
Abstract
Study Design:
A retrospective single-center analysis of 159 cases.
Objective:
To investigate differences between male and female patients, as spinal infection (SI) represents a life-threatening condition and numerous factors may facilitate the course and outcome of SI, including patients’ age and comorbidities, as well as gender. To date, no comparative data investigating sex differences in SI is available. Thus, the purpose of the present retrospective trial was to investigate differences between male and female patients.
Methods:
A total of 159 patients who were treated for a spinal infection between 2010 and 2016 at our department were included in the analysis. The patients were categorized into 2 groups based on gender. Evaluation included magnetic resonance imaging, laboratory values, clinical outcome, and conservative/operative management.
Results:
Male patients suffered from SI significantly more often than female patients (n = 101, 63.5% vs n = 58, 36.5%, P = .001). However, female patients were initially affected more severely, as infection parameters were significantly higher (P = .032) and vertebral destruction was more serious (P = .018). Furthermore, women suffered from intraoperative complications more often (P = .024) and received erythrocyte concentrates more frequently (P = .01). Nevertheless, mortality rates and outcome were comparable. Pain scales were significantly higher in female patients at 12-month follow-up (P = .042).
Conclusion:
Although male patients show a higher incidence for SI, the course of disease and the management is more challenging in female patients. Nevertheless, outcome after 12 months is comparably good. Underlying mechanisms may include a better immune response and dissimilar effects of antibiotic treatment in women. Pain management in female patients is still unsatisfactory after 12 months.
Keywords
Introduction
Spinal infection (SI) is defined as an infectious disease affecting the spine and/or paravertebral tissue and still represents a life-threatening condition. 1 An SI can arise primarily by hematogenous spread, or secondarily, following spinal surgery or trauma. 2,3 The incidence of SI is on the rise over the past decades, 4 mostly due to an aging population suffering from various comorbidities, the increasing number of spinal interventions and instrumentations, but also due to improved diagnostic capabilities. 5 To date, SI represents 2% to 7% of all musculoskeletal infections 6 and still shows mortality rates between 2% and 20%. 7,8 Due to unspecific symptoms, the early diagnosis of SI is challenging, and sufficient treatment is complex. Numerous factors may facilitate the course and outcome of SI, including etiology, severity of comorbidities and immune status, as well as gender. Prior gender-specific investigations showed a male/female ratio ranging between 2:1 and 5:1. 9,10 To the best of our knowledge, no comparative data investigating sex differences in management and outcome of SI is available. Thus, the purpose of the present retrospective study was to investigate variations between male and female patients.
Material and Methods
We performed a retrospective analysis of all patients who presented with a SI at our department between 2010 and 2016. Patients were categorized into 2 groups according to their sex: group female (F) and group male (M). Diagnosis was based on clinical as well as on magnetic resonance imaging (MRI) findings. Radiologic parameters were evaluated by an independent radiologist, assessing localization and expansion of the infection, as well as the extent of disc and vertebral destruction. Data was collected using the patients’ digital health records at the author’s clinical department (Cerner Millennium–Power Chart, Cerner Corporation 2011, Idstein, Germany) and was documented according to institutional standards and the general standards according to the principles of good clinical practice (GCP). Data included demographics, ASA (American Society of Anesthesiologists) scores, clinical and neurological characteristics, infectious parameters, such as C-reactive protein (CRP) and white blood cell (WBC) count, treatment details (ie, operative vs. conservative) and treatment outcomes. Pain values were assessed by numeric rating scale (NRS) scores and muscle force was graded according to Medical Research Council (MRC). Parameters were gathered at different time points, depending on the course of management: data of surgically treated patients was compared on the day of initial diagnosis, at discharge and at 3- and 12-month follow-up. Patients were discharged according to institutional standards: (1) when intravenous pain- and/or antibiotic therapy could adequately be replaced by oral medication and (2) when CRP levels reached normal values, or were reduced by at least <50% of the value at admission. In conservatively treated patients’ data was collected at the time of the initial diagnosis, 14 days after treatment initiation, and at 12-week follow-up. Long-term outcome was not available for conservatively treated patients, as follow-up is generally terminated after 3 months when the course is satisfactory and CRP levels normalized. Outcome after 12 months was measured by pain values and muscle force, as well as the achievement of full remission and mortality rates. Full remission was defined as the individual clinical status the patient held before symptom onset of the SI. Patients suffering from neurological deficits, progressive or intractable pain and/or progression on MRI despite maximum conservative treatment qualified for surgical treatment. The operative procedure was determined individually for each patient, depending on present comorbidities, the extent and location of the infection and the degree of vertebral destruction. All patients were additionally treated with intravenous broad-spectrum antibiotics for 2 to 6 weeks, followed by oral antibiotics for a total period of 3 months. Initially applied antibiotics included clindamycin and ciprofloxacin and were adjusted according to the antibiogram, when available.
Statistical Analysis
All patients with complete initial data were considered in this retrospective analysis. Values are expressed by mean ± standard deviation (SD). The Kolmogorov-Smirnov test was used for testing normal distribution. The unpaired Student’s t test and Mann-Whitney U test were performed to analyze differences in clinical and demographic characteristics and in clinical outcome variables. Frequencies were compared by the chi-square and Fisher’s exact tests. Spearman’s rho correlation (r) was determined to assess the relationship between clinical outcome and demographics. A P value <.05 was considered statistically significant. All statistical evaluations were performed with SPSS Version 21.0 (IBM Corp. Released 2012. IBM SPSS Statistics for Mac OS X, Version 21.0, Armonk, NY). Figures were designed using Microsoft Excel (Version 15.36 for Mac OS X, Microsoft Corporation 2017, Redmond, WA).
Results
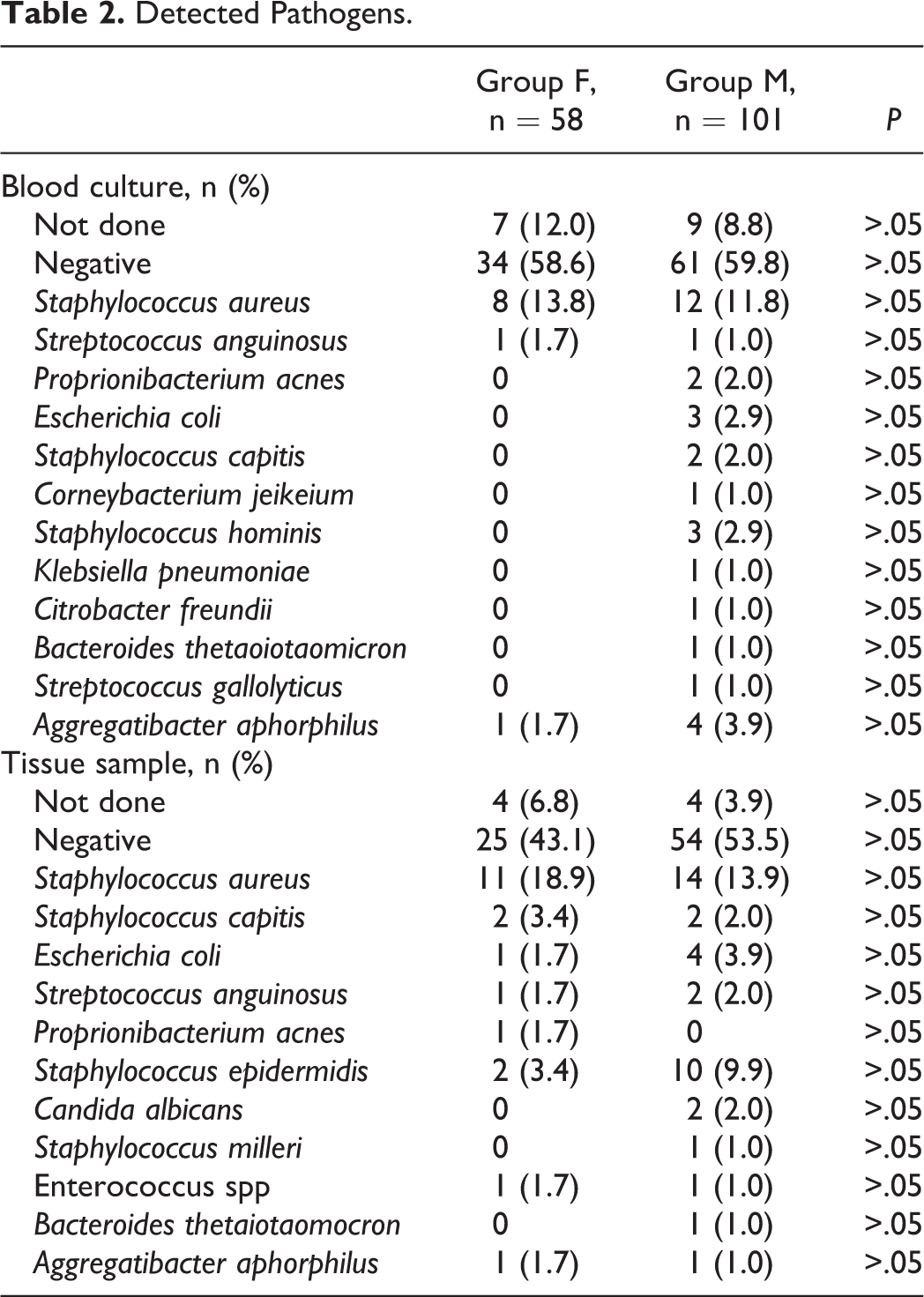
A total of 159 patients were identified and their data was investigated retrospectively. Demographic details and patients’ characteristics are outlined in Table 1. The proportion of female patients (group F, n = 58) to male individuals (group M, n = 101) was 36.5% and 63.5%, respectively (P ≤ .01). The mean age was 66 ± 12 years in group F and 65 ± 12 years in group M (P > .05). In both groups, the most common ASA score was 3 (n = 34, 59% in group F vs n = 55, 55% in group M, P > .05). The duration of the hospital stay did not differ significantly between group F (15 ± 12 days) and group M (11 ± 9 days, P > .05). Primary spondylodiscitis was as common in group F as in group M (group F: n = 36, 61%; group M: n = 68, 67%, P > .05). No significant differences were found with regard to comorbidities (P > .05). Nevertheless, some risk factors (eg, diabetes, active cancerous disease, alcohol abuse) were slightly more common among male patients (P > .05). Treatment did also not differ between groups: 44 female (76%) and 72 male patients (71%) were treated operatively (P > .05), whereas the remaining patients (14 female, 24% and 29 male, 29%) were treated conservatively (P > .05). No intergroup differences depending on the type of treatment were present. The location of the infection did not differ significantly between the 2 groups (P > .05) and no infection-specific differences (eg, type of pathogen, frequency of detection) could be detected (P > .05). Staphylococcus aureus was the most frequently isolated pathogen in both female (n = 6, 67%) and male patients (n = 8, 32%; P > .05; Table 2), At the time of diagnosis, group F showed significantly higher CRP levels than group M (15.2 ± 12.2 vs 11.1 ± 10.1 mg/dL; P = .032; (Figure 1). Radiographic analysis revealed a bony destruction of more than 50% in 9 patients (16%) in group F, whereas only 8 patients (8%) in group M showed the same degree of destruction (P = .018). Intraoperative complications (ie, bleeding, dural or pleural injury) were significantly more often observed in group F (F: n = 6, 11% vs M: n = 2, 2%; P = .024; Table 3), as well as a greater need of intraoperative blood products (573 ± 570 vs 351 ± 570 mL; P = .01; Table 3). Additionally, postoperative blood products were used in female patients more frequently, although this difference did not reach statistical significance (147 ± 450 vs 75 ± 240 mL; P > .05). Outcome was comparable after 12 months, as mortality rates were similar (n = 6, 10% in group F vs n = 8, 8% in group M; P > .05). Full remission was achieved in 55% (n = 32) in group F, and in 56% (n = 57) in group M (P > .05). Muscle force recovered equally in both groups (P > .05) (Figure 2). The NRS (0-10) after 12 months, however, differed significantly between the groups, as group F showed a mean pain scale of 1.8 ± 1.5, whereas group M presented with 1.0 ± 1.7 (P = .042) (Figure 1).
Demographic Details.
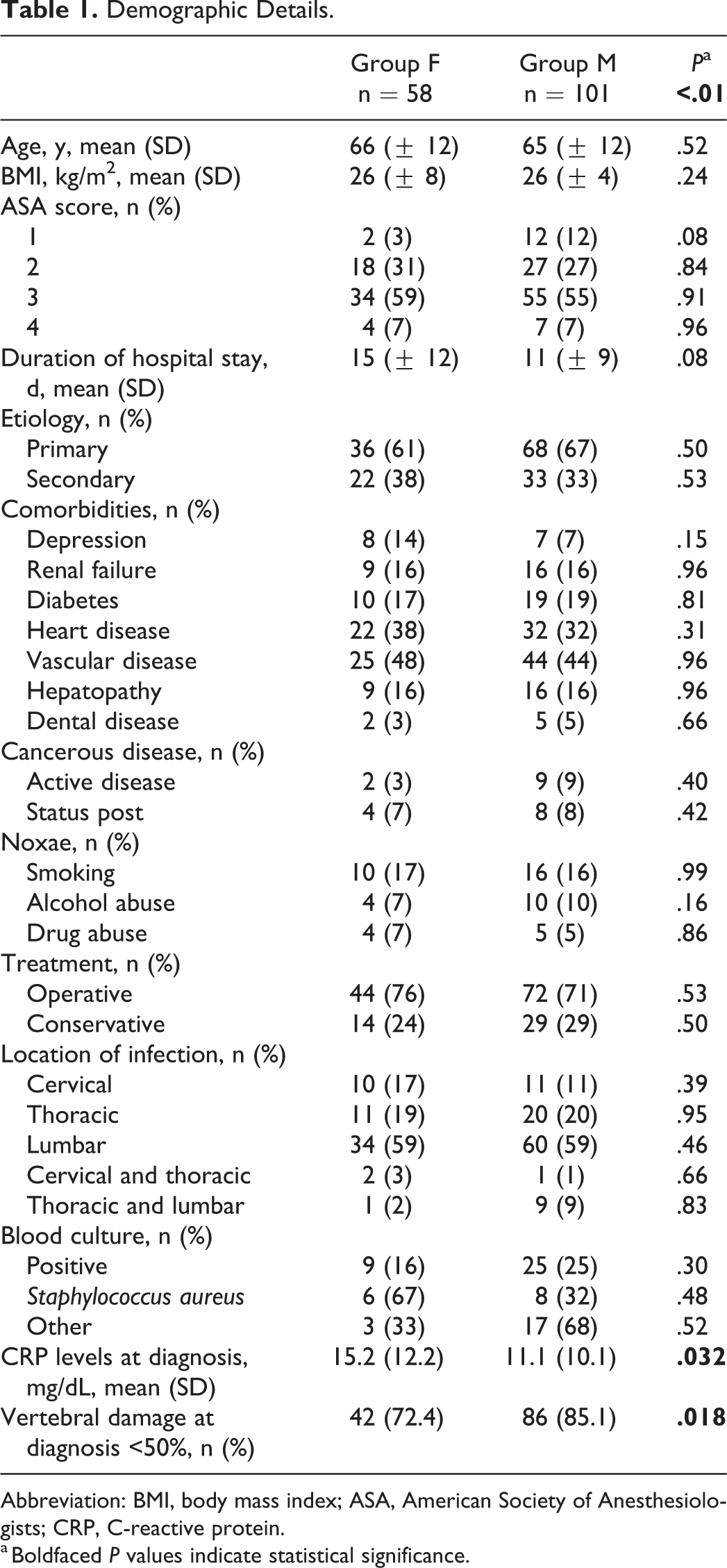
Abbreviation: BMI, body mass index; ASA, American Society of Anesthesiologists; CRP, C-reactive protein.
a Boldfaced P values indicate statistical significance.
Detected Pathogens.
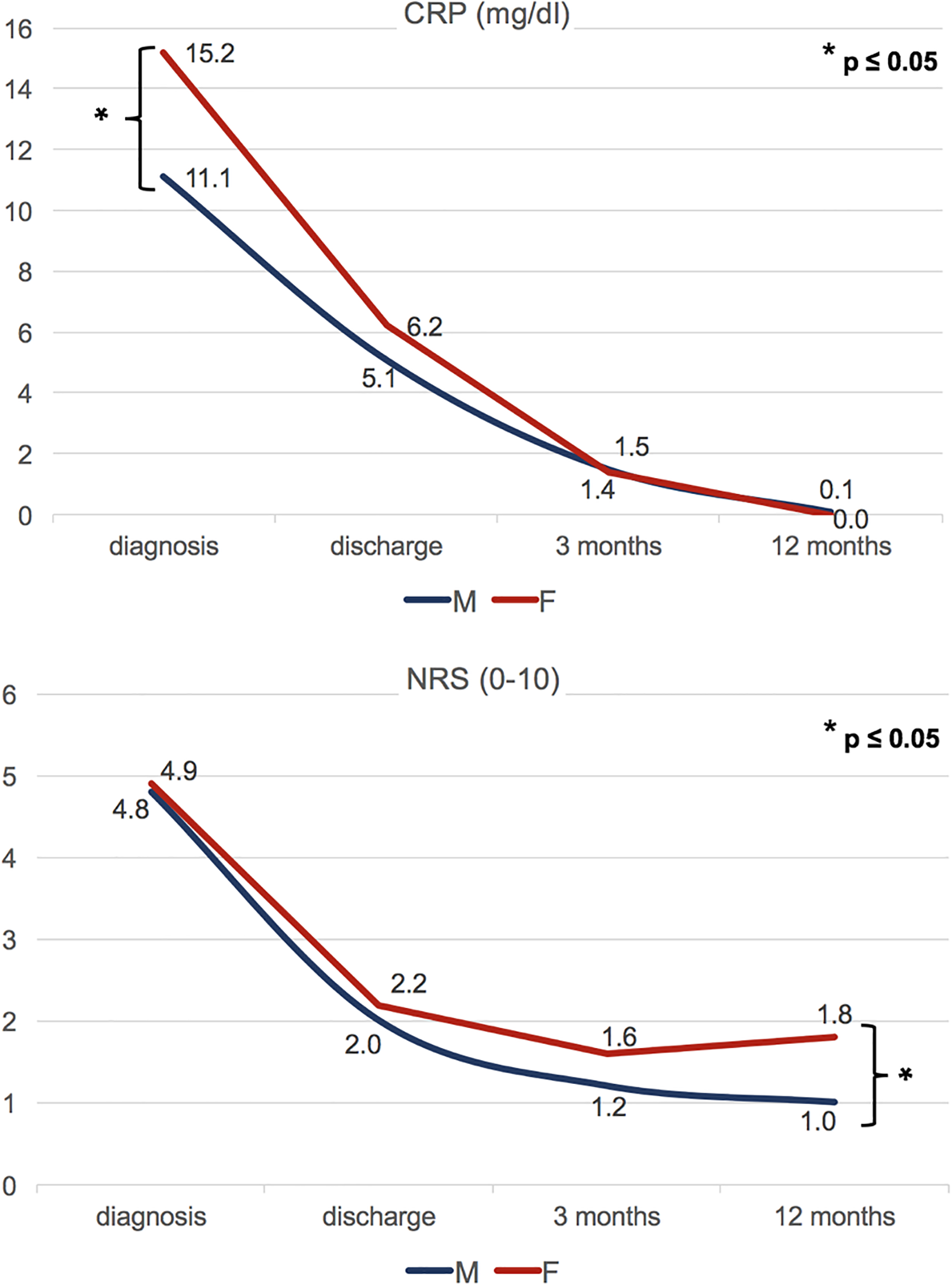
Course of C-reactive protein (CRP) levels (in mg/dL) and pain scales (numeric rating scale [NRS] 0-10) over a follow-up period of 12 months (F, female; M, male).
Intraoperative Complications.
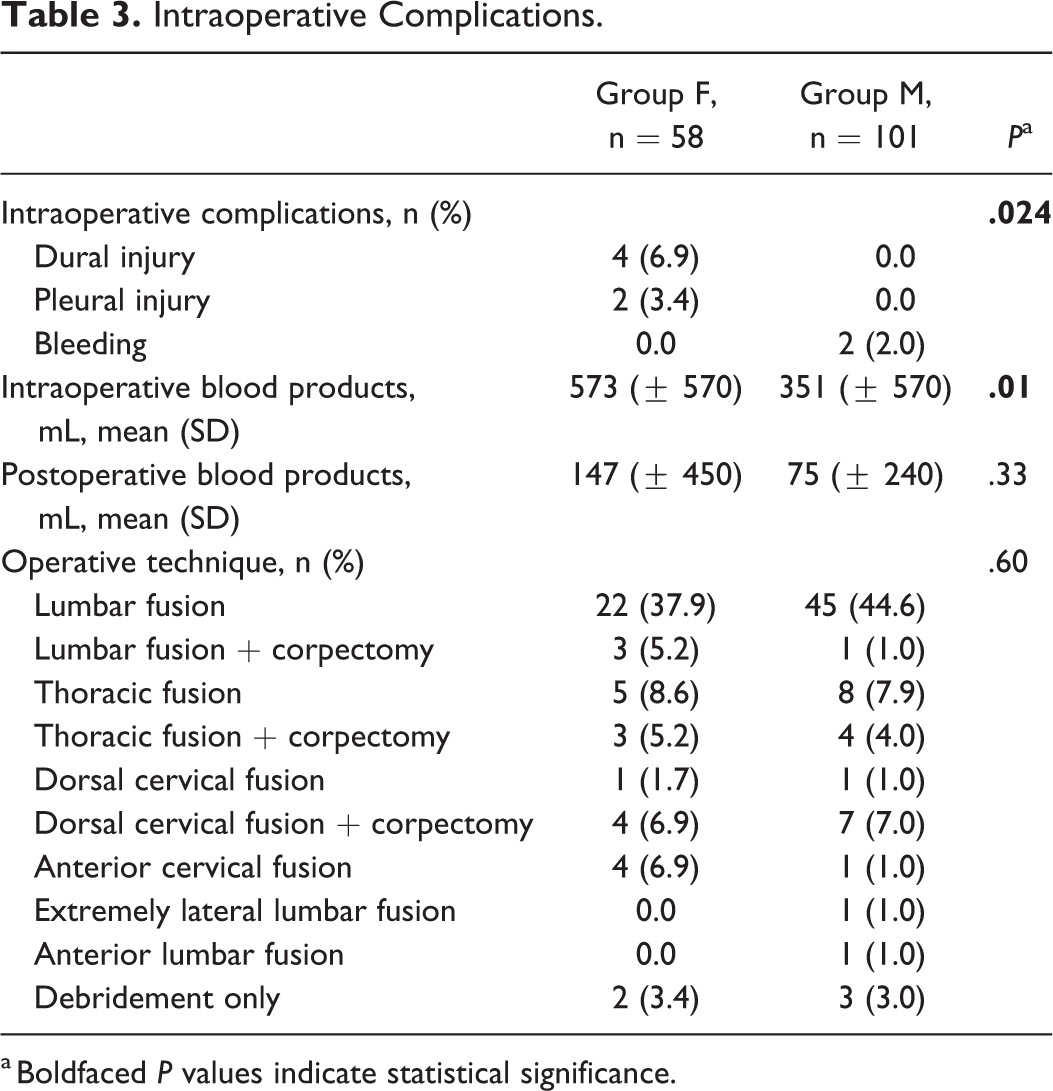
a Boldfaced P values indicate statistical significance.
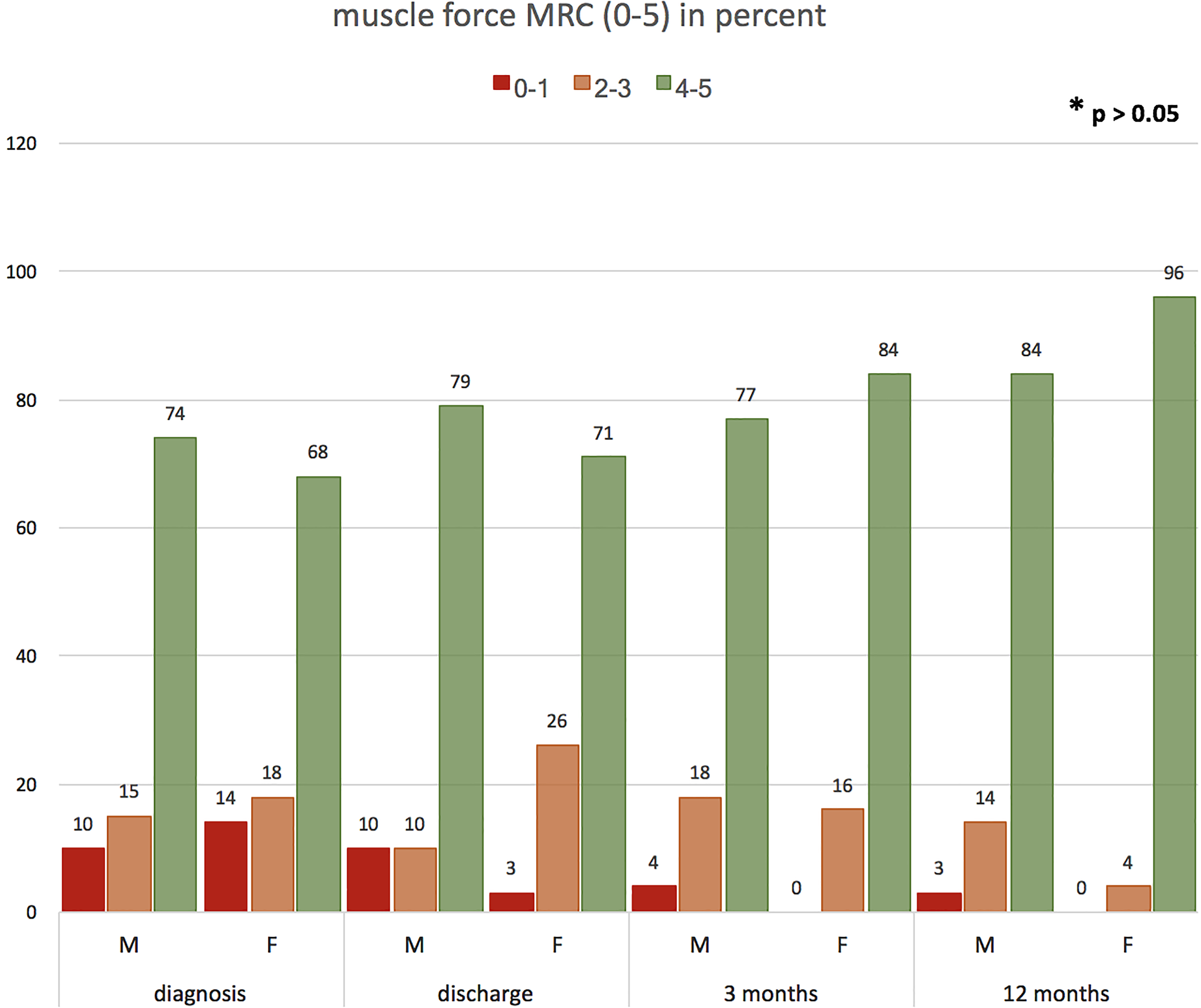
Course of muscle force (according to Medical Research Council [MRC] 0-5) over a follow-up period of 12 months listed in percent (F, female; M, male). Muscle force was subdivided into 3 groups regarding the patients’ functional restriction: 0-1, no function; 2-3, limited function; 4-5, unlimited function.
Discussion
We present the results of a retrospective single-center study investigating gender differences in SI. Male patients showed a higher incidence of the disease. Female patients presented with higher inflammatory laboratory parameters and more severe vertebral destruction at diagnosis. During the course of treatment, they also demonstrated a higher perioperative complication risk. Nevertheless, outcome after 12 months including mortality rates was comparable.
The majority of patients presenting with a SI were male. This is in line with previous reports, identifying the male gender as a risk factor for the development of a (postoperative) SI. 11,12 Reasons are still unknown and could also not be identified in our retrospective setting. Nevertheless, general risk factors for the development of a spinal infection, for example, immunodeficiency, alcohol/drug abuse, and severe comorbidities 5 tended to be more frequent in male than in female patients.
Female patients presented with higher serum parameters for infection and additionally showed a higher grade of vertebral destruction at diagnosis. Definite reasons for the progressed stage of the disease could not be found within our retrospective analysis, as the time span between symptom onset and diagnosis could not be investigated precisely. Presumably, as already analyzed in other trials showing differences in inflammatory spinal disorders, 13,14 female patients may have presented with more unspecific symptoms (eg, diffusely localized pain) than male patients and might have been misdiagnosed in early stages of disease. This may have led to a longer duration between symptom onset and diagnosis, thus consequently to an advanced stage of spinal infection at presentation.
Females showed a significantly higher perioperative risk for intraoperative complications as well as for the need of supporting blood products. The higher complication rate matches findings in prior trials, 15,16 as well as the higher amount of used blood products. 17,18 Reasons for those findings may include the relation to a preseptic state in female patients, as the duration of surgery increases in cases of more severe affection, and complication rates rise with extensive procedures. 19
Nevertheless, the outcome at 12 months of follow-up was comparably good. Mortality rates, as well as residual neurologic deficits (eg, muscle weakness), did not show any significant differences between both groups. Full remission was reached in comparable frequencies in group F and in group M. Still, women suffered from significantly more pain than men.
Reasons for those final findings are numerous. First, women are known to react differently to infection than men. Higher levels of estrogen seem to have immune-modulating effects and make female patients not only more resistant to major infection but also enhance recovery. 20,21 Advanced patients’ age and menopause may indeed lower the positive effects of estrogen on immunomodulation, but it is known that women show even more favorable factors on the control of infection (eg, expression of structures of the innate immunity). 22,23 Furthermore, female patients react differently to antibiotics, which may render them better responders for conservative or additional medical therapy in cases of SI. 24 -26
Regarding the fact that full remission was achieved in 55% of female and 56% of male patients, no significant differences could be demonstrated between the both groups. Nevertheless, this fact depicts the severity of the disease, as despite maximum treatment in a high-volume hospital only slightly more than half of the patients reach full remission 12 months after symptom onset. Reasons include the overall delayed diagnosis, the potentially long duration from symptom onset to the referral from low-volume hospitals and the timing of surgical intervention. 27,28
In summary, women may present with advanced stages of infection and may be affected more severely at diagnosis than men. Additionally, they show a higher perioperative complication risk. Nevertheless, female patients seem to compensate this disadvantage over time, as they show a higher ability of immune-modulation and resistance, as well as a superior response to antibiotic treatment. After 12 months, an unsatisfactory pain management was the only intergroup deficit female patients in our cohort showed. It is well known that pain therapy is more challenging in women. On one hand, the benefit of higher estrogen levels in the infectious setting may be a disfavor in pain management. High estrogen levels show a direct correlation with lower pain thresholds, in both experimental and natural pain. 29,30 Again, advanced patients’ age and menopause may counteract this fact. On the other hand, sufficient medical pain therapy in women may constitute a problem, as metabolism of preparations, but also psychological effects show differences in direct comparison with men. 26,31 -34 Furthermore, data suggests that female patients are likely to be treated less adequately, at least with regard to pain. 35
Our retrospective results demonstrate the clear differences in incidence, the severity of disease at diagnosis, in management and in outcome among female and male patients. However, several limitations have to be considered, including the retrospective study design. What is more, as a neurosurgical department our patient population represents a preselected group with a high proportion of patients that may have already failed conservative care at an outside institution. It may also be speculated that female patients are transferred to our unit later in the course of SI at a time point when they are already preseptic. If our findings should imply a change in treatment strategy for either men or women is currently unresolved. Mainly, special attention should be paid not only to early diagnosis and the reduction of perioperative complications but also to the efficacy of pursuing pain therapy in female patients, in terms of an even more individualized management strategy and, in cases of doubt, generous dose adjustment of pain medication. 36
Conclusion
Although male patients show a higher incidence for SI, the course of disease and the management is less challenging than in female patients, which are characterized by a more advanced stage of disease at diagnosis and significantly higher perioperative complication rates. Nevertheless, the outcome after 12 months is comparably good. Underlying mechanisms for this adaptation may include a better immune response and dissimilar effects of antibiotic treatment in women. Still, pain management in women is unsatisfactory after 12 months of follow up. To reduce limitations and support the evidence of our findings, further prospective clinical trials will be mandatory.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.