
Abstract
Study Design:
Retrospective cohort study.
Objective:
To provide insight into postoperative complications, short-term quality outcomes, and costs of the surgical approaches of adult cervical deformity (ACD).
Methods:
A national database was queried from 2007 to 2016 to identify patients who underwent cervical fusion for ACD. Patients were stratified by approach type—anterior, posterior, or circumferential. Patients undergoing anterior and posterior approach surgeries were additionally compared using propensity score matching.
Results:
A total of 6575 patients underwent multilevel cervical fusion for ACD correction. Circumferential fusion had the highest postoperative complication rate (46.9% vs posterior: 36.7% vs anterior: 18.5%, P < .0001). Anterior fusion patients more commonly required reoperation compared with posterior fusion patients (P < .0001), and 90-day readmission rate was highest for patients undergoing circumferential fusion (P < .0001). After propensity score matching, the complication rate remained higher in the posterior, as compared to the anterior fusion group (P < .0001). Readmission rate also remained higher in the posterior fusion group; however, anterior fusion patients were more likely to require reoperation. At index hospitalization, posterior fusion led to 1.5× higher costs, and total payments at 90 days were 1.6× higher than their anterior fusion counterparts.
Conclusion:
Patients who undergo posterior fusion for ACD have higher complication rates, readmission rates, and higher cost burden than patients who undergo anterior fusion; however, posterior correction of ACD is associated with a lower rate of reoperation.
Introduction
Adult cervical deformity (ACD) has a diverse etiology, including spondylosis, trauma, and inflammatory arthropathy among others, and typically manifests in the sagittal plane (kyphosis), whereas coronal (scoliotic) deformities are less frequent. ACD is often exacerbated by prior operative destabilization, weakness of the intervertebral discs, and/or posterior tension bands or develops on the grounds of ankylosing spondylitis (AS). Irrespective of the etiology, it is associated with high morbidity rates, and its correction is generally resource intensive. 1 -3
If left untreated, patients with ACD frequently suffer from debilitating pain, poor health-related quality of life, and patients’ risk to progressively lose function in case of associated myelopathy and neurological deficits. Severe forms of ACD, such as chin-on-chest deformities, can even lead to the inability to chew, swallow, or speak. Treatment options for the management of ACD include anterior, posterior, or circumferential approaches, and valuable guidance for choosing each approach based on morphological categories has recently been proposed. 4,5
However, literature addressing cost and quality metrics for each approach is currently limited. The objective of this study was to provide insight into postoperative complications, short-term quality outcomes, and costs of these approaches in an effort to aid the surgical decision making for ACD.
Methods
Ethical Considerations
All data from these databases is de-identified. Therefore, this study is exempt from institutional review board approval of Stanford University School of Medicine in accordance with the Health Insurance Portability and Accountability Act of 1996.
Data Source
The Thomson Reuters MarketScan Commercial Claims and Encounters Database and the Medicare Supplemental and Coordination of Benefits Database (Truven Health Analytics Inc, Ann Arbor, MI) were queried from 2007 to 2015 to identify adult patients who underwent fusion for primary cervical deformity. Both the Commercial Claims and Medicare Supplemental databases capture person-specific clinical utilization, expenditures, and enrolment across inpatient, outpatient, and prescription drug services. Diagnostic and procedural information is available in the form of International Classification of Diseases 9th Revision (ICD-9) and Current Procedural Terminology (CPT) codes.
Inclusion Criteria
Patients who underwent fusion for ACD were identified via use of the ICD-9 codes 737.0-737.9, 738.2, and 738.5. Of the patients who had one of the aforementioned cervical deformity ICD-9 codes, only those who also had a CPT code indicating multilevel cervical arthrodesis listed in Figure 1 were included in this study. Deformity surgery is inherently multilevel; however, given the potential error in administrative coding, the multilevel fusion requirement ensured the precise capture of patients undergoing fusion for deformity and not a nondeformity pathology that would only require a single-level fusion. Patients younger than 18 years of age or who underwent single-level fusions were excluded.
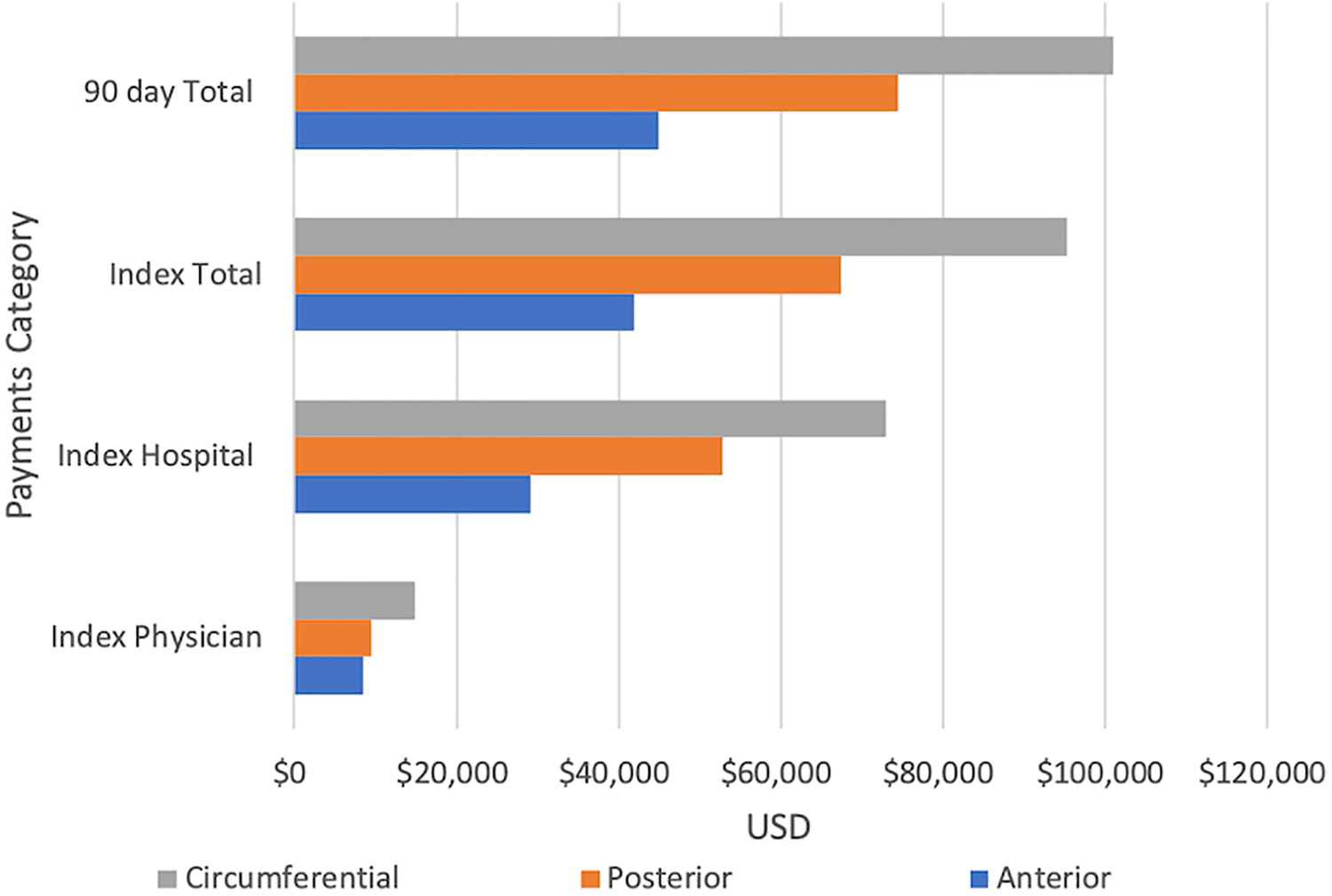
Payments for cervical fusion by type.
Variables and Outcomes
Individual demographic information such as age, sex, and region of admission and comorbidity status such as a history of diabetes, congestive heart failure (CHF), arterial hypertension (aHT), cardiac arrhythmia, myocardial infarction (MI), osteoporosis, and tobacco and alcohol use of each patient was gathered. The Charlson Comorbidity Index (CCI) score was calculated for each patient.
The primary outcome of this study was the presence of a postoperative complication (defined as a complication occurring within 90 days of the index ACD surgery). These included acute posthemorrhagic anemia, delirium, dysrhythmia, surgical site hematoma, wound dehiscence or surgical site infection (SSI), deep vein thrombosis (DVT), and MI. Complications related to the respiratory systems such pulmonary embolism (PE), pneumonia, acute respiratory distress syndrome (ARDS), or other unspecified pulmonary complications were also analyzed. Short-term outcomes, specifically length of stay after the index ACD surgery, readmissions, reoperations (defined as presence a cervical fusion CPT/ICD9 code after index stay), and costs (stratified into physician, hospital, and total payments of the index hospitalization, as well as 90-day total payments) were also considered.
Patient Groups, Propensity Score Matching, and Statistical Analysis
Patients were stratified into 3 groups in this study based on cervical fusion type: anterior, posterior, or circumferential approach. Anterior and posterior cervical fusions have unique CPT codes, and circumferential approach was defined as the presence of both an anterior and posterior CPT codes in the same admission—a methodology used often in the literature. The circumferential cohort also included patients undergoing posterior-anterior-posterior approaches.
To minimize the effect of potential confounding on the direct comparison of patients undergoing an anterior or posterior approach, a propensity-score match (PSM) was utilized. A greedy nearest-neighbor algorithm was employed to match patient cohorts with a 2:1 anterior to posterior ratio. A caliper of 0.01 was utilized in the match, and replacement of patients in the algorithm was not allowed. All baseline demographics and comorbidities (n = 12) were input into the algorithm, leading to the matched covariates having no statistically significant differences.
Two-sample t tests, ANOVA, χ2 tests, or Fisher’s exact tests were used as appropriate. P values were interpreted as significant only after applying the Bonferroni correction for multiple comparisons. Information about the level of significance is provided in each table caption. Statistical analysis was conducted in R Studio, version 1.0.153.
Results
Patient Cohort
A total of 6575 patients met the inclusion criteria of this study, of which 4819 patients (73.3%) had anterior cervical fusion, 1241 (18.8%) had posterior cervical fusion, and 515 (7.8%) had circumferential cervical fusion.
Table 1 contains the baseline demographic data of the 3 study groups. It is evident that study groups differed in particular with respect to age and comorbidity, with patients undergoing posterior cervical fusion being older and presenting with more comorbidities (higher CCI and higher rates of CHF, aHT, diabetes, cardiac arrhythmia) as compared to patients undergoing anterior cervical fusion. Female patients more frequently underwent anterior as opposed to posterior cervical fusion, as did patients treated in Southern and Western US regions (Table 1). Characteristics of patients undergoing circumferential fusions mostly ranged between those undergoing anterior or posterior fusion only with regard to age, sex, and comorbidity (CCI).
Demographics (P Value Threshold 0.05/12 = .004).a
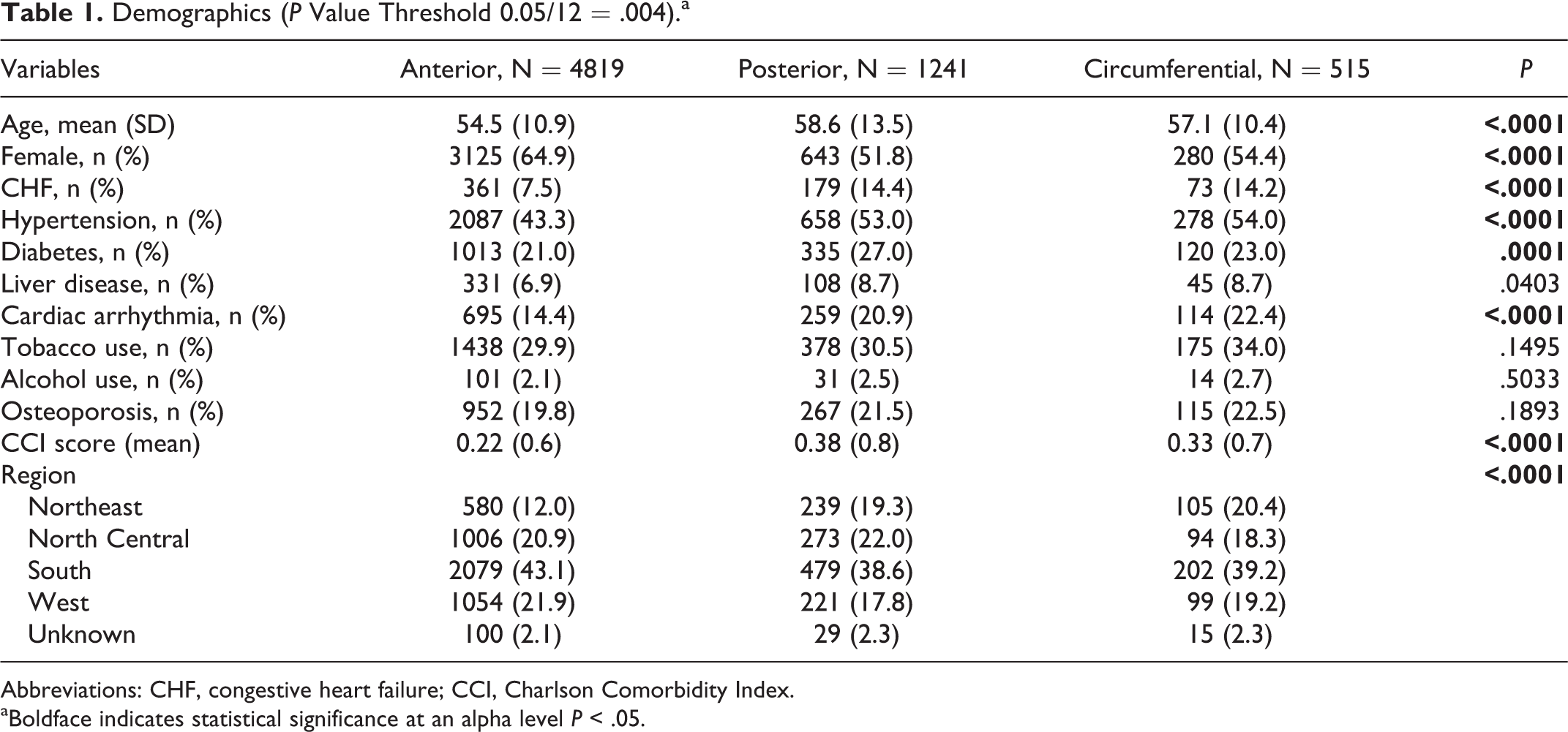
Abbreviations: CHF, congestive heart failure; CCI, Charlson Comorbidity Index.
aBoldface indicates statistical significance at an alpha level P < .05.
Complications
Patients in the circumferential group experienced the highest rates of postoperative complications within 90 days (46.9%) followed by the posterior (36.7%) and anterior groups (18.5%; P < .0001; Table 2). The most frequent postoperative complication types were pulmonary (anterior: 4.5%, posterior: 10.1%, circumferential: 19.8%, P < .0001) and anemia (anterior: 2.9%, posterior: 9.9%, circumferential: 13.3%, P < .0001). In contrast, dysrhythmia rates were highest in the posterior group (1.5% vs anterior at 0.6% and circumferential at 0.4% P = .001), as were surgical site hematomas (3.2% vs anterior at 1.3% and circumferential at 2.3%, P < .0001). PE rates were similar among the posterior (1.7%) and circumferential (1.6%) cohorts, but were significantly lower in the anterior cohort (0.6%; P < .0007). This observation was maintained in rates of wound complications: dehiscence (anterior 0.5%, posterior 3.4%, circumferential 3.3%, P < .0001), SSI (anterior 1.1%, posterior 6.3%, circumferential 5.8%, P < .0001), and other wound complications (anterior 0.3%, posterior 1.7%, circumferential 2.1%, P < .0001). Rates of MI were similar among anterior and posterior groups (1.5% and 1.6%, respectively), but were higher in the circumferential group (3.3%; P = .0014). Rates of ARDS and DVT were similarly low across all 3 groups.
Ninety-Day Complications (P Value Threshold 0.05/14 = .003).a
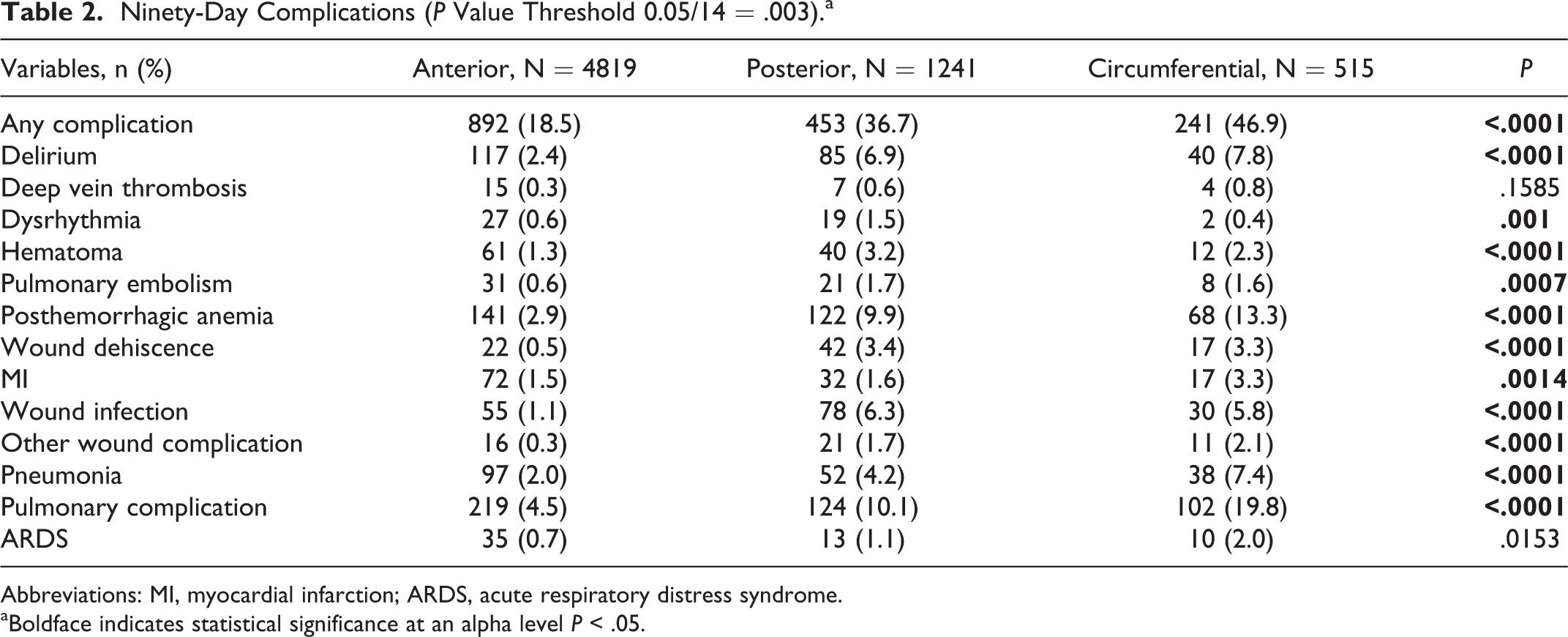
Abbreviations: MI, myocardial infarction; ARDS, acute respiratory distress syndrome.
aBoldface indicates statistical significance at an alpha level P < .05.
Quality Outcomes
Patients who underwent circumferential fusion had the highest mean length of stay (4.9 days), which was similar to the posterior group (4.4 days), but significantly higher than the anterior group (2.1 days; P < .0001; Table 3
Quality Outcomes (P Value Threshold 0.05/5 = .01).a
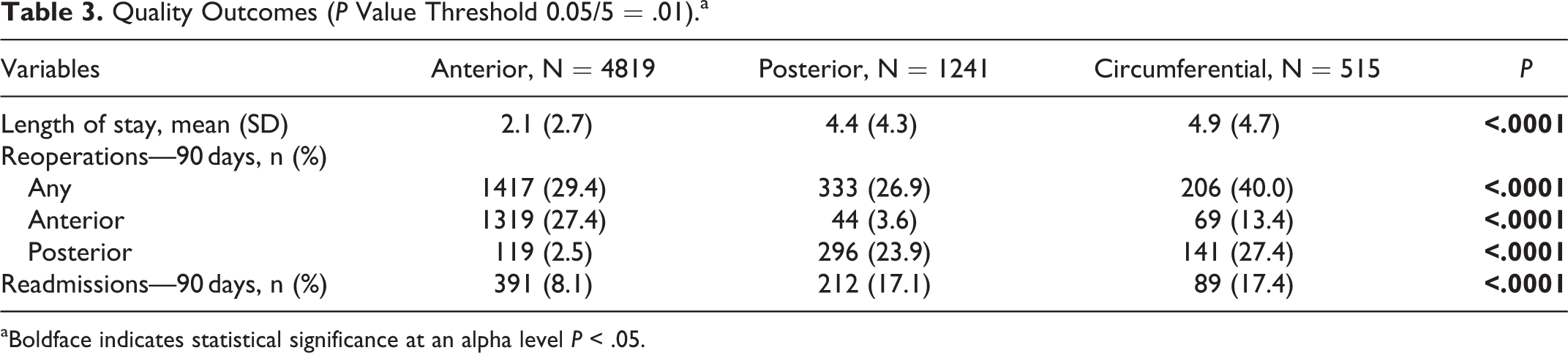
aBoldface indicates statistical significance at an alpha level P < .05.
Readmission rates within 90 days were similar among patients in the circumferential (17.4%) and posterior (17.1%) groups, but lower in patients after anterior fusion (8.1%; P < .0001; Table 3). The 90-day reoperation rate was 40% in the circumferential group, significantly higher than both the anterior (29.4%) and posterior groups (26.9%; P < .0001; Table 3).
Cost of Treatment
The costs were significantly higher in the circumferential group, as compared to both the posterior and anterior groups for all analyzed metrics (Table 4
Cost Outcomes (P Value Threshold 0.05/5 = .0125).a
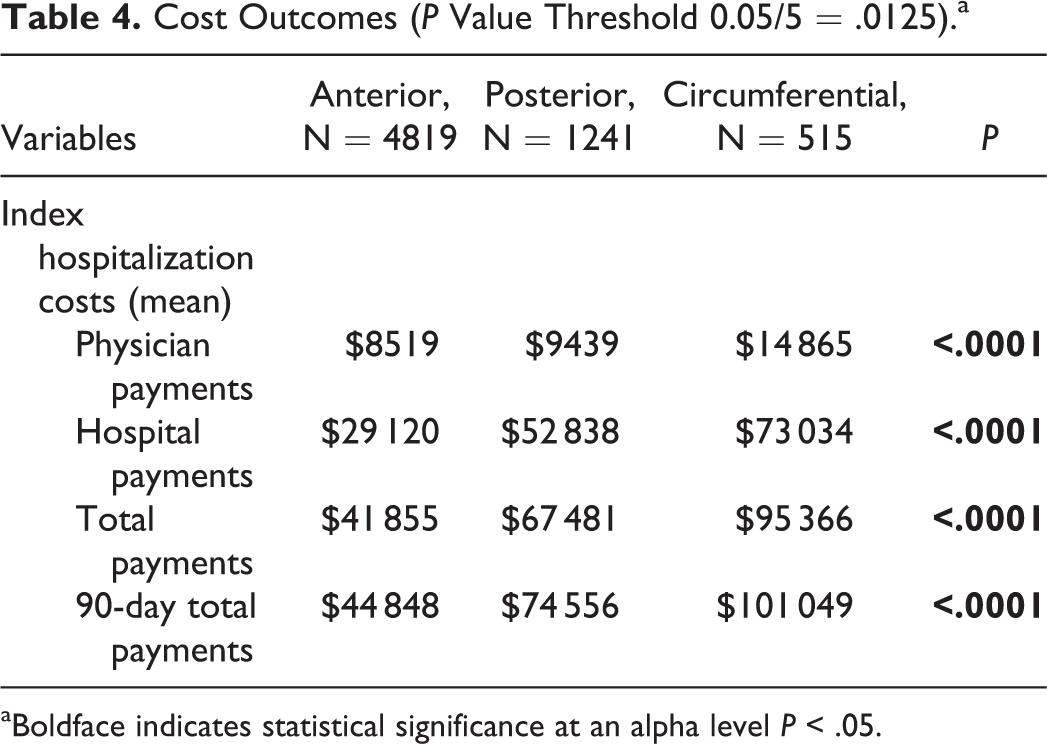
aBoldface indicates statistical significance at an alpha level P < .05.
Direct Comparison: Anterior Versus Posterior Cervical Fusion
The PSM algorithm successfully matched n = 2313 patients after anterior fusion to n = 1227 after posterior fusion, eliminating any statistically significant baseline differences (Table 5).
Demographics for PSM Cohort (P Value = 0.05/12 = .004).
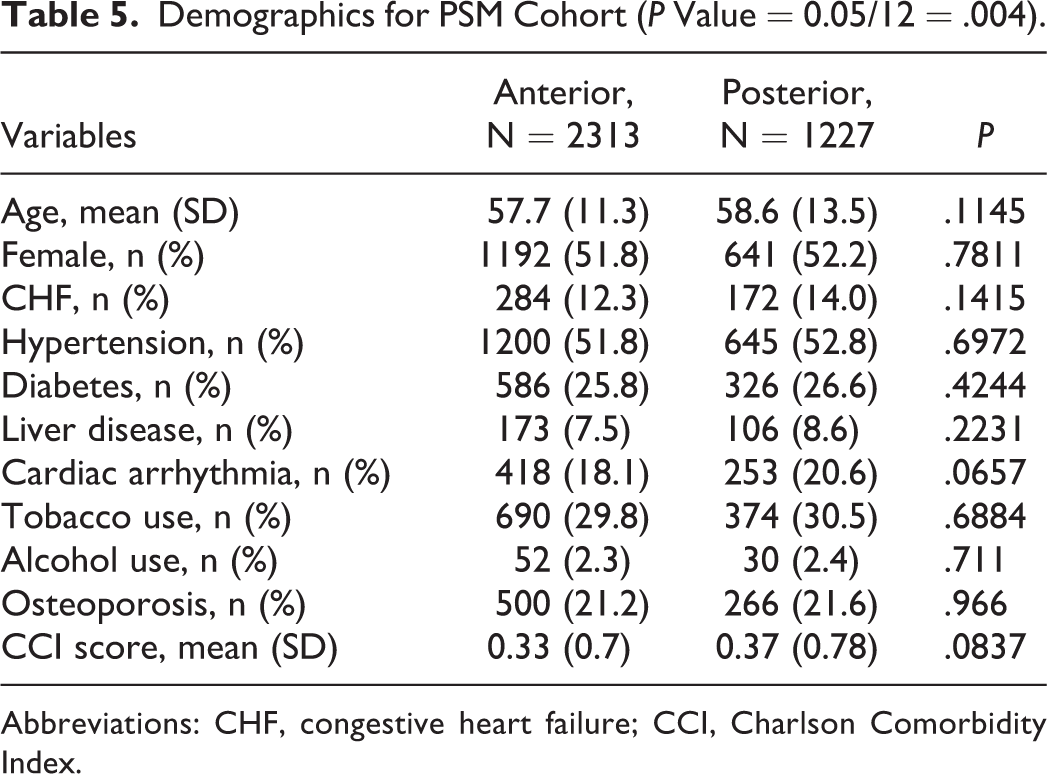
Abbreviations: CHF, congestive heart failure; CCI, Charlson Comorbidity Index.
Patients undergoing posterior cervical fusion were twice as likely as patients undergoing anterior cervical fusion to experience any kind of postoperative complication (odds ratio [OR] 2.0, 95% confidence interval [CI] 1.7-2.4, P < .0001; Table 6). The significantly higher likelihood for complications in the posterior fusion group was consistent across complication categories, including medical (delirium, anemia, pulmonary complications) and surgical (surgical site hematoma, wound dehiscence, SSI, and other wound complications), and trends were observed for cardiac dysrhythmia, PE, and pneumonia (all P > .003; Table 6).
Ninety-Day Complications for PSM Cohort (P Value Threshold 0.05/14 = .003).a
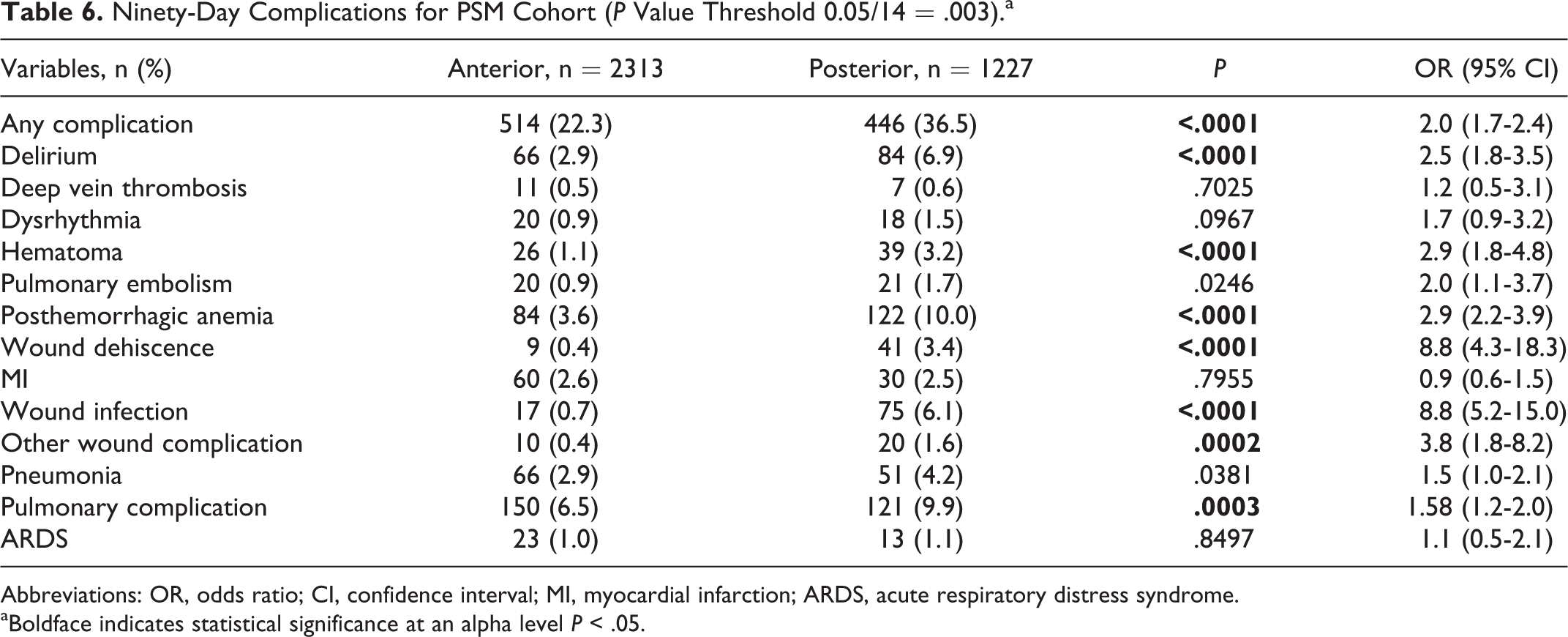
Abbreviations: OR, odds ratio; CI, confidence interval; MI, myocardial infarction; ARDS, acute respiratory distress syndrome.
aBoldface indicates statistical significance at an alpha level P < .05.
Patients undergoing posterior cervical fusion stayed about 2 days longer in the hospital than those undergoing anterior cervical fusion (P < .0001; Table 7). They were twice as likely as patients undergoing anterior cervical fusion to be readmitted to the hospital within 90 days (OR 2.0, 95% CI 1.6-2.4, P < .0001). The rates of reoperations were not statistically significant, but there was a trend toward more reoperations in the anterior (30.7%) as compared to the posterior fusion cohort (26.9%; P = .0173; Table 7).
Quality Outcomes for PSM Cohort (P Value Threshold 0.05/5 = .01).a
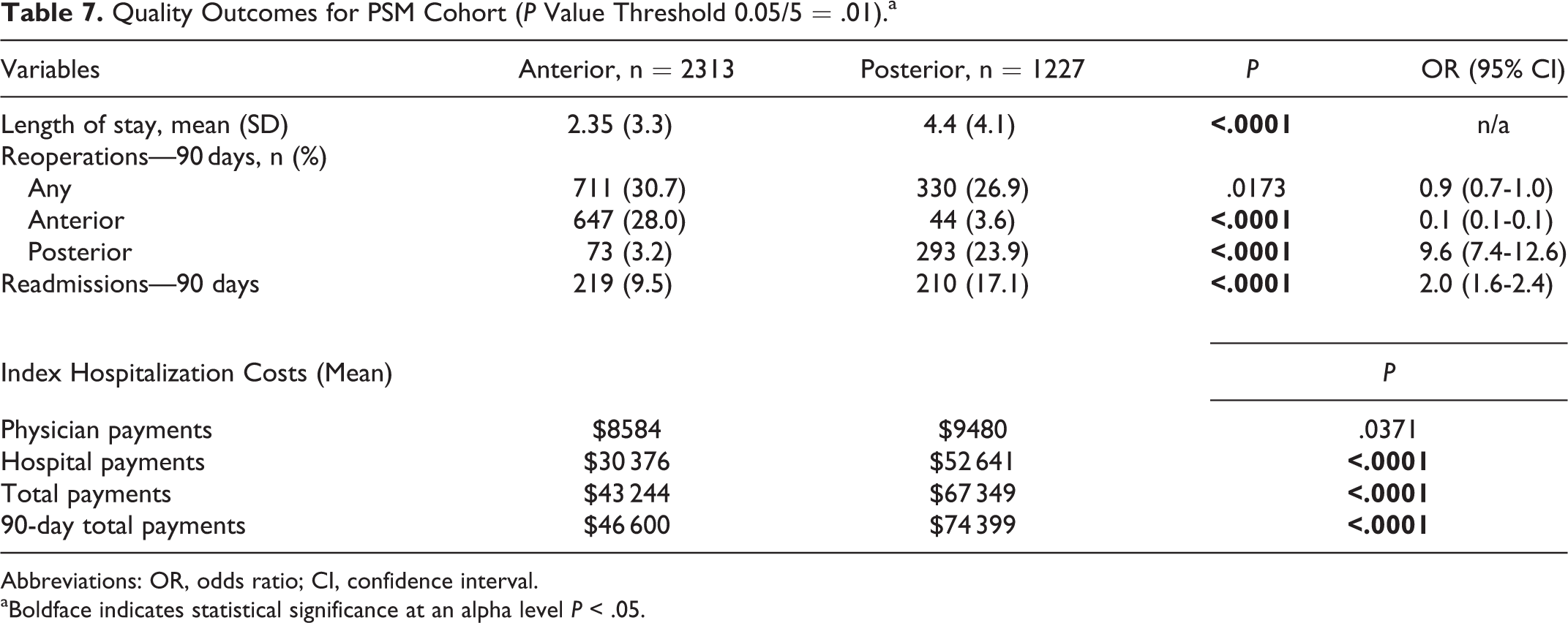
Abbreviations: OR, odds ratio; CI, confidence interval.
aBoldface indicates statistical significance at an alpha level P < .05.
With regard to costs, posterior cervical fusion patients registered higher index hospitalization costs (P < .0001) with a difference of +US$24 105. This difference was exacerbated by 90 days (+US$27 700, P < .0001; Table 7).
Discussion
Fusion procedures for the management of ACD typically include anterior, posterior, or combined (circumferential) approaches. Decision making in ACD includes defining one or a combination of several treatment aims (decompress nerves, stabilize motion segments, and correct deformity) together with the patient; however, the ideal approach for correction is often unknown. 2,3 The posterior approach is typically utilized in the surgical management of patients with flexible deformities, whereas anterior and combined approaches are used because of their ability to provide both ventral decompression and deformity correction. 6 -10 Both anterior and posterior approaches are effective in fixed deformity correction. 10 One particularly important factor in determine optimal treatment strategy is the degree of deformity correction required. Previous studies have reported anterior approaches achieving moderate deformity correction ranging from 11° to 32°, posterior approach achieving 23.3° to 53.8° of correction, and combined approach correction ranging from 24° to 61.3°. 10 Combined anterior-posterior approaches are becoming more popular given the potential for ventral lengthening and dorsal shortening in the corrective surgery. Abumi et al further corroborated the superiority of the combined approach in degree of correction, reporting reduction of kyphotic angles from 30.8° to 0.5° with combined anterior-posterior approaches. 11 Surgeons may also prefer combined or posterior approaches in lieu of anterior alone particularly in patients with postlaminectomy kyphosis where the risk of reconstructive failure is high. 12 The anterior approach is generally considered to be more tolerable and still effective in achieving significant deformity correction, whereas posterior and combined approaches offer greater mechanical advantage but higher morbidity risks. 1,3,6,13 -15
As each approach has particular strengths, understanding potential complications associated with each approach is also essential for spine surgeons and their patients. Here, the present study set out to determine complications and short-term quality outcomes in a large, comparative sample of patients undergoing each of the 3 approach types. Our findings reveal significantly higher complication rates after circumferential, as compared to anterior or posterior fusion procedures alone. Those results are somehow expected as the combined approach essentially combines the individual morbidity of each of the 2 isolated approached in the individual patient. The results are also consistent with previous retrospective single-center data from Cleveland (n = 76), where a total complication rate of 34% was described after fusion treatment for subaxial cervical deformity surgery. 16 The authors likewise found a higher complication rate after circumferential (40%), as compared to both ventral (30%) or dorsal approaches (27%). Whereas pulmonary complications and anemia were most common in the current sample, Grosso et al reported highest complication rates with regard to DVT (10.5%), deep wound infection (7.9%), pneumonia (5.2%), PE (3.9%), surgical site hematoma (3.9%), and nontransient dysphagia (>1 month) requiring a feeding tube (2.6%). 16 In a single-center comparative analysis of approach type for cervical deformity, Smith et al identified significantly higher complication rates: anterior only (27.3%), posterior only (68.4%), combined (79.3%; P = .007). This study also described an important point when comparing surgical approach for cervical deformity—patient selection and type and complexity of deformity may strongly influence outcomes. As previously discussed, anterior or posterior approaches may be preferred for specific deformities, a factor recognized as a limitation for this study. However, a PSM was utilized to equate morbidity between approach type cohorts, and both postoperative and quality outcomes remained significantly different between the 2 groups. Approach types may also have differing operative characteristics, for example, posterior approaches have been associated with fusions of a greater number of vertebral levels. 7,8,17 This increased operative burden is consistent with our findings of longer hospital stays and increased costs associated with posteriorly fused patients.
This study provides a comparative analysis of adult patients undergoing anterior and posterior cervical fusion for spinal deformity. Posterior and combined approaches carried higher rates of morbidity than anterior alone, along with longer length of stays, higher rates of revision surgery, and readmission. The adverse outcomes associated with posterior fusion remained after PSM to the anterior approach cohort. However, it is important to note that patient selection and complexity of deformity may be significant drivers of these outcome discrepancies. The database query did not allow us to obtain more detailed information about the specific type of ACD, whereas the surgical approach is known to differ in case of fixed (not passively correctable) versus non-fixed, ankylosed versus non-ankylosed, fused anterior versus posterior versus circumferentially. 4,18,19 The lack of data on number of levels fused, severity of curvature, and other metrics of deformity complexity particularly affected our ability to stratify the cohort by severity of disease. The lack of severity metrics is a significant limitation of this study. The specific indication for surgery, such as significant pain, intolerable deformity, or neurological deficit, was unavailable in this data set. Furthermore, as with all large database studies, interpretations of this study are limited by the administrative nature of this data. Further prospective studies should be conducted to provide clarity in defining optimal treatment strategies for patients with cervical deformities.
Conclusion
Patients undergoing posterior cervical fusion had higher rates of postoperative complications, reoperations, and readmissions than patients undergoing anterior cervical fusion. Of note, indications for anterior or posterior approach for cervical fusion may differ significantly, influencing outcomes. Nevertheless, this study identifies key differences in outcomes between the surgical approach types for cervical deformities and may be useful for surgical planning and patient education.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.