
Abstract
Study Design:
Retrospective radiographic investigation.
Objective:
To evaluate the long-term radiographic and functional outcomes of patients in whom there is absence of radiographic union at 2 years after single-level anterior cervical discectomy and fusion (ACDF).
Methods:
Thirty-one patients were evaluated at standard postoperative time intervals per index trial protocol. Plain film radiographic fusion criteria at the arthrodesis level was defined as interspinous motion (ISM) <1 mm with corresponding motion at a non-arthrodesed superjacent level ISM ≥4 mm. Radiographs and functional outcome measures were acquired at each follow-up visit. Delayed union was defined as lack of radiographic union by 24 months.
Results:
Nine patients demonstrated radiographic evidence of delayed radiographic union at 24 months. Of those 9 patients, 5 patients demonstrated evidence of union during the follow-up period to 72 months. Despite the absence of radiographic union based on our criteria, 3 of the 4 remaining patients reported remarkable improvements in pain scores and functional outcomes.
Conclusions:
The natural history of delayed union at 24 months after ACDF was still favorable despite the prolonged delay in union. The majority of patients (5 of 9) without radiographic union at 24 months did proceed to radiographic union by final follow-up. In addition, patients that did not meet our criteria for fusion maintained postoperative improvements in patient-reported outcome scores. In summary, our study patients undergoing a single-level ACDF with asymptomatic radiographic delayed union at 24 months can expect maintained improvements in postoperative patient-reported outcomes scores and can still progress to successful radiographic fusion.
Introduction
The gold-standard procedure for the treatment of symptomatic radiculopathy and myelopathy resulting from cervical disc disease that is refractory to nonsurgical management is anterior cervical discectomy and fusion (ACDF). The effectiveness of ACDF for providing durable improvement in patient-reported outcome scores has been well detailed in multiple studies. 1 –3 Despite the success of ACDF, nonunion, also referred to as pseudarthrosis (PA), is a known complication of ACDF and can negatively affect clinical outcomes. 4,5 There is a relative lack of consensus in the literature regarding criteria for the diagnosis of PA, and there is currently no consensus on the management of asymptomatic patients who have delays in radiographic union. 6 –8 A routine treatment currently utilized for the management of symptomatic PA is repeat surgical intervention with the goal of obtaining arthrodesis. A study by van Eck et al reported that among 672 patients undergoing ACDF, the reoperation rate was 15% within an average of 31 months of follow-up, and PA was the reason for reoperation in nearly half of patients. 9 However, reoperations due to PA expose the patients to the risks of reoperation from revision anterior cervical approaches, posterior cervical approaches, and potentially iliac crest autologous bone harvest. 10,11 In addition, there is a lack of available evidence describing the natural history of graft healing in cases of delayed union, making the prediction of long-term outcomes in patients without radiographic union at 1 or 2 years postoperatively difficult to determine. The purpose of this study is to evaluate the long-term radiographic and functional outcomes of patients with delayed union at 2 years postoperatively after a single-level ACDF.
Materials and Methods
Subjects
This study was a retrospective radiographic investigation of patients enrolled through a prospective, single-center, randomized controlled trial investigating the efficacy of P-15 peptide for single-level cervical fusion. To minimize the confounding effects of a novel bone graft extender on fusion rates, only the control group was analyzed for this study. All patients in the control group received autologous bone graft packed in an allograft cortical ring for interbody fusion. Following central and foraminal decompression, the endplate distraction using Caspar pins was maintained and a structural fibular ring allograft was selected based on trials that provided good cortical contact without excessive force required for insertion. Local autograft from osteophyte resection earlier in the case was morselized and placed within the allograft. Next, the allograft was inserted into the interspace and recessed approximately 1 mm posterior to the anterior vertebral cortex. This was followed by anterior cervical plating with 13 mm screws in the cephalad and caudad vertebral bodies. Postoperative immobilization of the cervical spine was performed at the discretion of the treating surgeon. All patients were evaluated at standard postoperative time intervals at 6 weeks, 3 months, 6 months, 9 months, 12 months, 18 months, 24 months, and then annually up to 72 months as per index trial design protocol. At each visit, flexion, extension, lateral, and upright AP views of the cervical spine were acquired. Visual Analogue Scale (VAS) scoring of the neck and arm/shoulder, as well as a neurological exam, was performed at baseline, immediately following intervention, and at the aforementioned standard follow-up intervals. Neck Disability Index (NDI), SF-36 scores, and the patient’s rating of outcome using the modified Odom’s criteria were performed at baseline, immediately following intervention, at 6 weeks, 9 months, 12 months, 18 months, 24 months, and each subsequent annual visit up to 72 months. Adverse events were monitored and collected during the entire length of the study.
Inclusion Criteria
Patients between the ages of 18 and 65 with radiographic evidence of degenerative disc disease (degenerative disc on magnetic resonance imaging [MRI], decreased disc height compared to adjacent levels on radiographic film, computed tomography [CT], or MRI, or disc herniation on CT or MRI) with a planned 1-level ACDF were screened to enter the study. In order to be a candidate for this trial, patients were required have one or more of the following radiculopathy and/or myelopathy exam findings: arm/shoulder pain, decreased reflexes, decreased strength, and/or abnormal sensation. Preoperative pain scores at the level of arm/shoulder and/or the neck were required to be greater than 4 on a 0 to 10 visual analog scale as well as an NDI score greater than 30 for enrollment in the trial.
Exclusion Criteria
Patients were excluded from the clinical trial if there was evidence of systemic infection (such as AIDS, HIV, or active hepatitis), significant metabolic disease, taking medication for the prevention of osteoporosis, cardiovascular or pulmonary disease that could cause excessive surgical risk, active malignancy, multilevel symptomatic cervical disease present, history of a prior cervical fusion and/or prior cervical decompression at the index level, history of acute cervical trauma or instability as the result of trauma, patients with a history of ongoing treatment for tumor or bone injury as the result of trauma in the cervical spine, and patients that were deemed to require both anterior and posterior cervical procedures to treat their disease process (Table 1). Also, patients were excluded if there was a history of substance abuse, they were imprisoned at the start of the study, or if they were currently involved in a study of another investigational product for a similar purpose.
Baseline and 24-Month Follow-up Patient-Reported Outcome Scores for Union and Delayed Union Groups.
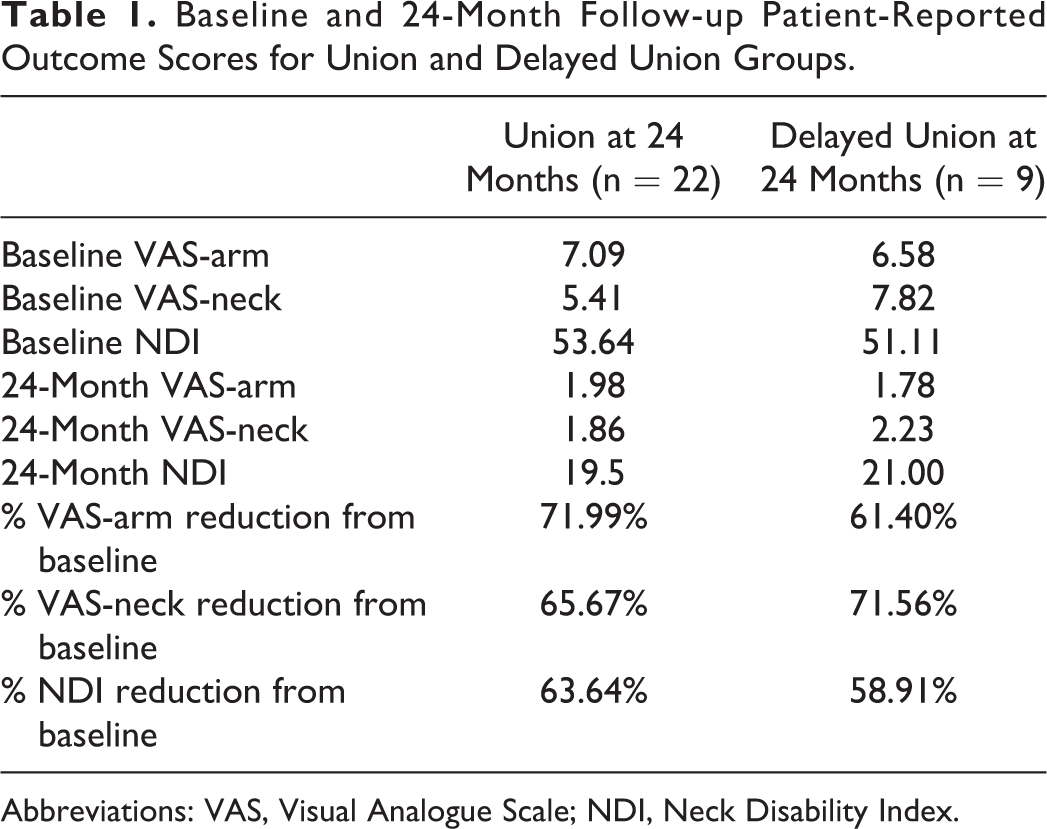
Abbreviations: VAS, Visual Analogue Scale; NDI, Neck Disability Index.
Data Analysis
The criteria used in this study utilized interspinous motion (ISM) at the arthrodesis level and the cephalad adjacent level. The widely recognized and Cervical Spine Research Society endorsed criteria published by Riew et al was utilized to assess arthrodesis. 12 The plain radiographic ISM criteria for fusion at the arthrodesis level was defined as ISM <1 mm, and at a non-arthrodesed superjacent level was defined as ISM ≥4 mm, based on 150% magnified dynamic radiographs stored in PACS. The criterion of non-arthrodesed superjacent ISM was utilized to establish whether the patient flexed and extended his/her neck sufficiently.
A significant number of the radiographs obtained were in nondigitized form. These films were digitized using a digital camera, tripod, and lightbox. The camera was positioned the same distance, approximately 24 inches, away from each radiograph to ensure standardized magnification. Once all radiographs were digitized, the image processing program ImageJ, developed by the National Institutes of Health, was used to measure ISM. The screw length of 13 mm was used to normalize the radiographs to control for magnification error in radiographic technique. ISM was measured using the distance between the most identifiable landmark around the tip of the spinous processes at the operative level. This distance was measured on both flexion and extension radiographs, and then the extension interspinous distance was subtracted from the flexion interspinous distance to yield the ISM at the operative level. This calculation was also performed at a non-arthrodesed superjacent level using flexion and extension views. Patients demonstrated delayed union if ISM at the arthrodesis level was ≥1 mm and/or ISM at a non-arthrodesed superjacent level was <4 mm by 24 months.
Patient-reported outcome measures, including VAS-arm, VAS-neck, and NDI were collected preoperatively and during each follow-up visit postoperatively, including 6 weeks, 3 months, 12 months, and yearly thereafter to 5 years postoperatively. After creation of union and delayed union groups, as determined by union status at 24 months, each group’s baseline patient-reported outcome data was compared to the 24-month follow-up scores using paired student t tests. Furthermore, 24-month patient-reported outcomes were compared between union versus delayed union groups using a Mann-Whitney U test due to small sample sizes precluding standard parametric assumptions. Further subgroup analysis within the delayed union group at 24 months was avoided due to small sample sizes and the long-term results of patients within this group is presented for review in a descriptive fashion.
To determine whether the observed changes in patient-reported outcome scores displayed clinically significant improvements, previously published literature on minimum clinically important difference (MCID) was reviewed. Parker and colleagues evaluated MCID values after ACDF for cervical radiculopathy, suggesting improvements of 2.6 and 4.1 (10-point scale) points for VAS-neck and VAS-arm, respectively, and 17.3-point improvement in NDI met thresholds for clinically significant improvements. 13 Similarly, Auffinger and colleagues evaluated MCID values after ACDF for cervical myelopathy, noting improvements of 3.1 (10-point scale) points for VAS-neck and 13.39-point improvement in NDI met thresholds for clinically significant improvements. 14
Results
Of the 34 patients in the control (autologous bone placed into interbody graft) group, 3 patients were either lost to follow-up or had poor film quality, rendering an analysis of ISM impossible. One patient was lost to follow-up at 6 months, but at the 3-month visit reported complete reduction in arm/shoulder and neck pain VAS. Another patient was lost to follow-up at 18 months, but at the 12-month visit reported complete reduction in arm/shoulder and neck pain VAS and a 94% reduction in NDI (went from a score of 36 to 2). The last patient withdrew after the 24-month visit due to adjacent level pathology and sought treatment with another local physician and the patient’s arm/shoulder and neck pain VAS and NDI were approximately the same at 12 months compared to the baseline value. Radiographs were not analyzed at this visit due to poor quality.
At 24 months, 71% (22/31) of patients had demonstrated evidence of union, while 29% of patients (9/31) demonstrated some evidence of delayed union by the metrics defined herein. Of these 9 patients, 5 had ISM ≥1 mm at the arthrodesis level only, 3 had ISM <4 mm at a non-arthrodesed superjacent level only, and 1 had both ISM ≥1 mm at the arthrodesis level and ISM <4 mm at a non-arthrodesed superjacent level (Figures 1 and 2).
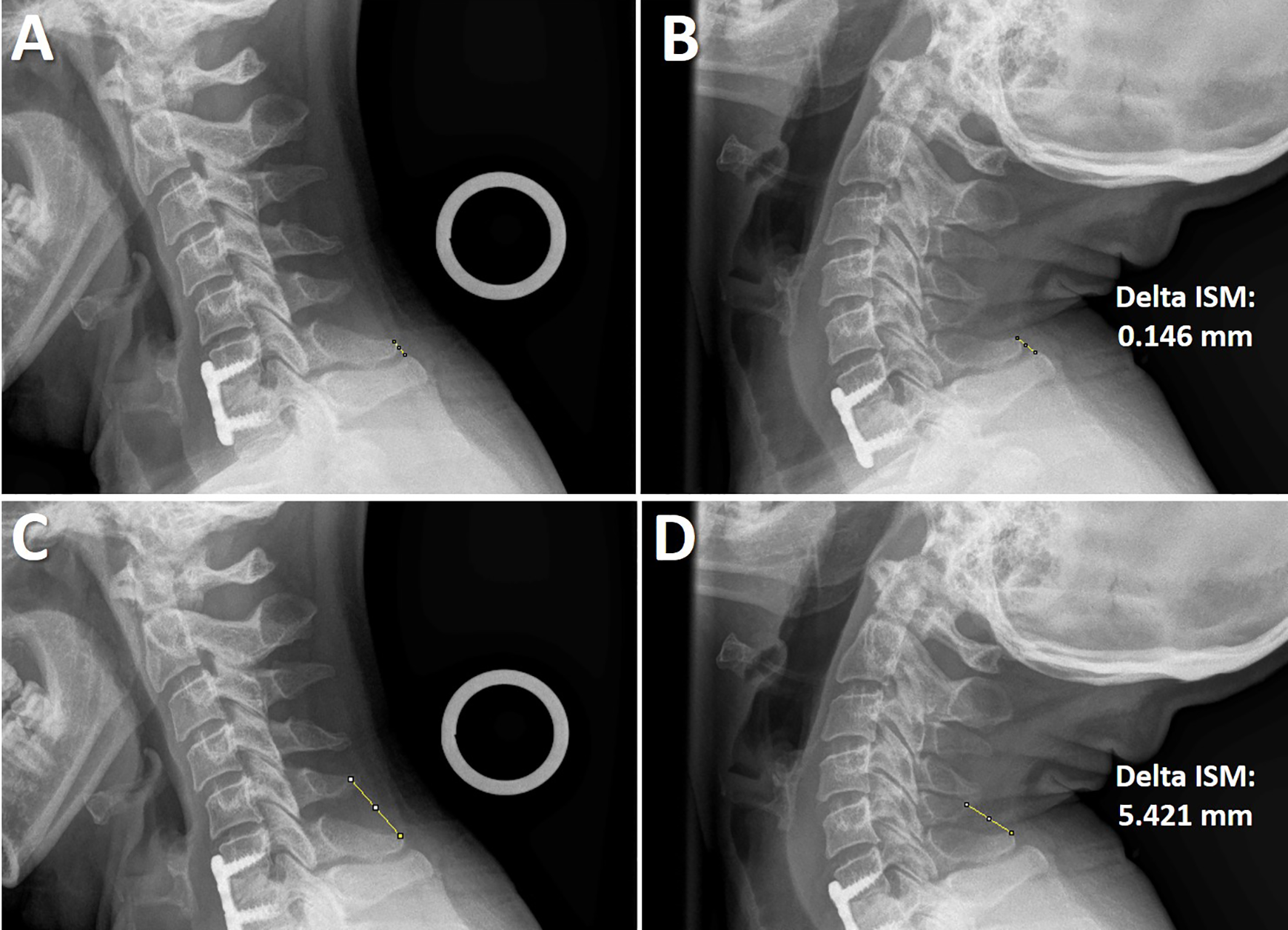
Twenty-four-month follow-up flexion and extension X-rays for a patient with radiographic union. “A” and “B” demonstrate examples of interspinous motion (ISM) measurements on flexion and extension, respectively, at the level of surgery. The absolute difference between these values is 0.146 mm. “C” and “D” demonstrate examples of ISM measurements on flexion and extension, respectively, at the cephalad adjacent level. The absolute difference between these values is 5.421 mm.
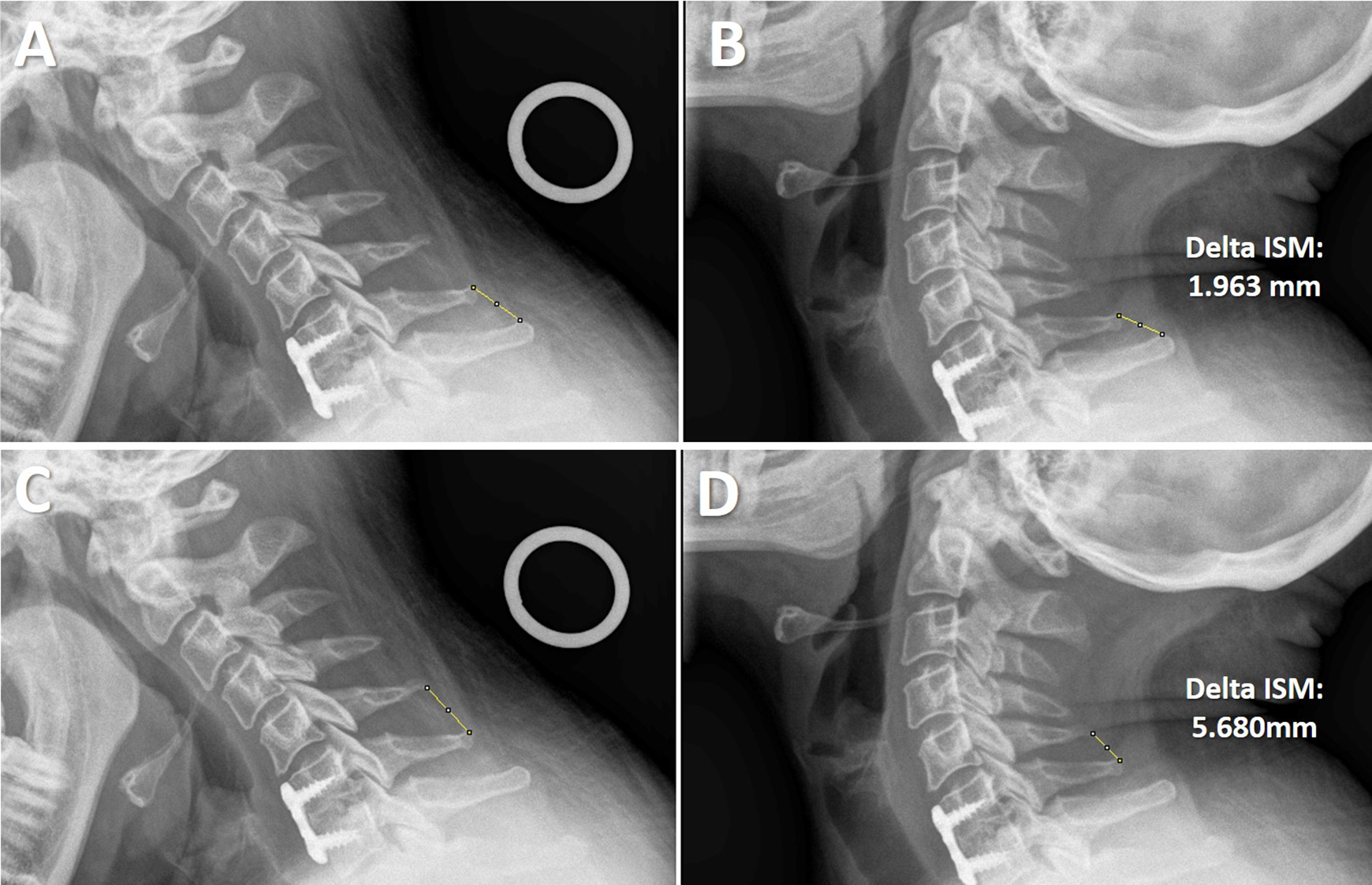
Twenty-four-month follow-up flexion and extension X-rays for a patient with radiographic delayed union. “A” and “B” demonstrate examples of interspinous motion (ISM) measurements on flexion and extension, respectively, at the level of surgery. The absolute difference between these values is 1.963 mm. “C” and “D” demonstrate examples of ISM measurements on flexion and extension, respectively, at the cephalad adjacent level. The absolute difference between these values is 5.680 mm.
Both union and delayed union at 24-month groups demonstrated significant improvements in VAS-neck, VAS-arm/shoulder, and NDI scores when compared to preoperative scores (paired t test; P < .0001 for all 3 variables). Additionally for both the union and delayed union groups, the average reported improvements for VAS-neck, VAS-arm/shoulder, and NDI scores between baseline and 24-month follow-up visits were greater than previously reported values for reaching MCID thresholds, suggesting significant clinical improvements in all patient-reported outcomes. Furthermore, no significant difference was found between the groups for VAS-neck, VAS-arm/shoulder, or NDI scores at 24 months (Mann-Whitney U test; P = .562, P = .562, P = .779, respectively; Table 1).
Of the 9 patients without evidence of union at 24 months, 5 patients demonstrated evidence of union during the follow-up period to 72 months. Three patients demonstrated ISM <1 mm at the arthrodesis level and ISM ≥4 mm at a non-arthrodesed superjacent level at 36 months, 1 patient demonstrated union at 48 months, and 1 patient demonstrated union at 60 months (Table 2). The remaining 4 patients lacked evidence of radiographic union through the 72-month follow-up period. Two patients had ISM ≥1 mm at the arthrodesis level with ISM ≥4 mm at a non-arthrodesed superjacent level, while the other 2 patients had ISM <1 mm at the arthrodesis level with ISM <4 mm at a non-arthrodesed superjacent level (Table 3). Despite their lack of radiographic union, 3 of the 4 patients reported remarkable improvements in pain scores and functional outcomes, while 1 patient reported substantial pain and poor function based on VAS and NDI scores at 6 weeks follow-up and continued to report scores with minimal changes in outcome scores during scheduled follow-ups out to 72 months follow-up (Table 4).
Delayed Union in Patients Demonstrating Pseudarthrosis at 24 Months.
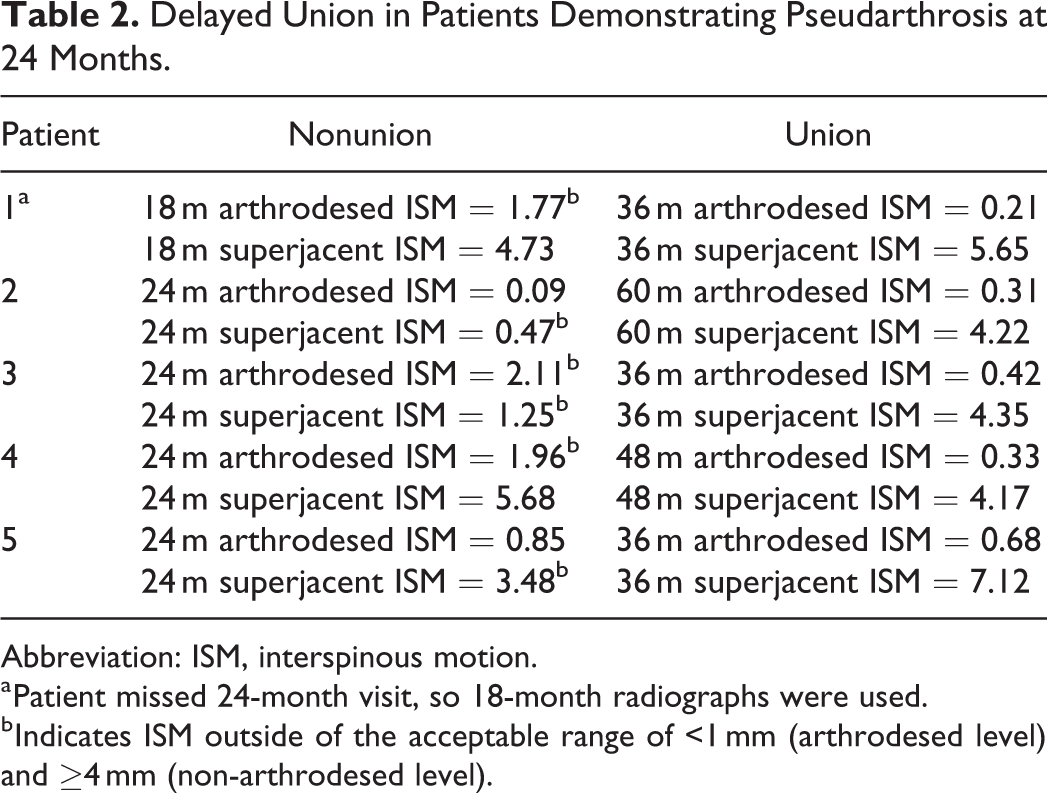
Abbreviation: ISM, interspinous motion.
a Patient missed 24-month visit, so 18-month radiographs were used.
b Indicates ISM outside of the acceptable range of <1 mm (arthrodesed level) and ≥4 mm (non-arthrodesed level).
Nonunion in Patients Demonstrating Pseudarthrosis at 24 Months.
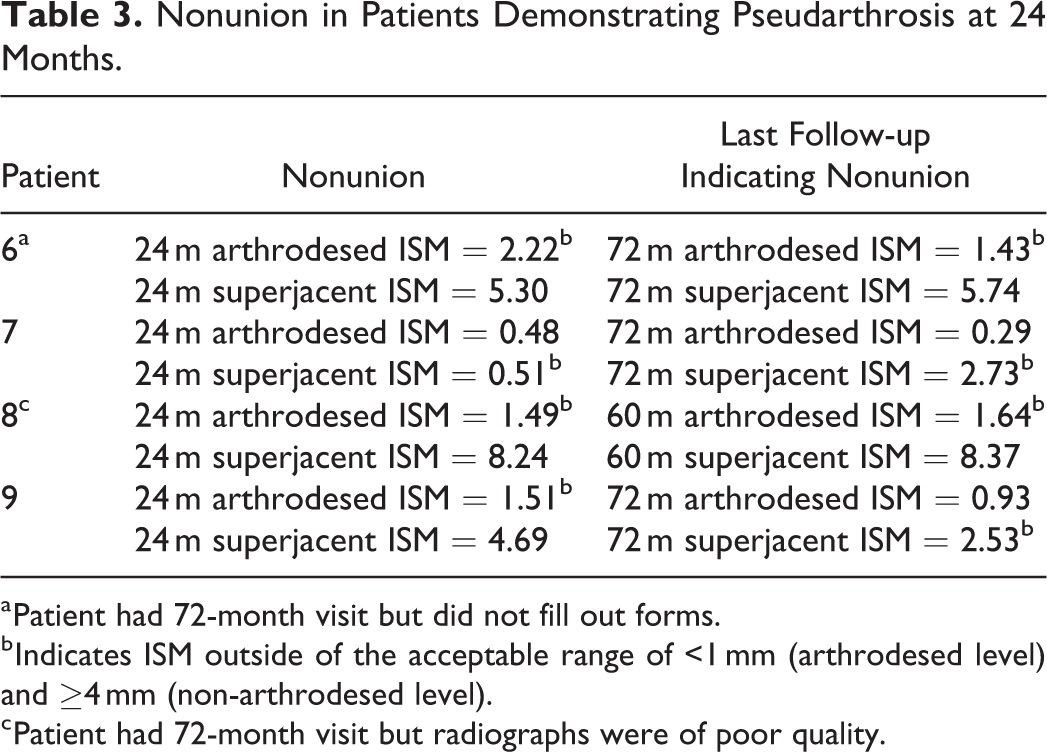
a Patient had 72-month visit but did not fill out forms.
b Indicates ISM outside of the acceptable range of <1 mm (arthrodesed level) and ≥4 mm (non-arthrodesed level).
c Patient had 72-month visit but radiographs were of poor quality.
Clinical Outcomes for Patients With Evidence of Nonunion After 72 Months of Follow-up.
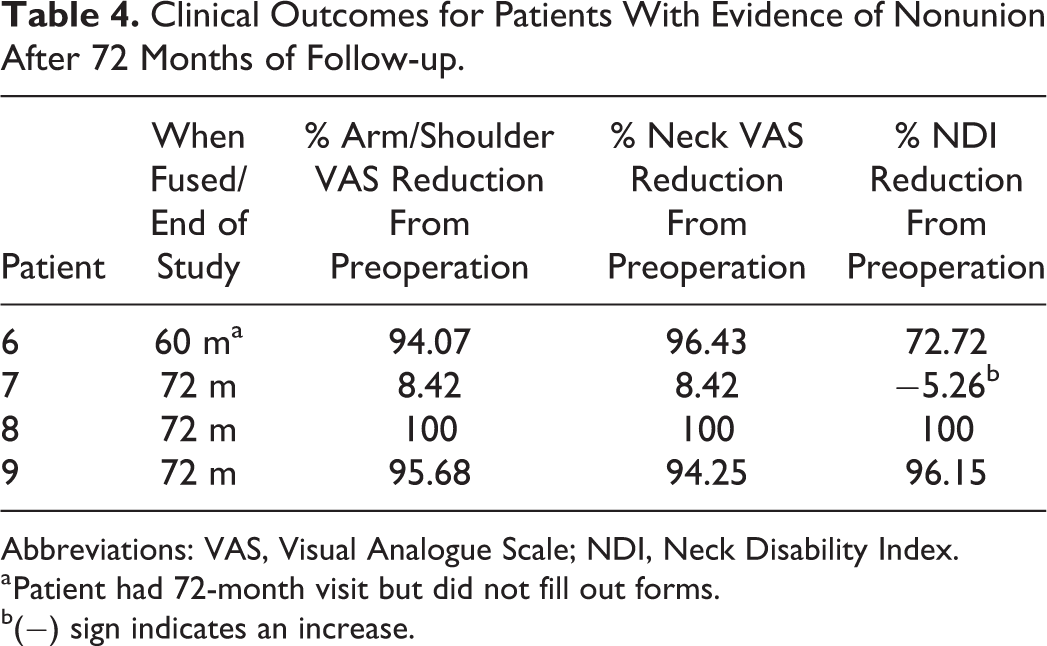
Abbreviations: VAS, Visual Analogue Scale; NDI, Neck Disability Index.
a Patient had 72-month visit but did not fill out forms.
b(−) sign indicates an increase.
Discussion
Our results suggest that patients delayed union at 2 years after ACDF can expect maintained patient-reported outcome scores and can potentially proceed to radiographic union without further operative intervention. Our study found that 5 of 9 patients without radiographic signs of union at 2 years postoperatively progressed to radiographic union without further surgical intervention. Furthermore, the 4 patients who did not proceed to radiographic union after 5 years did not see any decreases in patient-reported outcome scores between 2-year to 5-year follow-up.
A recent meta-analysis of PA rates for ACDF by Shriver et al reported an overall PA rate of 3.1% and 2.3% for studies with 12- to 24-month follow-up and greater than 24 months follow-up, respectively. However, significant heterogeneity for fusion assessment criteria was reported, and of the reported definitions used, none of the included 17 studies reported a >1 mm of ISM at the operative level as a threshold for delayed union or PA. 15 Additionally, minimal comparative literature exists that discuss the natural history of delayed union with ACDF. A comparable study to our current study was recently performed by Lee and colleagues reviewed 1- to 3-level ACDFs using cortical ring allografts and anterior cervical plating. Using a stringent definition of delayed union, defined as any findings of >1 mm change in ISM at the operative level, absence of bridging bone across the endplates, or radiolucent lines >50% from the cortical-host bone interface on CT or X-ray, they reported an overall 32.6% delayed union rate at 1 year postoperatively (15/51 single level, 9/26 2-level ACDFs, and 5/12 3-level ACDFs). The delayed unions were followed to 2 years postoperatively with 72.4% of delayed unions at 1 year eventually reaching union at 2 years without subsequent intervention. They further noted persistent delayed unions at 2 years displayed significantly less postoperative improvement in NDI and VAS-neck compared to union at 2 years, but similar overall improvements in VAS-arm scores between groups. 16
The effectiveness of ACDF treatment for cervical radiculopathy secondary to spondylosis has been well described. 17 There have been several studies that have examined the outcomes of surgical management of cervical PA, but few studies have considered the outcome of expectant management for asymptomatic patients without radiographic fusion at expected time points. Currently, there are no universally agreed upon diagnostic radiographic or clinical criteria for PA. Several sets of criteria have been used to assess fusion status based on radiographic evidence. 6 –8,18 The plain radiographic ISM criteria for fusion at the arthrodesis level was defined in this study as ISM <1 mm, and at a non-arthrodesed superjacent level was defined as ISM ≥4 mm. This set of criteria is endorsed by the Cervical Spine Research Society and is well-accepted in the literature. 12,17,19 It is worth noting that our criteria are more stringent than other radiographic fusion criteria and have been demonstrated to correlated with CT-based assessments, as alternative metrics used in published literature define fusion as less than 3 mm or 4 mm of ISM at the index operative level. 20,21 This may have led to our higher delayed union rate for 1-level ACDF at 2 years than otherwise reported in the literature. Less stringent criteria, though more inclusive, may create the need for CT-based assessment, which can be costly and generates greater radiation exposure. 17 However, Park and colleagues suggested CT scans may overestimate fusion rates, with 23% to 41% of levels thought to be fused on CT scans demonstrating persistent motion on dynamic X-rays. 22
There are several limitations with our study. As the study sample only included cortical allograft interbody grafts, we cannot extrapolate our results to prosthetic intervertebral cages, such as PEEK or titanium cages. Allograft subsidence is a common finding and grafts may soften and lose height over time, resulting in delayed radiographic healing during this phase. Additionally, high graft resorption rates have been reported for dense cancellous allografts (53% of grafts displaying resorption by 15 months) and similar resorption effects may take place with cortical grafts over time. 23 Similar delayed union scenarios with prosthetic cages may not demonstrate our observed results of delayed healing effect seen with cortical allograft. Furthermore, small sample sizes limit rigorous statistical analysis of our data, and accordingly, we report our data in a descriptive fashion. Furthermore, stringent inclusion and exclusion criteria for the trial limit the extent to which the results can be generalized. The criteria utilized herein could potentially exclude patients who have gone on to radiographic union, but do not have adequate effort to yield a result of ISM ≥4 mm at a non-arthrodesed superjacent level, even though they have ISM <1 mm at the arthrodesis level. This occurred in 2 of the 4 patients that demonstrated nonunion (patients 7 and 9 in Table 3). As seen in Table 4, patient 7 demonstrated a slight increase in NDI. However, this patient experienced several confounding adverse events, most notably a motor vehicle accident between 6 and 9 months postoperatively. In contrast, though patient 9 did not demonstrate union based on our criteria, the patient reported a 96% decrease in NDI. Furthermore, patients 6 and 8 demonstrated 72% and 100% reductions in NDI even though they did not demonstrate union based on our radiographic criteria. This, as well as the fact that NDI has been shown to sufficiently evaluate and represent a patient’s physical and mental quality of life, suggests that fusion status alone may not be a significant predictor of successful outcome. 24 Although our small sample sizes are small, we believe the rigorous patient selection, data collection, and postoperative follow-up monitoring afforded by the clinical trial creates high-quality data. Because the sample sizes were small, we avoid ascribing statistical significance to our findings and instead focus on descriptive reporting our experience with delayed union in ACDF due to the paucity of data available to clinicians for decision making in this difficult scenario.
Conclusion
Though little is known about the natural history of delayed radiographic union, our study suggests patients with initial delays in union can proceed to eventual radiographic union. In addition, even the patients that did not meet our criteria for radiographic union maintained their postoperative patient-reported outcome scores. These findings suggest that patients after a single-level ACDF who demonstrate a 2-year delay in radiographic union may still progress to successful radiographic union and can expect maintained functional outcomes regardless of union status.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Cerapedics funds were received in support of this work.