
Abstract
Study Design:
Systematic review and meta-analysis.
Objectives:
To determine the efficacy of intrawound treatments in reducing deep surgical site infections (SSIs) in instrumented spinal surgery.
Methods:
The electronic databases MEDLINE, EMBASE, and Cochrane were systematically searched for intrawound treatments for the prevention of SSIs in clean instrumented spine surgery. Both randomized controlled trials and comparative cohort studies were included. The results of included studies were pooled for meta-analysis.
Results:
After full text- and reference screening, 20 articles were included. There were 2 randomized controlled trials and 18 observational studies. Sixteen studies investigated the use of intrawound antibiotics, and 4 studies investigated the use of intrawound antiseptics. The relative risk of deep SSI for any treatment was 0.26 (95% confidence interval [CI] 0.16-0.44, P < .0001), a significant reduction compared with controls receiving no treatment. For patients treated with local antibiotics the relative risk was 0.29 (95% CI 0.17-0.51, P < .0001), and patients treated with local antiseptics had a relative risk of 0.14 (95% CI 0.05-0.44, P = .0006).
Conclusions:
Both the use of antibiotic and antiseptic intrawound prophylactics was associated with a significant 3 to 7 times reduction of deep SSIs in instrumented spine surgery. No adverse events were reported in the included studies.
Keywords
Introduction
Surgical site infections (SSIs) are serious adverse events with substantial patient morbidity and increased mortality. 1 The incidence of SSIs is highly dependent on the type of surgery; in spinal surgery, the overall incidence is around 4%. 2 The incidence is substantially higher in implant-related surgery, with SSIs developing in 9.4% of patients undergoing instrumented spinal surgery for traumatic fractures and in up to 19.2% of patients undergoing pediatric deformity surgery. 3,4 SSIs in instrumented spinal surgery are a challenge to treat. 5 Besides having a profound impact on patients, SSIs are a substantial financial burden on the health care system as well, costing up to $30 000 per patient for patients undergoing orthopedic surgery. 6,7 With the increasing focus on preventing complications and limiting health care costs, finding new ways to avert SSIs is of critical importance. Aseptic surgical techniques and perioperative intravenous antibiotic prophylaxis have proven to be effective. 8 –11 For other measures like nasal Staphylococcus aureus decontamination, preoperative chlorhexidine baths, and many forms of surgical attire, the effect has not been shown unequivocally. 12 –14 In the past years, there has been an increased interest in additional decontamination of the surgical wound before closure. One of the strategies involves the application of antibiotics, like vancomycin, directly into the wound. 15 –17 Alternatively, antiseptic irrigation solutions are used, like povidone-iodine and hydrogen peroxide. 18 The former antiseptic is most often used, in varying concentrations. 18 Antiseptics have the advantage of not inducing bacterial resistance. They are, however, cytotoxic when used in high concentrations. 19,20 Current evidence regarding efficacy and side effects associated with the use of intrawound antibiotics and antiseptics is still limited. Therefore, their use is not generally adopted in clinical practice.
The aim of this study was to determine the efficacy and potential side effects of intrawound prophylactic treatments in instrumented spinal surgery. A secondary goal was to compare the different methods used as intrawound treatment. Since meta-epidemiological research has shown that for surgical research questions, both randomized controlled trials (RCTs) and well-designed observational comparative study designs should be analyzed, 21 –24 we included both to make this review as representative and comprehensive as possible.
Methods
This systematic review and meta-analysis was performed in accordance with the items outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement 25 and the Cochrane Handbook for Systematic Reviews of Interventions. 26 The electronic databases MEDLINE, EMBASE, and Cochrane were systematically searched for articles that investigated the use of intrawound treatments for the prevention of SSIs in all types of clean instrumented spinal surgery. We searched for all possible types of prophylactic wound treatment and all phrases that were synonymous with SSI. The complete syntax used for each database can be found in the appendix.
Eligibility Criteria and Study Selection
Studies were limited to articles published in English, German, or French until April 16, 2018, with no restriction on publication date. Articles were screened for eligibility by 2 independent reviewers (JVCL and WB). Any disagreement between the reviewers was resolved through discussion or, if no consensus was reached, through consultation of a third reviewer (MCK). Reference screening and citation tracking was performed to find additional relevant articles. Human, comparative studies that investigated clean, instrumented spinal surgery were included. Treatment had to be given peroperatively, inside the wound before closure, with the intention to prevent infection. Studies with a reported mean follow-up time of less than 3 months, studies from which deep SSI rates in instrumented patients could not be extracted, studies with treatments that were applied onto the implants instead of into the wound, and studies with treatments in which a prolonged effect was intended (eg, antibiotic bone cement) were excluded. To minimize the apparent risk of bias as a result of selection by indication (treatment allocation based on surgeons judgment), these studies were also excluded. 27
Data Collection and Study Quality Evaluation
Relevant study data was collected by one reviewer (JVCL) and checked by a second reviewer (SPJW). Disagreements were resolved through discussion. Deep SSI rates in instrumented patients were extracted from the article or were calculated by using the information reported in the article. We assessed the presence and extent of heterogeneity between studies based on data extracted from each article. Study quality for observational studies and randomized trials was determined using the Methodological Index for Non-Randomized Studies (MINORS) grading tool. 28 The articles were independently graded by 2 reviewers (JVCL and SPJW).
Statistical Analysis
We combined the studies in a random-effects meta-analysis to calculate the relative risk and the 95% confidence intervals (CIs) by using the restricted maximum likelihood estimator. 29 Due to the expected few cases in either group, a relative outcome measure was chosen in order to better illustrate differences. The Mantel-Haenszel method with a fixed-effects model was used to provide an unbiased pooled estimate. To gauge the effect of heterogeneity (ie, the different clinical settings and study methodologies), Tau2 was used as an estimate of the total amount of statistical heterogeneity. The I 2 index was used to quantify the influence of heterogeneity on the final result. Heterogeneity was considered relevant when I 2 was >50%. Publication bias, based on standard error, was explored with a funnel plot with random-effects pseudo–confidence limits.
To assess the effect of the different intrawound prophylactic methods, a subgroup analysis of both antibiotics and antiseptics was done. Furthermore, to assess the effect of study quality, a sensitivity analysis was done based on study quality. We arbitrarily divided the included studies in 3 groups, based on their MINORS score. Low-quality studies were defined as a MINORS score ≤12 (out of a maximum of 24). Medium-quality studies were defined as a MINORS score between 12 and 16, and high-quality studies were defined as a score ≥16.
Since the effect of prophylactic treatment was compared with historical control groups in many of the retrospective studies, the bias of a potential time-related effect caused by improved infection prevention over time was studied with a weighted regression analysis, by plotting the incidence of SSIs in the control groups against the year of operation. The Metafor package (R Foundation for Statistical Computing, Vienna, Austria, 2012) was used for all statistical analyses. A P < .05 was considered to be significant.
Results
Search
The search in the MEDLINE, EMBASE, and Cochrane libraries yielded a total of 4074 results. After removal of duplicates and title and abstract screening, 133 articles were eligible for full-text assessment. After review, 114 articles were excluded. Through reference screening and citation tracking, one additional article was found that matched the eligibility criteria. Finally, a total of 20 studies were included in the systematic review and meta-analysis. A PRISMA flowchart of this process can be found in Figure 1.
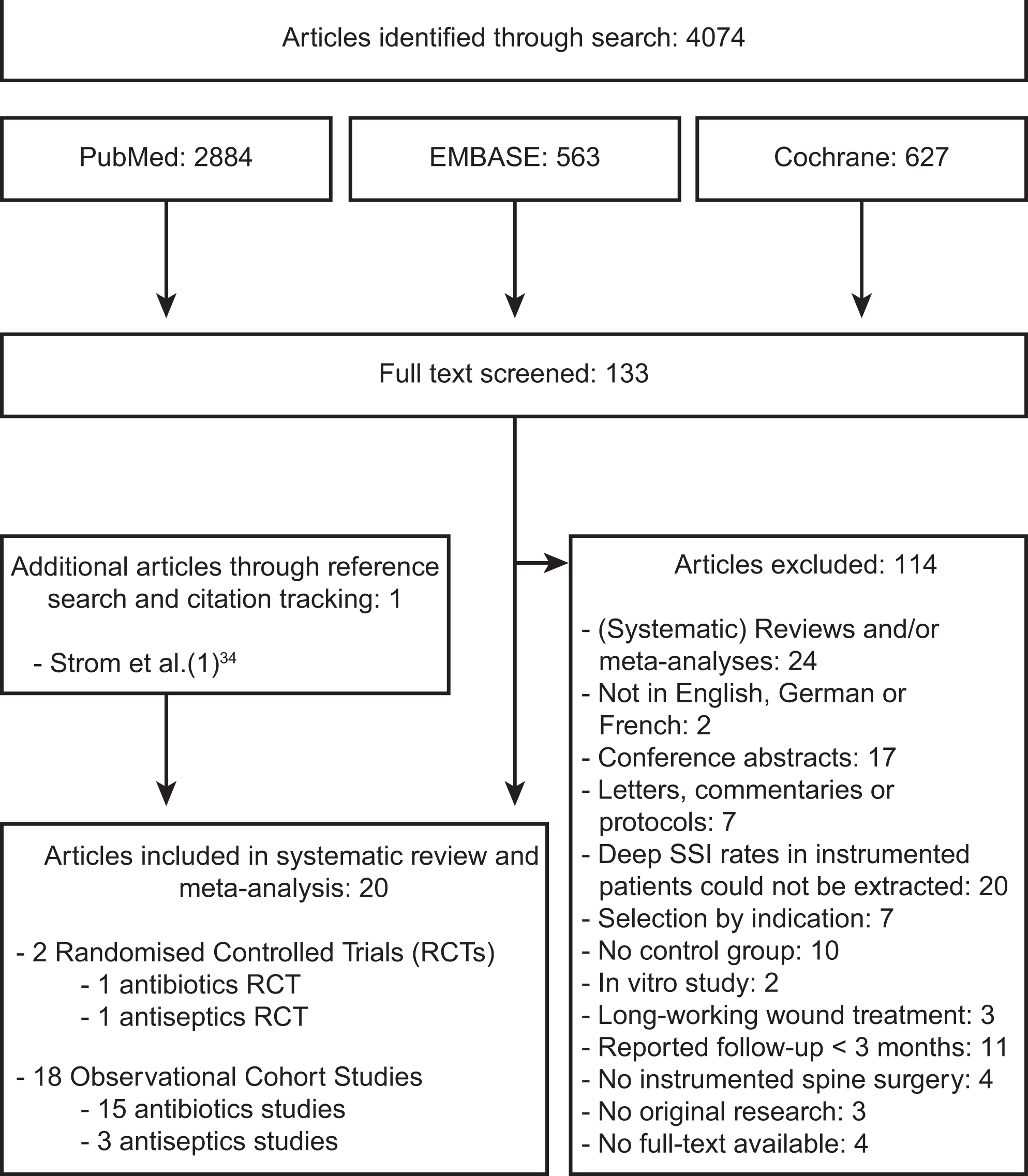
PRISMA flow diagram.
Baseline Characteristics
Of the 20 included studies, 2 were RCTs 30,31 and 18 were observational cohort studies (Table 1). 32 –49 Eight studies investigated many different types of spinal surgery. 30,38 –41,43,46,47 Five studies investigated deformity surgery, in either adults, 42 children, 45,48,49 or both. 32 One study investigated all types of spinal surgery in children. 44 Three studies investigated cervical spinal surgery, 34,36,37 and 3 studies investigated thoracolumbar or lumbar spinal surgery. 31,33,35 Sixteen studies investigated the use of intrawound antibiotics (all studies investigated vancomycin), 30,33 –42,44 –48 while 4 studies investigated the use of intrawound irrigation with antiseptics (all studies investigated povidone-iodine, one study also added hydrogen peroxide). 31,32,43,49 Baseline equivalence regarding characteristics between control and intervention groups was present in 11 studies 30 –35,37 –39,47,49 and unclear or not present in 9 studies. 36,40 –46,48 Characteristics of the intervention treatments and the use of perioperative antibiotic prophylaxis can be found in Table 2.
Study Demographics.
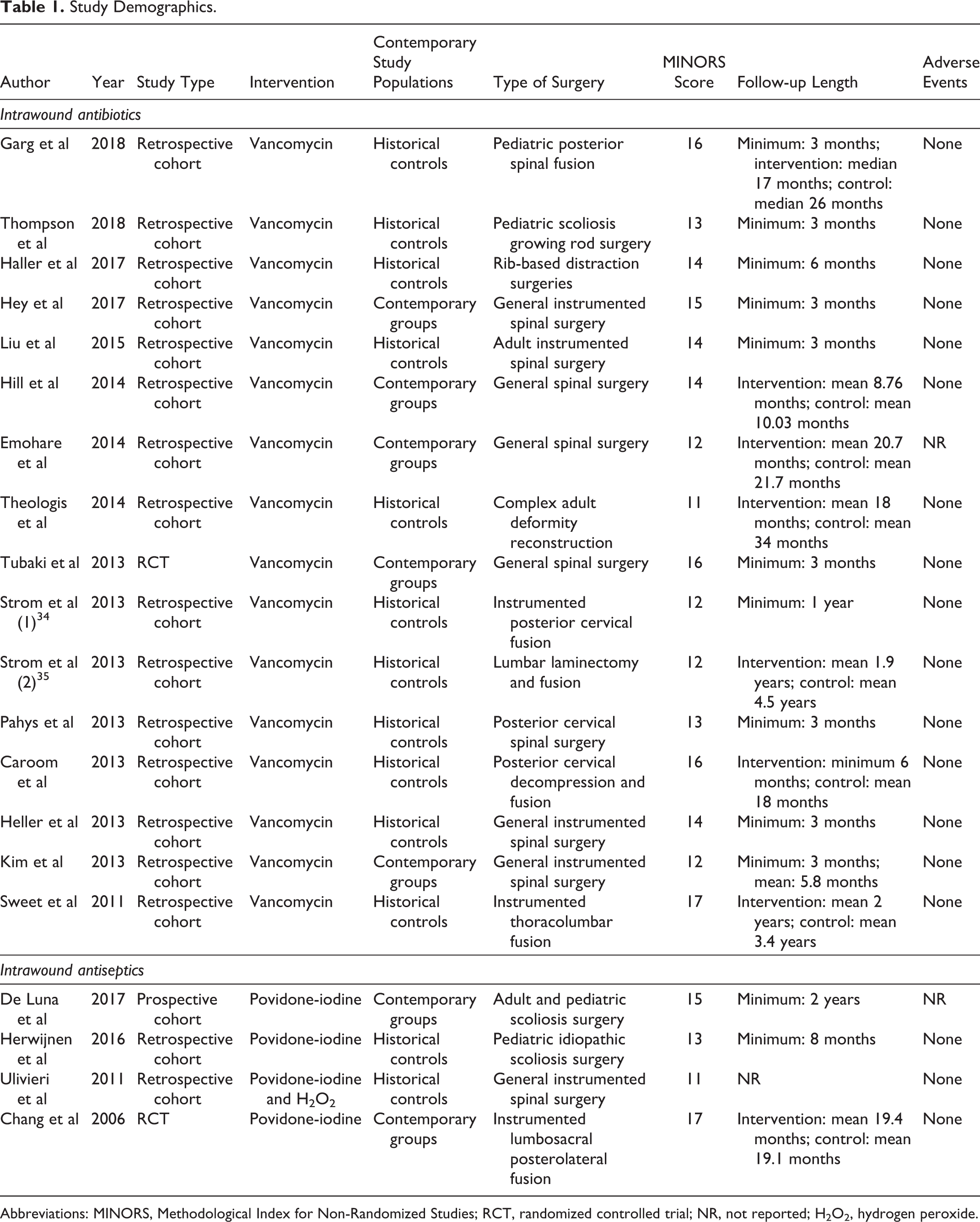
Abbreviations: MINORS, Methodological Index for Non-Randomized Studies; RCT, randomized controlled trial; NR, not reported; H2O2, hydrogen peroxide.
Treatment Characteristics
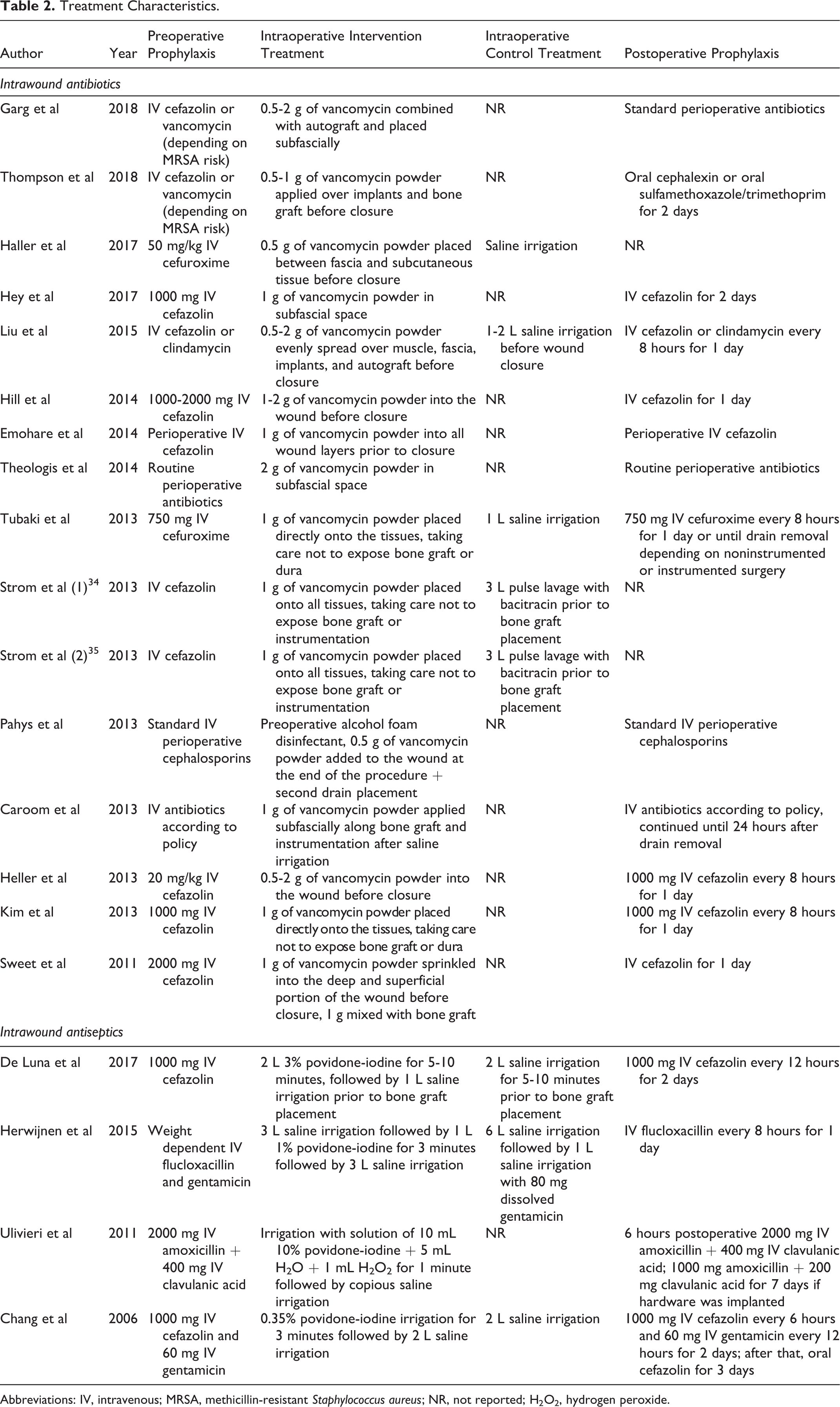
Abbreviations: IV, intravenous; MRSA, methicillin-resistant Staphylococcus aureus; NR, not reported; H2O2, hydrogen peroxide.
Fourteen studies provided a clear definition of SSI. In 5 studies, 32,44 –46,48 this was the (deep) SSI definition used by the Centers for Disease Control and Prevention. 50 Three studies defined SSI as a combination of clinical symptoms, elevated serum inflammation markers (erythrocyte sedimentation rate, C-reactive protein, white blood cell count), and bacterial culture results. 31,33,43 One study solely relied on the results of culture and/or radiographic findings. 39 Five studies used the need for reoperation or nonresponse to antibiotics, 36,38,42,47,49 and 6 studies did not provide a clear SSI definition. 30,34,35,37,40,41
Study Quality and Heterogeneity
The median MINORS quality score for all studies was 14 (range 11-17) out of a maximum score of 24. The 2 RCTs included in this review yielded a higher median score of 16.5 (range 16-17), while the observational studies had a median score of 13.5 (range 11-17). Some statistical heterogeneity was observed when looking at the pooled result with a Tau2 of 0.43. The I 2 index for heterogeneity remained <50% (I 2 = 38.6%) and may represent moderate heterogeneity.
Meta-Analysis
Deep SSIs were reported in 38 of the 3439 patients that received intrawound treatments (1.1%), compared with 189 deep SSIs in the 4529 control patients (4.2%). Table 3 contains the deep SSI rates for all studies. With this data, a meta-analysis was performed (Figure 2). When the results of the antibiotic interventions and the antiseptic irrigation interventions were pooled, the relative risk for deep SSI was 0.26 (95% CI 0.16-0.44, P < .0001). For the patients treated with local antibiotics, the pooled relative risk for deep SSI was 0.29 (95% CI 0.17-0.51, P < .0001) when compared with the control group. Patients that were irrigated with antiseptics had a pooled relative risk of 0.14 (95% CI 0.05-0.44, P = .0006). If heterogeneity would be ignored, the Mantel-Haenszel method that uses the fixed-effects model yields even lower relative risks with a relative risk of deep SSI for antibiotics and antiseptics combined of 0.23 (95% CI 0.16-0.33), a relative risk for antibiotics of 0.26 (95% CI 0.18-0.37), and a relative risk for antiseptics of 0.05 (95% CI 0.01-0.31).
Instrumented Deep Surgical Site Infection Rates.
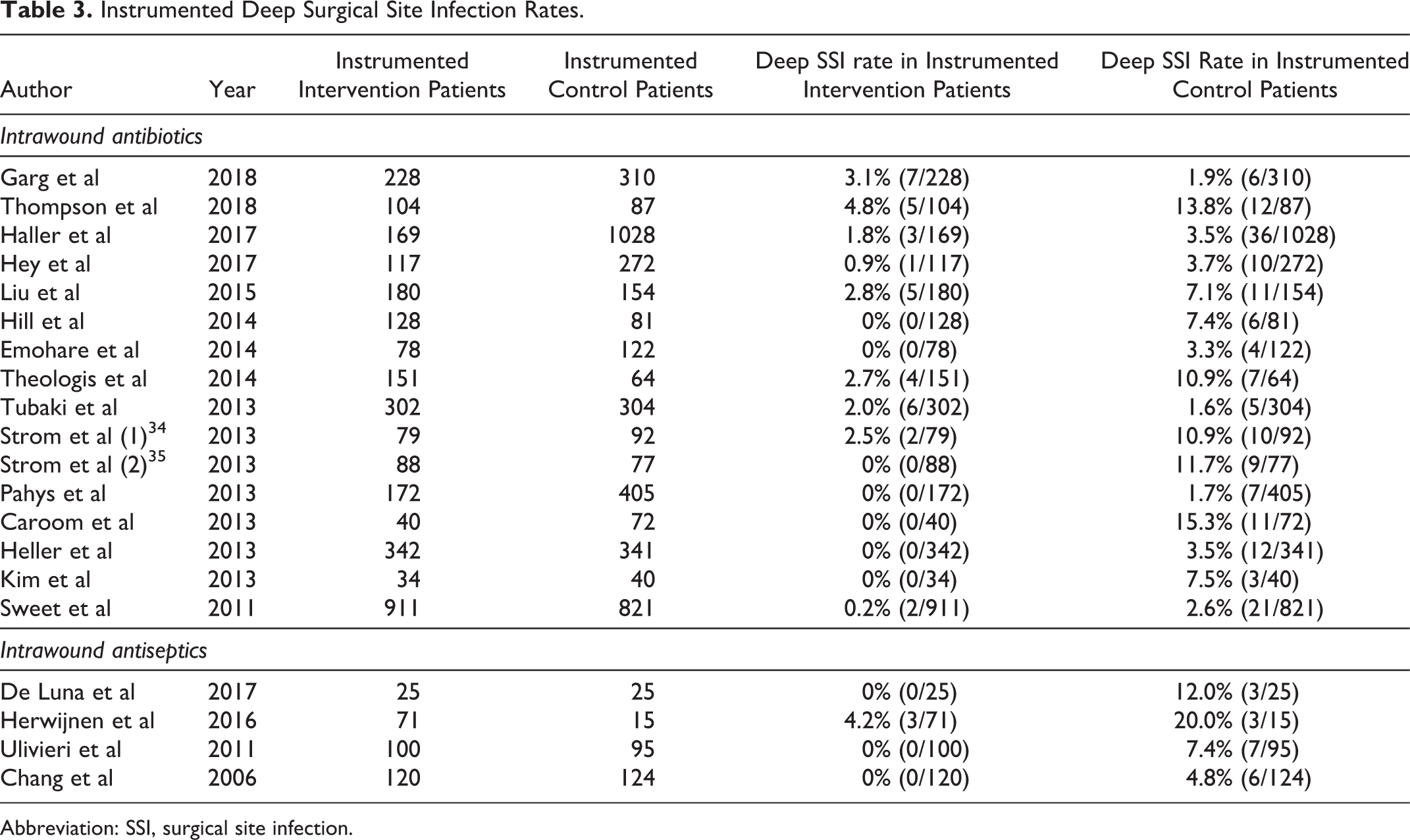
Abbreviation: SSI, surgical site infection.
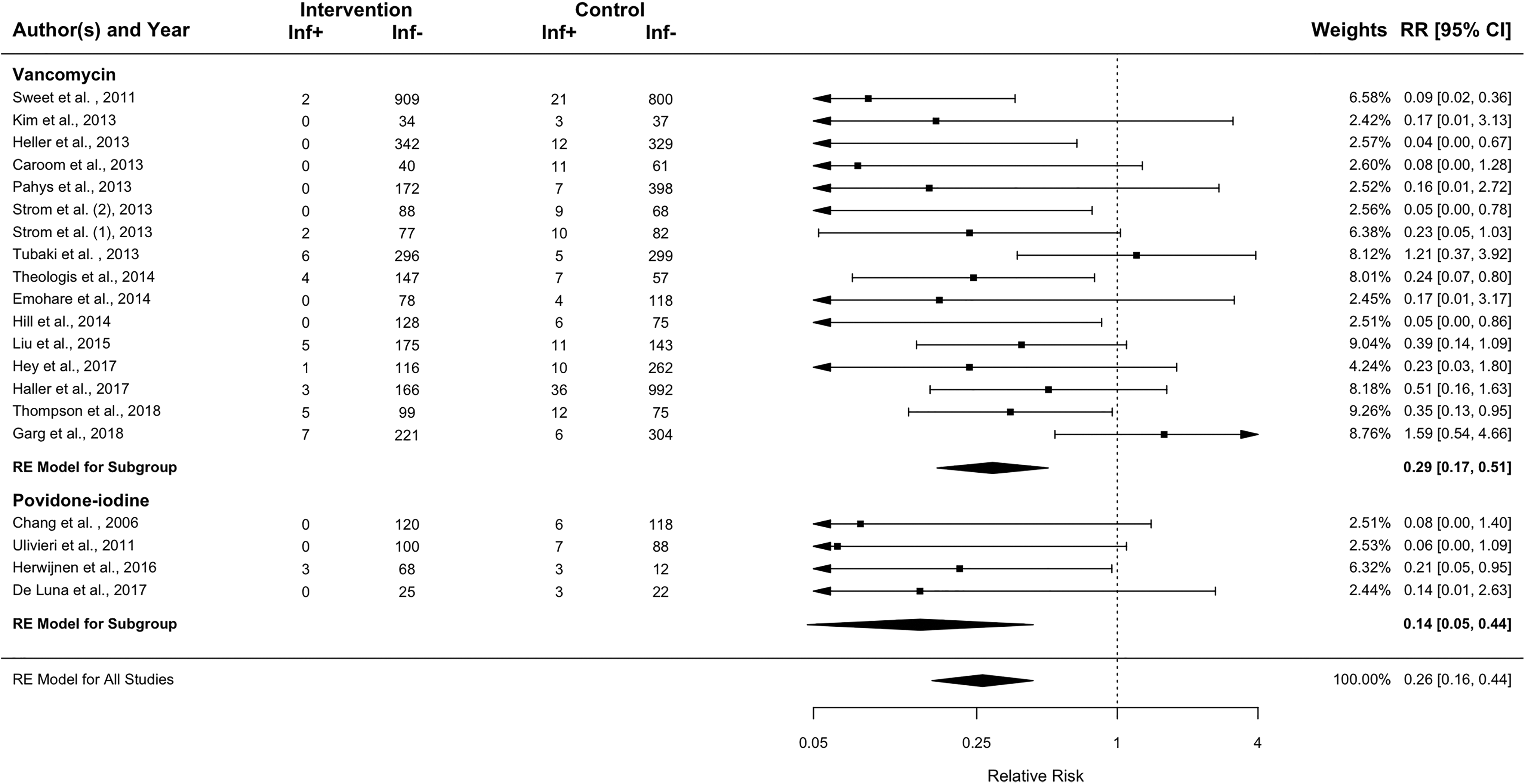
Forest plot of random effects model showing the relative risks and 95% confidence intervals of intrawound treatment compared to controls. A relative risk below 1 favors intervention treatment over control treatment.
Pooling the high-quality studies (5 studies) resulted in a relative risk of 0.33 (95% CI 0.08-1.42). Pooling the medium (9 studies) and lower (6 studies) quality studies resulted in a relative risk of 0.29 (95% CI 0.18-0.49) and 0.18 (95% CI 0.08-0.40), respectively, indicating that the lower quality studies may overestimate an effect.
The regression analysis of the incidence of SSIs over time shows that the risk of deep SSI in the control groups did not decrease but rather showed a nonsignificant, inclining slope (Figure 3). From this, we can conclude that in a period of about 12 years, the incidence of deep SSI has not significantly decreased in the study populations.
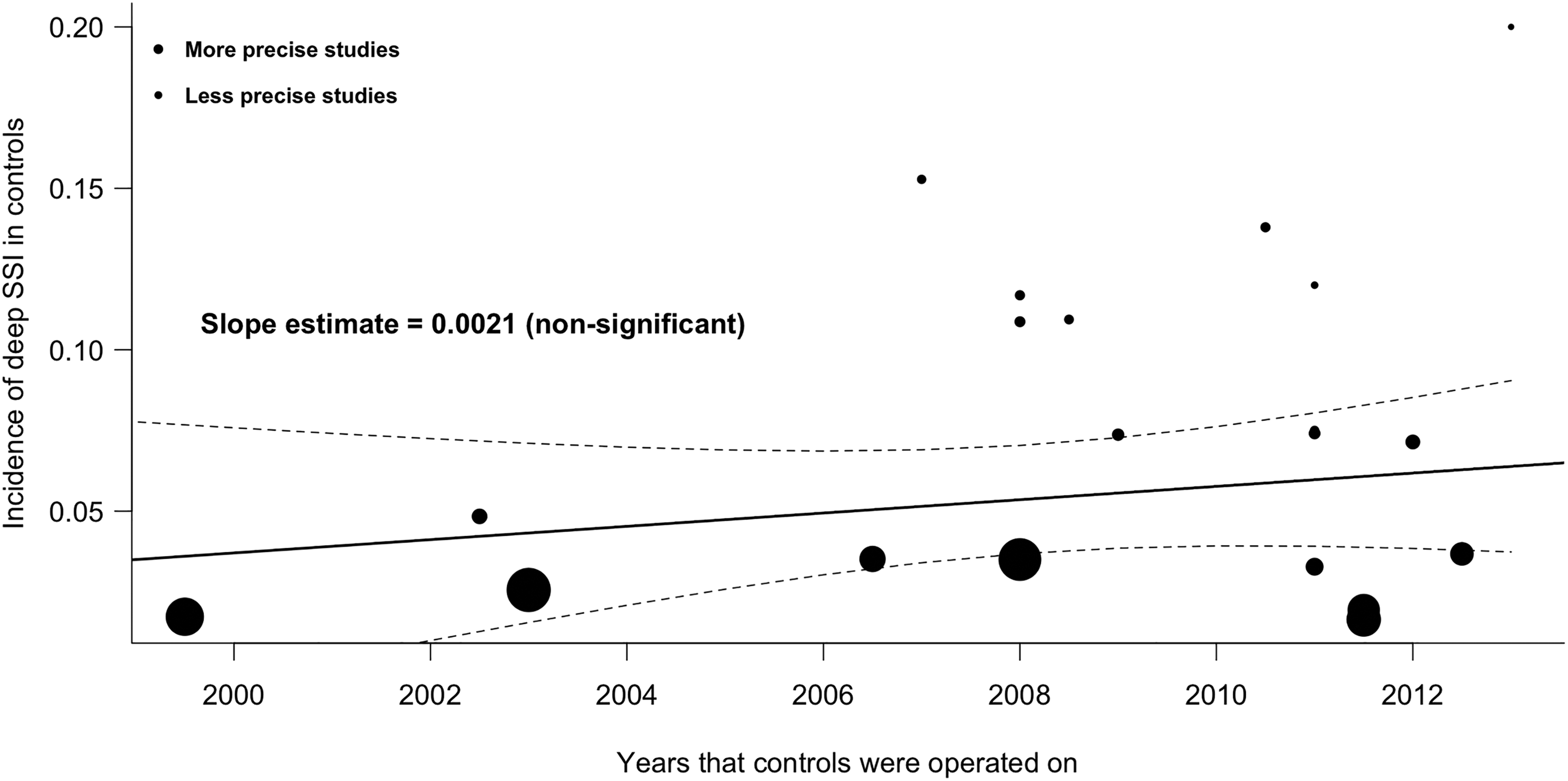
Weighted regression analysis of the incidence of SSI in control groups over time. Area between dashed lines is 95% confidence interval.
To analyze publication bias, a funnel plot was made that indicated asymmetry (Figure 4). This may be explained by the difficulty to publish studies without an effect (publication bias). However, since the standard error (the y-axis) of the relative risks is mathematically linked to the relative risk itself, studies with few events automatically have a high standard error, which causes the clustering in the lower left corner.
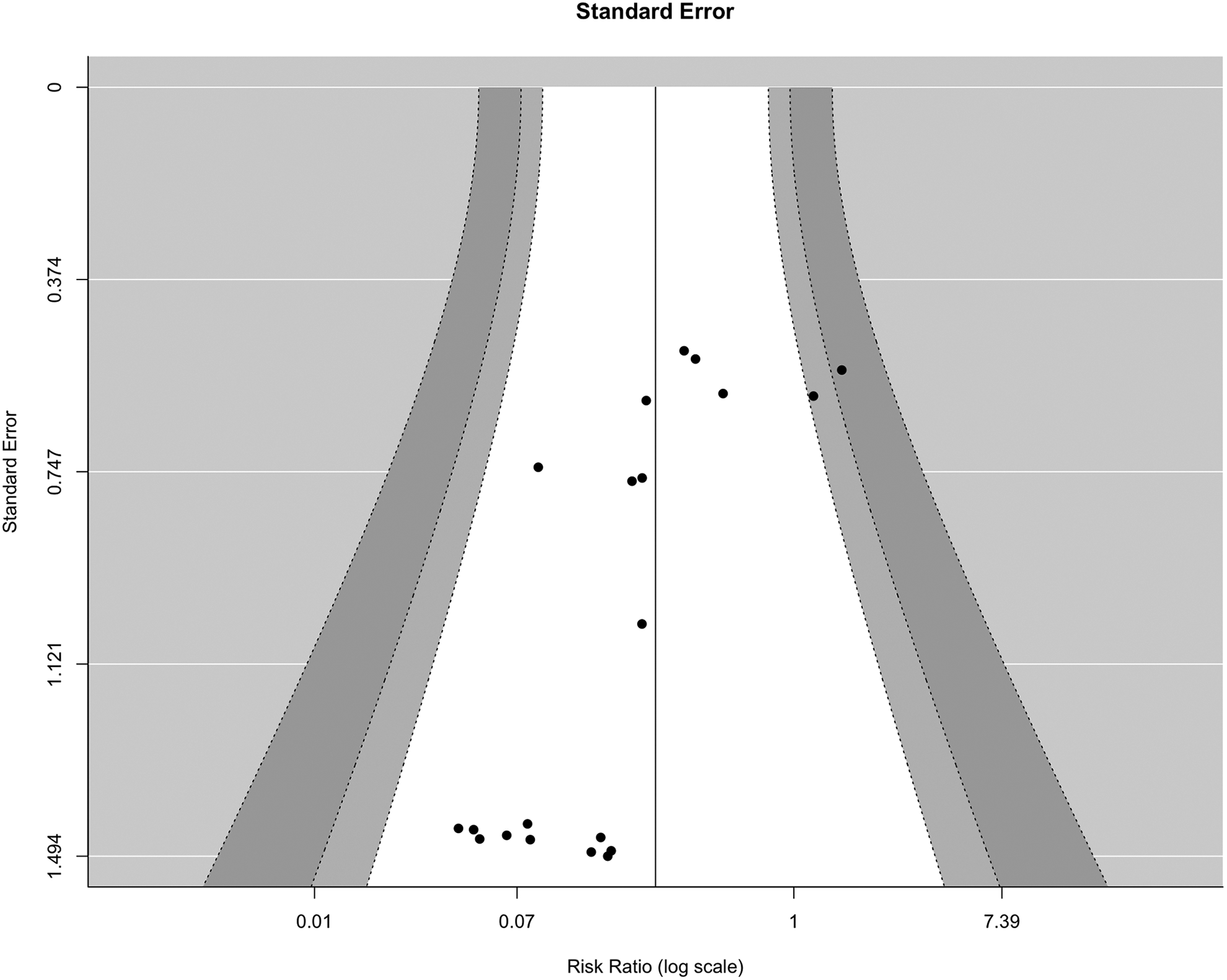
Funnel plot to assess publication bias. White area is within 95% pseudo–confidence interval limits.
Adverse Events
None of the included articles reported any adverse events such as renal toxicity, hypotension, or prolonged wound leakage. Two articles studied the potential effects of vancomycin on compromised bone healing in terms of nonunion rate. 33,34 Strom et al 34 found a nonunion rate of 5.1% for the treated group versus 5.4% for the control group (P = 1.000). Sweet et al 33 found no significant difference between the intervention and control groups either (0.33% for the treated group vs 0.49% for the control group). For the application of antiseptics, only Chang et al 31 investigated the nonunion rates and found no significant difference between treated patients and controls when using a 3-minute 0.35% povidone-iodine irrigation (10.8% vs 12.1%, P = .28).
Discussion
This systematic review and meta-analysis indicates a positive effect of perioperative intrawound prophylaxis to reduce the risk of SSI, with a relative risk of 0.26 (95% CI 0.16-0.44) compared with no intrawound treatment. When viewed separately, both antibiotics and antiseptics were significantly effective with relative risks of 0.29 (∼3 times lower risk) and 0.14 (∼7 times lower risk), respectively.
In the present review, we deliberately decided to include both RCTs and observational studies. The reason for this is that the RCT is no longer regarded as the only optimal design for surgical (intervention) studies, mainly due to inherent disadvantages. 22 –24,51 For example, double blinding is difficult or impossible. 52 Furthermore, surgical RCTs often have very low recruitment rates, which make them less representative of usual practice. 22,53 Due to the limited financial resources, sample size is often small and the follow-up period is short, which makes these studies less useful for complication research. 22,24,51,54,55 Observational comparative studies are by design more subjected to confounders and bias. However, a large part of confounding bias in observational comparative studies can be mitigated by sound methodological practices. In fact, meta-epidemiological studies have shown that both designs provide a comparable level of evidence for surgical research questions. 21,23,55 –57 To limit bias by selection on indication, we specifically addressed this item in the study selection process.
Interestingly, the only RCT investigating intrawound antibiotics found no effect of treatment. 30 However, this study investigated treatment in both instrumented and uninstrumented spine surgeries and therefore yielded a relatively low total SSI rate of 1.65%. The RCT investigating intrawound antiseptic prophylaxis in instrumented spine surgery found a reduction of deep SSIs, with a rate of 0% in the intervention group versus 4.84% in the control group. 31
To our knowledge, this is the first systematic review and meta-analysis in spinal surgery patients to pool data from both antibiotic and antiseptic intrawound treatments into a single meta-analysis. By focusing on deep SSIs (as opposed to superficial SSIs) and instrumented patients only, we also investigated the most clinically relevant complication in a vulnerable patient group, as deep SSIs in instrumented spine surgery patients often have disastrous consequences. We are also the first to analyze SSI rates against time in a meta-regression analysis. In a recent systematic review and meta-analysis of the prophylactic use of vancomycin powder in spine surgery, Evaniew et al 17 found results similar to our study (OR 0.19, 95% CI 0.08-0.47), but they included only 8 studies, included all types of patients (implanted and non-implanted) and both deep and superficial SSIs. Also, Bakhsheshian et al 58 found an effect of vancomycin powder in the prevention of deep SSIs in their meta-analysis of 12 studies with an odds ratio of 0.23 (95% CI 0.11-0.50). With respect to intrawound povidone-iodine treatment, the meta-analysis by Mueller et al 18 that included many different types of surgery and both contaminated and infected wounds also indicated a protective effect (OR 0.70, 95% CI 0.51-0.97).
Complications and Adverse Events
Based on the literature search that we performed, few adverse events have been reported of any intrawound prophylaxis. Vancomycin is most often used as intrawound antibiotic prophylaxis because of its potency to treat infections with gram-positive skin commensals such as Staphylococcus aureus and Staphylococcus epidermidis. Side effects mentioned in the literature are sudden hypotension, renal toxicity, ototoxicity, and the Red Man syndrome, 59 which, however, have only been reported in cases when vancomycin was administered intravenously. 59 The literature on adverse events when using intrawound vancomycin mostly consists of case reports, which mention one anaphylactic reaction with circulatory collapse 30 minutes after administration, 60 one patient with unexplained renal failure and 2 patients with transient hearing loss. 61 A recent systematic review of DeFrancesco et al found only one case of adverse drug reaction (transient rash) in almost 1400 children undergoing posterior spinal surgery for early onset scoliosis, a rate of only 0.072%. 62 In addition, patients in this study that had previously shown adverse drug reactions to intravenous vancomycin did not react to intrawound vancomycin powder. Nonunion of bone is another potential complication of local antibiotics at high concentrations. Edin et al 63 reported cytotoxicity occurring at vancomycin levels ≥10 000 µg/mL; Rathbone et al 64 found that concentrations ≥5000 µg/mL impaired the number of osteoblasts and their function; and a recent study by Eder et al 65 reported similar dose-dependent effects at concentrations of only 3000 µg/mL. The included clinical studies did not report increased nonunion rates. This is likely because the vancomycin levels in the drain fluid never exceeded 1500 µg/mL 33,65,66 and resorption into the blood was negligible, with mean serum levels not exceeding 2.5 µg/mL, far below the toxic serum concentrations. 33,66 It is important to note that vancomycin seems to be the least cytotoxic of studied antibiotics. Other antibiotics (eg, gentamicin) can be more harmful to osteoblasts and especially to cartilage when applied intra-articularly. 64 A serious disadvantage of intrawound antibiotics is its effect on antimicrobial resistance. Studying this phenomenon following intrawound use is difficult, but some studies that investigated culture findings after vancomycin use exist. One such study found no increase in the number of SSIs with vancomycin-resistant strains in patients treated with intrawound vancomycin. 67 It did, however, find significantly more infections with gram-negative bacteria. In contrast to this, however, another study found no differences in culture profiles when comparing the period before and after intrawound vancomycin. 68 Although these 2 studies have not yet shown the onset of vancomycin-resistant infections, the theoretical effects are definitely a cause for concern and therefore a preference for irrigation with antiseptics to antibiotics could be argued.
Most antiseptics are cytotoxic well before they achieve the minimal bactericidal concentration. 19 Povidone-iodine is an exception to this by achieving bactericidal concentrations before cytotoxicity occurs at the relatively low concentration of 1.3 g/L. 19 Although the included studies used substantially higher concentrations, no adverse events associated with the use of povidone-iodine were reported. Also, nonunion rates between treated patients and controls did not differ. 31
Limitations
Our study had several limitations. First, deep SSI rates in many different types of instrumented spinal surgery were studied. This makes general applicability of the observed results difficult. Second, a publication bias based on the included studies cannot be excluded. Third, many different patient demographics and highly divergent follow-up times were present in the included studies, which caused study heterogeneity. Fourth, the SSI definitions were not similar in the included studies and were not always clearly defined, making it easier for the investigators to be biased when defining whether someone developed an SSI based on the desired outcome (expectancy bias). Finally, the amount, concentration, and method of application varied across studies, as did the type, amount, and length of the perioperative antibiotics that were used.
Conclusion
Based on data from 20 studies, we found a 3 to 7 times reduction in deep SSIs in instrumented spinal surgery when antibiotic intrawound prophylaxis (relative risk 0.29, 95% CI 0.17-0.51, P < .0001) or antiseptic intrawound prophylaxis (relative risk 0.14, 95% CI 0.05-0.44, P = .0006) was used. No adverse events were reported. Although the nonstandardized methods and the large heterogeneity of the currently investigated interventions preclude recommendation for a specific treatment regime, the application of intrawound treatments in general should be considered for instrumented spinal surgery patients.
Footnotes
Appendix
Authors’ Note
No ethical committee approval was deemed necessary for this systematic review and meta-analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.