
Abstract
Study Design:
Single-center prospective cohort.
Objectives:
To evaluate a multidisciplinary led, structured protocol for reducing surgical site infections (SSIs) in pediatric scoliosis surgery.
Methods:
Following a spike to 8.6% in local annual infection rate, a multidisciplinary team was convened to identify interventions. The team consisted of spinal surgeons, infectious diseases consultants, physiotherapists, specialist nurses, and theatre managers. A protocol was initiated, including preoperative skin decontamination; standardized operative site prepreparation; betadine-soaked swabs sutured to wound edges; blood loss minimization; 3 L0.9% saline pulsed-lavage; defined protocol of glove changes; antibiotic regime of preoperative gentamicin, intraoperative subfascial vancomycin powder, 48-hour cefuroxime; and intraoperative normothermia. A 4-year audit was initiated of all patients aged ≤18 years undergoing corrective spinal deformity surgery. Institutional board review was not required.
Results:
Between January 1, 2014 and January 1, 2018, 414 operations were performed on 355 patients: male:female = 1:2.2, mean age 13.7 years (range 2.5-17.9), 233 idiopathic (mean operated vertebral levels 12), 122 neuromuscular (mean operated vertebral levels 14), 66 growing rod procedures, 41 multistage procedures. The mean number of operated vertebral levels both overall and in infected cases was 13 (range 2-17). Nine SSIs occurred in 8 patients at 3 months (4 neuromuscular), resulting in an overall SSI per operation of 2.2%.
Conclusion:
A multidisciplinary approach with standardized measures significantly reduced SSIs in the unit’s pediatric scoliosis surgery.
Introduction
Surgical site infection (SSI) is a well-recognized cause of morbidity and expense. In the United States, the annual cost of SSIs reached 1.6 billion dollars in 2017, 1 with some estimates putting it significantly higher. 2 Patients who develop an SSI are 5 times more likely to be readmitted and twice as likely to die. 3 In pediatric scoliosis surgery, an SSI leads to prolonged hospital stay in a vulnerable patient group and the potential for further surgery with its inherent risks, including worsening of the deformity. Debate continues surrounding the individual interventions to reduce the risk of SSIs. However, there is a growing consensus that the most effective means of reducing the risk of SSIs is a broad based, multidisciplinary approach. 4 -6
Our unit operates from a purpose-built children’s hospital. Over the study period, 5 consultant surgeons performed scoliosis corrective surgery. All 5 had undergone a period of training at the unit prior to taking up post, leading to a consensus regarding operating techniques, but previously no formalized protocol. The published rates of SSI in pediatric scoliosis surgery are as high as 22%, 7 with widespread recognition that children with neuromuscular conditions are at significantly greater risk of infection than those with idiopathic scoliosis. 4,8,9 In one series of 227 pediatric patients undergoing corrective surgery, the relative risk for patients with neuromuscular conditions was calculated as 8.65. 8 Our records indicate that our rate had been within accepted standards. However, an unprecedented cluster of SSIs in 2013 caused a spike in the annual incidence to 8.6%. The infections were correlated with each of the 5 surgeons and were found to be essentially in proportion to the volume of operations each had performed; there appeared to be no overt cause or surgeon(s) with suboptimal technique. This prompted a root cause analysis and multidisciplinary review of practice.
The advisory team consisted of the spinal orthopedic consultants, specialist spinal surgery nurses, theatre managers, physiotherapists, and consultants in infectious disease. An infection control nurse practitioner was engaged with the specific remit to prospectively monitor the incidences of SSIs and to collate data of all surgical procedure in the pediatric deformity unit. As no individual or single circumstance was identified as a cause for this rise in SSIs, a more general approach and analysis was initiated. This identified a series of interventions as part of a new protocol for the standard of practice.
These interventions commence with the admission of the patient and continue throughout postoperative care. This discrete, multistep process includes pre-theatre skin decontamination, standardized operative site preparation, minimization of blood loss, pulsed lavage postinsertion of metalwork, double-gloving with timed changes of the outer glove, a rationalized antibiotic regime, and maintaining intraoperative patient normothermia. These interventions are listed in Table 1 and further described in the discussion.
Series of Interventions.
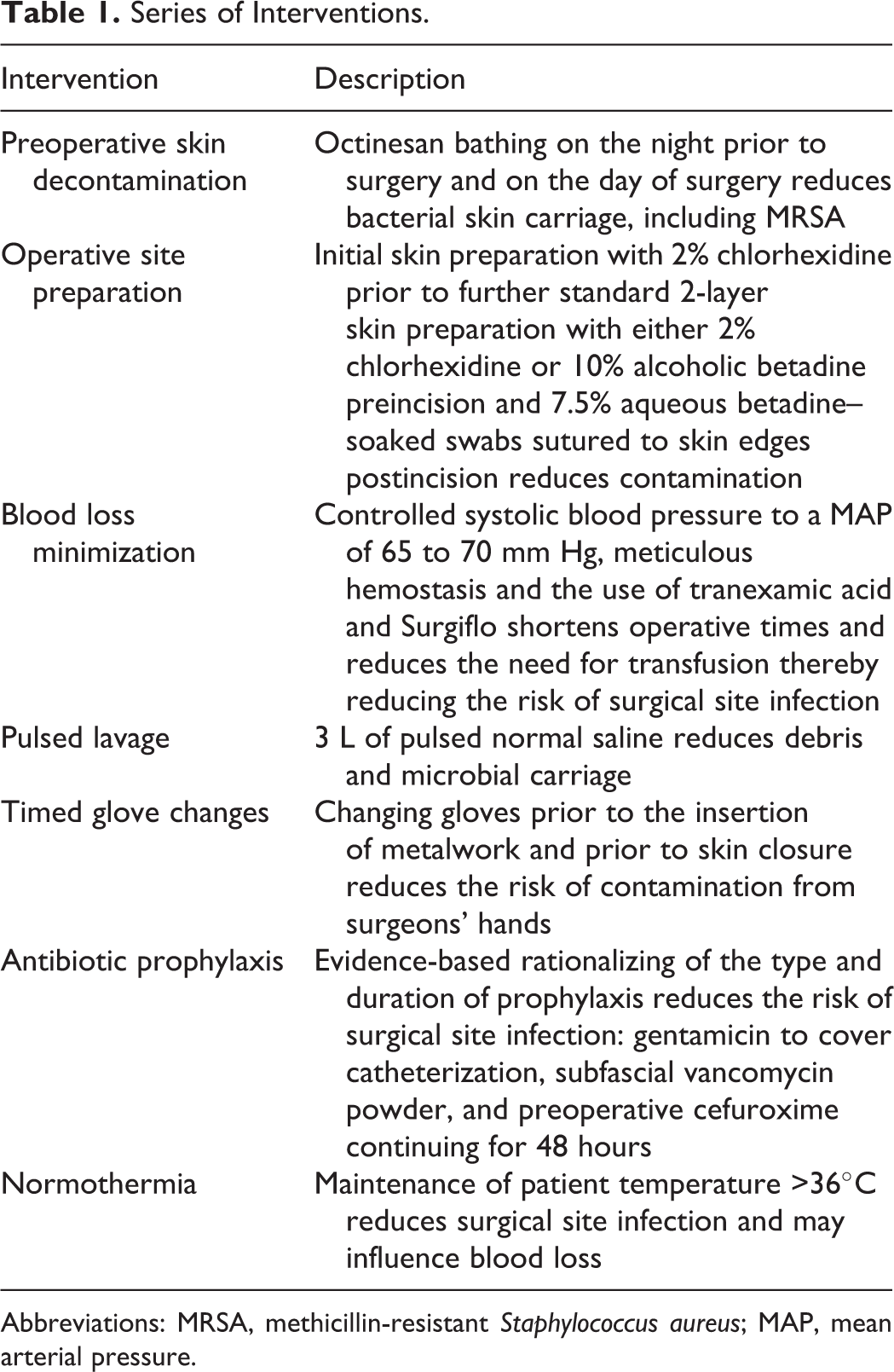
Abbreviations: MRSA, methicillin-resistant Staphylococcus aureus; MAP, mean arterial pressure.
Methods
Study Design and Population
The unit operates within a larger London hospital and is a tertiary referral center for spinal conditions with a catchment of 4.5 million people covering southeast England, the Channel Islands, Gibraltar, and Malta. The unit currently has 3 consultant surgeons who operate in a purpose-designed orthopedic theatre with laminar flow.
Consultant surgeons operated with the assistance of a senior spinal fellow, or more rarely with a second consultant. Length of surgery was not directly audited, but the number of operated levels was used as a surrogate marker for duration. Wound closure was performed with Vicryl sutures to the subcutaneous tissues. Regarding skin closure, for adolescent idiopathic scoliosis cases subcutaneous 3.0 Monocryl with skin glue. For neuromuscular cases 2.0 nylon interrupted sutures were applied, also with glue.
In the time period for the study, the patient population included idiopathic scoliosis and neuromuscular conditions, including cerebral palsy (42 cases), Sotos syndrome (1 case), neurofibromatosis (15 cases), Alagille syndrome (2 cases), Charcot-Marie-Tooth syndrome (1 case), CHARGE syndrome (1 case), Di George syndrome (7 cases), Duchenne’s (4 cases), Dysmorphic syndrome (1 case), Marfan’s syndrome (1 case), Tay-Sachs syndrome (1 case), Rett’s syndrome (3 cases), Down syndrome (2 cases), Wolff-Hirschorn syndrome (2 cases), Aicardi-Guitierre’s syndrome (1 case), Lennox-Gastaut syndrome (1 case), Prader-Willi syndrome (3 cases), Bardet-Biedl syndrome (1 case), achrondroplasia (1 case), spinal muscular atrophy (7 cases), Klinefelter’s syndrome (1 case), Ullrich syndrome (1 case), Williams syndrome (1 case), and VACTERL syndrome (1 case).
The increased rate of SSIs in 2013 prompted the review and commencement of the new protocol:
The 4-year period from January 1, 2014 to January 1, 2018 was included in this study. Ongoing data collection continued and provided a minimum of 3 months’ follow-up for the patient cohort.
Surgical site infection was defined by the Public Health England guidelines 10 (Figure 1).
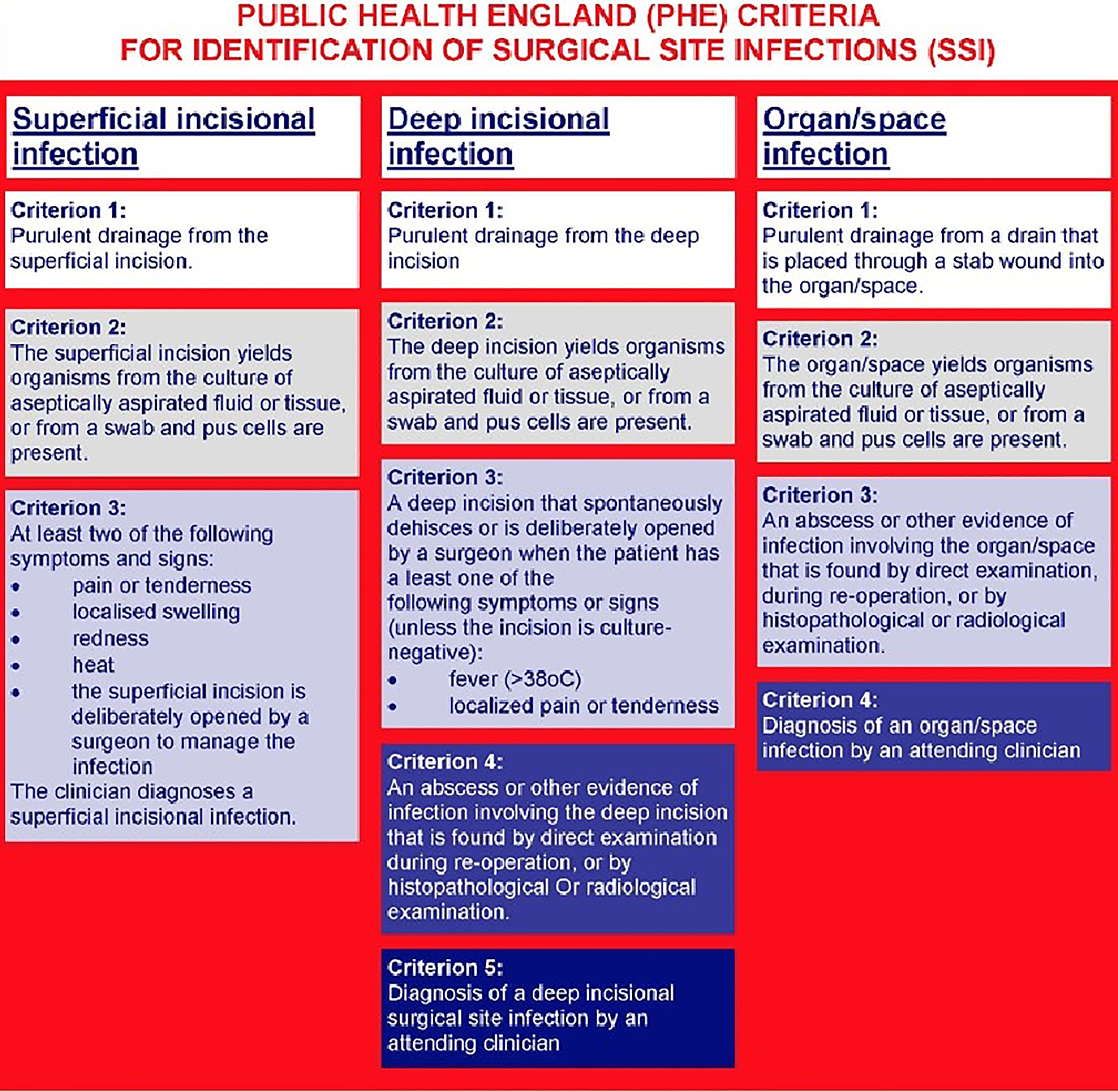
Public Health England (PHE) criteria for identification of surgical site infections (SSIs).
Fisher’s exact test was used to analyze the percentage of infections pre- and postprotocol to determine the chi-square value and establish significance (Table 2).
Statistical Analysis.a
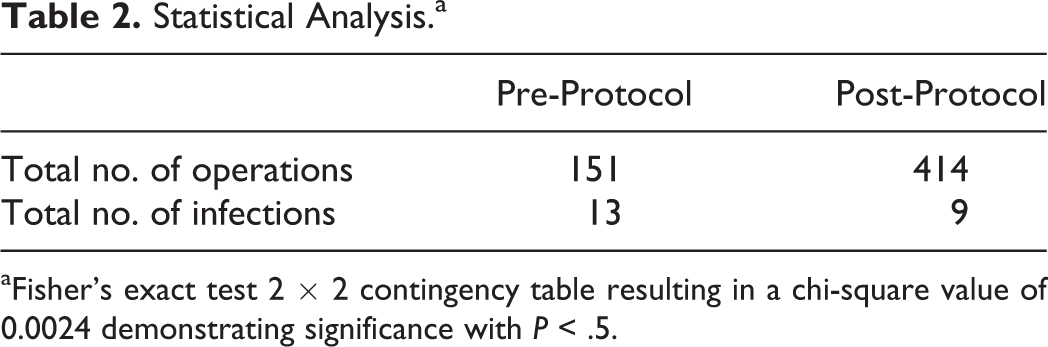
aFisher’s exact test 2 × 2 contingency table resulting in a chi-square value of 0.0024 demonstrating significance with P < .5.
Results
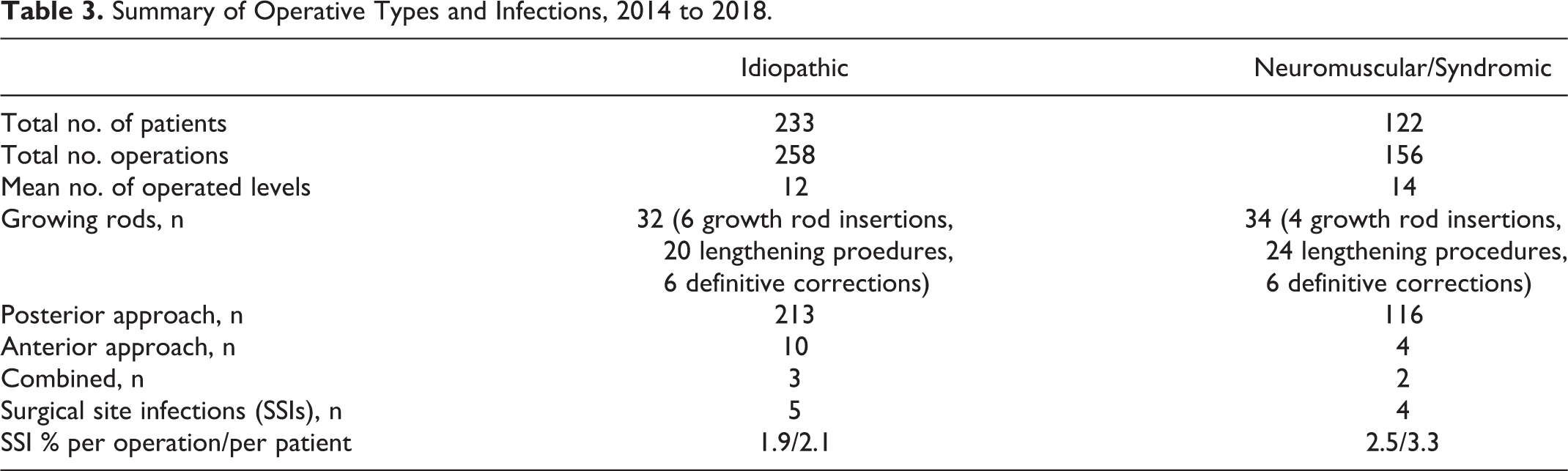
A total of 414 operations were performed on 355 patients: 111 male, 244 female, mean age 13.7 years (range 2.5-17.9 years). Overall, 233 patients had adolescent idiopathic scoliosis (mean operated vertebral levels 12), 122 patients had underlying neuromuscular diagnoses (mean operated vertebral levels 14). 66 procedures were the insertion of growing rods or their revision. There were 41 multistage procedures. The mean number of operated vertebral levels both overall and in infected cases was 13 (range 2-17), with no indication that more levels led to an increase risk of infection. Nine surgical site infections occurred in eight patients at 3 months (4 neuromuscular), resulting an SSI rate per operation of 1.9% in the idiopathic group and 2.5% in the neuromuscular group (Table 3). Once again, no individual surgeon was identified as having a greater risk of infection.
Summary of Operative Types and Infections, 2014 to 2018.
Organisms were cultured from all the infected cases (Table 4). Five infections were due to Staphylococcus aureus (56%). Four cases showed coliforms and fecal organisms (44%). Of note, all of these were in cases with an underlying neuromuscular diagnosis. Only 1 of the 9 episodes of infection required revision of the metalwork; this was the single patient who presented twice with an SSI.
Detailed Breakdown of Infected Cases During the Study Period.a
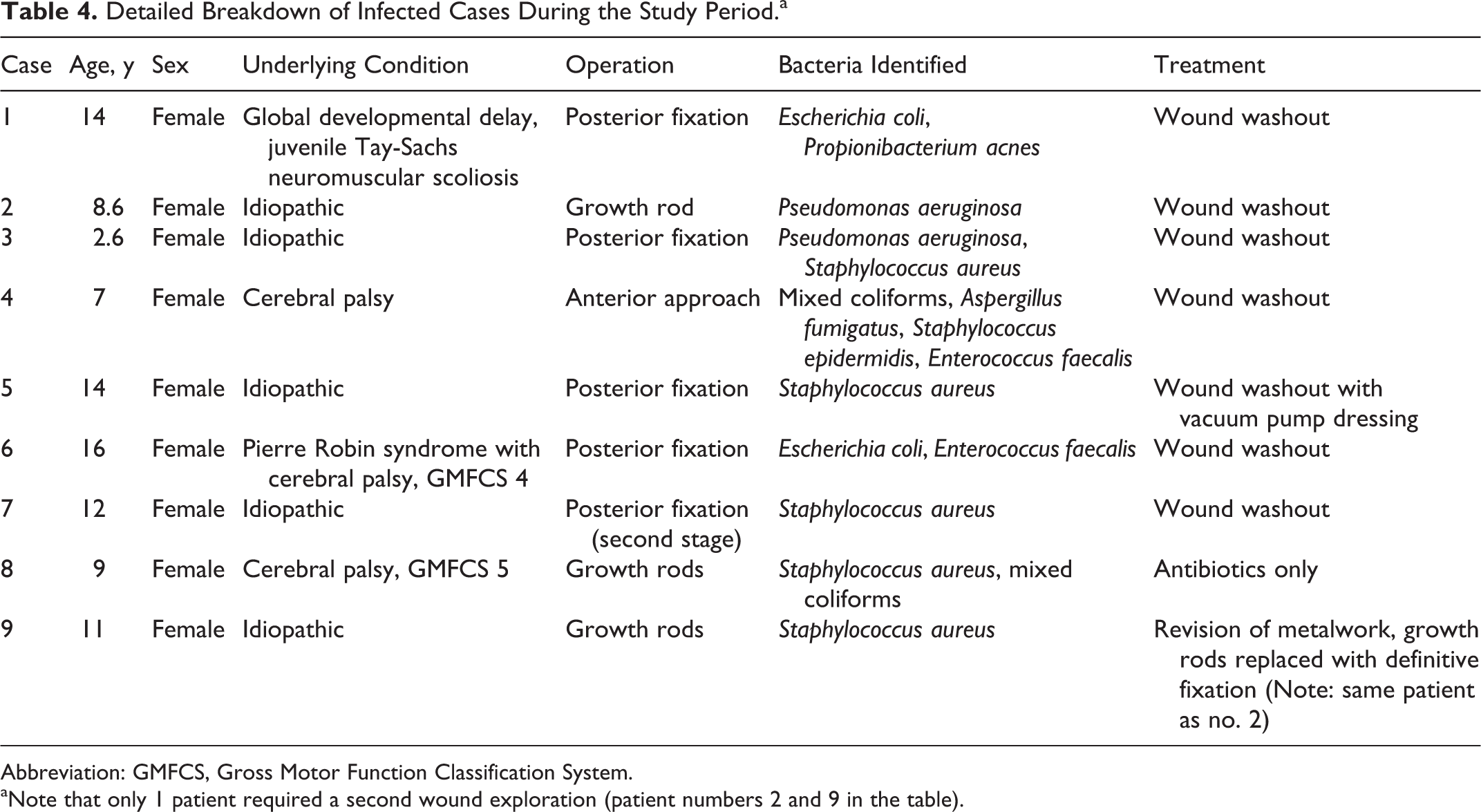
Abbreviation: GMFCS, Gross Motor Function Classification System.
aNote that only 1 patient required a second wound exploration (patient numbers 2 and 9 in the table).
Operative Categories
Fusion procedures with fixed rod insertion, growth rod insertion, planned and emergency revision surgery, and osteotomies.
Discussion
Health care–associated infections (HCAIs) have a significant and potentially preventable impact on patient care. Currently for all hospital inpatients in the United Kingdom, 20% of HCAIs are SSIs. This percentage of the whole has shown a progressive increase year on year from 14% in 2008. 11 This seems to be due to improved prophylaxis against other HCAIs rather than a rise in SSIs themselves. The general risk for patients undergoing surgical procedures developing an SSI remains static at 5%, 12 suggesting that there remains scope for intervention.
Cost analysis for SSI treatment ranges between £814 and £6626 per episode for all types of operations. 12 Given the inherent high cost of spinal surgery, it can be inferred that pediatric SSIs are on the upper end of this spectrum. These costs largely reflect extra interventions, nursing care, and additional therapies. Not reflected in this cost analysis are the risks of reoperation. In one series, 50% of the patients who developed infection following scoliosis surgery required removal of their metalwork, and 44% had worsening of their deformity as a result. 9 In addition, these costs are certainly an underestimate: Incidences of infection treated by general practitioners in the community tend to go unreported. Furthermore, these costs do not represent patient distress, loss of productivity to the unit, and litigation. Figures from the United States dwarf those from the United Kingdom, with the cost of a single episode of SSI rising as high as $961 722. 10
Patients with neuromuscular diagnoses have an increased risk of SSI compared to those with idiopathic deformities. With neuromuscular conditions, the spinal deformity is frequently one of many comorbidities in a generally more vulnerable patient. Associated factors include reduced mobility, recurrent chest infections, recurrent urinary tract infections, poor nutrition, limited ability for self-care, and increased dependence. Each of these aspects increases the risk of SSI, with a recognized relative risk ratio of 8.9 compared to those with idiopathic scoliosis. 8 Our results support this trend. Although neuromuscular cases made up 34% of the total number of patients, the incidence of infections seen was 50% of the total. It is also interesting to note that the organisms in this study for the neuromuscular cases were predominantly mixed cultures of fecal organisms, contrasting with the S aureus trend seen in the idiopathic cases. Nonetheless, analysis of the data reveals that although the neuromuscular cases had a predictably higher rate of SSI than the idiopathic cases, the protocol has been effective with them as well. The initiation of the protocol led to an average infection rate in idiopathic cases of 2.1% per patient. The per patient risk of infection in neuromuscular cases was only marginally higher at 3.3%.
Appropriate bathing reduces the risk of SSI, as recognized by both the British NICE guidelines 12 and by the World Health Organization. 13 Reducing the carriage of methicillin-resistant S aureus (MRSA) is beneficial, 14 with 44% of S aureus infections currently demonstrating methicillin resistance. 15 Although these guidelines do not recommend a specific detergent, Octinesan (Schulke & Mayr UK Ltd, Sheffield, UK) is endorsed by the NHS’s Infection Prevention Control Centre and is effective against MRSA. Patients are prescreened for MRSA prior to admission, and all receive Octinesan bathing on the night before the operation and on the morning of surgery.
The protocol rationalized the immediate preoperative skin preparation to 2% chlorhexidine (“double strength”). Most skin preparations are in essence either iodophor or chlorhexidine based. Iodine acts as an oxidizing agent, damaging the sulfhydryl groups of bacterial proteins as it dries. Chlorhexidine breaks down bacterial cell walls and starts to work within 20 seconds. Some evidence suggests that chlorhexidine-based preparations are more effective, 16,17 other reviews are less conclusive. 18,19 The new protocol harnesses both mechanisms through their combined use. Chlorhexidine is used for the initial skin preparation. Once the incision has been made, 7.5% aqueous betadine-soaked swabs are used to cover the wound edges throughout the procedure (Figure 2). A large, betadine-soaked swab is folded and applied to each side of the wound such that the skin edge and superficial centimeter of exposed tissue were covered. A nylon continuous suture is applied from the cranial to caudal end of the wound securing the swab in this configuration. This does not interfere with either tissue access or fluoroscopic visualization.

Aqueous betadine (7.5%)–soaked swabs applied to wound edges.
Allogenic blood transfusion increases the risk of surgical site infection, 20 -22 with a reported odds ratio of 3.3 for developing an SSI when more than 2 units are transfused. 23 Methods to reduce blood loss include controlled mild hypotension with a mean arterial pressure of 65 to 70 mm Hg, meticulous hemostasis, the use of a cell-saver device, tranexamic acid, and topical procoagulant preparations. The protocol made these steps standard practice, including the use of the fibrin-based Surgiflo (Ethicon Biosurgery, Limerick, Ireland) at the screw insertion points and ad hoc throughout the operation when bleeding is encountered. This expedited hemostasis reduces both blood loss as well as operative time, another potential factor in developing an SSI. 5
Wound irrigation reduces the amount of debris that harbors infection and may reduce the microbial count itself. The addition of iodine has been shown to have no benefit, and the recommended amount of lavage varies with different centers. 24 The multidisciplinary team (MDT) consensus was to use 3 L of pulsed normal saline following the insertion of metalwork.
Theatre management techniques such as reducing the amount of staff present to the minimum and utilizing laminar flow systems are well established, 25 and were already in use prior to 2013. However, the MDT analysis determined that there was no established protocol for surgical glove changes. The evidence for sterile glove use is varied, 26,27 but there is evidence and a degree of common sense to suggest that the longer the operation, the more likely the surgeon’s hands are to be contaminated. 28 The recommendation of the MDT was to use double gloves, changing the outer layer prior to the insertion of metalwork and again prior to closing the skin edges, and at other times during the surgical procedure if contamination of the gloves was suspected.
The MDT reviewed the antibiotic prophylaxis. Although in 23% of clinically suspected SSI no organism is identified, 29 a 2017 study of HCAIs in the United States demonstrated that 83% of infections were due to just 8 common pathogens. Staphylococcus aureus represented 16% of the total. The remaining organisms included low-virulence organisms such as Propionibacterium acnes (now described as Cutibacterium acnes) and coagulase negative staphylococcal species. Others included fecal organisms and those associated with urinary tract infections. Of note, preoperative catheterization includes a risk of bacteremia, even in asymptomatic cases. 30 The prophylactic regime was tailored accordingly. A single dose of gentamicin is administered to cover the catheterization and low-virulence organisms. Cefuroxime, efficacious against Staphylococcus species, is initiated prior to skin incision and continued for 48 hours postoperatively. The initial dosing schedule is 6 hourly, so a prolonged operation may result in a second dose. Following the pulsed-lavage, 1 g (500 mg if patient weight <20 kg) of vancomycin powder is lain down subfascially, covering a broad spectrum of species, including further cover against low-virulence organisms. 31 The safety and efficacy of topical vancomycin is becoming increasingly recognized, with evidence suggesting that systemic absorption is minimal. 2
The final criterion of the protocol was to maintain patient normothermia. An odds ratio of 2.2 for developing an SSI has been shown in patients whose temperatures dropped below 35°C. 32 In addition, hemostasis is impaired by hypothermia. Normothermia may therefore reduce operative blood loss. 32,33
Optimizing patients with neuromuscular conditions includes addressing aspects such as skin care and nutrition. This is beyond the scope of this work. The aim was to produce a robust, reproducible protocol for the reduction of SSIs in pediatric spinal deformity operations applicable to all patients. The need for this is well established, both locally and globally. The results support the strength of the protocol.
Potential weaknesses of the study include the fact that the protocol documents several separate interventions, and the results rely on the strength of the whole rather than any individual aspect. This reflects the multidisciplinary process as much as the fact that each individual intervention when studied in isolation has a relatively modest odds ratio for reducing infection. The protocol therefore maximizes these benefits by introducing a cumulative effect.
A further limitation is the omission of lengths of surgery. In this work, the number of operated vertebral levels was used as a surrogate for this variable. As described, there was no difference in the average number of operated levels between the infected and the noninfected cohort. However, a more accurate analysis would be useful. As the data set continues to grow, this is an interesting proposal for further work, including variables such as implant density and experience level of the individual surgeons.
Another consideration is the so-called “Hawthorne effect.” 34 Paraphrased, this suggests that with any intervention the process of studying it in and of itself can have positive effects. In this case, the team would have been mindful of the fact that they would have been under the microscope. However, with over 4 years of study and over 400 operations, this effect would certainly have been diluted with time. As our data demonstrates, the rapid drop in infections with the initiation of the new protocol has been consistent and sustained.
At present, the work reflects a minimum follow-up of 3 months. The prospective data collection continues, and a 2-year follow up of this cohort will be forthcoming.
Conclusion
The multidisciplinary approach adopted at the unit with standardized measures significantly and consistently reduced SSIs in pediatric scoliosis surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.