
Abstract
Study Design:
Evaluation of new technology.
Objectives:
To evaluate the utility of a novel biomimetic spine model as a surgical planning and education resource in the treatment of cervical spine deformities (CSD).
Methods:
Three patients with CSD were identified and synthetic spine models were manufactured to match the anatomical and biomechanical properties of each patient. Each model underwent 3 phases of surgical correction: maximum correction with no osteotomies performed, with posterior column osteotomies (PCOs) only, and with PCOs and a 3-column osteotomy (3CO). Lateral fluoroscopic films were obtained after each phase of correction for measurement of cervical lordosis. Surgeons were surveyed to obtain subjective feedback on the perceived model utility.
Results:
Each model began with a kyphotic deformity that was mobile, rigid, or fixed. The mobile model achieved successive lordotic correction with each phase of correction. The rigid and fixed models achieved much less correction with no osteotomies and PCOs only, and the majority of correction with 3COs. Each model predicted with varying, but overall high, accuracy the amount of correction achieved in each patient. The surgeons felt the model had very high utility as a surgical education platform.
Conclusions:
The models appeared to accurately replicate the gross anatomy and biomechanical performance of the patients’ spines. This high fidelity to the individual patient’s anatomy, bone quality, and segmental mobility resulted in a custom model that provides an invaluable learning platform for surgical education. These results suggest the models may have utility in surgical planning, but further studies are needed.
Introduction
Cervical spine deformities (CSD) are a complex and heterogeneous group of spinal disorders caused by a wide range of underlying conditions, including spondylosis, inflammatory arthropathies, neuromuscular conditions, neoplasms, infection, and trauma. 1 The most common type of CSD is cervical kyphosis, which in its most severe form can lead to a chin-on-chest deformity, or dropped head syndrome. 1 -4 The surgical treatment of CSD can be risky, with known complications, including dysphagia, vocal cord paralysis, tracheal or esophageal injury, vertebral artery injury/ cerebrovascular accident, spinal cord or nerve root injury, pseudoarthrosis, hardware failure, and wound complications. Early case series of surgically treated CSD noted high rates of significant complications. 5 -7 Although improvements in anesthesia and critical care techniques as well as in our surgical techniques and strategies have resulted in improved outcomes for these complex cases, the risks of CSD correction remain high. 3 The overall rate of neurological injury is reportedly as high as 23%, with major medical complications ranging from 3.1% to 44.4%, and mortality rates ranging from 3.1% to 6.7%. 8,9 Although several surgeons have provided general classification schema for various types of CSD, there remains wide disagreement among experts on the best surgical approach for a given deformity. 1,10 -12 In a recent study by the International Spine Study Group, a panel of 14 expert deformity surgeons demonstrated wide disagreement when asked about their recommended surgical treatment strategy for 18 cases of CSD. For even the least complex case, the panel showed a marked lack of consensus in all answer categories, including the surgical approach or approaches, the levels treated, and the presence or type of osteotomies. 4 Furthermore, there is a notable lack of data on the effectiveness and safety profiles of various surgical treatment strategies. As such, the surgical treatment of CSD remains highly variable with numerous acceptable but nonstandardized treatment algorithms. 1 -12 This variability can make planning for these procedures a difficult task and may compromise any attempt at standardized training for residents and fellows.
The primary challenge in determining which surgical strategies for CSD correction provide the best balance between effectiveness and risk mitigation is the inability to compare 2 or more strategies on the same patient. A potential solution to this challenge might lie in the recent development of custom 3-dimensionally (3D) printed spine models with high bony and ligamentous fidelity to human tissue. 13 -17 The increasing ability of 3D manufacturing technologies to mimic various human features portends the eventual development of a synthetic spine model with high anatomic and biomechanical fidelity. With this new technology, numerous identical models of the same patient can be manufactured and surgically corrected using various strategies, enabling us to begin comparing the effectiveness of different surgical strategies as applied to anatomically and biomechanically identical curve types. These types of models would also provide unique opportunities for residents and fellows to independently “perform” the critical portions of a complex procedure prior to the actual case, therefore improving the educational experience and preparation for a procedure. The potential utility of a patient-specific model with high biomechanical fidelity as applied to various types of CSD has yet to be determined. The purpose of this study was to evaluate the utility of a novel biomimetic spine model as a surgical planning and education resource in the treatment of CSD.
Materials and Methods
Institutional review board approval for this study was not needed as this was a study on the utility of a novel technology in surgical planning and education. The presented clinical cases have been de-identified and presented in terms of cervicothoracic curve parameters.
Biomimetic Spine Models
Three patients with CSD of varying type and severity were identified from the lead authors’ (J-CL and RS) clinical practices. See Table 1 for a summary of each patient’s demographic and cervical deformity characteristics. Each patient had high-resolution computed tomograms (CT) and bone densitometry scans performed as part of their preoperative workup. The CT scans were converted into stereolithography files for 3D printing of the patients’ anatomy, and the densitometry data was used to inform the printing process such that synthetic bone could be produced with biomechanical properties similar to each patient’s bone. 16 A flexible material was used to print the discs and longitudinal ligaments into the model to provide segmental range of motion. 13,15 Each model included vertebral bodies from occiput to mid-thoracic spine (the exact distal level depended on where the patient’s CT scan ended), as well as anterior and posterior longitudinal ligaments, intervertebral discs, posterior column ligaments, and radiolucent soft tissue (see Figure 1A-D).
Patient and Cervical Deformity Characteristics.a
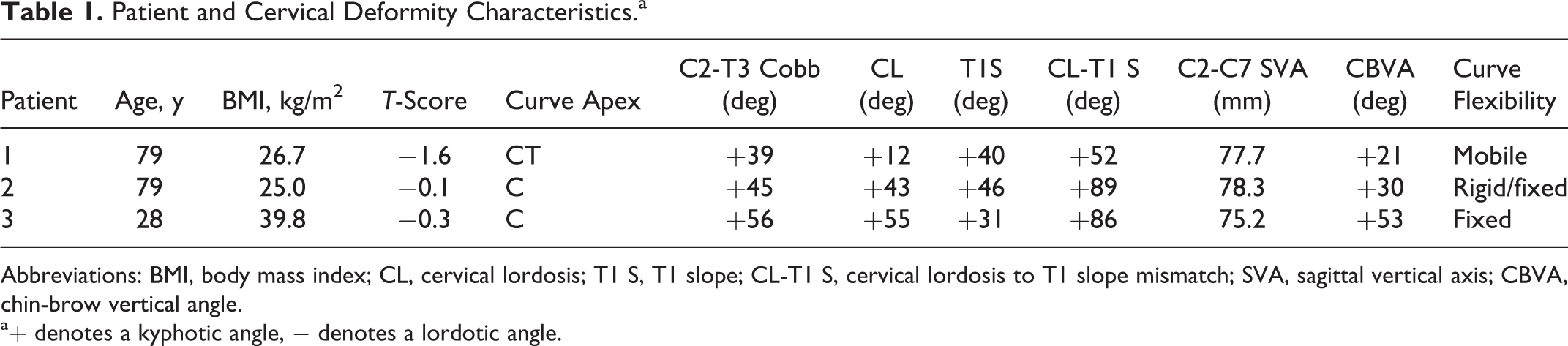
Abbreviations: BMI, body mass index; CL, cervical lordosis; T1 S, T1 slope; CL-T1 S, cervical lordosis to T1 slope mismatch; SVA, sagittal vertical axis; CBVA, chin-brow vertical angle.
a+ denotes a kyphotic angle, − denotes a lordotic angle.
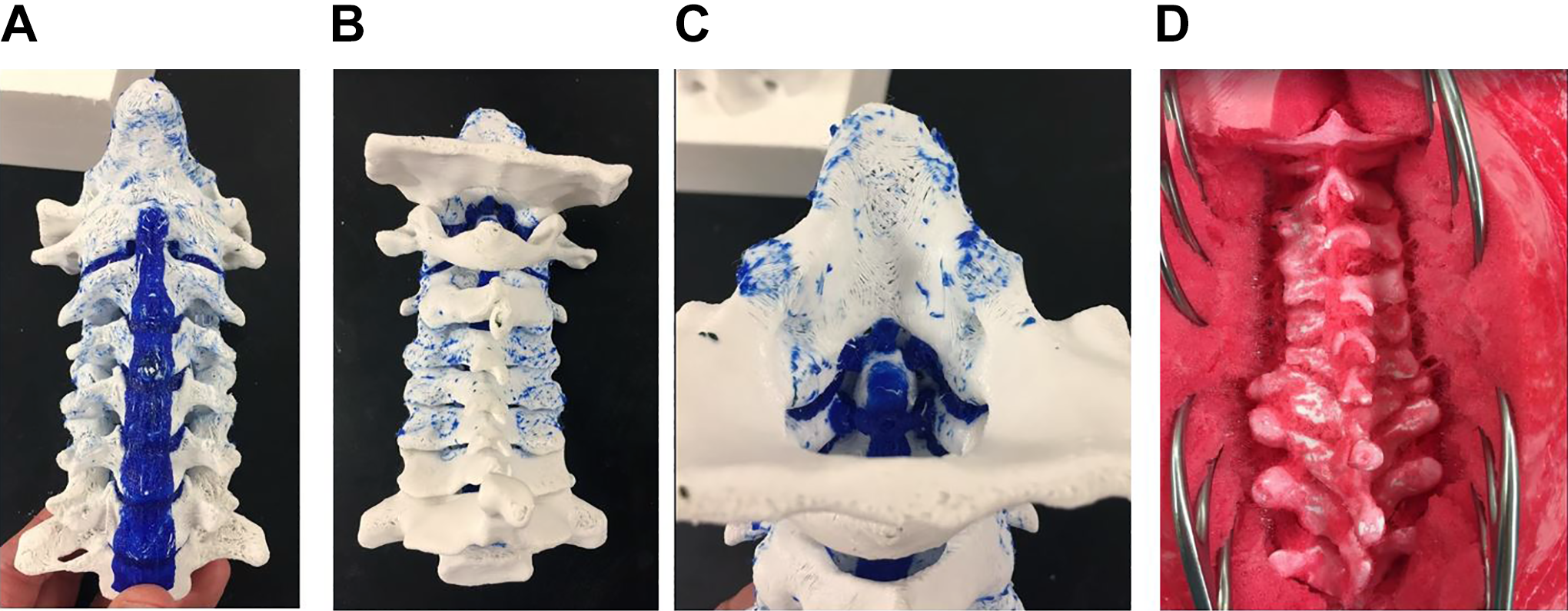
(A) Synthetic model of a normal cervical spine from an anterior view. The synthetic bone is white, the anterior longitudinal ligament and intervertebral discs are blue. (B) Photograph of the same model from a posterior view. (C) Photograph of the same model with a view of the dens, posterior longitudinal ligament, transverse atlantal ligament, apical ligament, and alar ligaments. (D) Photograph of a spine model in radiolucent soft tissue (red) with an open posterior exposure. The occiput is at the top of the picture and T3 is at the bottom of the picture. The left C2-C4 facets are fused in this model.
Data Collection and Analysis
Each synthetic model was taken to a vacant operating room where there was a complete surgical instrumentation set and c-arm fluoroscopy unit available. In each case, the synthetic model was exposed and had spinal fixation screws placed at the appropriate levels. Each model then underwent 3 phases of correction: maximum correction with no bony osteotomies performed, maximum correction with posterior column osteotomies (PCOs) only, and maximum correction with PCOs and a 3-column osteotomy (3CO). The correction achievable at each stage was considered maximum when further screw reduction or in situ bending resulted in either no increase in cervical lordosis or failure of spinal fixation screws.
Anteroposterior and lateral fluoroscopic films were obtained before and after each phase of deformity correction. Postcorrection lateral fluoroscopic views were used to measure cervical lordosis and the C2-T3 Cobb angle. All measurements were taken three times and averaged for a final measurement. For each model, measurements were compared across all 3 phases of correction, as well as to the correction achieved in the patient following the actual surgical procedure. No statistical comparisons were calculated as each model represented a different type of CSD, and the purpose of the study was to evaluate the model’s ability to respond appropriately to surgical correction. Finally, the attending surgeons (RS and J-CL) and fellow (MAB) performing the model corrections and actual patient procedures were anonymously surveyed on their impressions of the model’s utility as a surgical planning and surgical education platform for CSD. The survey consisted of 4 questions answered on a modified-Likert scale from 1 to 7, with 1 correlating to the most negative response, 4 to a moderate response, and 7 to the most positive response. The final question asked for comments about the perceived strengths and weaknesses of the models.
Results
Model Results
All 3 models underwent the 3 phases of surgical correction as described above. Models 1 and 2 underwent correction after patients 1 and 2 underwent their procedures, respectively. Model 3 underwent correction before patient 3 had surgery. Table 2 provides the final surgical procedure that each patient and their respective model underwent, as well as the amount of correction achieved in the models with each phase of surgical correction.
Model and Patient Surgical Corrections.a
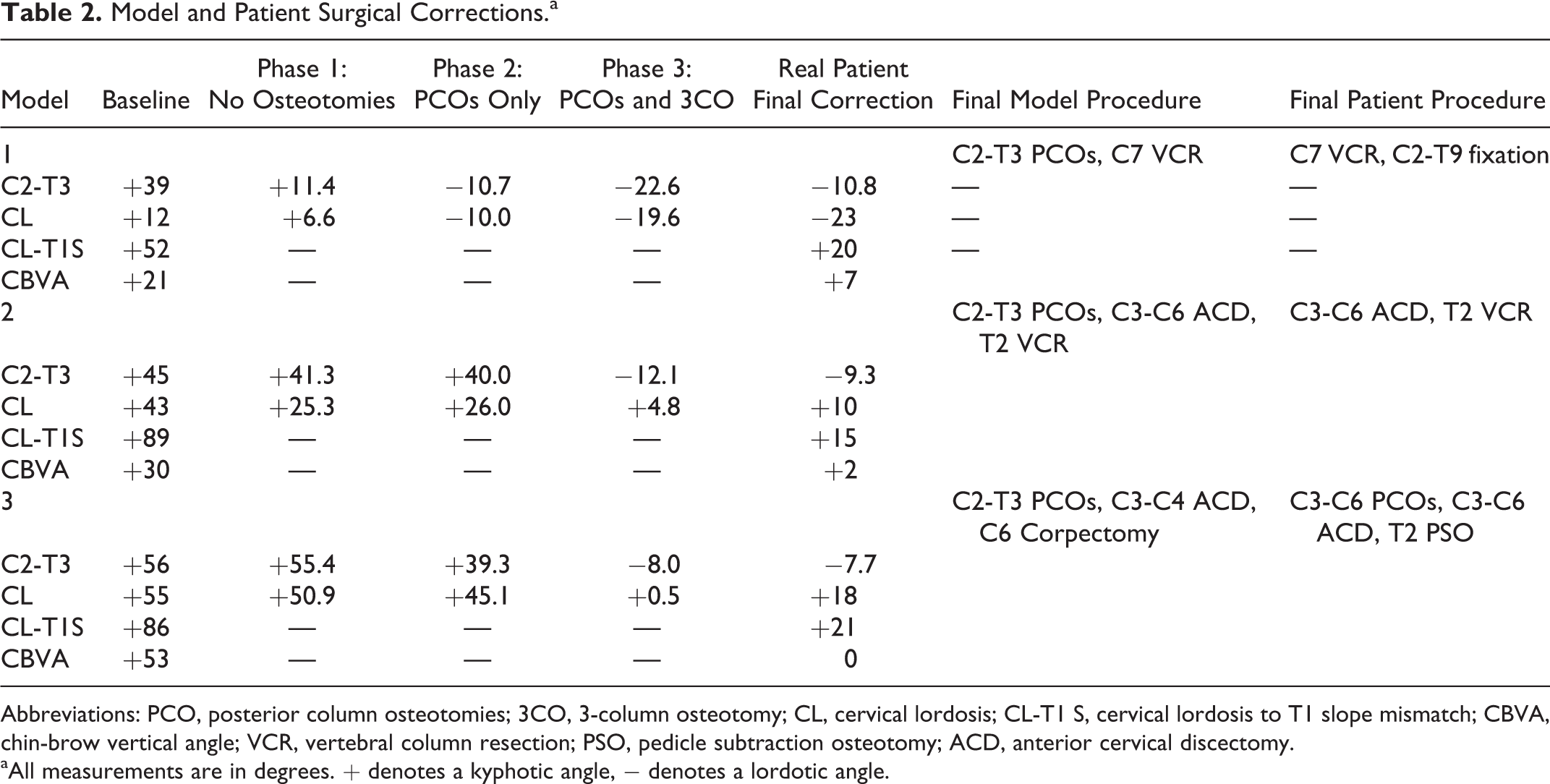
Abbreviations: PCO, posterior column osteotomies; 3CO, 3-column osteotomy; CL, cervical lordosis; CL-T1 S, cervical lordosis to T1 slope mismatch; CBVA, chin-brow vertical angle; VCR, vertebral column resection; PSO, pedicle subtraction osteotomy; ACD, anterior cervical discectomy.
aAll measurements are in degrees. + denotes a kyphotic angle, − denotes a lordotic angle.
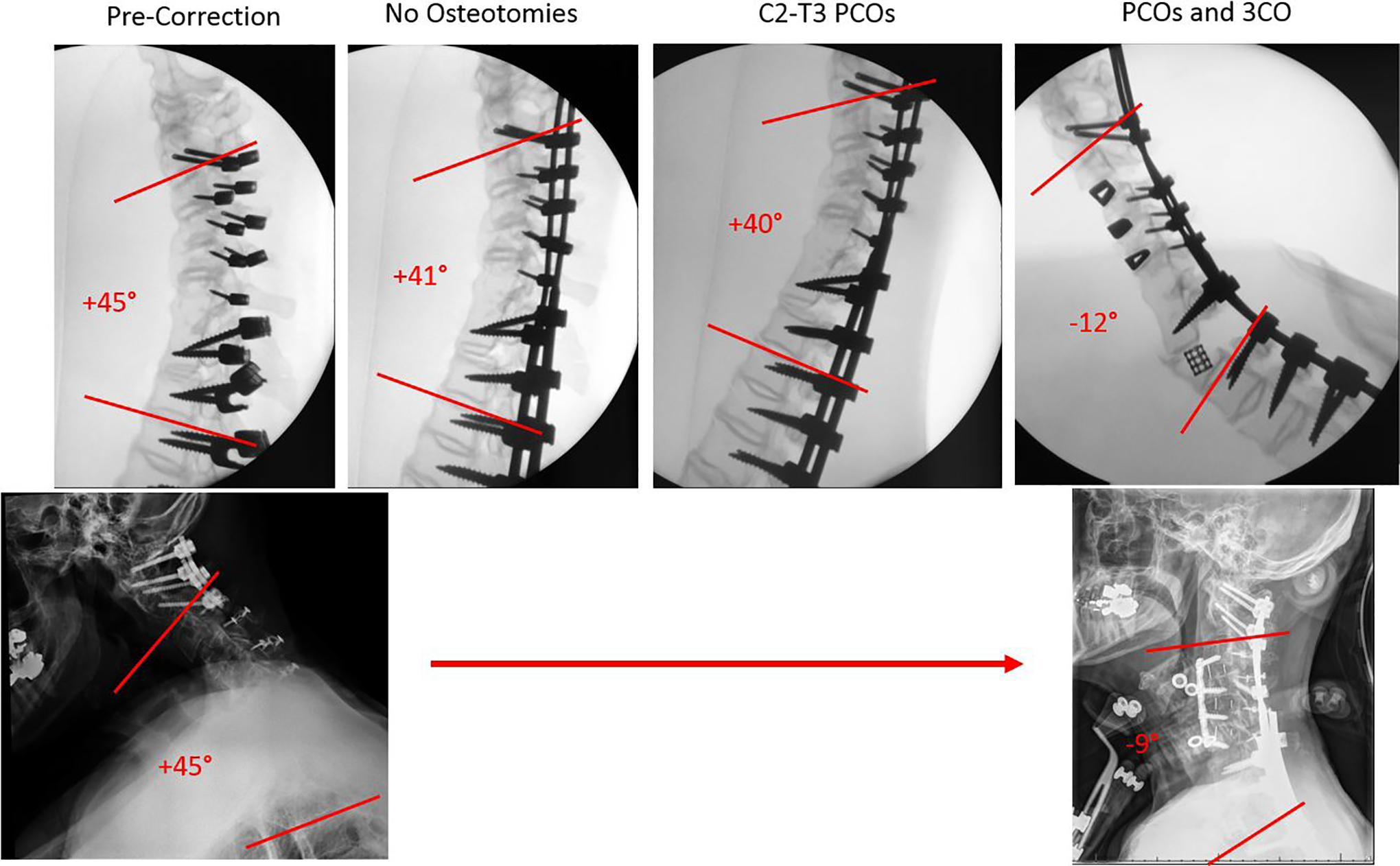
Model 1 represented a patient with a mobile chin-on-chest deformity secondary to cervical spondylosis and a wedged compression fracture at C7. Preoperative C2-T3 Cobb angle for the patient and model were +39°. Correction with no osteotomies achieved a C2-T3 Cobb angle of +11°, PCOs yielded additional correction to −11°, and finally the addition of a C7 3CO resulted in a final C2-T3 Cobb angle of −22°. Patient 1 achieved a final C2-T3 Cobb angle of −10.8° after undergoing the same 3CO at C7 and fewer PCOs (see Figure 2).
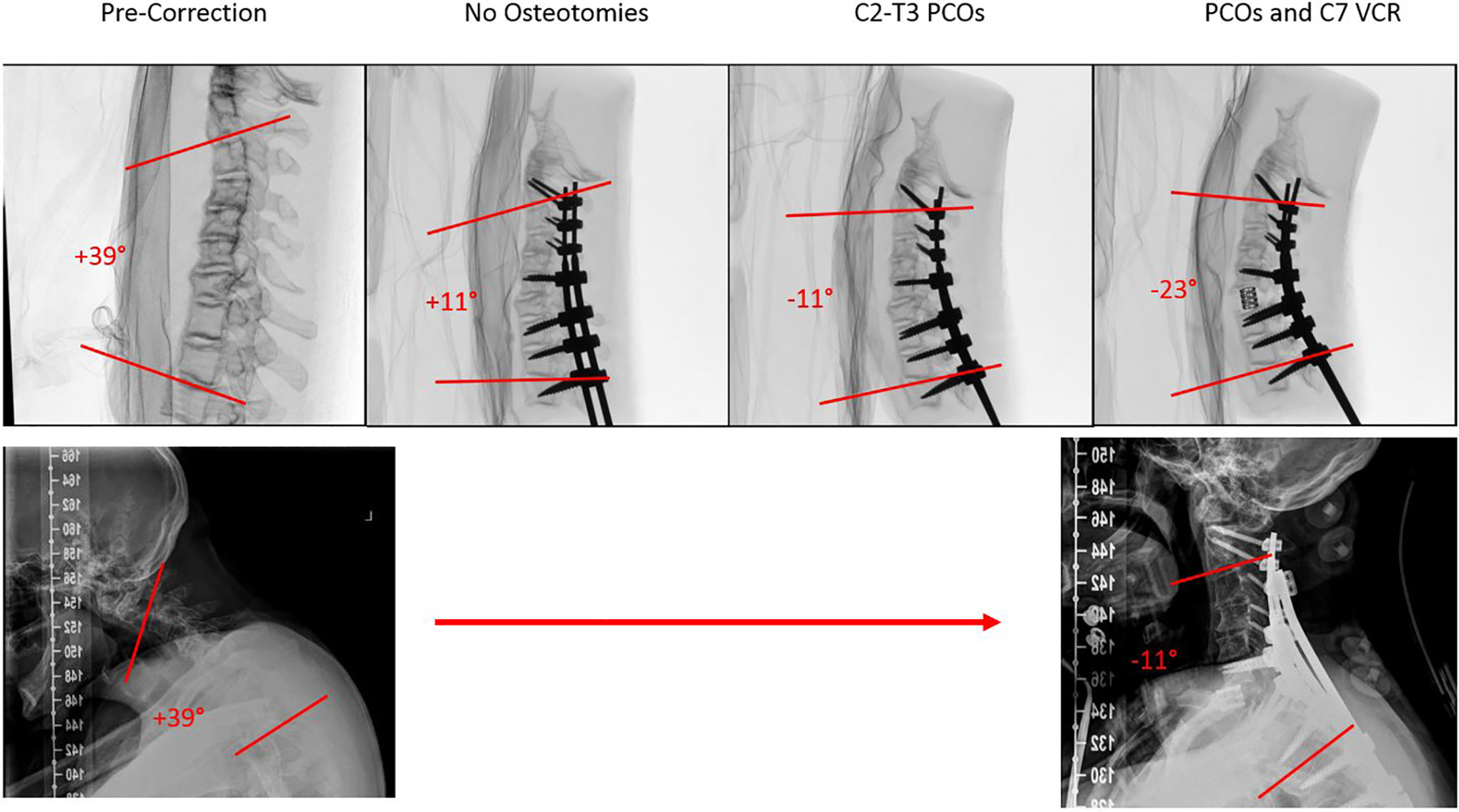
Lateral fluoroscopic views of model 1 and patient 1. Top row from left to right, lateral fluoroscopic views of model 1 in precorrection baseline, correction with no osteotomies, correction with posterior column osteotomies only, and correction with posterior column osteotomies and 3-column osteotomies. Bottom row from left to right, lateral radiographs of patient 1 preoperatively and following surgical correction.
Model 2 represented a patient with a CSD consisting of both mobile and rigid segments. This patient had undergone a previous C1-C2 fusion and had auto-fused from C4-C6 due to a large anterior bridging osteophyte, and from C6-T1 through the disc spaces. The upper thoracic discs were open but completely collapsed. Preoperative C2-T3 Cobb angle for the patient and model were +44°. Correction with no osteotomies yielded only 3° of lordosis, and the addition of PCOs only an additional 1° of lordosis. With the addition of C3-C6 anterior cervical discectomies and interbody graft placement, and a T2 3CO, a final C2-T3 Cobb angle of −12° was achieved. Having undergone the same procedure with fewer thoracic PCOs, the patient’s final C2-T3 Cobb angle was −9° (see Figure 3).
Lateral fluoroscopic views of model 2 and patient 2. Top row from left to right, lateral fluoroscopic views of model 2 in precorrection baseline, correction with no osteotomies, correction with posterior column osteotomies only, and correction with posterior column osteotomies and 3-column osteotomies. Bottom row from left to right, lateral radiographs of patient 2 preoperatively and following surgical correction.
Model 3 represented a patient with a globally rigid kyphoscoliotic CSD resulting from an aggressive inflammatory arthropathy that lead to the ossification of all the cervical facet joints and supportive ligaments of the cervicothoracic spine. Preoperative C2-T3 Cobb angle for the patient and model were +67°. Correction without osteotomies yielded 14° of lordosis, and the addition of PCOs yielded another 16° of lordosis for a C2-T3 Cobb angle of +37°. With a C3-C4 anterior cervical discectomy and uncovertebral facetectomy, as well as anterior C5 corpectomy and expandable cage placement, a final C2-T3 Cobb angle of −12° was achieved. The patient underwent C3-C7 PCOs, C3-C6 anterior cervical discectomies and interbody placement, and a T2 3CO to achieve a final C2-T3 Cobb angle of −8° (see Figure 4). The surgical plan for patient 3 was changed based on the experience gained while operating on the model, with the initial plan of an anterior-posterior procedure changed to posterior releases followed by anterior-posterior correction and fixation.
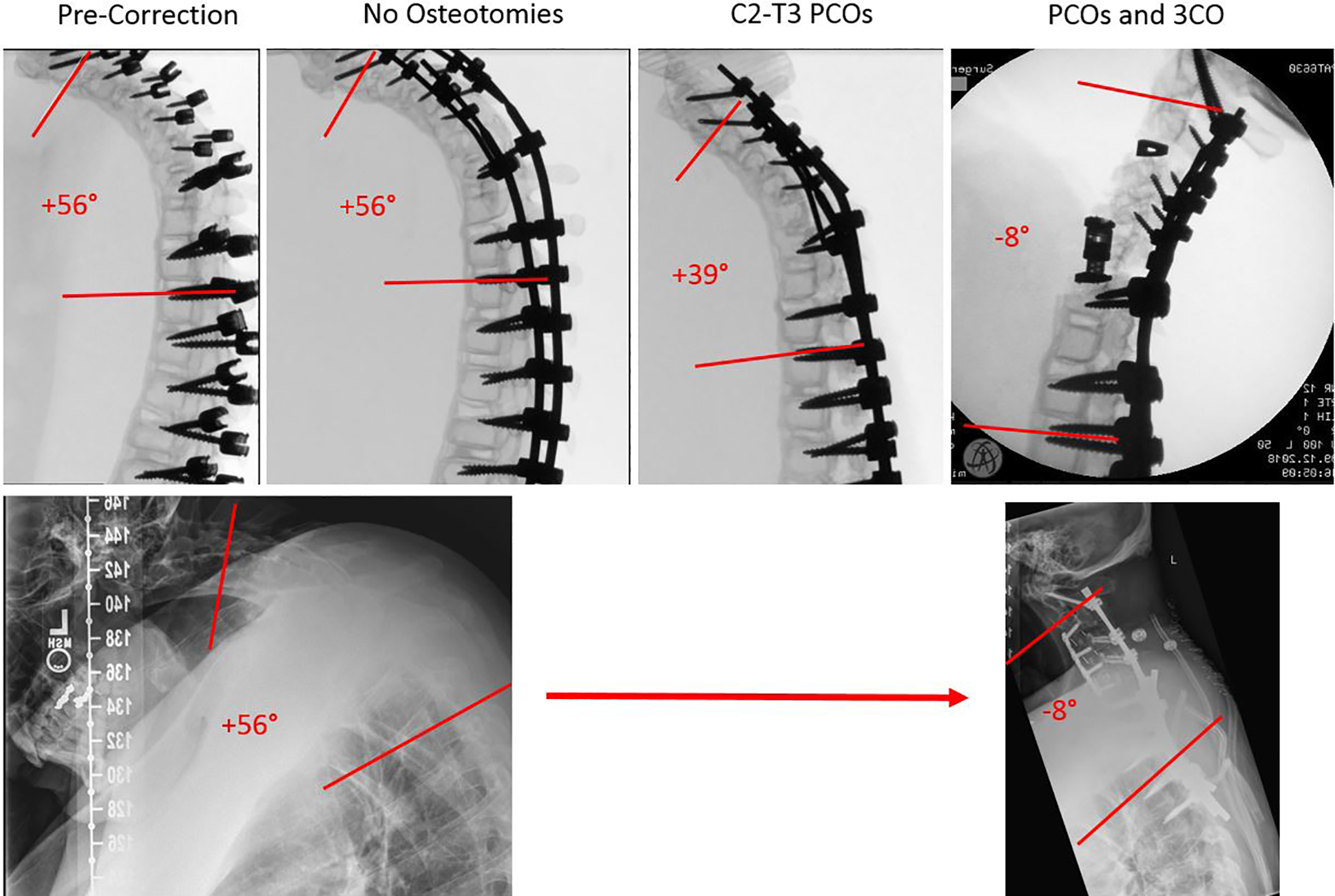
Lateral fluoroscopic views of model 3 and patient 3. Top row from left to right, lateral fluoroscopic views of model 3 in precorrection baseline, correction with no osteotomies, correction with posterior column osteotomies only, and correction with posterior column osteotomies and 3-column osteotomies. Bottom row from left to right, lateral radiographs of patient 3 preoperatively and following surgical correction.
Survey Results
The survey was administered to the 2 attending surgeons and 1 fellow who performed the surgical corrections on the models and actual patients. All 3 surgeons responded to the survey. The respondents were unanimous in their impression that the model had “very high” utility as an educational platform, and they unanimously claimed they were “very likely” to use similar models again for education. Two respondents furthermore felt that model had “very high” utility as a surgical planning tool and they were “very likely” to use it again as such. One respondent gave slightly lower scores of 6 and 5 for utility of the model in surgical planning and likelihood of using the model again for planning, respectively. See Table 3 for complete results of the survey. Two of the 3 respondents provided comments. The first comment was, “An important replacement for a cadaver. This is a model that can actually replicate pathological anatomy and give the learner a much more realistic experience.” The second comment, “Time limitation of performing ‘model surgery’ makes clinical implementation a bit more difficult. Ability to view the model in 3-D versus on screen is invaluable, helps to understand flexible/ rigid segments and adjust surgical plan.”
Survey Responses.a
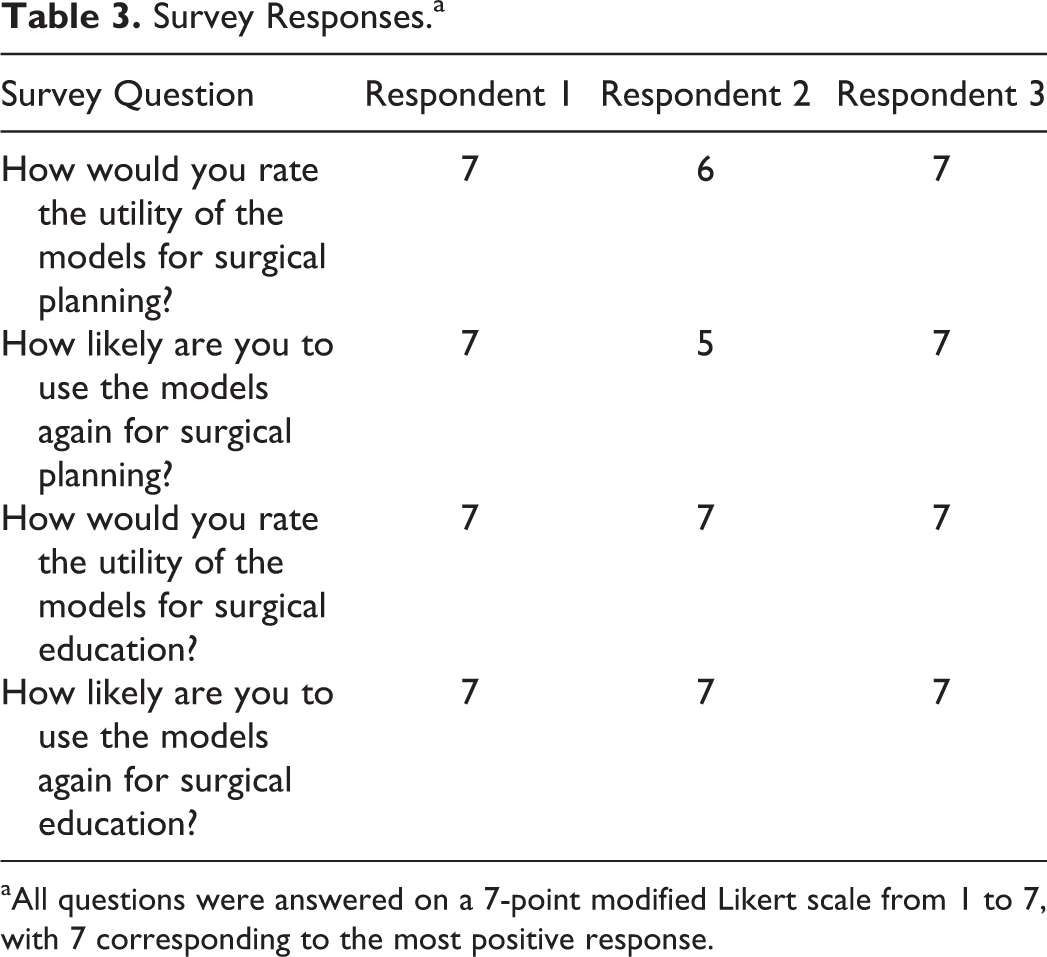
aAll questions were answered on a 7-point modified Likert scale from 1 to 7, with 7 corresponding to the most positive response.
Discussion
Improvements in 3D printing and other additive manufacturing technologies have resulted in an increased ability to replicate both the gross anatomy and biomechanical properties of the human spine. 13,14,16,17 Three-dimensionally printed spine models are becoming increasingly common in complex spine deformity cases, and numerous industry partners are currently offering sterilized models to physicians for use as intraoperative anatomical references. The new models evaluated in this study provide not only high-fidelity replications of the patient’s anatomical properties but also mimic the biomechanical properties of the spine, and therefore have tremendous potential utility in surgical planning, education, and research. This is the first study, however, to evaluate both the perceived utility of these models for use as surgical planning and education platforms as well as the surgical performance of these models when placed under the stress of a surgical deformity correction.
As can be seen in Table 2, each model demonstrated very different responses to attempted correction without osteotomies, with PCOs, and with PCOs and a 3CO. The differences in response to each of these surgical correction techniques is fitting with what one might expect given the relative rigidity and location of fused segments in each model. For example, Model 1 had open disc spaces and open facets at each spine segment (like the patient), and consequently demonstrated gradual correction of the kyphotic deformity with increasing number and size of osteotomies. Model 2, on the other hand, had large osteophytic bridges, collapsed disc spaces, and several auto-fused disc spaces. This model achieved minimal correction with posterior column osteotomies, likely secondary to the robust bony fusion along the anterior column of the spine. It was only when anterior column osteotomies and vertebral column resection was performed that this model was able to be corrected to a lordotic cervical curvature. Patient 3 similarly had a rigid deformity, but unlike patient 2, this patient had normal disc height throughout the cervical and upper thoracic spine (Figure 3). Model 3 demonstrated essentially no change in cervical kyphosis when a correction was attempted without osteotomies. This was exactly what would be expected given the extensive fusing of facet joints throughout the cervical and upper thoracic spine. Interestingly, model 3 achieved 16° of lordosis with PCOs only, despite the extensive fusing of the anterior column. In contrast to model 2, which did not achieve significant correction with PCOs, model 3 likely achieved better correction with PCOs due to the increased height of the intervertebral disc spaces and the lack of posterior longitudinal ligament ossification. Several reports have, in fact, correlated disc space height to achievable lordotic correction following PCOs in both cadaver models and biomimetic spine models. 13,15
It is also interesting to note the differences in cervical lordosis achieved in the models versus the patients. Patient 1, for example, achieved a final lordosis that was 12° less than what was achieved in the model. This difference in final correction is probably best explained by the difference in number and extent of PCOs performed in the model versus the patient. In the model, one may have the tendency to perform more aggressive osteotomies than in real patients. Furthermore, we performed complete PCOs at all the cervical levels in the model, and only select cervical levels in the patient given concerns about operative length and blood loss. Finally, we compressed all the screws in model 1 just to the point of screw failure, whereas in the patient screws were protected from overly aggressive compressive or distractive forces to prevent screw failure in the postoperative period. Together, these differences between the model and patient reflect a major drawback of using the models, namely the tendency to be more aggressive with osteotomies and correction maneuvers than one would be in the actual patient. Patient 3 also had interesting differences in the correction achieved compared with model 3. Patient 3 had a cervical lordosis of +18°, whereas the model had a cervical lordosis of +0.5°. Despite this difference, both the patient and the model ended with very similar C2-T3 angles (−8.0° vs −7.7°). Patient 3 underwent C3-C6 anterior cervical discectomies and a T2 PSO, whereas the model underwent C3-C4 ACDF and a C6 anterior corpectomy. Given that the model underwent a 3CO at a higher spinal level than the patient (C6 vs T2), this explains the much greater cervical lordosis seen in the model compared to the patient. Interestingly, the patient achieved nearly the same final C2-T3 angle, likely because the patient underwent a T2 PSO to make up for the more positive cervical lordosis. Additionally, the more distal PSO level in the patient would allow for greater correction of C2-T3 angle with a smaller focal correction at the PSO level. This case also demonstrates the models potential utility in comparing different surgical strategies for deformity correction.
Altogether, these results suggests the models may have utility as predictors of achievable correction in living patients, as they produce a deformity correction that appears accurate given what we believe to be true regarding the use of various osteotomies in mobile, rigid, and fixed deformities at more proximal or distal levels of the spine. All 3 models furthermore achieved a final correction that was very near, though slightly greater than, each corresponding patient’s correction. The greater correction in the models than in the patients can likely be attributed to a greater number of PCOs, and potentially more complete osteotomies, in the models than in the patients. If the goal of the study were to measure the accuracy of the model in predicting the correction achieved on each patient, the percent error calculated for each model would be 23.5%, 0.5%, and 5.2%, respectively. Furthermore, model 3 was operated on before patient 3, and the experience gained during work on the model lead to a change in the surgical plan, specifically with regard to the use of a T2 pedicle subtraction osteotomy before performing an anterior approach. Collectively, these results that suggest potential utility of these models as surgical planning tools, but further studies are needed to better evaluate model ability to prospectively predict surgical corrections.
The survey results further corroborate the conclusion that these models have potential utility in surgical planning and education. Although the survey was only administered and taken by 3 authors, there was consensus on the high potential utility of the models. There was concern by 1 respondent that the model held less utility as a surgical planning tool, primarily because of the “time limitation of performing surgery on models.”
Study Limitations
This study is the first analysis of the utility of a novel synthetic spine model of CSD, and as such it comes with several limitations. The survey was administered to only 3 people, each of them an author on this paper and therefore potentially biased. The spine models were also operated on by a fellow under the direction of his attending surgeons. It is possible that if the attending surgeons or a different trainee were to complete the 3 phases of model correction, the results would be different. We attempted to account for this potential source of error by standardizing the criteria for achieving maximal correction of the spine during each phase of correction. In each phase, attempts at further correction were halted either when screws began to pull out of the bone with additional correction, or when it became clear that no additional lordotic correction was achieved with increasing force applied to the screws. The use of a fellow for the correction of these spine models should also be considered a strength of the study, however, as it demonstrates how a trainee can be given the opportunity to independently perform model procedures either before or after an actual procedure, both of which have tremendous educational value.
Models 1 and 2 were corrected after the procedure was performed on the respectively modeled patients. The reason for performing the model corrections after the actual case had to do with the logistics of getting the models manufactured and reserving a vacant operating room and equipment. Ideally the models would have all been corrected prior to the patients’ procedures, thereby eliminating the potential for bias in performing the model correction. It is certainly possible that the corrections of models 1 and 2 were biased by the experience of operating on the actual patient. We tried to minimize this potential bias by adhering to a strict set of rules regarding the types of osteotomies and corrective forces applied to the spine models. Although the models still provided educational value to the fellow performing the model corrections after the surgical procedure, this likely represents a lost opportunity to rehearse a surgical procedure prospectively and therefore provide both a better assessment of the models’ ability to predict intraoperative corrections and a better educational experience for the fellow during the actual procedure. Future studies evaluating both the educational and surgical planning utility of these types of models should adhere to a rule of correcting models preoperatively.
Although this preliminary data suggests potential utility of these models as surgical planning tools, further data is needed to corroborate and expand on these findings. The potential increase in cost and time that would be associated with model correction prior to a case must also be considered, especially considering the wide availability of software programs that aid in surgical planning. The major disadvantage of these software programs is that they are entirely reliant on surgeon estimates of the correction that will be achieved at any given spinal level following certain surgical maneuvers. There is tremendous potential for bias and error in these estimates. A model with demonstrated biofidelity to the patient would eliminate this error and provide both an opportunity for case rehearsal and a more accurate prediction of the correction that could be achieved with certain surgical maneuvers.
This is a small case series. Severe cases of CSD leading to dropped-head syndrome are rare, with most busy spinal deformity practices only operating on a few per year. Although the small size of this case series is a weakness, it also serves as a call to other centers who see these patients to begin collaborating via the use of biomimetic spine models. This way we can begin evaluating the numerous surgical strategies that have been described by using models of identical anatomy and biomechanical performance and comparing the results obtained with different surgical strategies.
Finally, during the peer-review process a patent filing describing this new technology was licensed to a new company, thereby creating a potential conflict of interest that did not exist at the time of data collection, data analysis, or manuscript drafting and submission. The patent is owned by the hospital where this work was conducted, and it lists the first author (MAB) as the inventor. Because this potential conflict arose after data collection and manuscript drafting, we do not believe that it had any effect on our data collection, analysis, or reporting of results.
Conclusions
The synthetic spine model evaluated in this study appears to accurately replicate both the gross anatomical appearance and biomechanical performance of patient-specific spines. This high fidelity to the individual patient’s anatomy, bone quality, and segmental mobility result in a custom model that provides a valuable learning platform for resident and fellow education and might have utility as surgical planning tool. Future research should focus on continued validation of the model as a biomechanical research, surgical planning, and surgical education platform.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author MAB is the inventor on a patent for a spine modeling technology relevant to this article. The patent application is owned by the sponsoring hospital system and is pending review by the US Patent and Trademark Office. The pending patent was licensed to a new company during the peer-review process for this manuscript. Authors MAB, SM, UK, J-CL, and RS have financial interests in this new company.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.