
Abstract
Study design
An umbrella systematic review.
Objective
To identify historically recognized injury characteristics that may affect treatment decisions of traumatic C2 injuries and help improve the description of the “modifiers” presented in the AO Upper Cervical Injury Classification (UCIC).
Methods
We performed an umbrella review of systematic reviews evaluating studies about the management of axis fractures that identify potential modifiers in the treatment of these injuries. These modifiers were grouped according to the new AO UCIC.
Results
Eight systematic reviews were included. They were divided into three groups: (1) Axis body fractures – one study, (2) Hangman´s fractures – one study, and (3) Odontoid fractures, six studies. For axis body fractures, most injuries were treated non-operatively, except some Benzel type 3 fractures (AO Type A) with displacement or severe comminution (M1). Hangman´s fractures classified as Effendi I and Levine-Edwards I and II were treated non-operatively with success, with no modifiers identified for non-union or instability. For Levine-Edwards type IIA and III surgery was generally recommended, but these should be classified as AO type B and C respectively without a need for modifiers. For odontoid fractures, fractures in the dens base, with displacement, or in elderly patients were associated with non-union (M1) and patients’ specific factors (surgical condition) seem to affect the decision of treatment (M3) for considering surgery.
Conclusions
We identified from the literature some axis injury characteristics that seem to affect the treatment decision in historical series. Knowledge of these modifiers may further enhance the system’s clinical utility.
Introduction
Upper cervical or craniocervical spine trauma can result in severe disability or even death.1,2 Axis injuries are one of the most common sites of cervical spine traumatic injuries.
3
The management of these injuries was previously based on many different classification systems, such as the Anderson and D´Alonzo for odontoid fractures – Traynelis classification for occipital-condyle dislocations – Effendi and Levine and Edwards for axis injuries, among many others.4-8 Considering the difficulty in proper classification and treatment for these injuries in a uniform manner, the AO Spine KF Trauma and Infection study group proposed and developed a new system – the Upper Cervical Injury Classification System (UCIC).
8
In this system, injuries were grouped according to the affected region (Region I – occipital condyle and craniocervical junction; Region II – C1 ring and C1-2 joint and Region III – axis body, odontoid process, and C2-3 joint), followed by a subtype classification in a crescent degree of injury severity (A – primary bone injuries; B- injuries that may affect the bone but also with a suspected or clear ligamentous injury but without important dislocation/ displacement and C- translation or dislocation of the vertebral elements clearly configuring some degree of instability). The classification is fully presented in Figure 1. For the classification of the neurological status, the previously described AO Spine neurologic injury classification is used. The AO Spine Upper Cervical Injury Classification System.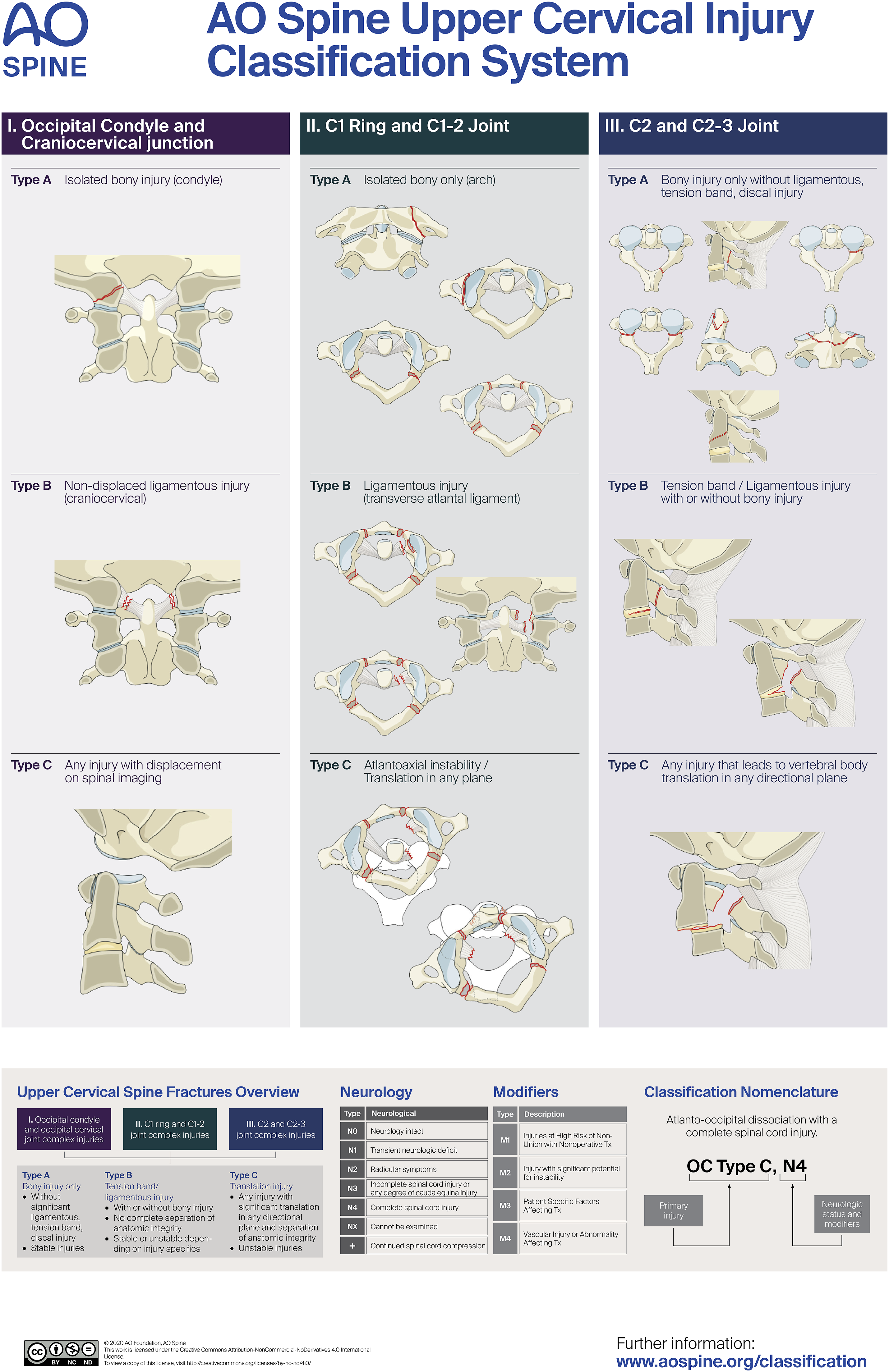
The main morphologic classification of the UCIC has been proven to be reliable and well reproducible.9,10 It is a promising effort to unify the fracture classifications and therefore also unify treatment guidelines in the future. However, the definite treatment decision is in many cases still reliant on ‘Modifiers’. The four proposed modifiers are: M1- injuries at high risk of nonunion with non-operative management, M2 – injuries with significant potential for instability, M3 – patients’ specific factors affecting treatment and M4 – vascular injury or abnormality affecting treatment.
Considering the importance of these modifiers in the final treatment decision and the fact that they are broadly described, the objective of the present study is to identify potential characteristics that seem to influence treatment decision of UCIC in the literature. Specifically, this umbrella review aims to search for factors that affect treatment of acute traumatic Region III (axis body, odontoid process, and C2-3 joint) injuries to sharpen the definition of the modifiers used within the UCIC at this level.
Methods
An umbrella literature review following the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) Guidelines was performed to identify the risk factors and injury characteristics that may affect the treatment decision of traumatic axis injuries. 11
We only included systematic reviews and/ or meta-analyses evaluating clinical studies about the management (operative and/ or non-operative) of axis traumatic injuries in any region (body, posterior elements, odontoid process, facet joints, and disc) that identify potential modifiers affecting the treatment decision. The included studies were grouped according to the affected axis segment (odontoid, body and posterior elements) and the modifiers grouped according to the new AO Spine Injury Classification in: M1 - high-risk of non-union with non-operative management; M2- injuries at high risk of instability, M3 injury or patient characteristics that may affect management and M4- vascular injury or abnormality. 8 Clinical studies which were not systematic reviews or meta-analyses were excluded from the Results.
The following search entries were used in the PubMed database for search “axis AND fractures AND systematic review” on July 28th, 2024. We obtained a total of 56 studies. After screening the abstract and the full title, a total of 17 systematic reviews were fully evaluated (Figure 2). After full manuscript evaluation, we included a total of eight systematic reviews, all of them with results that may affect the management of axis injury. The eight included articles were then grouped according to the exact location involved, as it follows: A- Axis Body Fractures – one study, B- Posterior elements of the axis injuries (Hangman´s fractures) – one study and C2- Odontoid fractures – six studies. The nine excluded papers did not report information about the potential factors that modify the management of axis fractures. The information influencing the modifiers was extracted from the Results or the Discussion of the included articles. Flow chart of our search mechanism.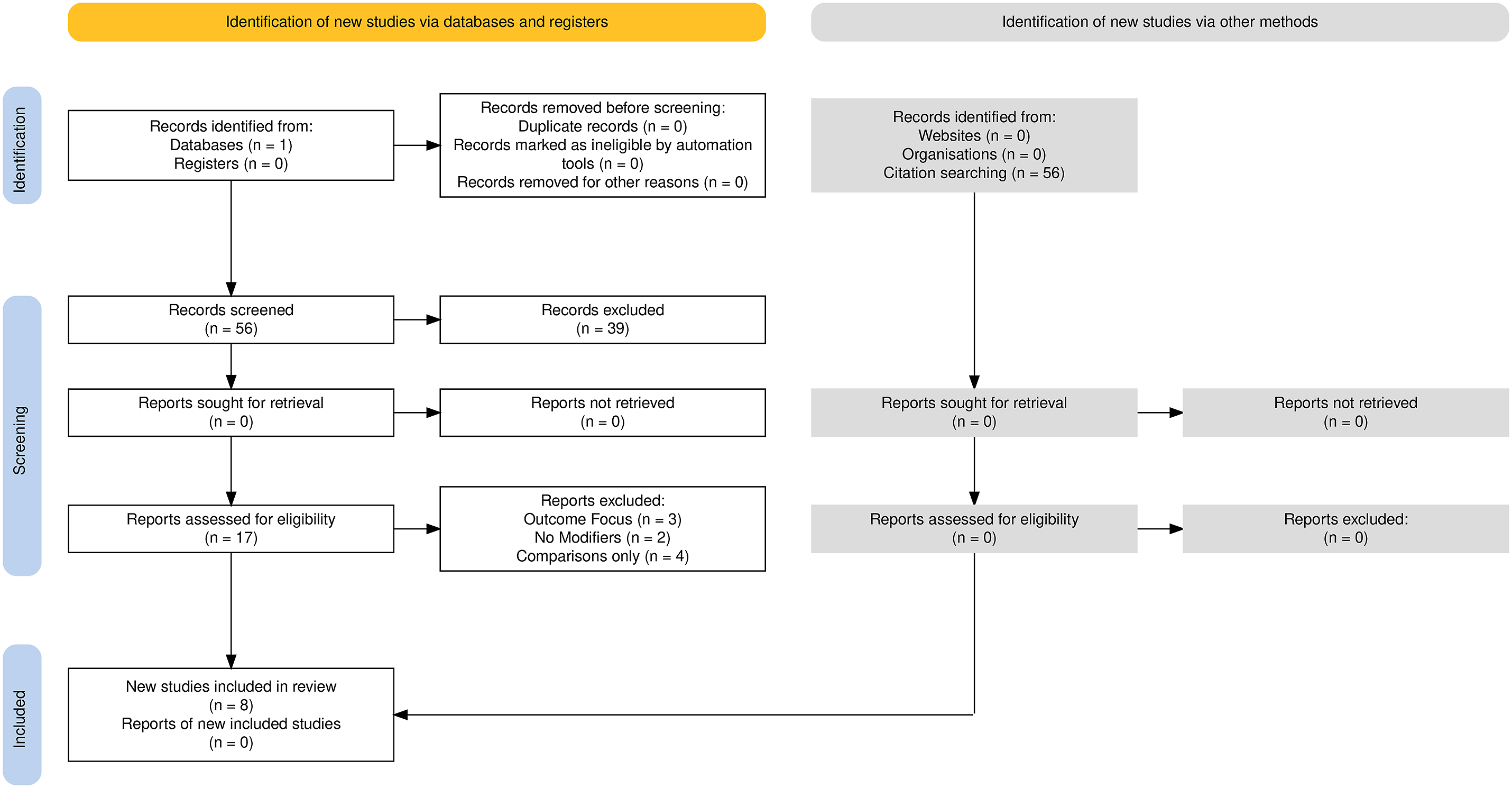
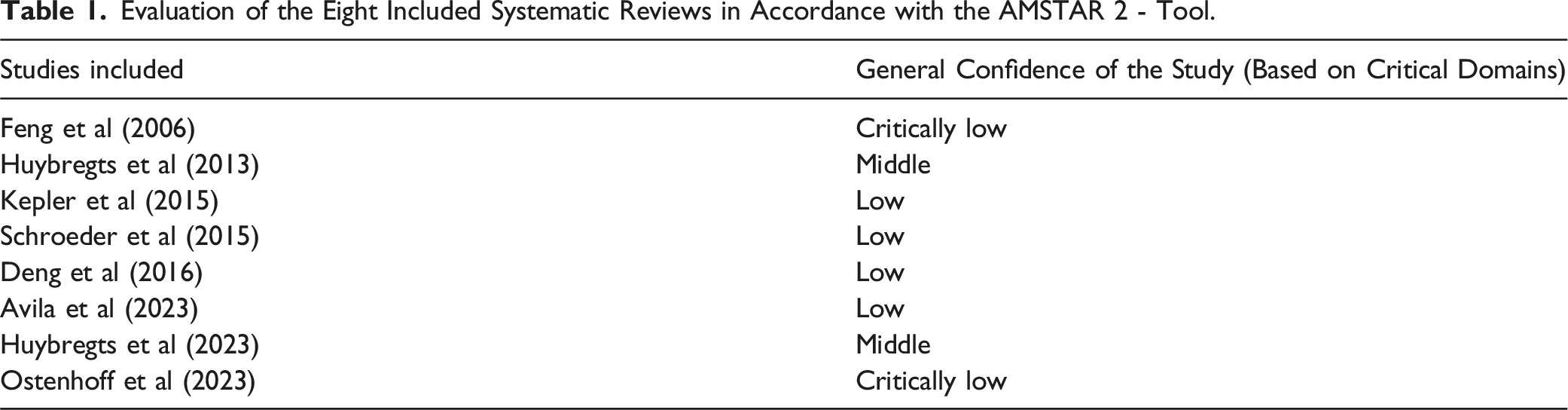
Evaluation of the Eight Included Systematic Reviews in Accordance with the AMSTAR 2 - Tool.
Results
We presented the results of the eight included reviews grouped according to the purpose of the systematic review. The quality of assessment in accordance with the AMSTAR 2 tool was low for four included reviews, critically low for two, and middle for two, suggesting that the studies had, in general, important methodological flaws (Table 1).
Axis Body Fracture – One Study
Kepler et al, in 2017, performed a systematic review to evaluate the best treatment options for axis body fractures. 13 They graded the quality of evidence with the Grading tool developed by the Center for Evidence-based Medicine. Operative and nonoperative treatment of axis body fractures were compared using fracture bony union as the primary outcome measure. As risk factors for nonunion were not consistently reported, cases were analyzed individually. A total of 52 studies with 920 patients were included and almost all studies (48 of 52) had less than 50 cases. The level of evidence of the included studies was: four type 2b, one type C, and 47 type 4 (LoE Oxford). 14 The overall bone union was 91%. They classified injuries according to the Benzel classification for axis body fractures (type 1 – coronally oriented fractures, type 2 – sagittally oriented fractures, and type 3 – horizontal rostral C2 fracture previously described as type III odontoid process fracture described by Anderson and D´Alonzo). 15
About 24% of patients with Benzel type III were surgically treated. From the 920 axis body fractures (from the 3030 fractures included in the entire review), 70 patients (7.6%) had type I, 22 (2.5%) had type II, and 696 (75.7%) had type III fractures.
Most of the injuries were treated nonoperatively - 713 of 868 (920- 52 patients who were lost to follow-up or died before treatment) – 82.1% - were treated non-operatively. The type III fractures were treated non surgically in 76% of the cases and nearly all Benzel types I and II were successfully treated nonoperatively. Type I and II cases treated operatively had generally a concomitant injury. The overall union rate for all 734 fractures studied was 91.0%.
Operative treatment of 68 fractures resulted in 64 successful unions, with a union rate of 94.1% (95% CI, 88.5-99.7). All four cases of nonunion occurred after anterior approach interventions, which decreased the overall union rate for anterior operative cases to 90.5% (95% CI, 81.6%–99.4%).
Considerably more type III axis body fractures were treated operatively. Authors concluded that Type III were more prone to be treated operatively 147 (22.3%), compared with 8 (3.8%) type I or II fractures (P < 0.001).
Indications for surgery (reported in only 10 studies) were an important degree of displacement between the fragments and facet subluxation.16-19 Two studies proposed surgical fixation for fractures with displacement greater than 4 mm without mentioning the radiological modality (CT or x-rays).19,20
Spinal malalignment and C2-3 subluxation associated with axis body fractures were also considered for surgical fixation – although the degree of these findings was imprecisely described (5 mm of subluxation in two cases).17,18 Finally, comminuted fractures and fractures in patients older than 40-65 years old were an indication for surgery.16-19
Of note, older injuries, with a spinal trauma >3 weeks, were considered for surgical treatment by some authors, but they are out of the scope of our review.21,22
After evaluating this systematic review, the following risk factors for non-union (M1)/ operative treatment could be identified in some of the included studies, potentially favoring surgical treatment: - Type III axis body fracture according to Benzel classification, injuries associated with facet subluxation, fracture displacement (4-6 mm?), comminution, concurrent injuries requiring surgical treatment, older age, older fractures (>3 weeks after trauma).
Axis Body Fractures – Potential Modifiers
M1 – Used For Injuries at High Risk of Non-Union Without Operative Management
- Vertebral body with displacement between the fragments* - Transverse vertebral body comminution (type III Benzel fracture) (22.3% of them compared with 3.8% in type I and type II) - Delayed treatment (more than 3 weeks)
*Note from the authors – the degree of displacement between the fragment’s threshold for describing an injury as type A M1 vs a type C is controversial. Displacement of more than 4 mm based on CT scan may be considered as a risk factor for non-union. 23
M3 is Used for Patient Specific Characteristics, Which May Affect Management
- Patient age (older patients may have a high non-union rate) (the age limit is unclear – some authors proposed >65 years-old)
Note: a C2-3 subluxation should not be considered as a Modifier because this would change the classification to type C.
Hangman´s Fracture – One Study
Xin-Feng et al, in 2006, performed a systematic review to evaluate the management of hangman´s fractures. 24
A total of 357 patients were included, with 104 treated operatively and 253 non operatively. Most patients with Type I and Type II (Effendi) and Type II (Levine-Edwards) were treated non-operatively, whereas the majority of Type IIa (Levine-Edwards) and Type III had surgical treatment with anterior, posterior, or combined approach. Of note, in this review, no quality assessment of the included studies was performed, and 31 were retrospective case series and only one prospective study (Govender et al, 1987). All Effendi type I injuries treated non-operatively healed well. For Effendi type II and Levine-Edwards type II, high healing rates were reported (up to 80% and 60% respectively). On the other hand, for type Levine Edwards type IIA and III, the healing rates were below 50% when treated non-operatively.
Many criteria of instability were proposed for Hangman´s fractures, such as displacement of C2 greater than 6 mm anteriorly, displacement greater than 2 mm on flexion/ extension radiographs, angulation of the dens greater than 20°, pedicle injuries, among others.
As a general conclusion, Xin-Feng et al reported that types I and II for both Effendi and Levine-Edwards may not need surgical stabilization. However, Levine-Edwards Type IIA and type III, as well as Effendi type III required surgical fixation.
Hangman´s Fractures – Potential Modifiers
For Type I and Type II (Effendi) and Type II (Levine-Edwards) no modifiers were identified that may lead to surgical treatment – once non-operative management is safe and well established for these injury patterns.
Note: type II A (Levine-Edwards) and type III and may not be considered as Modifiers as they would change the classification to type B and C, respectively, in accordance with the new AO UCIC.
Odontoid Fractures – 6 Studies
For odontoid fractures six studies were identified and included: (1) Huybregts et al, 2013, (2) Schroeder et al, 2015; (3) Deng et al, 2016; (4) Osterhoff et al, 2023; (5) Avila et al, 2023 and (6) Huybregts et al, 2023.25-30
1- Huybregts et al., 2013, performed a systematic review to evaluate the outcome of surgical and conservative interventions in the elderly (>65 years). 25 A total of 19 studies were included. All of them were retrospective. Authors included patients with type II and III odontoid fractures, with different age limits (65, 70, 80, etc.). The risk of bias in the included studies was assessed with the Cochrane form (II for RCT, III for cohort studies, IV for patient control studies, and a self-designed appraisal form for uncontrolled case series) – limited quality of evidence was reported once there is no control group and a small number of patients.
Osseous union was achieved in 66% (225/343) of patients surgically treated and in 28% (58/204) of those treated conservatively. No statistical analysis was performed.
Stability was achieved in most patients regardless of treatment (95% - 268/281 of those surgically treated and 77% - 117/151) of those treated non operatively.
2- Schroeder et al., 2015, performed a systematic review to compare early (<3 months) vs late (>12 months) mortality and complication rates of patients >60 years in type II odontoid fractures managed either operatively or nonoperatively. 26 This systematic review included 21 studies: one level 2, 12 level 3, and 8 level 4 of evidence, under the JBJS classification of the level of evidence, with 1233 patients evaluated.
Patients who had surgical treatment had short-term mortality (odds ratio, 0.43; 95% confidence interval, 0.30-0.63) and long-term mortality (odds ratio, 0.47; 95% confidence interval, 0.34-0.64) lower than patients who underwent nonsurgical treatment, and there were no significant differences in the rate of complications (odds ratio, 1.01; 95% confidence interval, 0.63-1.63).
They concluded that in well-selected patients older than 60 years surgical treatment decreased the risk of short- and long-term mortality without an increased risk of complications. However, the authors emphasized that a potential bias may be that patients unfit to undergo surgery were included in the nonoperative group and may be responsible for the higher mortality rate in this group. Additionally, the role of comorbidities could not be assessed in the systematic review of heterogeneous case series.
3- Deng et al., 2016, performed a systematic review and meta-analysis to evaluate patients older than 80 years with acute odontoid fractures (91.9% of type II, 237/258, and 8.1% type III, 21/258 patients). 27 They evaluated 22 case series and retrospective studies – five comparatives, 11 surgical series, and six non–surgical series. Two of them were classified as level III and 19 level IV of evidence.
The mortality rate was 5.4% (8/149) in the surgical vs 10.1% (10/99) in the non-surgery group (P = 0.159). The overall complication rate was higher in the surgically treated group – 38.9% (58/149) vs 24.5% (26/106) than in the non-operative group (OR 1.96 – 1.13-3.40), P = 0.016. Patients who had surgery had a higher osseous union (68.5%; 37/54 vs 43.2%, 16/37 – OR 2.86 – 1.2-6.8); P = 0.016. Fracture stability was higher in the surgical group 86% (49/57) vs 63.6% (28/44) – OR 3.5 – 1.33-9.21 P = 0.009 but was not clearly defined by the authors.
They concluded that octogenarians who had surgery had higher fusion and stability rates but also higher complications with similar mortality.
4- Osterhoff et al, 2023, performed a systematic review and expert consensus of the German Society for Orthopaedics and Trauma. 28 Prospective and retrospective observational investigations in patients more than 60 years, involved in the treatment of odontoid fractures. The level of evidence according to the Oxford Centre for Evidence-Based Medicine was used to classify the studies. Twelve articles were included. Five are retrospective case series and seven are national databases. All studies reported at least 100 patients in a total number of 48.316 cases.
They reported some risk factors for instability in their results – angulation greater than 11° and displacement >5 mm.
They recommend that other factors such as concomitant injuries, patient’s age and comorbidities should be considered in the decision for surgery vs conservative approach. For type 1 and type 3 of Anderson and D’Alonzo, there was consensus for initial non-operative management for injuries without gross dislocation or concomitant ligamentous instability.
For displaced type 2 and patients without clinical contraindications/extremely old, surgery was recommended.
5- Avila et al, 2023, performed a systematic review of type II odontoid fractures in patients older than 65 years, with a meta-analysis. 29 Studies were included if they reported more than 5 cases. A total of 46 papers were included with 2822 patients. The mean age was 81.5 ± 3.6 years. Considering age, those in the operative group were younger than those in the non-operative group (81.5 ± 3.5 vs 83.4 ± 2.5 years, P < 0.001). The fusion rate was higher in the operative group (74.3%) compared with the nonoperative treatment (40.3%) (OR 4.27, 95% CI 3.36-5.44). Secondary surgery in patients initially managed nonoperatively was 4.8% (46/964).
The mortality rate was lower in the operative cohort - 16.6% (452/2721) compared with the nonoperative cohort (19.0%) (OR 0.64, 95% CI 0.52-0.80) but complications were higher for those who had surgery (26.0% vs 18.5%) (OR 1.55, 95% CI 1.23-1.95) as well as a higher length of stay (13.6 ± 3.8 vs 8.1 ± 1.9 days, P < 0.001).
The likelihood of stable or unstable nonunion was lower in patients who underwent surgery (OR 0.37, 95% CI 0.28-0.49 vs OR 0.32, 95% CI 0.22-0.47).
They concluded patients who had type II odontoid fractures and were older than 65 years had better fusion rates, but also higher complication rates. Mortality on the other hand was lower – but this can be secondary to selection bias. Non-operative management was safe with a failure rate of less than 5% if we considered that a stable non-union was an acceptable outcome.
6- Huybregts et al, 2023, update their systematic review of 2013. 30 Authors performed a systematic review to evaluate the outcome of surgical and conservative interventions in the elderly (defined as age >65 years) with type 2 and 3 odontoid fractures. A total of 41 studies were included – four prospective and 37 retrospective studies. The primary outcome was clinical outcome, while the secondary outcomes were fracture union and stability. The risk of bias was assessed with Newcastle-Ottawa Quality Assessment Scale – NOS.
Analysis of the clinical outcome was possible in some studies with three valid instruments – the Neck Disability Index (NDI), Visual Analogue Scale (VAS), and Simley-Webster Scale (SWS). There was no clinical difference between the outcome measurements assessed in the systematic review: NDI (700 patients), VAS (180 patients), and Simley—Webster Scale SWS (231) scores between surgical and conservatively managed patients.
Surgically treated patients had higher fracture union compared with non-operative patients (pooled incidence 72.7%, 95% CI 66.1%, 78.5%, 31 studies, 988 patients vs 40.2%, 95% CI 32.0%, 49.0%, 22 studies, 912 patients).
Fracture stability did not differ statistically between treatment groups (41 studies, 1917 patients), although there was a trend to stability in the surgical group.
In conclusion, surgically treated patients had higher rates of union when compared with non-operated patients, but clinically relevant differences were not detected. Data were substantially heterogeneous, limiting the possibilities for analysis and strengths of the recommendations derived from these results.
Summary of the Key Findings of the Six Odontoid Reviews Included.

Abbreviations: SR – systematic review; MA – meta-analysis.
Discussion
Clinical Implications of AO UCIC Modifiers
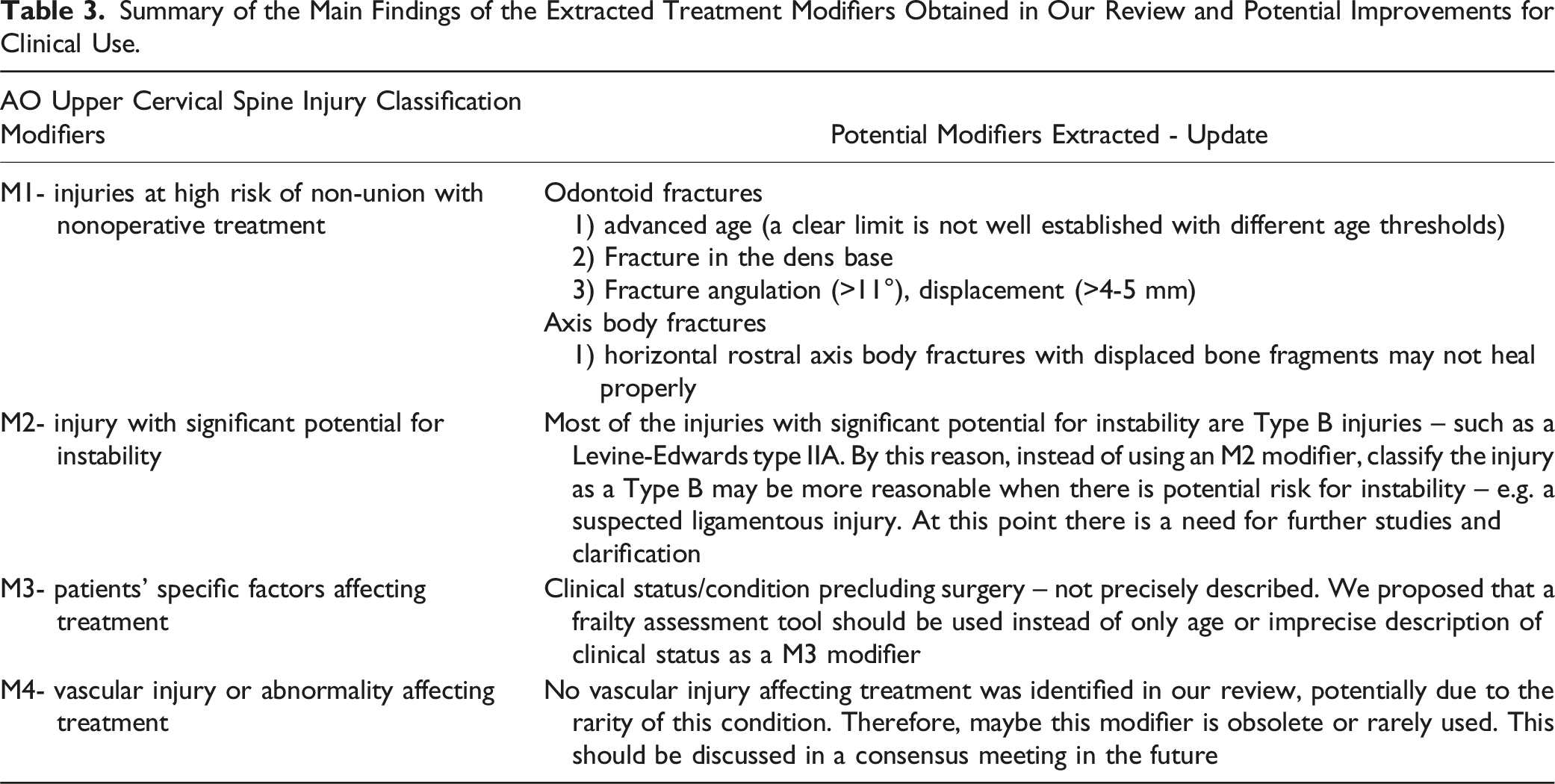
Summary of the Main Findings of the Extracted Treatment Modifiers Obtained in Our Review and Potential Improvements for Clinical Use.
AOSpine UCIC clarifies many issues in the distinction of many morphological patterns, making some of the long-standing controversies redundant. 8 However, the modifiers remain important as they may directly affect the treatment decision in some types of injuries. To adapt the knowledge obtained throughout the years is of paramount importance to increase the utility and validity of the new AO Spine UCIC. 8
For axis body fractures, the Benzel et al. classification was often used. All three types of morphologies proposed by Benzel (type I, II, and III) can be grouped as type A according to the new AO Spine UCIC. 15 This is very reasonable, once most of them can be safely treated non-operatively, as documented in the Kepler et al. systematic review (82.1% of 868 injuries). 13 Some type III with displacement between the fracture fragments (>4 mm), C2-3 subluxation, higher age, comminution, or malalignment were surgically treated in their review. Displacement of fracture fragments and comminution are modifiers suggesting a high risk of pseudoarthrosis (M1). C2-3 subluxation, or malalignment, should assign the injury to type C according to the AO Spine UCIC. Older injuries that are not consolidated generally also would require surgical stabilization.
For Hangman´s fracture, the previous classification of Effendi et al and its modification proposed by Levine-Edwards were the most commonly used systems.5,7 As already mentioned, for those non-displaced injuries (type I and II of both systems), non-operative treatment was well documented and we did not identify any modifier in this injury type, suggesting that non-operative management can be considered in almost all cases. For type IIA of Levine-Edwards, there is C2-3 disc injury with ligamentous disruption, the consolidation rate with non-surgical treatment was low, justifying the assignment of these injuries to type B according to the AO UCIC. For type III classification according to Effendi et al or Levine-Edwards, there is next to ligamentous disruption also facet dislocation making this injury type C in AO UCIC scheme. Surgical treatment is consequently strongly recommended.
Odontoid fractures are the most controversial topic. All the included reviews reported that surgical treatment is a better option to achieve fracture union, especially in elderly patients. So, odontoid fractures in the base of the dens may receive a modifier M1, especially in elderly patients.25-30 Of note, the risk of instability with pseudoarthrosis was not higher in non-operative management of odontoid fractures, as demonstrated by Avila et al. (<5%), but we should consider that most of the included studies were in geriatric odontoid fractures – which may not be applied for young patients with normal bone stock. 29 Besides, better results of surgical treatment might have been related to a selection bias in all the included reviews – as surgery is usually not offered to patients with serious co-morbidities. In the Osterhoff et al. study, authors proposed some classic considerations for surgical treatment such as fracture angulation >11°, displacement of the dens greater than 4-5 mm, and gross displacement of fragments for type 3 of Anderson and D´Alonzo. 28 Of note, this latter is also type 3 of axis body classification proposed by Benzel et al. and was described in the axis body injury as a risk for surgical treatment when displaced fragments were found. 15 For this reason, clinical status was reported as an important modifier for odontoid fractures (M3).
Not mentioned in the reviews but also important, is that surgical treatment should be considered for those injuries with neurological deficits. The AO Spine UCIC algorithm incorporates neurological status in the decision-making. This was not found in the studies included in our review, probably due to the relatively low frequency of neurologic deficits in the upper C-spine as serious neurologic injury is usually fatal at this level (Table 3).
Finally, a summary of the main findings of the extracted treatment modifiers obtained in our review and potential improvements for clinical use are presented in Table 3.
Comparison of AO Spine UCIC with Previous Classification Systems
The AO Spine UCIC system represents a significant improvement over previous classification systems like Anderson and D'Alonzo for odontoid fractures or Levine-Edwards for Hangman’s fractures. These older systems were primarily based on the anatomical location and morphology of the fracture, without taking into account important factors such as the risk of non-union, patient frailty, or the potential for instability. By incorporating modifiers that reflect both the injury and the patient’s specific characteristics, the AO Spine UCIC system offers a more holistic approach to fracture management.
For instance, in the case of Levine-Edwards Type IIA fractures, the AO Spine UCIC system recognizes that ligamentous injury increases the risk of non-union and instability, necessitating surgical intervention in many cases. Similarly, the inclusion of patient-specific factors, such as frailty (M3- patient-specific factors affecting treatment), allows for a more tailored approach to treatment. In older systems, a patient with an odontoid fracture might have been treated conservatively based solely on radiographic findings, but the AO Spine UCIC system considers additional factors that might necessitate surgical treatment to prevent complications. This shift towards a more nuanced classification system enhances the ability to personalize care and improve patient outcomes.
Frailty Over Age: A Critical Modifier
While age has traditionally been used as a key determinant in the management of cervical spine injuries, frailty offers a more comprehensive and clinically relevant measure of a patient’s capacity to recover from injury. Frailty, as assessed by the Modified Frailty Index (mFI), provides a multidimensional view of a patient’s physiological reserve, taking into account factors such as comorbidities, functional status, and overall resilience. 31 This concept has already been incorporated into the AO Spine-DGOU OF (Osteoporotic Fracture) Score for osteoporotic vertebral fractures, where frailty is a critical determinant of treatment outcomes. 32
In the context of axis fractures, frailty is probably a far better predictor of complications and recovery potential than chronological age alone. Older patients may be at higher risk for non-union or complications due to decreased bone quality and comorbidities, but it is the degree of frailty—rather than age itself—that should guide treatment decisions. For instance, a robust 70-year-old patient with few comorbidities may tolerate surgery well, while a frail 65-year-old patient may have poor outcomes even with conservative management. Incorporating frailty assessments, as a more reliable way to evaluate the M3 modifier, like the mFI into the AO Spine UCIC classification system would improve the precision of treatment decisions, ensuring that patients receive care that is appropriate for their overall health status rather than their chronological age.
Limitations in the Available Evidence
The use of previous systematic reviews instead of isolated case series is a limitation of this study that may affect specifically the odontoid reviews because some patients may be counted twice. However, due to the qualitative analysis of this review, it may not bias the identification of factors that affect management. Besides, this review provides a comprehensive evaluation of the literature once we extract the most important data from each included review. Additionally, the lack of systematic reviews about axis body fracture and Hangman´s fractures, which only one study, suggested that this field needs to be better explored. Finally, most of the odontoid studies only evaluated the role of age in fracture consolidation. It is well known that age is a risk for pseudoarthrosis, but the impact of non-healed odontoid fracture may not be as relevant as we believed in the past. A significant challenge in interpreting the current body of literature on axis fractures is the quality of available evidence. The majority of the studies included in systematic reviews is retrospective and often suffer from selection bias, where healthier patients are more likely to undergo surgery, while more frail or comorbid patients are managed non-operatively. This bias skews the results, as surgical patients may appear to have better outcomes due to their better baseline health, rather than the superiority of surgical intervention itself. In reviews of odontoid fractures, patients undergoing surgery are often those with fewer comorbidities, making it difficult to draw firm conclusions about the benefits of surgical treatment across all patient populations.
Moreover, the methodological limitations of many included studies, as assessed by the AMSTAR 2 tool, raise concerns about the reliability of some findings. The low to moderate quality of most reviews, particularly those focusing on non-surgical management, suggests that the evidence supporting the use of certain modifiers is not as robust as desired. Many studies lack control groups, long-term follow-up, or adequate sample sizes, making it difficult to definitively assess the impact of modifiers on patient outcomes. It is important to emphasize that the M4 modifier was not mentioned in the reviewed literature. Future research must focus on high-quality, prospective studies that can provide more definitive answers regarding the role of these modifiers in clinical decision-making.
Conclusions
We identify many axis injury characteristics that may affect final treatment. A better understanding of these modifiers may improve the use of the system.
This umbrella review highlights the importance of modifiers in the management of traumatic axis fractures, as integrated into the AO UCIC classification system. The identified modifiers—non-union risk, instability, and patient-specific factors such as frailty— play a pivotal role in guiding treatment decisions. Notably, frailty offers a more accurate predictor of treatment outcomes than chronological age, particularly in older patients with odontoid fractures. Incorporating frailty assessments, like the Modified Frailty Index, into treatment algorithms may further enhance the system’s clinical utility.
While the AO Spine UCIC system represents a significant advancement by including patient-specific modifiers, the quality of existing evidence remains a concern, especially regarding odontoid fractures. High-quality prospective studies are needed to validate and especially specify these modifiers to refine clinical guidelines further.
Supplemental Material
Supplemental Material - The AO Spine Upper Cervical Injury Classification System (AO UCIC) – An Umbrella Review of Traumatic Axis Injuries Factors that May Affect Treatment Decision
Supplemental Material for The AO Spine Upper Cervical Injury Classification System (AO UCIC) – An Umbrella Review of Traumatic Axis Injuries Factors that May Affect Treatment Decision by Andrei F. Joaquim, Sebastian F. Bigdon, Gaston Camino-Willhuber, Cumhur F. Öner, Klaus J. Schnake, Richard Bransford, Harvinder Singh Chhabra, Mohammad El-Skarkawi, Alexander R. Vaccaro, Gregory D. Schroeder, and On behalf of the AO Spine Knowledge Forum Trauma & Infection in Global Spine Journal.
Footnotes
Acknowledgments
The AO Spine Injury Classification Systems were developed and funded by AO Spine through the AO Spine Knowledge Forum Trauma, a focused group of international spine trauma experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically guided not-for-profit organization. Study support was provided directly through AO Network Clinical Research and AO ITC, Clinical Evidence.”
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: I'm currently an AO Spine Trauma Knowledge Forum Steering Committee Member.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.