
Abstract
Study Design:
Retrospective cohort study.
Objectives:
Decompression without fusion is a standard surgical treatment for lumbar spinal stenosis (LSS) with reasonable surgical outcomes. Nevertheless, some studies have reported low patient satisfaction (PS) following decompression surgery. The cause of the discrepancy between reasonable clinical outcomes and PS is unknown; moreover, the factors associated with PS are expected to be complex, and little is known about them. This study aimed to identify satisfaction rate and to clarify the factors related to PS following decompression surgery in LSS patients.
Methods:
We retrospectively reviewed 126 patients who underwent lumbar decompression with a minimum follow-up of 1 year. Patients were divided into 2 groups based on the PS question. The Japanese Orthopaedic Association (JOA) scores, and the Numeric Rating Scale (NRS) scores of low back pain (LBP), leg pain, and leg numbness were compared between the 2 groups preoperatively and at the latest visit. To identify the prognostic factors for dissatisfaction, multiple logistic regression analysis was performed.
Results:
Overall satisfaction rate was 75%. The JOA recovery rate, NRS improvement, and Short Form–8 (SF-8) were significantly higher in the satisfied group. Postoperative NRS scores of LBP, leg pain, and leg numbness were significantly lower in the satisfied group. Multivariate logistic regression analysis showed that smoking and scoliosis were significant risk factors for dissatisfaction.
Conclusions:
Overall satisfaction rate was 75% in patients with LSS undergoing decompression surgery. This study found that smoking status and scoliosis were associated with patient dissatisfaction following decompression in LSS patients.
Keywords
Introduction
Lumbar spinal stenosis (LSS) is a common disease that causes leg pain, intermittent claudication, and low back pain (LBP). Surgical treatment is necessary if symptoms are not relieved with conservative treatments. Decompression without fusion is a standard surgical treatment for LSS; several studies showed improved surgical outcomes using various outcome measures, such as the Oswestry Disability Index (ODI), Roland Morris Disability Questionnaire, Japanese Orthopaedic Association (JOA) score, or JOA Back Pain Evaluation Questionnaire (JOABPEQ). However, some studies reported low patient satisfaction (PS). Katz et al 1 reported that 22% of patients were not satisfied after surgery. Other reports also showed that 10% to 20% of patients were dissatisfied after surgery. 2 -4 This discrepancy may be because of the fact that outcome measures used in these studies do not reflect PS.
Over the past decades, PS is becoming increasingly important as an index for fulfilling patients’ expectations. The factors associated with PS are expected to be complex, and little is known about them. Especially in LSS, it is difficult to understand which factors influence PS because patients have a wide range of symptoms preoperatively, and some of the symptoms could be residual postoperatively. Furthermore, patients with LSS have various radiographic findings because of its degenerative nature. To provide better care, it is extremely important to clarify the factors that influence PS in LSS patients following decompression surgery. The purpose of this study was to investigate the causative factors for PS in patients with LSS who underwent decompression surgery without fusion.
Materials and Methods
Subjects
We recruited LSS patients who underwent lumbar decompression without fusion between January 2014 and March 2016. Decompression surgery was performed as previously described. 5 Patients were included if they fulfilled the following criteria: minimum one-year follow-up, no intervertebral instability (an intervertebral angle change of <10° on preoperative functional radiographs and no spondylolisthesis of grade 2 or above), scoliosis with a Cobb angle of <15°, and available preoperative and final follow-up questionnaires. Revision cases were excluded from the cohort. Informed consent was obtained from all participants. Our hospital institutional review board approved this study. In total, we evaluated 126 patients (80 males and 46 females). The patients’ mean age at the time of surgery was 69.4 years (range 27-89 years). The mean follow-up period was 24.6 months (range 12-37 months).
Patient Satisfaction
Patients were divided into satisfied (S) and dissatisfied (D) groups based on the question, “How satisfied are you with the overall result of your back operation?,” which was quoted from Zurich Claudication Questionnaire (ZCQ). Patients who answered “very satisfied” or “somewhat satisfied” were allocated into the S group whereas patients who answered “very dissatisfied” or “somewhat dissatisfied” were allocated into the D group.
Clinical Outcomes
We evaluated the JOA score, the Numeric Rating Scale (NRS) scores of LBP, leg pain, and leg numbness preoperatively and at the latest visit. The JOA recovery rate was calculated as (postoperative JOA score − preoperative JOA score) / (29 − preoperative JOA score) × 100 (%). 6
We used the Short Form–8 (SF-8) Health Survey 7 to evaluate health-related quality of life (HRQOL) preoperatively and at the latest visit. The SF-8 has 8 domains, which were summarized into physical component summary (PCS) and mental component summary (MCS), with a higher score indicating a better outcome.
Statistical Analysis
Difference between the 2 groups was analyzed using Fisher exact probability test or Mann-Whitney U test depending on the variable type. Fisher exact probability test or one-way analysis of variance (ANOVA) was performed to compare the variables between the 4 satisfaction subgroups based on the variable types. The Spearman’s rank correlation coefficient was used to discover the strength of a correlation between PS and other variables. Multiple logistic regression analysis with adjusted odds ratios was performed to identify the associations between baseline parameters and postoperative satisfaction. All parameters were analyzed individually and adjusted for potential confounders. All statistical analyses were performed using SPSS Statistics 25 (IBM Corp, Armonk, NY, USA). A P value of <.05 was considered as statistically significant.
Results
Difference in Preoperative Background Characteristics Between the 2 Groups
Of 126 patients, 95 (75%) were satisfied and 36 were dissatisfied; there were 42 “very satisfied” and 53 “somewhat satisfied” patients in the S group whereas there were 6 “very dissatisfied” and 25 “somewhat dissatisfied” patients in the D group. The patients’ background characteristics are shown in Table 1. The percentage of smokers was significantly higher in the D group (29.0%) than that in the S (10.5%) group (P = .015). There was no difference in age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) grade, and drinking status between the 2 groups. Next, we stratified the patients according to the presence of anterior spondylolisthesis, posterior spondylolisthesis, and mild scoliosis with a Cobb angle between 10° and 15°. The presence of mild scoliosis was related to PS (P = 0.004). Interestingly, no association was found between anterior or posterior spondylolisthesis and PS.
Background Characteristics in Each Group.
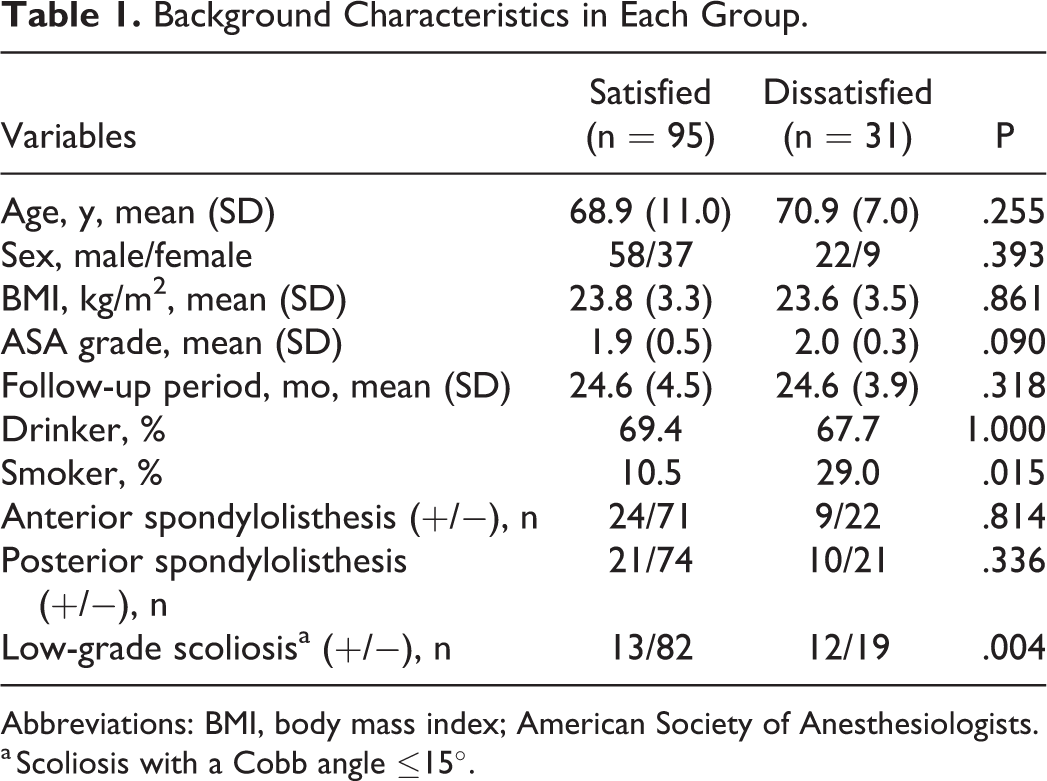
Abbreviations: BMI, body mass index; American Society of Anesthesiologists.
a Scoliosis with a Cobb angle ≤15°.
Difference in Preoperative Symptoms Between the 2 Groups
We compared the preoperative symptoms between the 2 groups using the JOA score, NRS scores of LBP, leg pain, and leg numbness, and SF-8 score. No difference was observed in preoperative symptoms (Table 2).
Preoperative Clinical Outcomes in Each Group.
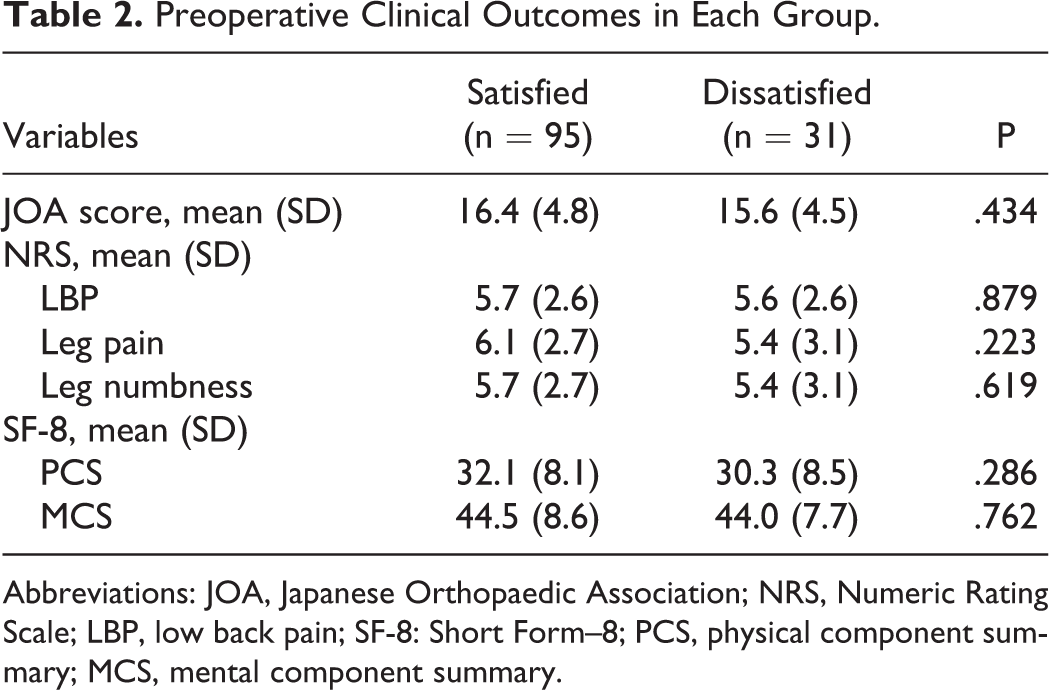
Abbreviations: JOA, Japanese Orthopaedic Association; NRS, Numeric Rating Scale; LBP, low back pain; SF-8: Short Form–8; PCS, physical component summary; MCS, mental component summary.
Difference in Operative and Postoperative Variables Between the 2 Groups
We compared the operation time, estimated blood loss (EBL), and number of decompression level between the 2 groups. No difference was observed (Table 3).
Postoperative Variables in Each Group.
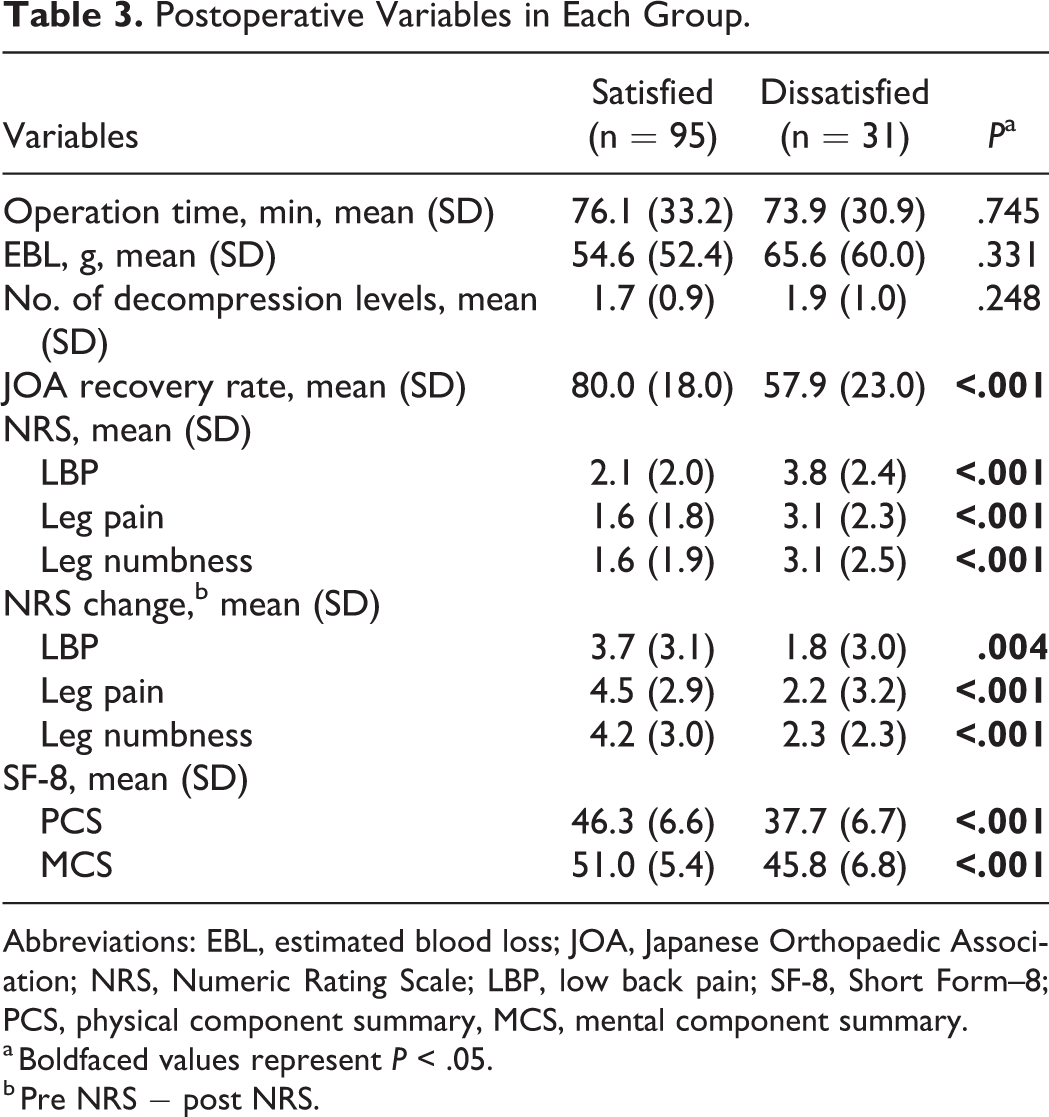
Abbreviations: EBL, estimated blood loss; JOA, Japanese Orthopaedic Association; NRS, Numeric Rating Scale; LBP, low back pain; SF-8, Short Form–8; PCS, physical component summary, MCS, mental component summary.
a Boldfaced values represent P < .05.
b Pre NRS − post NRS.
The JOA recovery rate was significantly higher in the satisfied group (80.0%) than in the dissatisfied (57.9%) group. Similar trend was observed for NRS and SF-8.
Difference in Medical Comorbidities Between the 2 Groups
We compared the prevalence of diabetes mellitus, history of cancer, and neurological diseases between the two groups as these comorbidities have been related to PS. 1,3 These comorbidities were not significantly different between the 2 groups. Diabetes mellitus was found in 17% and 26% in the S and D groups, respectively (P = .808). History of cancer was found in 2% and 6% in the S and D groups, respectively (P = .253). Neurological disease was found in 5% and 6% in the S and D groups, respectively (P = .681).
Difference in Complication Rate Between the 2 Groups
We compared the complication rate between the 2 groups. Any of complication rate was not significantly different between the 2 groups. There were 2 patients with postoperative epidural hematoma that needed evacuation in the S group whereas 1 patient needed postoperative hematoma evacuation in the D group (P = 1.000). Dural tear was recognized in 5% and 6%, respectively (P = .681). No infection or neurological deficit was recognized in both groups.
Correlation Between PS and Symptoms
We assessed correlation between PS and each symptom including LBP, leg pain, and numbness. Preoperative NRS did not show any correlation with PS. Postoperative NRS and postoperative improvement of NRS in all components had weak correlation with PS (Table 4).
Correlation Between Patient Satisfaction and Symptoms.a
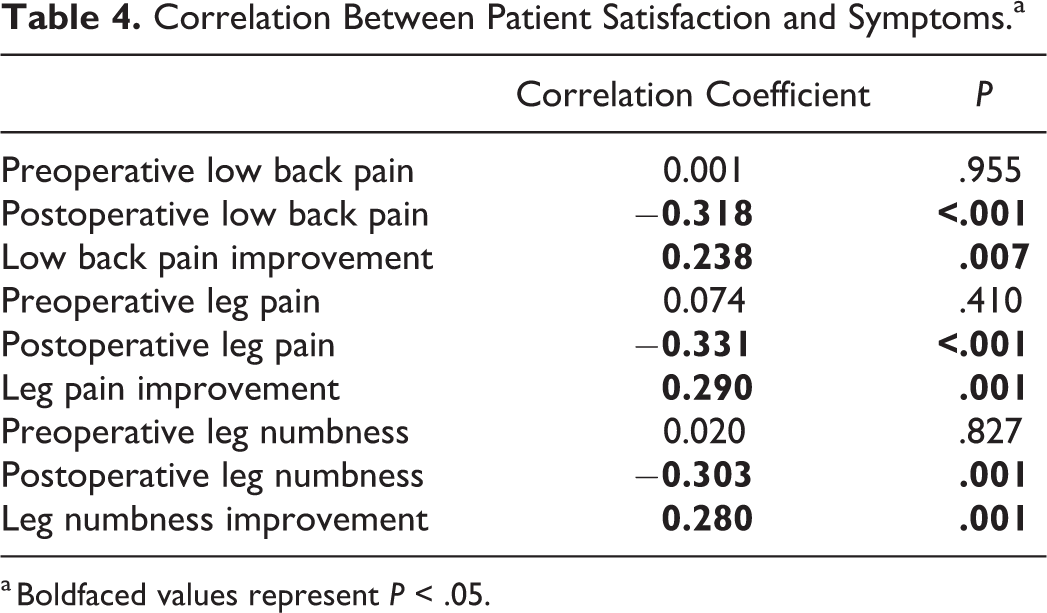
a Boldfaced values represent P < .05.
Multivariate Logistic Regression Analysis of the Variables for Dissatisfaction
Given the results of univariate analyses, smoking status and preoperative scoliosis were considered as the dependent variables. Both variables were found to be significant risk factors for dissatisfaction even in the multivariate logistic regression analysis (Table 5). The odds ratios were 4.08 and 4.32, respectively.
Multivariate Logistic Regression Analysis Evaluation for Dissatisfaction.
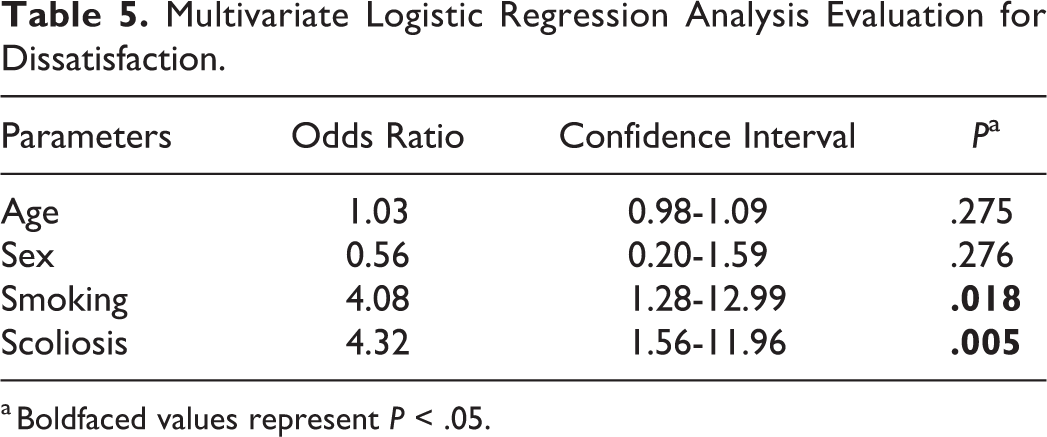
a Boldfaced values represent P < .05.
Subanalysis Between the 4 Groups
We compared the variables between very satisfied, somewhat satisfied, somewhat dissatisfied, and very dissatisfied groups to find factors differentiating very satisfied from somewhat satisfied, or very dissatisfied from somewhat dissatisfied. There was no difference in age, sex, BMI, ASA grade, drinking status, presence of anterior or posterior spondylolisthesis, operation time, EBL, and number of decompression level. The percentage of smokers had linear relationship with PS; smokers were found in 9.5%, 11.3%, 16.0%, and 83.3% in very satisfied, somewhat satisfied, somewhat dissatisfied, and very dissatisfied groups, respectively (P = .001). A similar finding was found in the presence of mild scoliosis. Mild scoliosis was recognized in 7.1%, 18.9%, 36.0%, and 50.0%, respectively (P = .010).
Discussion
The aim of this study was to investigate the satisfaction rate in LSS patients following decompression without fusion, as well as to identify the risk factors related to dissatisfaction. The satisfaction rate was 75% and is consistent with previous reports. 1 -4 PS is expected to be multifactorial and not necessarily consistent with improvements in the clinical outcomes. 8 Preoperative expectations, physical or mental condition, and lifestyle may be related to patient satisfaction. 1,3,9 In this study, we examined a broad range of factors to address this issue. First, we assessed the background characteristics of patients. Age and sex were not found to be related to PS. Previous studies implied that medical comorbidities, such as neurological diseases or cancer status, were associated with PS. 1,3 We examined the association of PS with diabetes mellitus, neurological diseases, and cancer and found no association. We also evaluated ASA grade; however, no difference was observed between the groups.
We evaluated PS by analyzing the preoperative symptoms using JOA score, NRS, and PCS (Table 2). There was no difference between the 2 groups, implying preoperative symptoms may not be associated with PS. Next, we assessed postoperative NRS and the amount of improvement in 3 symptoms (LBP, leg pain, and leg numbness) using the NRS scores (Table 3). Overall, the satisfied group had significantly lower NRS score and higher improvement in all the 3 symptoms. We also examined whether a specific symptom was associated with PS. All of LBP, leg pain and numbness had weak correlation to a similar extent (Table 4).
Previous studies found mental distress as one of the risk factors for patient dissatisfaction in lumbar surgery. 9 We assessed mental status using the MCS domain of SF-8. Preoperative MCS was not different between the 2 groups in our cohort. We did not evaluate mental status using the Distress and Risk Assessment Method (DRAM) questionnaire, which is a more detailed evaluation method for psychological distress. Abtahi et al 9 showed association between PS after spine surgery and psychological distress as measured with the DRAM questionnaire where mentally distressed patients gave significantly lower scores for overall satisfaction compared with patients categorized as normal. They concluded that psychological factors may influence patients’ perception of the medical care. 9 Their cohort included fusion surgery as well as decompression surgery whereas our cohort only included decompression surgery, which may lead to the discrepancy of the results. Further investigation with larger sample size and detailed mental evaluation may be necessary to conclude this issue in decompression surgery.
To the best of our knowledge, we for the first time used radiographic findings for the evaluation of PS. Decompression without fusion is a reasonable option for patients with scoliosis or spondylolisthesis as long as the condition is mild and stable. 10 According to our findings, anterior or posterior spondylolisthesis was not related to PS; however, scoliosis was associated with PS. We included only mild scoliosis with a Cobb angle between 10° and 15°. However, these patients had worse PS than that in nonscoliotic patients. This may be due to foraminal stenosis or low back pain associated with the progression of the curve. The cause remained unidentified; however, we should pay more attention to patients with mild scoliosis after decompression surgery.
From the univariate analysis, we found that smoking and scoliosis were possible prognostic factors for dissatisfaction following decompression surgery. We further investigated the prognostic factors using the multivariate logistic regression analysis. Even after adjustment, smoking status and preoperative scoliosis remained as significant risk factors for postoperative dissatisfaction. Numerous reports have shown that smoking had negative effects on clinical outcomes and satisfaction. 3,11,12 Thus, smoking cessation before surgery should be mandatory although there is no definitive data regarding how long to refrain from smoking. Glassman et al 13 showed significant improvements in fusion rates, PS, and return to work rates in patients who refrained from smoking postoperatively, with results tending to be better in patients who quit for more than 6 months after surgery. They found no association between preoperative smoking cessation and fusion rates, PS, or return to work rates. 13 Other studies showed preoperative smoking cessation for 4 weeks is associated with a decreased risk of infection, perioperative respiratory, and wound complications. 14 -16 Thus, it would be necessary to refrain from smoking at least 4 weeks before surgery and 6 months after surgery.
Preexisting degenerative lumbar scoliosis (DLS) was reported to be associated with worse clinical outcomes after decompression for LSS. 17,18 On the contrary, Toyoda et al 10 reported DLS was 5-year and longer clinical outcomes in patients with LSS treated with microsurgical decompression, and DLS was not associated with worse clinical outcome. We excluded moderate or high-grade scoliosis from the current study. Patients with mild scoliosis with a Cobb angle of ≤15° were included. Of 31 dissatisfied patients, 12 had mild scoliosis. Three patients had exacerbation in leg pain and 4 patients had unchanged or worse LBP at the final follow-up. The remaining 5 patients had improvement in all NRS domains but were dissatisfied due to unknown reasons, possibly improvement did not reach patients’ expectation; this is illustrating multifactorial nature of PS and discrepancy between improvement in clinical outcomes and PS.
There are several limitations to this study. First, it was a retrospective study and the follow-up period was minimum 1 year. Second, we did not evaluate the duration of symptoms before surgery. Previous studies showed that duration of symptoms was associated with the clinical outcomes or PS 3,12,19 -21 ; however, some reviews have reported no association. 22,23 LSS symptoms are usually episodic, and patients do not always remember the onset. In our study, it was hard to obtain the accurate onset from each patient. A prospective study with a larger sample size and long-term follow-up would be necessary to confirm our findings. Last, we divided patients into 2 groups although there were 4 answers, including very satisfied, somewhat satisfied, somewhat dissatisfied, and very dissatisfied. This is because we found only 6 patients in the very dissatisfied group, making the subanalysis difficult with insufficient power. However, 2 risk factors for dissatisfaction were also significant when comparing the 4 groups. However, analysis with more sample size may yield other factors that differentiate very satisfied from somewhat satisfied, or very dissatisfied from somewhat dissatisfied.
Conclusion
Smoking status and scoliosis with a mild curve were associated with patient dissatisfaction following decompression without fusion for LSS. This information may help surgeon’s decision making for surgical and nonsurgical treatments, as well as for the addition of fusion in LSS patients even with a mild scoliosis.
Footnotes
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.