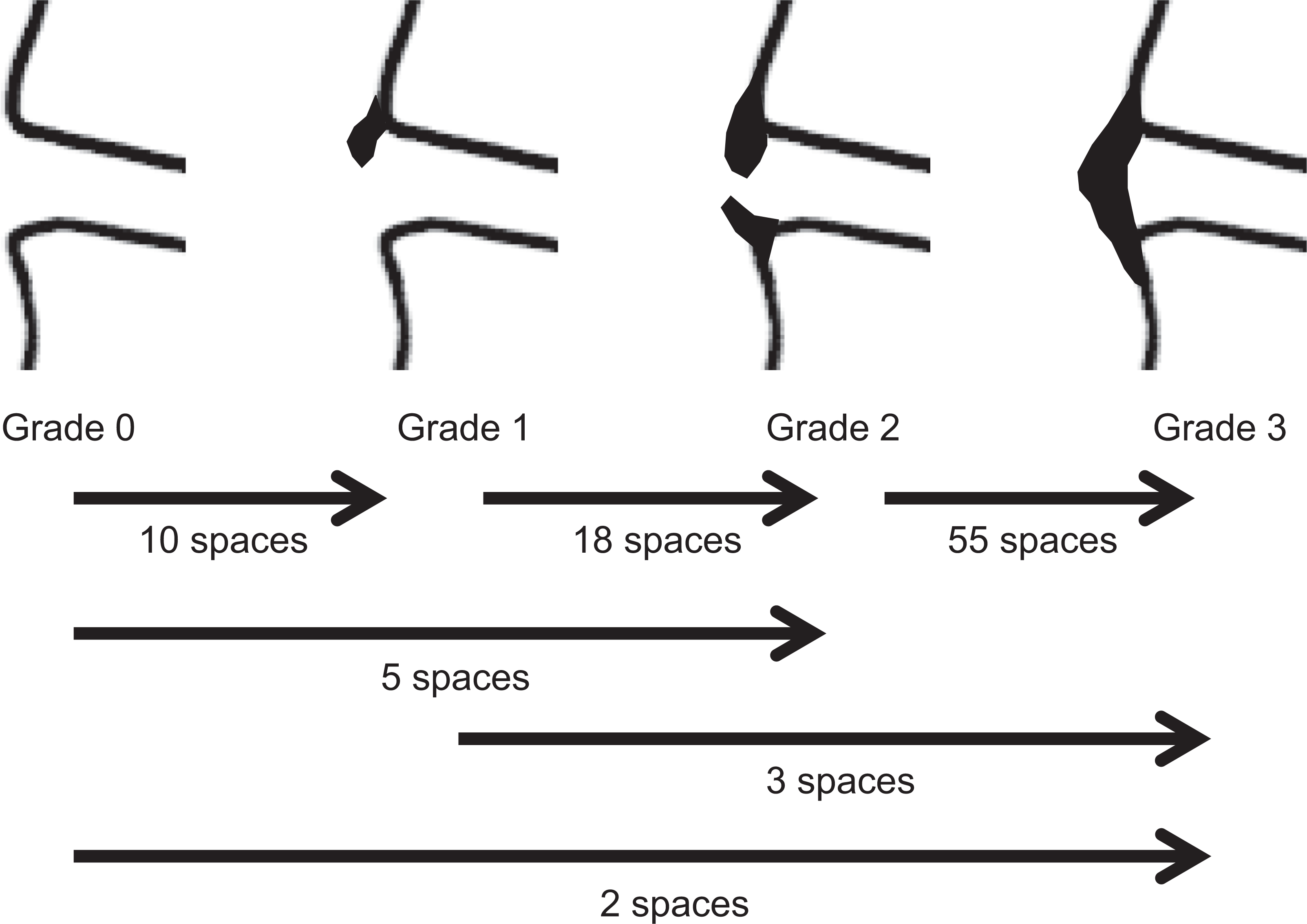
Number of intervertebral spaces showing progression of ossification during the 5-year period. Number of intervertebral spaces showing an increase in the grade of ligament ossification at 5 years after the first computed tomography scan.
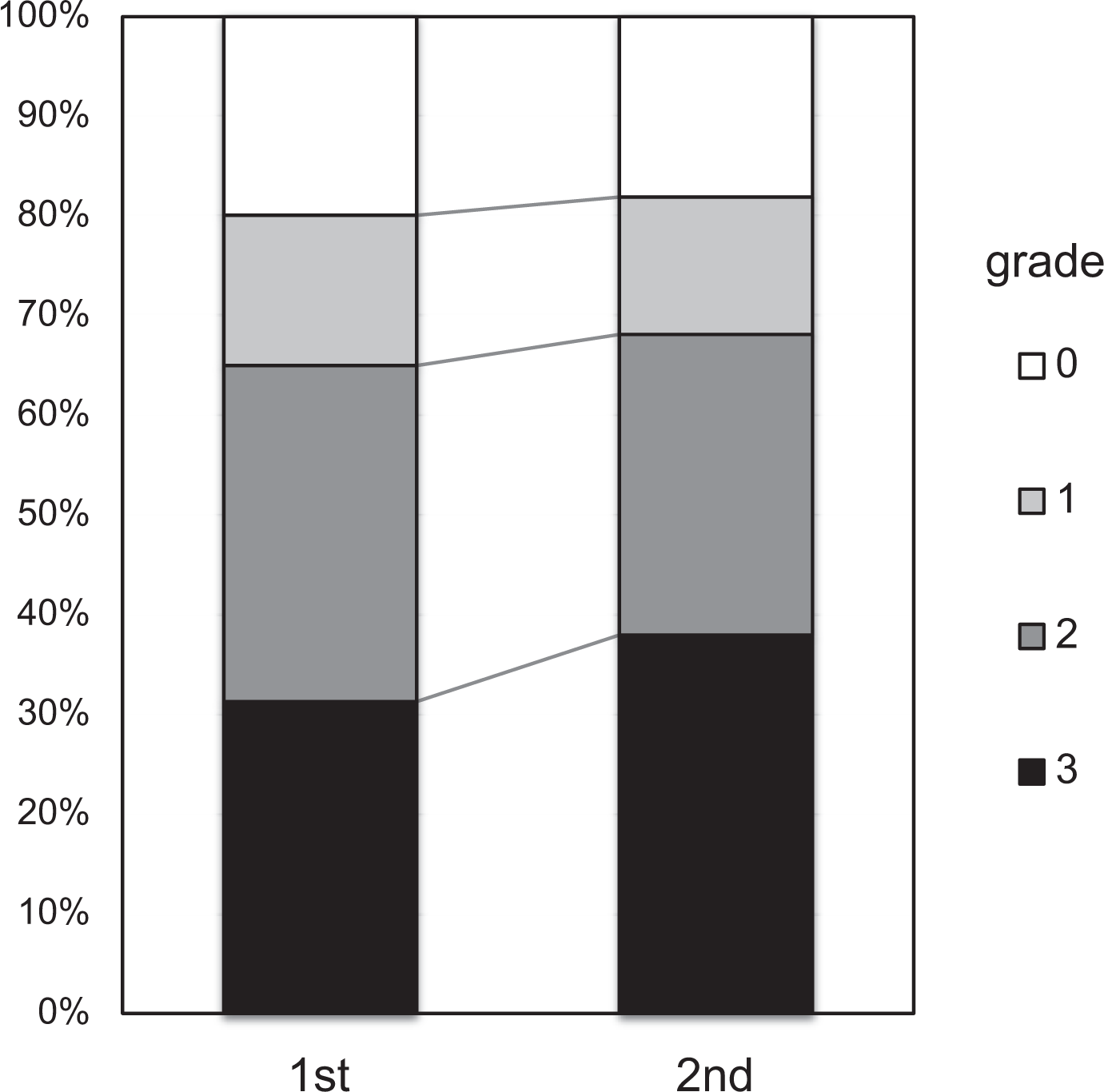
Comparison of the number of intervertebral spaces of each grade between the first computed tomography (CT) scan and the CT scan taken 5 years later. Comparison of the number of each grade between the first and second CT scan. The percentage of grade 3 intervertebral spaces (completely fused) increased by 6.7% from 31.3% to 38.0% during the 5-year period.
Comparison of the Increase in the Modified Mata Score Between the ≤70-Year-Old Group and the ≥70-Year-Old Group.
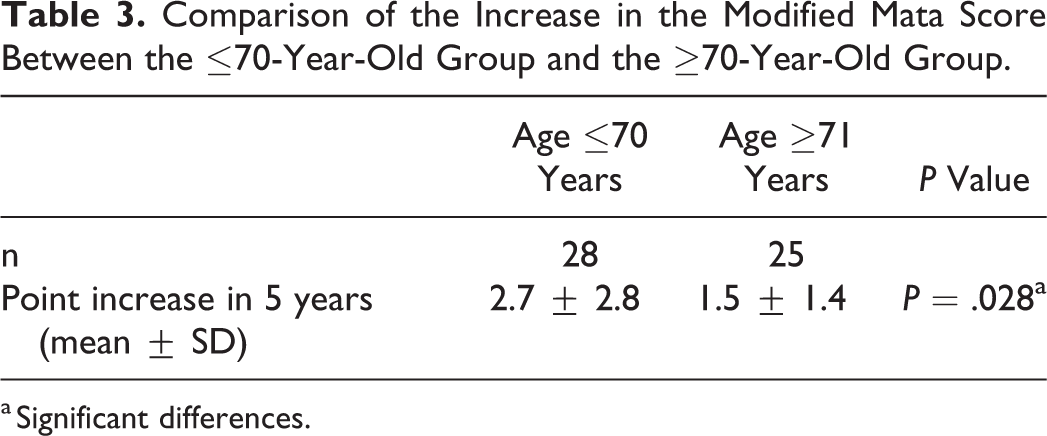
a Significant differences.
Comparison Between the Group Without an Increase in the Modified Mata Score and the Group With an Increase in the Score During the 5-Year Period.
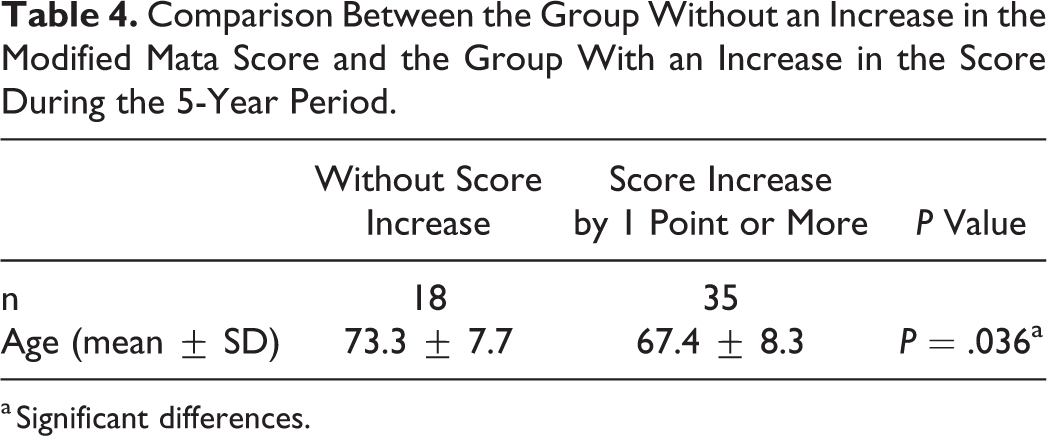
a Significant differences.
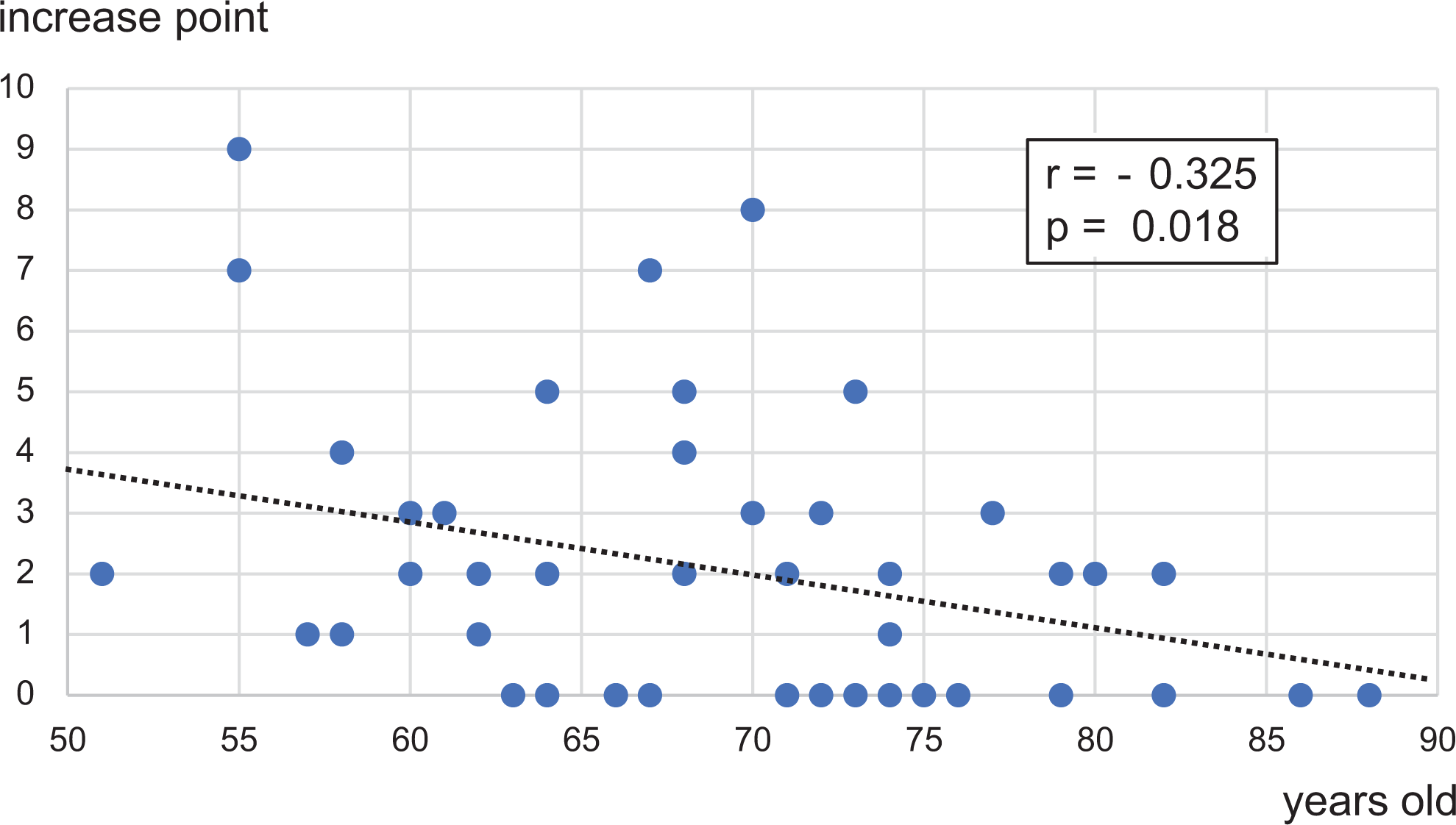
Relationship between age and increase in the modified Mata's score. The increase in score (y-axis) is plotted against age (x-axis). A statistically significant weak negative correlation is seen (r = −0.325, P = .018).
Discussion
This study’s results indicate the possibility that vertebral body ligament ossification in patients with DISH is more progressive in younger patients than in older patients. This is a significant finding, considering that no report on the progression of vertebral body ligament ossification in relation to age has been published before.
The prevalence of DISH among adults in general has been reported to be 2.9% to 27.2%. 10,15 -18 In recent years, the accuracy in diagnosis of this disease has been improved by the use of CT instead of radiography, resulting in an approximately 25% increase in the number of DISH cases reported. 10 -18 The prevalence of DISH increases with advanced age and is associated with sex (male) and complications caused by diabetes mellitus or obesity. 19 -22 However, there are many unresolved questions about the pathophysiology of DISH, and it is unknown how quickly ossification progresses. In the present study, the prevalence of DISH in the population studied was 27.7%, and it was significantly higher in men (39.0%) than in women (17.4%). The mean age of patients was significantly higher in the DISH group (69.7 years) than in the non-DISH group (58.7 years). These results are comparable to the findings in a previous report. 10
Mata et al 28 scored ligament ossification using anteroposterior and lateral radiographs of the cervical, thoracic, and lumbar spinal column; lateral views of both malleoli, heels, and elbows; and anteroposterior views of the pelvis and shoulder in 55 patients with DISH and 35 patients with spondylosis, assigning a score of 0 to cases with no ossification, a score of 1 to cases with ligament ossification but without bridging, a score of 2 to cases with incomplete bridging, and score of 3 to cases with complete ossification (Table 1). They reported that scoring would enable quantitative analysis of the relationship of changes in ligament ossification and diagnostic imaging findings to the clinical features. In the present study, scoring was conducted using the partially modified version of the Mata scoring system. Because the difference between score 1 and 2 was ambiguous in the original Mata scoring system, we modified the scoring system by assigning a score of 1 to cases where the total ossification height was less than half of the intervertebral space height at the anterior edge of the vertebral body and a score of 2 to cases where the total ossification height was half or more of the intervertebral space height at the anterior edge of the vertebral body. We believe that this modified scoring system is more suitable for scoring the extent of ossification.
In the present study, the progression speed of ligament ossification over a period of 5 years was evaluated. The evaluation period was set at 5 years because sufficient reports were available on the extent of ligament ossification progression over a 5-year period. 29,30 A sufficient number of cases was not available from 6 years ago or beyond.
Yanivi et al 29 investigated the natural course of ligament ossification for a mean period of 5.6 years (3-10 years) in 26 patients with DISH. They divided DISH into 6 types depending on the formation of ligament ossification. They reported that it took an average of 1.6 years for the score to increase by 1, although they did not refer to the relationship between the progression of ossification and age. Kuperus et al 30 evaluated ligament ossification based on CT findings in 1367 patients. According to their report, the DISH group (mean age 63.2 years) showed a 10.8% increase in the percentage of completely fused intervertebral spaces—that is, an increase by about 1.3 completely fused intervertebral spaces during the average 5-year period (range 2.5-7.4 years). Thus, the percentage of completely fused intervertebral spaces was slightly higher in the report by Kuperus et al, 30 but it could be deemed as approximately comparable to that in the present study. Furthermore, in our study, the mean age of patients with an increase in the recorded score by at least 1 point was 67.4 years, which was significantly lower than that of patients with no increase in the score (73.3 years). A significant negative correlation was noted between age and score increase. This result suggests that ossification is more progressive in younger patients than in older patients.
The risk of fracture and degenerative disease, indications for surgery, and optimal operative procedure can vary depending on the severity of ossification. Therefore, it seems important to understand factors such as the timing of onset of ligament ossification and its natural course in patients with DISH. In our study, the prevalence of DISH tended to be higher among elderly patients than in younger patients, but ligament ossification was more progressive in younger patients than in elderly patients. Hence, the need for fixation and extent of fixation needed during surgical treatment may vary depending on the individual patient’s age.
The limitations of this study lie in the fact that it did not evaluate ossification of the cervical spine, and the sample size was small. There are still many unresolved questions about the natural course of ossification, and further studies on this topic are needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.