
Abstract
Study Design:
A single-center, retrospective cohort study.
Objective:
To predict patient-reported outcomes (PROs) using preoperative health-related quality-of-life (HRQoL) scores by quantifying the correlation between them, so as to aid selection of surgical candidates and preoperative counselling.
Methods:
All patients who underwent single-level elective lumbar spine surgery over a 2-year period were divided into 3 diagnosis groups: spondylolisthesis, spinal stenosis, and disc herniation. Patient characteristics and health scores (Oswestry Low Back Pain and Disability Index [ODI], EQ-5D, and Short Form-36 version 2 [SF-36v2]) were collected at 6 and 24 months and compared between the 3 diagnosis groups. Multivariate modelling was performed to investigate the predictive value of each parameter, particularly preoperative ODI and EQ-5D, on postoperative ODI and EQ-5D scores for all the patients.
Results:
ODI and EQ-5D at 6 and 24 months improved significantly for all patients, especially in the disc herniation group, compared to the baseline. The magnitude of improvement in ODI and EQ-5D was predictable using preoperative ODI, EQ-5D, and SF-36v2 Mental Component Score. At 6 months, 1-point baseline ODI predicts for 0.7-point increase in changed ODI, and a 0.01-point increase in baseline EQ-5D predicts for 0.01-point decrease in changed EQ-5D score. At 24 months, 1-point baseline ODI predicts for 1-point increase in changed ODI, and a 0.01-point increase in baseline EQ-5D predicts for 0.009-point decrease in changed EQ-5D. A younger age is shown to be a positive predictor of ODI at 24 months.
Conclusions:
Poorer baseline health scores predict greater improvement in postoperative PROs at 6 and 24 months after the surgery. HRQoL scores can be used to decide on surgery and in preoperative counselling.
Keywords
Introduction
Patient-reported outcomes (PROs), 1 defined as the measurement of any aspect of a patient’s health status that comes directly from the patient (ie, without the interpretation of the patient’s responses by a physician or anyone else), have emerged as an important technique for assessing the effectiveness of surgical treatment. 2 -6 This greatly complements the previous method of assessing outcomes using gross patient symptoms and functions as well as the radiological quality of fixation, bone alignment, and fusion.
In terms of lumbar spine surgery for conditions such as spondylolisthesis, spinal stenosis, and disc herniation, 7 -10 PROs are recognized widely as the gold standard in the evaluation of these patients. 11 Many studies have shown that the severity of preoperative symptoms to be a prognostic factor for postoperative patient outcomes. In this study, we hope to affirm these findings in patients undergoing degenerative lumbar spine surgeries using PROs.
The primary objective of this study was to predict postoperative PROs using preoperative health-related quality-of-life (HRQoL) scores by quantifying the correlation between them. The form of quantifying PROs has never been used as a primary objective in any study from an Asian perspective. The results of this study will allow us to understand the magnitude of improvement expected for each lumbar condition undergoing surgery. It will also become a valuable tool in preoperative patient counselling and perhaps enable us to refine our selection criteria when identifying suitable candidates for surgery in the future. This study will allow comparison for future studies using health questionnaires, particularly in an Asian perspective.
Methods
Study Design
This is a single-center, retrospective cohort study conducted in an academic hospital with tertiary health care facilities. Institutional review board approval was obtained prior to the initiation of the study. In this study, we included all patients who underwent single-level elective lumbar spine surgery over a 2-year period. Patients with spine conditions secondary to tumor, fractures, infection, inflammatory spondyloarthropathies, previous spine surgeries, and those who underwent emergency surgery for cauda equine syndrome were excluded from this study.
Apart from standard clinical assessments for patients with low back pain or radiculopathy, all patients had X-rays and magnetic resonance imaging scans of the lumbar spine. They were subdivided into 3 groups according to their main diagnosis: spondylolisthesis, spinal stenosis, and disc herniation. All patients had received a trial of physiotherapy up to 3 months before surgical intervention. Indications for surgery include persistence of symptoms despite physiotherapy, progressively deteriorating neurological status, and worsening deformity.
These patients underwent a wide variety of surgical procedures including microdiscectomy, decompression laminectomy, and instrumented fusions. All patients undergoing surgery were first audited by a panel of spine surgeons within the department preoperatively to review the indication of surgery and the surgical procedure suitable for their condition.
Data Collection Procedure
All health questionnaires were self-administered, and patients were only approached by the trained staff if the questionnaires were incomplete. The questionnaires were given to the patient on enlistment for spine surgery for preoperative assessment, and during each follow-up clinic visit for postoperative assessments (at 6 months and 24 months postoperatively). Patients who did not attend the follow-up clinic were contacted by a trained staff via mail, phone, or email to complete the questionnaires.
The PRO questionnaires used were the Oswestry Low Back Pain and Disability Index (ODI) Version 1.0, 12 EQ-5D, 13 and Short Form-36 version 2 (SF-36v2). 14 The questionnaires used came in 2 languages—English and Mandarin—depending on patient’s preference.
All information collected were stored in the electronic Central Clinical Research Database established by the department for the purpose of collecting data for clinical audit, quality control, and research.
Data Analysis
Data analysis was performed using the Statistical Package for the Social Sciences (SPSS, version 17) software. The patient background characteristics (demographics, health and functional status, diagnosis, and type of operations) were examined.
The ODI and EQ-5D scores at 6 and 24 months from baseline were calculated for the entire patient population as well as for each diagnosis group. One-way ANOVA analysis was carried out to detect if there was any difference in the scores between these groups.
The change in postoperative ODI and EQ-5D scores at 6 and 24 months were analyzed using linear regression. The diagnosis group was coded to spondylolisthesis, stenosis, and disc herniation. Age, preoperative ODI, EQ-5D, and both the Physical Component Score (PCS) and Mental Component Score (MCS) from SF-36v2 remained as continuous variables.
A univariate linear analysis was carried out to investigate the effect of baseline ODI, EQ-5D, and SF36v2 scores on changed ODI and EQ-5D scores at 6 and 24 months, which is the primary objective of the study. Other baseline patient demography, comorbidities, and symptoms were also analyzed as covariates to identify predictors of ODI and EQ-5D change. Only clinically or statistically significant variables were included in the multivariate linear regression predictive modelling. Clinically significant variables were defined as those with known effects on ODI or EQ-5D scores—gender, age, comorbidities, duration of symptoms—while statistically significant variables were those with the conventional P value less than .05 in the univariate analysis.
Results
A total of 292 patients who underwent lumbar spine surgery were surveyed over a 2-year period. For the entire study population, the majority of the patients were within the age group of 41 to 64 years (52%). There was a substantial group of patients with comorbidities such as hypertension (36%), hyperlipidemia (24%), and diabetes (16%). Forty-seven percent of the surgical procedures performed was instrumented fusion, followed by microdiscectomy (32%) and decompression laminectomy (21%).
Baseline characteristics of patients (demographics, patient symptoms, comorbidities, and type of operations) in the 3 groups are as shown in Table 1. In terms of gender, patients with spondylolisthesis were predominantly female (75%) compared to the other 2 groups, which were predominantly male. The mean age for patients with disc herniation was the youngest (40 years) compared to the other 2 groups (both 59 years). The ethnicity proportions followed the national demography closely with a higher proportion of Chinese for all diagnosis. For the duration of symptoms, patients with spondylolisthesis exhibited the longest mean duration of back pain (1640 days), and patients with disc herniation had the shortest mean duration of back pain (780 days). The predominant surgical procedure for spondylolisthesis was instrumented fusion (99%). In spinal stenosis, 60% of the patients required decompression laminectomy while 38% underwent instrumented fusion. The majority of patients with disc herniation underwent microdiscectomy (86%).
Patient Characteristics for Different Groupsa.
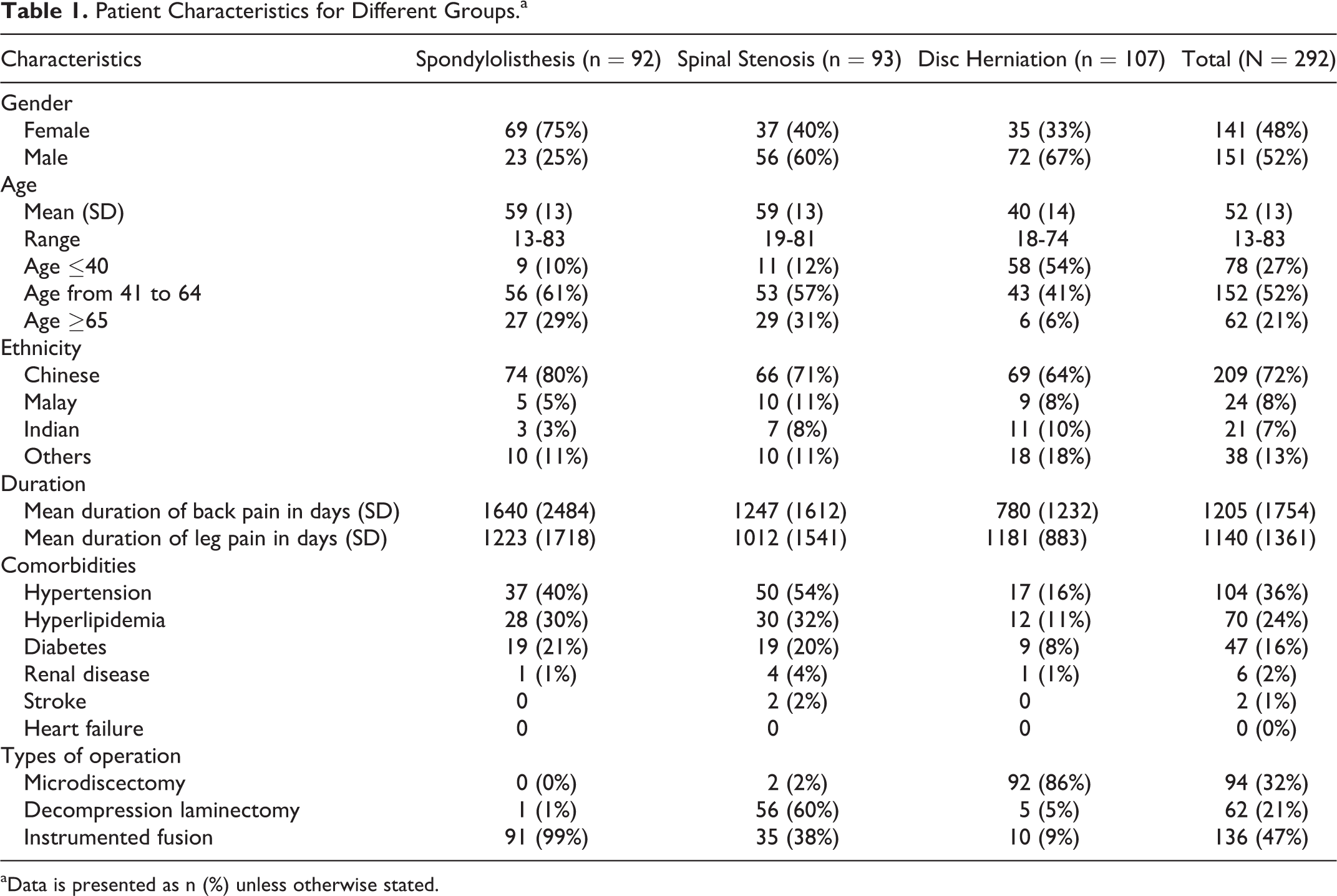
aData is presented as n (%) unless otherwise stated.
In terms of preoperative health scores, patients in the spondylolisthesis group showed the highest mean ODI scores (44.5), while patients with spondylolisthesis showed the lowest mean EQ-5D scores (0.43). The mean ODI and EQ-5D scores at 6 and 24 months were also calculated for these 3 diagnosis groups (Table 2). For the entire patient population, the mean change in ODI and EQ-5D scores at 6 and 24 months were statistically significant compared to the baseline. Those with disc herniation had the highest mean change in ODI scores at 6 months, and those with spondylolisthesis had the highest mean change in EQ-5D scores at 6 months. However, patients in 2 groups (disc herniation and spondylolisthesis) showed a similar mean change in both ODI and EQ-5D scores at 24 months. Patients in the spinal stenosis group fared worse at both time points when compared with those with disc herniation and spondylolisthesis. This was statistically significant when comparing the spinal stenosis group with the disc herniation group (P = .03).
ODI and EQ-5D Scores at Baseline, 6 Months, and 24 Months by Diagnosis Group.
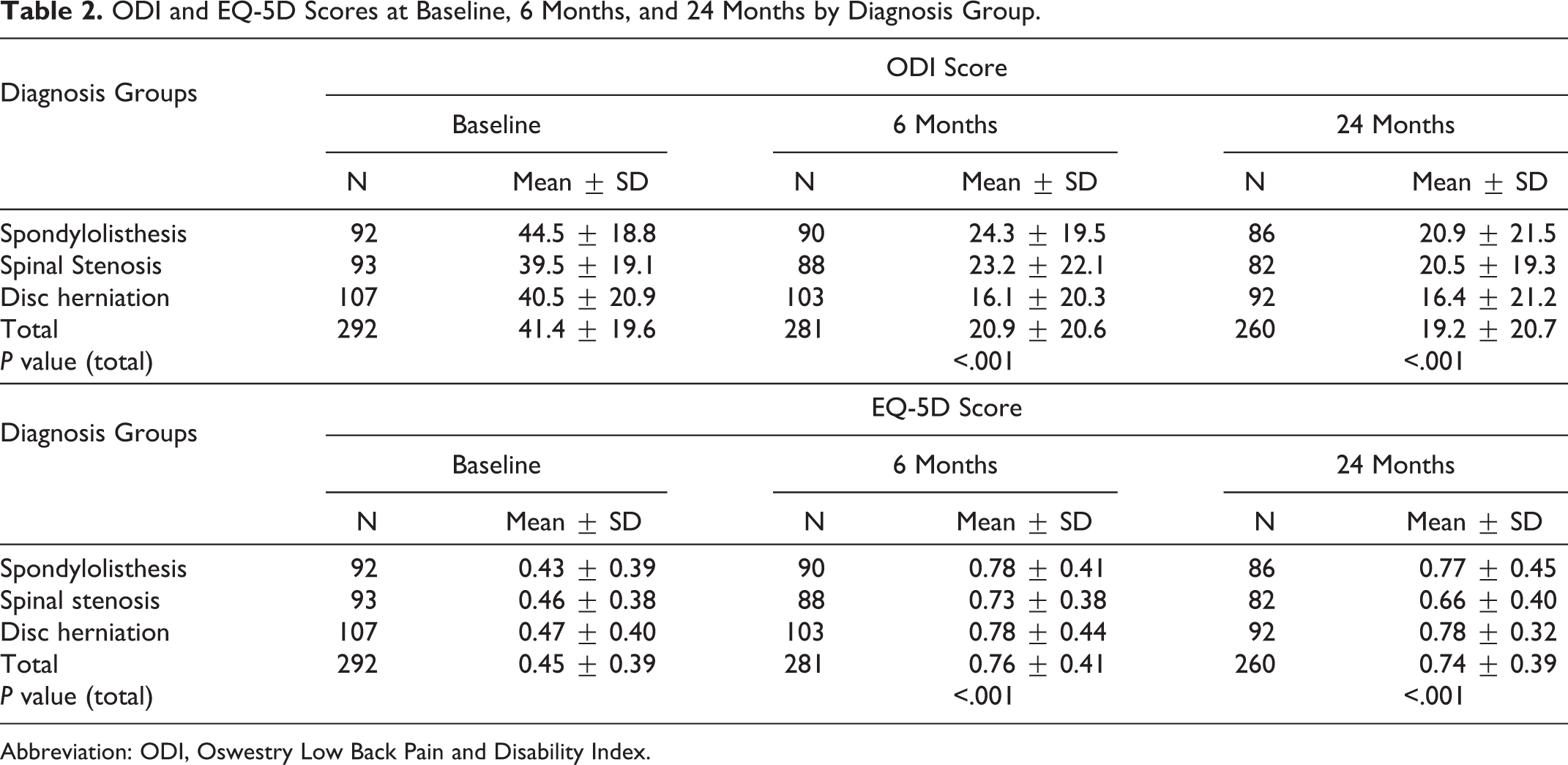
Abbreviation: ODI, Oswestry Low Back Pain and Disability Index.
Baseline health scores are predictive of postoperative PROs at 6 and 24 months after the surgery (Table 3) and their correlation can be quantified (Table 4). Based on this relationship between baseline health scores and PROs, the expected improvement in PROs can be calculated for each patient.
Linear Regression Models With Both Bivariate and Multivariate Analyses for Both ODI and EQ-5D Scores at 6 and 24 Monthsa.
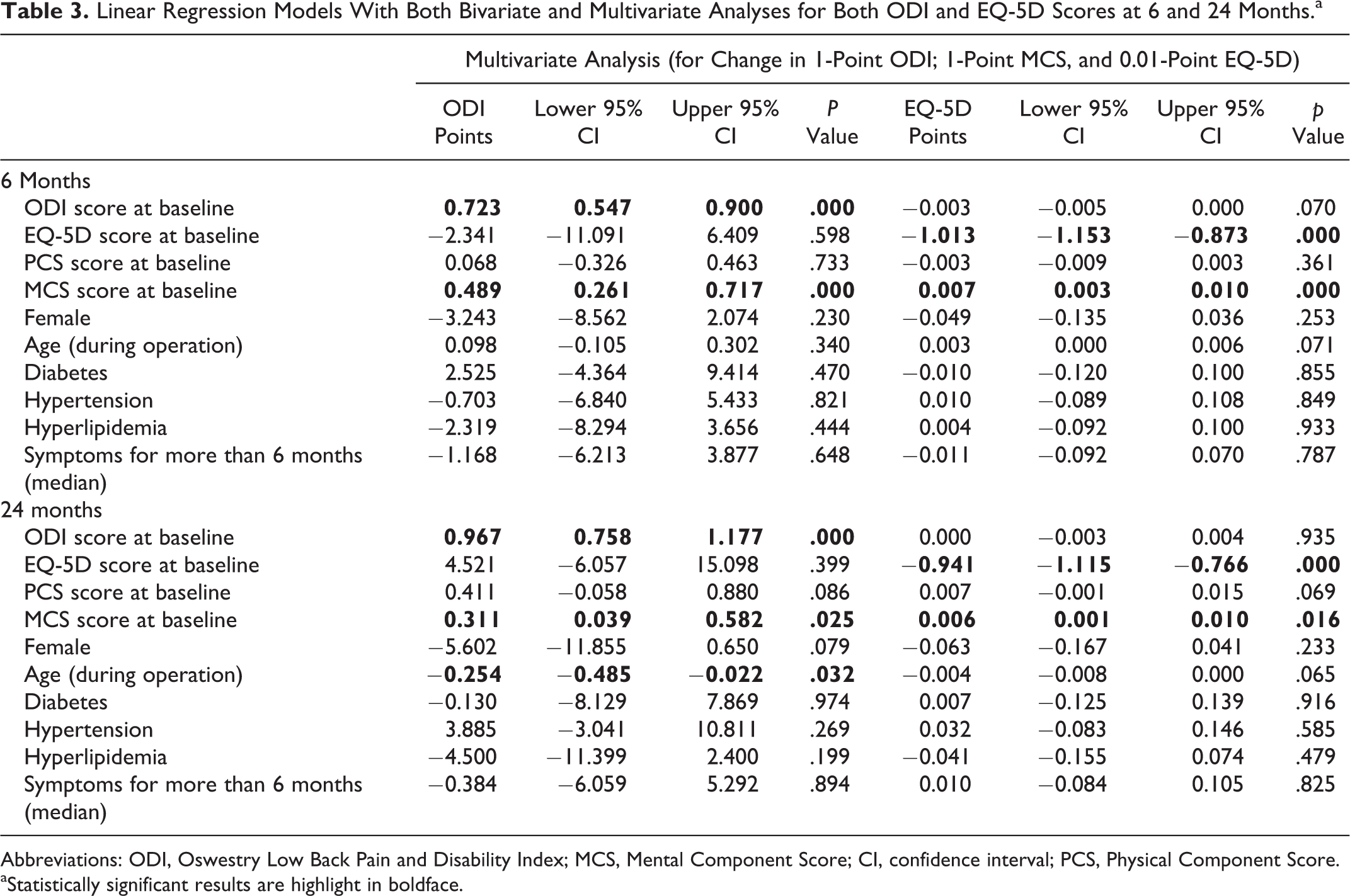
Abbreviations: ODI, Oswestry Low Back Pain and Disability Index; MCS, Mental Component Score; CI, confidence interval; PCS, Physical Component Score.
aStatistically significant results are highlight in boldface.
Predicting Corresponding Changes in Postoperative PROs Using Baseline Health Score Values.
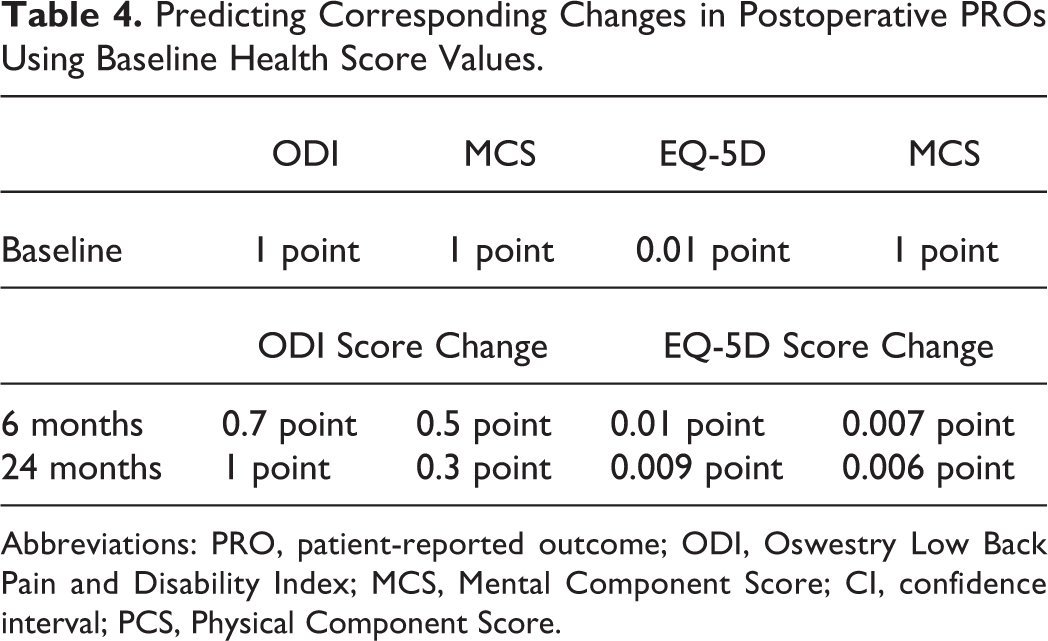
Abbreviations: PRO, patient-reported outcome; ODI, Oswestry Low Back Pain and Disability Index; MCS, Mental Component Score; CI, confidence interval; PCS, Physical Component Score.
In terms of postoperative ODI scores, the multivariate linear regression predictive model shows that baseline ODI and MCS scores were consistent predictors at both 6 and 24 months (Table 3). At 6 months, every 1-point increase in baseline ODI score is associated with a 0.7-point increase in changed ODI score (P < .01), and every 1-point increase in baseline MCS score is associated with a 0.5-increase in changed ODI score (P < .01). At 24 months, every 1-point increase in baseline ODI score is associated with a 1-point increase in changed ODI score (P < .01), and every 1-point increase in baseline MCS score is associated with a 0.3-point increase in changed ODI score (P < .025). Therefore, a poorer baseline functional score and a better baseline mental score predict better improvement after surgery. A younger age is also shown to be a positive predictor of ODI scores only at 24 months (P < .032).
In a similar way, for the linear regression predictive model for change in EQ-5D scores, both baseline EQ-5D and MCS scores were consistent and statistically significant predictors. At 6 months, every 0.01-point increase in baseline EQ-5D score is associated with a 0.01-point decrease in changed EQ-5D score (P < .01), and every 1-point increase in baseline MCS score is associated with a 0.007-point increase in changed EQ-5D score (P < .01). At 24 months, every 0.01-point increase in baseline EQ-5D score is associated with a 0.009-point decrease in changed EQ-5D score (P < .01), and every 1-point increase in baseline MCS score is associated with a 0.006-point increase in changed EQ-5D score (P < .02).
Multivariate analysis of other clinical parameters showed age as the only significant predictor under linear regression of ODI scores at 24 months and not at 6 months when compared with preoperative baseline. Gender, comorbidities, and duration of symptoms are not found to be significant (Table 4).
Discussion
This study presents an Asian population comprising multiple ethnicities, and its results are suitable for comparison with other similar population. The proportion of Chinese, Malays, and Indians resemble the national demographics, and the patient age groups match the various clinical diagnosis shown in the literature. Patients with disc herniation have the lowest mean age group of 40 years, while patients with spondylolisthesis and spinal stenosis have a mean age of 59 years. Chronic medical conditions are prevalent in this country and comprise mainly hypertension, hyperlipidemia, and diabetes mellitus.
The results obtained from this study should be interpreted bearing in mind the type of operation that has been performed for the 3 main diagnoses—spondylolisthesis, spinal stenosis, and disc herniation. The choice of operation is decided by the attending surgeon and audited by a panel of spine surgeons in the institution. Patients with spondylolisthesis diagnosed either by X-rays in the standing neutral or flexion-extension views almost always undergo instrumented fixation (99%), as they are deemed unstable and should be stabilized. Although recent studies may suggest otherwise, 15,16 this topic remains a highly controversial issue. 17,18
Majority of patients with disc herniation underwent microdiscectomy (86%) as the operation of choice while some underwent instrumented fusion (9%) due to a predominance of axial back pain over leg pain, or when diagnosed with foraminal disc herniation, recurrent disc herniation, and large herniated disc, which was deemed not possible to remove without rendering the spine unstable. For patients with spinal stenosis, there was a tendency toward performing decompression laminectomy (60%) rather than instrumented fusion (38%). Patients who required fusion had concurrent severe axial back pain, vacuum disc spaces, or hyperintense fluid signal in the facet joints. Although the heterogeneity in surgical treatment does not allow this study to answer specific clinical questions regarding the effectiveness of each treatment, this study offers valuable pragmatic information close to reality. Exceptional cases that warrant a slightly different form of management are allowed to vary in terms of the surgical plan as long as the indication can be supported by evidence. This happens in normal clinical situations.
The Spine Patient Outcomes Research Trial (SPORT) 19 classified degenerative lumbar spine conditions identical to our study. Its main objective is to compare Western patients who had undergone surgery for the conditions of spondylolisthesis, spinal stenosis, and disc herniation, with those who underwent conservative treatment. In this large study, both treatment methods were effective, although a greater magnitude of the treatment effect of surgery over conservative treatment was found. 20 -23 Although it was not designed to compare the surgical benefits across all 3 conditions, the magnitude of improvement appears to be greatest for patients with spondylolisthesis, followed by spinal stenosis and then disc herniation. 23 Our study showed a slightly opposite result with patients who were treated for disc herniation having the best outcome that was maintained up to 2 years in terms of both ODI and EQ-5D scores. Patients with spondylolisthesis had improvement in ODI scores at 6 months but minimal further improvement up to 2 years. EQ-5D plateaued on reaching 6 months. Patients with spinal stenosis fared worst with ODI outcomes similar to patients with spondylolisthesis but showed a further worsening of EQ-5D scores between 6 and 24 months.
It is an undisputable fact that in patients with spinal conditions, the source of symptoms may not be easily localized. In the circumstances of a radiculopathy occurring with a concordant disc herniation, the diagnosis is clear and surgery to decompress the nerve in the form of a microdiscectomy should deliver good results. 24 This is shown in our patients where their PROs improved the most at 6 months and at 24 months. On the contrary, the assessment of patients with spondylolisthesis may not be as straightforward. Unless there is a concomitant radiculopathy that matches the exact location of nerve root compression, symptoms otherwise may not be fully addressed by surgery. In our study, most patients in this group underwent instrumented fusion of the affected unstable spinal levels. It is, therefore, likely that if the symptoms were to be truly secondary to instability, they should be addressed, which is reflected in the improvement in symptoms postoperatively at 6 months. Further improvement in symptoms is therefore not likely and may be due to overall spinal rebalance and its effects on muscle strain and facet joint loading.
Patients with spinal stenosis present with the greatest diagnostic challenge. Multiple areas of pathology that may result in axial back pain and radiculopathy are often difficult to accurately assess. 25 Moreover, various degrees of compression from various pathologies such as facet arthropathy, thickened ligamentum flavum, and disc bulges make surgery outcome less predictable. To make situations worse, nerve compression could occur either at the lateral recess or at the neuroforamen; the latter requiring foraminotomy and possibly an interbody fusion. These issues reflect our study population, wherein the majority (60%) underwent instrumented fusion. Although the 6-month PROs showed significant improvement, no further improvement in ODI was observed at 24 months. EQ-5D, on the contrary, showed worsening scores. We hypothesized that this could be a result of the existing problem being partially addressed, or worsening of adjacent levels that were previously asymptomatic. Recent results from Cochrane reviews on surgical treatment for spinal stenosis and spondylolisthesis also showed conflicting results and permitted limited conclusions. 26 -28
The findings of baseline health scores being predictive of postoperative PROs at 6 months and 24 months confirms our hypothesis that patients with more disability or poorer perception of their own quality of life get more benefit from the surgery. Similar results were reported by Leatherman Spine Center, 29 but the authors did not quantify the effect these scores had on PROs. The probable reason why baseline disability and quality-of-life scores are predictors of such outcomes is that patients who have more severe preoperative symptoms are more sensitive to improvements following surgery. Moreover, these patients may be keener in the perception of their symptoms, making them more appreciative of the outcome of surgery. 30 This could also explain why better baseline mental health was associated with greater improvement in PROs at 6 and 24 months in our study. This emphasizes the need to assess the severity of each condition and its associated disability in order to achieve maximal beneficial gains of surgery for every patient. Patients with more severe conditions should be counselled appropriately so that they would understand the benefits of surgical treatment. Management of patient expectations before and after surgery may also improve outcomes, especially to those with poor mental status. 31,32
Using multivariate regression modelling, a correlation is obtained between baseline health scores and PRO at 6 and 24 months. This correlation helps predict the expected significant change in ODI and EQ-5D using every single unit increase in baseline ODI, EQ-5D, and MCS scores. The information can be applied in the preoperative context to guide surgical decision making and patient counselling. Moreover, both ODI and EQ-5D are found to self-predict. This could be due to the use of identical items in each questionnaire instrument such that specific differences in pre- and postoperative results can be easily identified. Since preoperative HRQoL scores predict patient outcomes as shown in this study, patients can be better counselled prior to surgery on the outcomes to expect. The ultimate decision on surgery can then be improved weighing the risks and benefits. This will value add to the combined decision-making process between the surgeon and the patient.
In this study, age is found to be an independent predictor for PROs postoperatively. It becomes statistically significant for the linear regression model at 24 months and not at 6 months when compared with preoperative baseline. This has also been shown in other studies where factors such as gender, age, comorbidities, and duration of symptoms have all been found to be predictors. 33 -36 The possible reason why age is the only significant parameter identified in this study could be due to study sample size, differences in population demography, and the differences in surgical preferences for various conditions. 37 In order to address this issue, future studies involving larger samples should be conducted. We hypothesize that age being the only significant predictor at 24 months could be secondary to time-varying factors in the patient’s life that affect the intermediate-term PRO measurement at 24 months. A person is likely to be more different after 24 months if old compared to when he is younger. A review by Mannion and Elfering 38 relates this finding and suggested repeating the analyses at various follow-ups to identify stable and consistent predictors. This finding should be further explored to see if an earlier operation can be recommended in patients with the aforementioned conditions.
The main limitation of this study lies in its retrospective nature such that data collection may not be complete. Patients in the disc herniation group are observed to have a longer mean duration of symptoms (back pain 780 days and leg pain 1181 days) than expected. It is likely that these symptoms do not truly reflect the acute component of the condition. As many of these patients will have nonspecific symptoms secondary to spinal degeneration, this finding reflects the practical limitations during history-taking. Ideally, more details with regard to the pain will be helpful to differentiate between the acute and chronic components. This is however not possible due to the retrospective nature of our study. Although this study is able to evaluate the use of baseline health scores in predicting PROs due to small sample size, future studies should be performed to improve the utility of HRQoL scores in specific spinal conditions.
The loss to follow-up seen for the collection of ODI and EQ-5D scores is inevitable in such clinical studies and may have confounded some of the results. Nevertheless, there remains a good follow-up for both ODI and EQ-5D scores at 6 months (96.2%) and at 24 months (89.0%). The magnitude of improvement expected of PROs given in this study remains valuable information in our determining which patients would best benefit from surgery and will be a valuable tool for better patient preoperative counselling, particularly in the Asian population context.
Conclusion
In conclusion, baseline health scores are predictive of functional outcome postoperatively. A more severe disability and poorer quality-of-life scores before surgery were associated with greater improvement in disability and quality of life, respectively, at 6 and 24 months after the surgery. This supports the need to assess disease severity and patient disability prior to surgery. Information from this study can be used for preoperative counseling to manage patient expectations prior to surgery. Age as a time-varying predictor of outcome is an interesting finding that should be further explored to see if an earlier operation can be recommended in the conditions studied in this article.
Footnotes
Acknowledgments
We would like to acknowledge help from Dr Lin Shu Xun and Dr Desmond Thiam Wai for their help in proofreading the manuscript prior to submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.