
Abstract
Study Design:
Case series/systematic review.
Objectives:
To report on patients undergoing posterior cervical fusion for symptomatic pseudarthrosis following anterior cervical discectomy and fusion (ACDF), and to assess outcomes reporting in the literature.
Methods:
Patients undergoing posterior instrumented fusion for pseudarthrosis after primary ACDF from 2013 to 2018 by a single surgeon were reviewed consecutively. Neck Disability Index (NDI) and visual analogue scale (VAS) arm/neck were recorded at preoperative, 6-month, and 1-year time points. A systematic review of the literature was performed, and outcomes reporting was recorded.
Results:
NDI scores were 54.4 (SD 19.1), 36.6 (SD 18.1), and 41.2 (SD 19.2) at preoperative, 6-month, and 1-year time points, respectively, with improvement from preoperatively to 6 months (P = .004). VAS neck scores were 8.1 (SD 1.3), 5.0 (SD 2.9), and 5.8 (SD 2.2) at preoperative, 6-month, and 1-year time points, respectively, with improvement from preoperatively to 6 months (P = .038). VAS arm scores were 5.1 (SD 4.1), 3.5 (SD 3.2), and 3.6 (SD 2.7) at preoperative, 6-month, and 1-year time points, respectively, with improvement although these did not reach statistical significance (P = .145). The most common subjective outcomes reported in the literature were general symptoms assessments (43%), ordinal scales (43%), and VAS neck (19%) scales, with the majority of studies (67%) documenting one measure.
Conclusions:
Patient-reported outcomes demonstrate clinically meaningful improvement within the first 6 months after posterior fusion for pseudarthrosis. Studies demonstrate substantial variability and no standardization in outcomes reporting, limiting the ability to compare results across interventions and pathologies. Standardized reporting will enable comparisons to inform patients and physicians on the optimal approach to treat this difficult problem.
Keywords
Introduction
One of the most common spinal procedures, anterior cervical discectomy and fusion (ACDF) accounts for approximately 80% of cervical surgeries. 1 While its success in improving pain, quality of life, and disability scores has been well documented, 2 -6 one complication that remains a significant challenge is pseudarthrosis, which has been shown to occur at a rate of up to 20% in single level cases and at even higher rates in multilevel surgery. 7 -11 A failure of postoperative fusion, pseudarthrosis should be suspected based on a clinical history of persistent neck pain or radicular symptoms. 3,12 -16 Radiographically, signs of pseudarthrosis include lack of bridging trabeculae between the endplates, graft resorption, and/or motion exceeding 1 to 2 mm between spinous processes on flexion-extension radiographs. 17,18 This phenomenon is clinically relevant, as pseudarthrosis has been shown to compromise improvements in neck pain and Neck Disability Index (NDI) scores, 19 and is one of the most common indications for additional intervention after ACDF, implicated in up to 56% of revision cases. 17,20,21
Multiple strategies have been employed to treat symptomatic pseudarthrosis, including anterior, posterior, or circumferential approaches, and attempts have been made to identify those at highest risk before surgery. 22 There has been some debate in the literature regarding which of these treatments is most effective, 11,23 yet there is a paucity of data to support any given approach, as the majority of studies available do not report standardized outcomes and often lack the power necessary to draw generalizable conclusions about the superiority of one approach over another.
The objective of this study is to report on a consecutive series of single-surgeon patients who underwent posterior cervical fusion for symptomatic pseudarthrosis following ACDF. Additionally, we provide a systematic review of the currently available literature regarding management of these cases to report on the data and to assess the variability in outcomes reporting following revision for pseudarthrosis after ACDF.
Materials and Methods
Data Collection
Institutional review board approval was obtained prior to initiation of the study (ID, 2018-1580). Fourteen consecutive patients undergoing revision surgery for symptomatic pseudarthrosis from 2013 to 2018 by a single surgeon were reviewed. Exclusion criteria included patients who did not undergo revision surgery or those undergoing revision without pseudarthrosis. All 14 patients had previously undergone attempted cervical fusion and underwent revision surgery for pseudarthrosis via posterior instrumented fusion. The majority (n = 11) of patients had their index operations performed at outside facilities. Patients were indicated for surgery based on findings of radiographic and clinical pseudarthrosis, using criteria by Song et al 24 whereby fusion was defined as <1-mm motion between flexion/extension radiographs as well as computed tomography. 24 Demographic characteristics and surgical details were obtained and recorded. Patients underwent a posterior approach to the cervical spine via a midline approach to expose the levels of interest. 3.5 mm and/or 4.0 mm lateral mass screws and 3.5 mm and/or 4.0 mm titanium or cobalt-chromium rods were placed and the fusion bed was prepared using a high-speed burr, decorticating the facet joints. Morselized local autograft in all cases, and biologic augmentation (recombinant human bone morphogenetic protein–2 [INFUSE Bone Graft, Medtronic Spinal and Biologics, Memphis, TN], demineralized bone matrix [Grafton, Medtronic Spinal and Biologics, Memphis, TN], and/or allograft) was used to enhance the fusion bed. Selection of fusion levels was based on the levels of pseudarthrosis as well as any additional sites of pathology at the time of revision, based on history, physical exam, imaging, and intraoperative findings. Vancomycin powder (1 g) was placed in the wound prior to layered closure. All patients were placed into a brace postoperatively. One patient with failed prior posterior fusion underwent removal of hardware at the pseudarthrosis levels with wire fixation and anterior fusion. Patient-reported outcomes including NDI and visual analogue scale (VAS) Neck and Arm pain were collected preoperatively, and at 6 months and 1 year postoperatively. All patients were assessed for fusion based on the aforementioned criteria on dynamic radiographs at 6 months and 1 year postoperatively.
Systematic Review
A systematic review of the available literature was performed, adhering to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 25 The search was performed in the Medline, PubMed, Embase, and Cochrane Library databases, using Medical Subject Headings and keyword search terms and their respective combinations, including “pseudarthrosis,” “anterior cervical discectomy,” and “treatment outcome” (full search is given in the appendix). The final search was performed on October 23, 2018.
Selection Criteria
Clinical studies were evaluated and included if they were in English and reported patient outcomes after revision for pseudarthrosis following ACDF. Nonclinical studies, literature reviews, expert opinions, case reports, conference abstracts, and those not reporting on outcomes were excluded. Studies were reviewed by 2 of the study authors (M.E.S. and P.J.Y.), who performed title and abstract reviews separately. The full texts of articles meeting inclusion criteria based on title and abstract were then reviewed for final inclusion in the study, with authors coming to a consensus in the case of disagreement. A total of 21 studies were included in the systematic review, with selection process summarized in Figure 1.
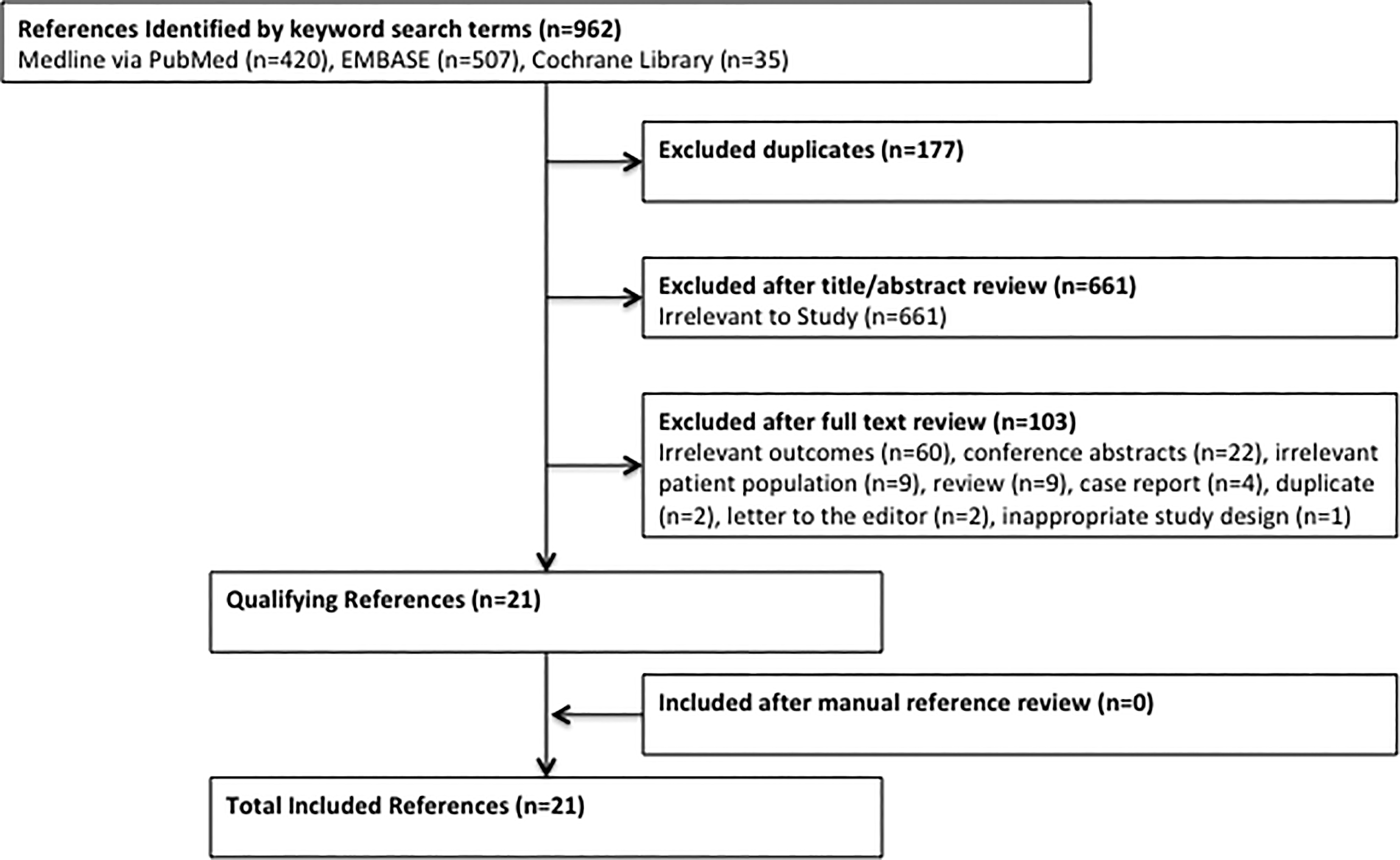
Flow diagram of systematic review: A total of 21 studies were included.
Quality Evaluation
Included studies were evaluated using the MINORS (Methodological Index for Nonrandomized Studies) checklist. 26 Studies were evaluated on 8 to 12 items, with each scored as 0 (not reported), 1 (reported but poorly or inadequately done), or 2 (reported, well done and adequate), with a maximum score of 16 and 24 for noncomparative and comparative studies, respectively. Articles were each scored by 2 of the study authors (M.E.S. and P.J.Y.) with the authors coming to consensus in the case of disagreement.
Statistical Analysis
Descriptive statistics of the study cohort were summarized as mean (±SD) for normally distributed continuous variables, median (interquartile range [IQR]) for nonnormally distributed continuous variables and count (frequency) for categorical variables. All analyses were conducted using Stata SE 14.0 (Stata Corp, College Station, TX).
Results
A total of 14 patients were included in the study (Table 1). Mean age at revision surgery was 53.6 years (range 40-68 years) with mean follow-up of 12.3 months (range 6.0-22.9 months). The mean time between index and revision surgery was 86.8 months (range 23.5-323.8 months). Four (29%) patients had pseudarthrosis at a single level, while 10 (71%) had pseudarthrosis at 2 levels. Revision surgery involved 2, 3, and 4 levels in 7 (50%), 6 (43%), and 1 (7%) patients, respectively. Mean intraoperative blood loss (n = 10) was 130 mL (range 50-200 mL) and mean procedure duration was 131 minutes (range 55-280 minutes). Of note, 3 additional cases had “minimal” blood loss and were not included in the calculation. The mean length of stay was 2.9 days (range 2-5 days). Thirteen patients demonstrated radiographic fusion at 6 months postoperatively. One patient did not follow-up at 6 months but presented at 8 months postoperatively with evidence of fusion on computed tomography scan. Individual patient characteristics are shown in Table 2. Patients presented with axial neck pain, while a subset also had radicular symptoms and headaches. Recombinant human bone morphogenetic protein-2 (rhBMP-2) was used in 10 (71%) of the revisions to enhance the fusion, whereas 7 (50%) had demineralized bone matrix (DBM) and 6 (43%) had allograft. Morselized local autograft was used in all cases.
Demographics and Operative Details.
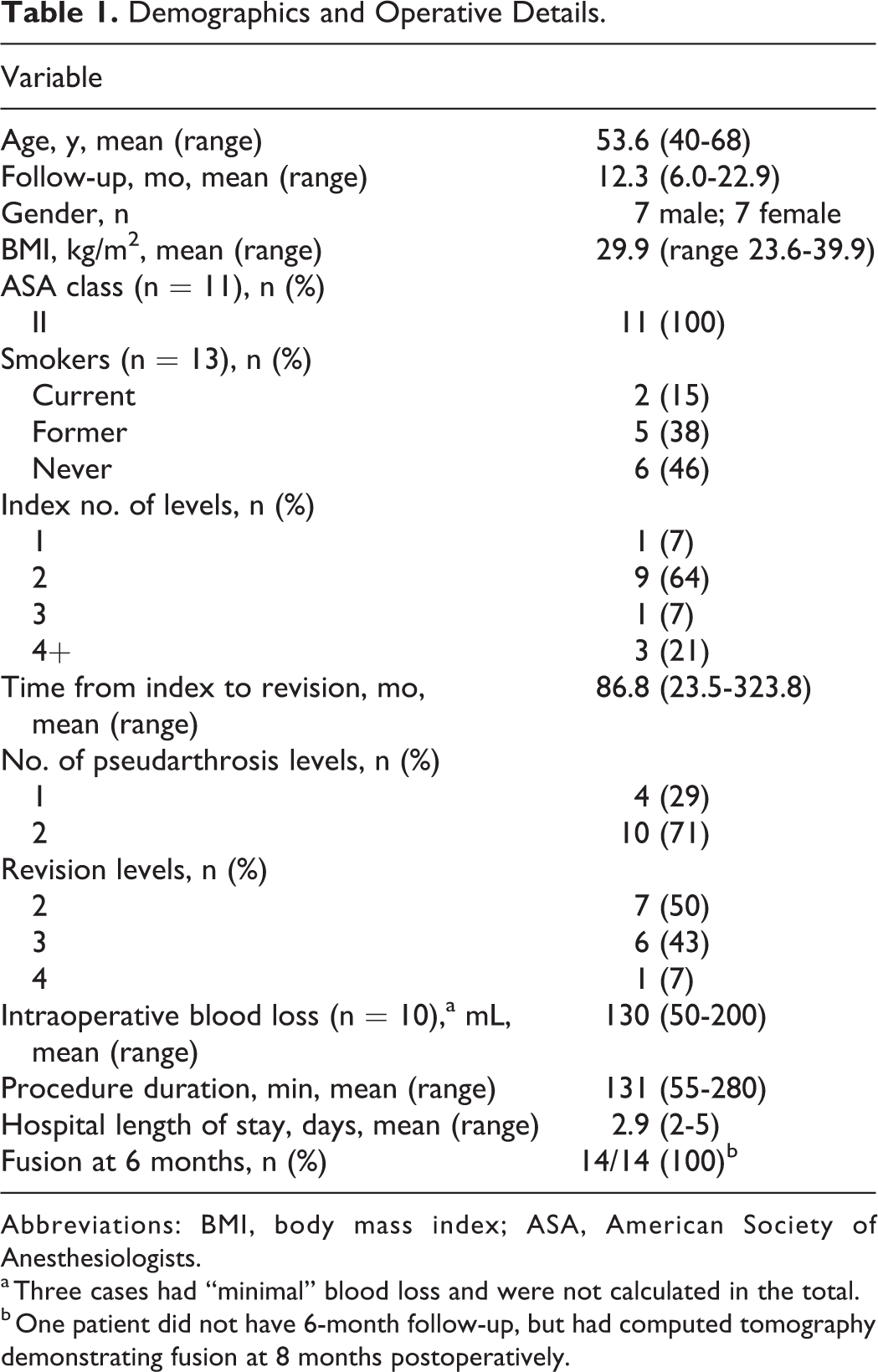
Abbreviations: BMI, body mass index; ASA, American Society of Anesthesiologists.
a Three cases had “minimal” blood loss and were not calculated in the total.
b One patient did not have 6-month follow-up, but had computed tomography demonstrating fusion at 8 months postoperatively.
Individual Patient Characteristics.
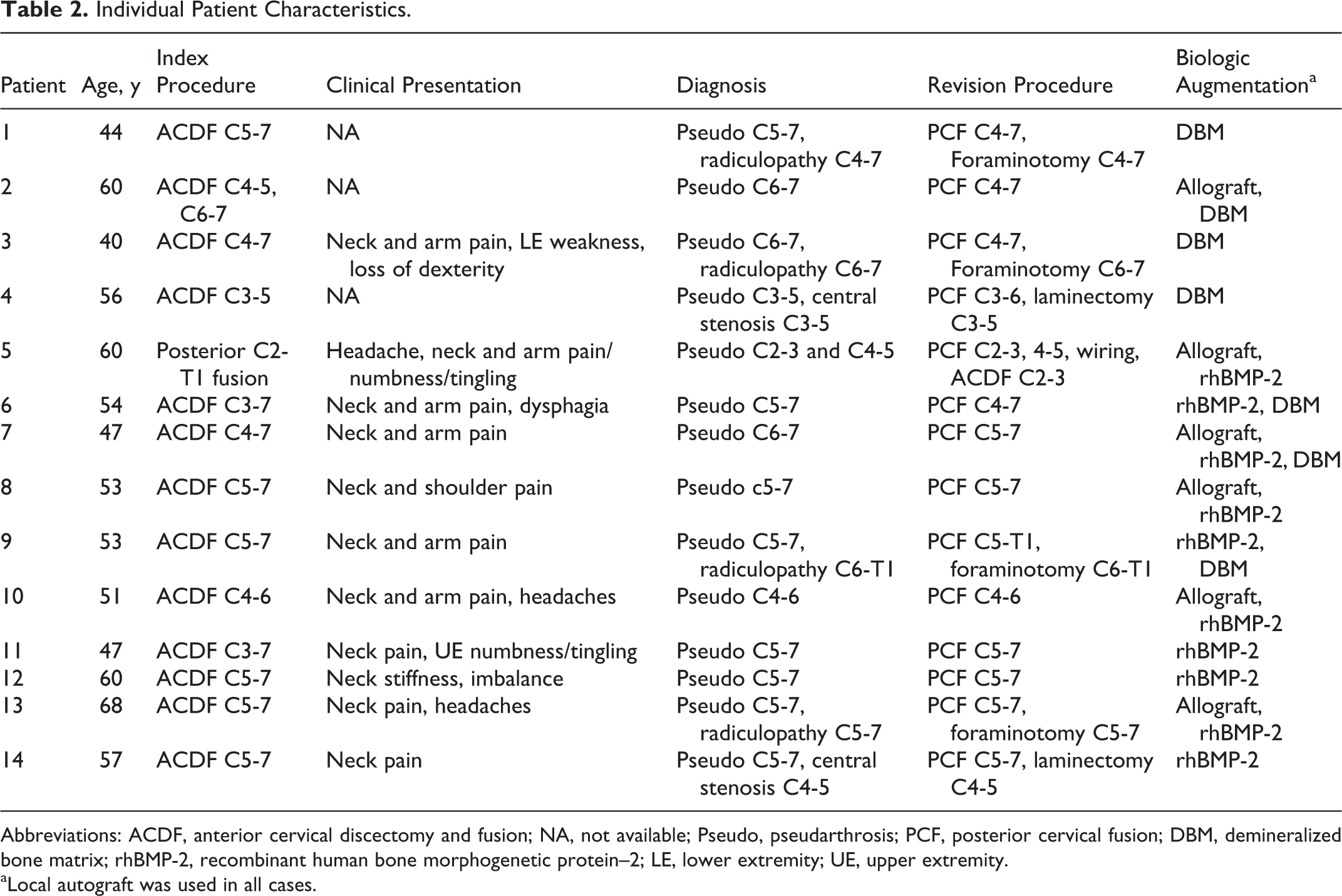
Abbreviations: ACDF, anterior cervical discectomy and fusion; NA, not available; Pseudo, pseudarthrosis; PCF, posterior cervical fusion; DBM, demineralized bone matrix; rhBMP-2, recombinant human bone morphogenetic protein–2; LE, lower extremity; UE, upper extremity.
aLocal autograft was used in all cases.
Patient-reported outcomes are shown in Figures 2, 3, and 4. NDI scores were 54.4 (SD 19.1), 36.6 (SD 18.1), and 41.2 (SD 19.2) at the preoperative, 6-month, and 1-year time points, respectively. There was a significant improvement noted in NDI from preoperatively to 6 months postoperatively (P = .004). VAS neck scores were 8.1 (SD 1.3), 5.0 (SD 2.9), and 5.8 (SD 2.2) at the preoperative, 6-month, and 1-year time points, respectively. There was significant improvement noted from preoperatively to 6 months postoperatively (P = .038). While mean VAS Arm pain scores improved over time, these results were not statistically significant (P = .145 from preoperative to 6 months).
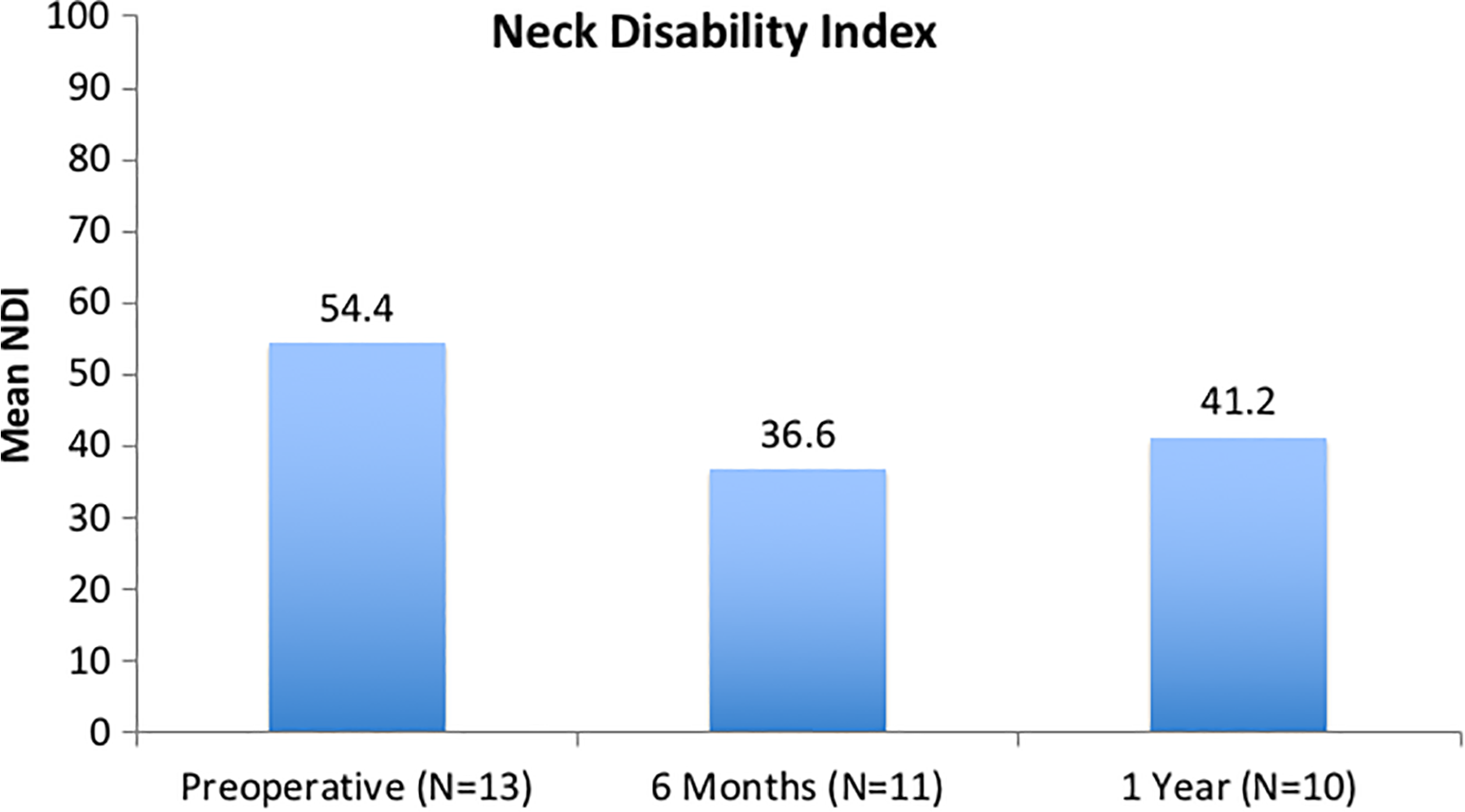
Neck Disability Index (NDI): There was a significant, clinically important improvement noted from preoperatively to 6 months postoperatively (P = .004).
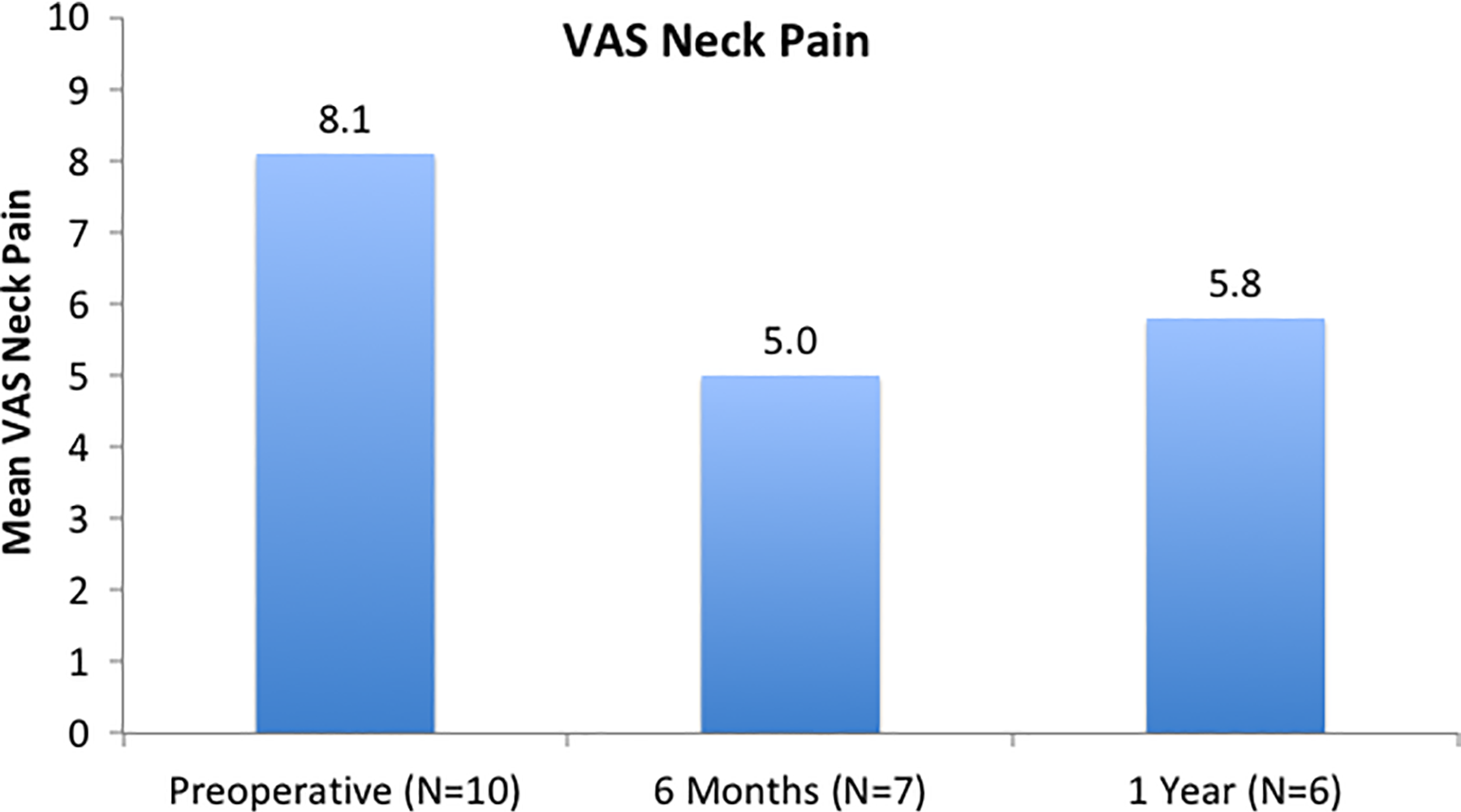
Visual analogue scale (VAS) Neck: There was a significant, clinically important improvement noted from preoperatively to 6 months postoperatively (P = .038).
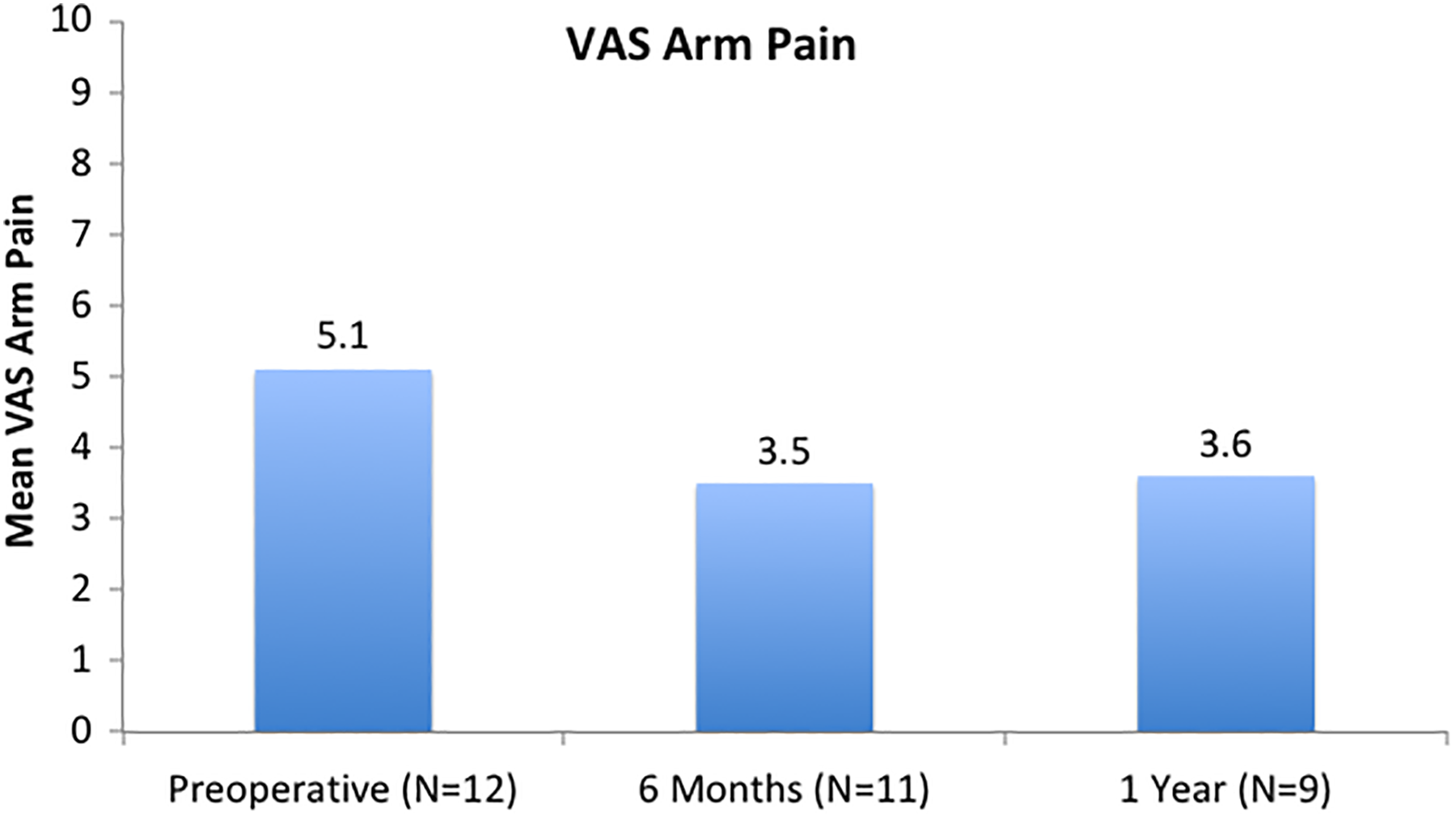
Visual analogue scale (VAS) Arm: While mean VAS arm pain scores improved over time, these results were not statistically significant (P = .145).
Systematic Review
Twenty-one studies, published between 1990 and 2017, were included in the systematic review (Table 3). 10,13,23,27 -44 The majority of studies were retrospective (n = 19) with level IV evidence (n = 16). Of the 21 studies, 19 were specifically assessing the outcomes after revision for pseudarthrosis, whereas in 2 studies this data was reported as a subgroup of the overall population. A total of 530 patients were included in the review. The mean number of patients in each study was 25.2 (range 3-120) with a frequency-weighted mean age of 48.3 years (n = 16 studies; range 18-79 years) and follow-up of 39.6 months (n = 17 studies; range 2-216 months). The frequency-weighted mean number of revision levels was 1.43 (n = 12 studies; range 1-4 levels) with a mean interval from index to revision procedure of 23.5 months (n = 17 studies; range 2-230 months). The posterior approach was most commonly used (n = 18 studies), followed by anterior (n = 9 studies), and circumferential (n = 2 studies) approaches. Five studies 13,23,40 -42 reported on subgroups undergoing anterior and posterior revision; one study 27 noted subgroups undergoing posterior and circumferential fusion; and another study 39 reported on subgroups undergoing anterior, posterior, and circumferential fusion. On quality evaluation, 16 noncomparative studies were found to have a mean MINORS score of 8.9 (range 5-12) of 16, and 5 comparative studies had a mean MINORS score of 9.2 (range 6-13) of 24.
Details on Included Studies.
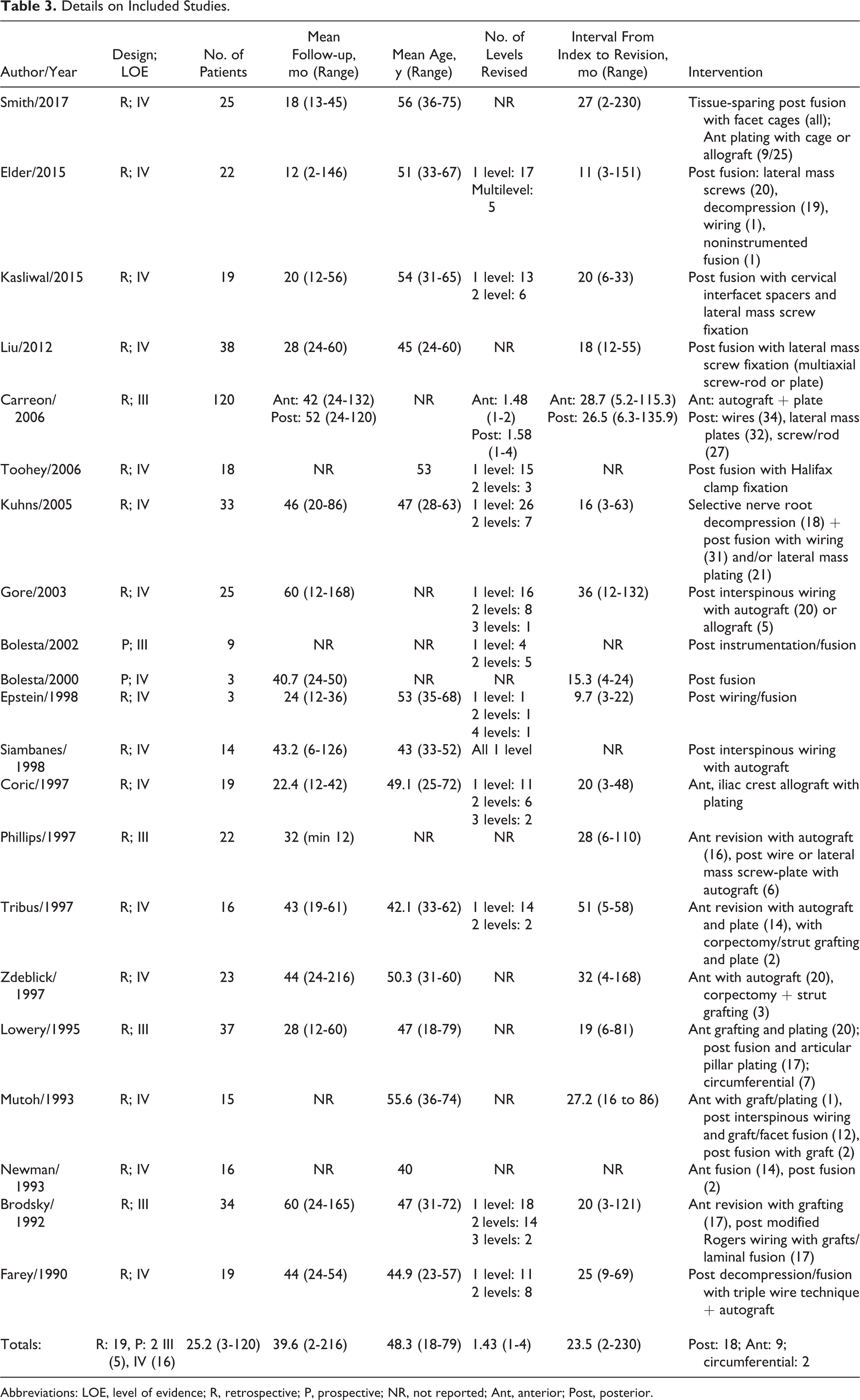
Abbreviations: LOE, level of evidence; R, retrospective; P, prospective; NR, not reported; Ant, anterior; Post, posterior.
Outcomes Reporting
Outcomes following revision for pseudarthrosis are shown in Table 4. Objective outcomes were reported sparsely in the reviewed studies. Length of hospital stay was most frequently reported, noted in 24% (n = 5) of studies, whereas estimated blood loss and duration of operation were reported by 19% (n = 4) and 14% (n = 3) of studies, respectively. Each study was assessed for inclusion of patient-reported outcomes with respect to frequency of reporting. The 10 most commonly cited outcomes are shown in Figure 5a. The most common subjective outcomes reported were general symptoms assessments (n = 9 studies) and ordinal scales (n = 9 studies), frequently with Odom’s criteria. 45 The next most commonly noted subjective instruments were VAS Neck and Arm pain, reported in 4 (19%) and 3 (14%) studies, respectively. The majority of subjective outcomes were noted in one study each. The number of subjective outcomes reported per study is depicted in Figure 5b. The majority of studies (67%) document one subjective outcome measure. One study 10 was found to report 5 subjective measures, whereas one study 23 supplied none.
Outcomes of Included Studies.
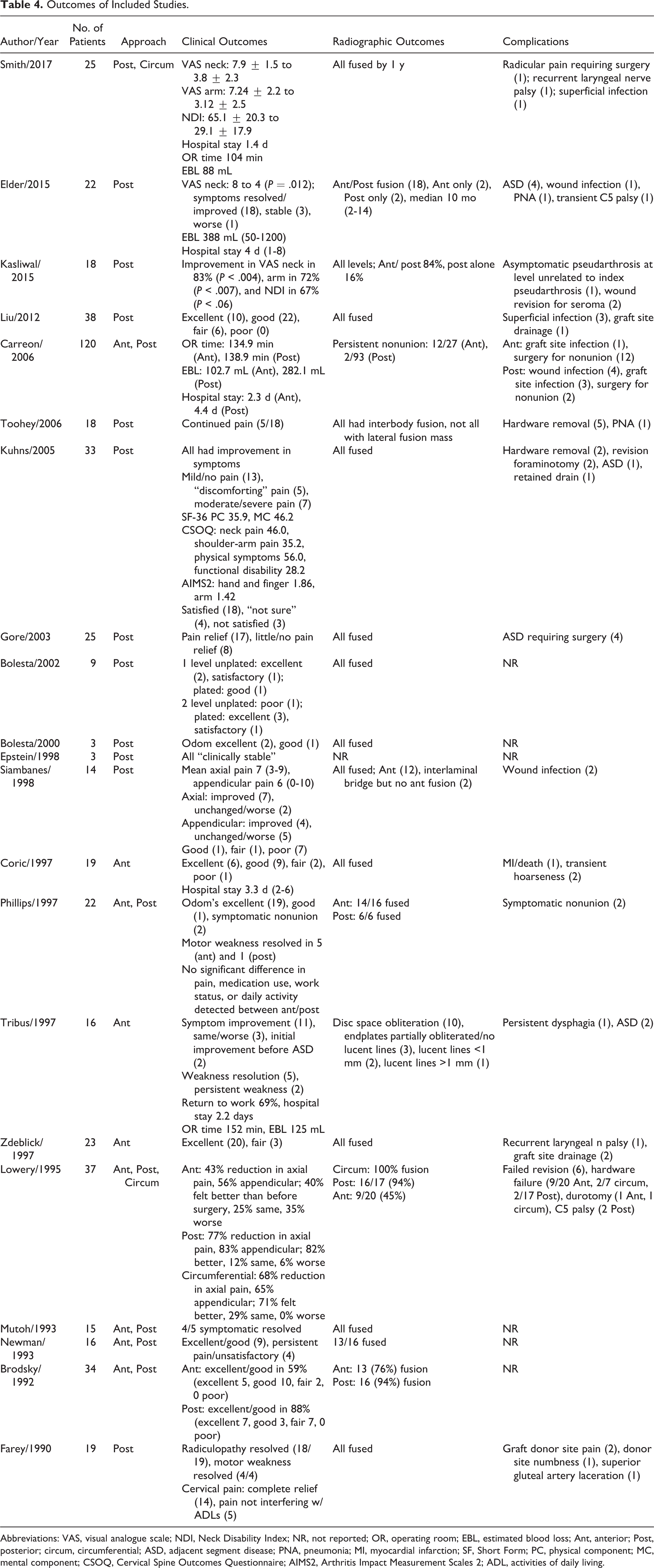
Abbreviations: VAS, visual analogue scale; NDI, Neck Disability Index; NR, not reported; OR, operating room; EBL, estimated blood loss; Ant, anterior; Post, posterior; circum, circumferential; ASD, adjacent segment disease; PNA, pneumonia; MI, myocardial infarction; SF, Short Form; PC, physical component; MC, mental component; CSOQ, Cervical Spine Outcomes Questionnaire; AIMS2, Arthritis Impact Measurement Scales 2; ADL, activities of daily living.
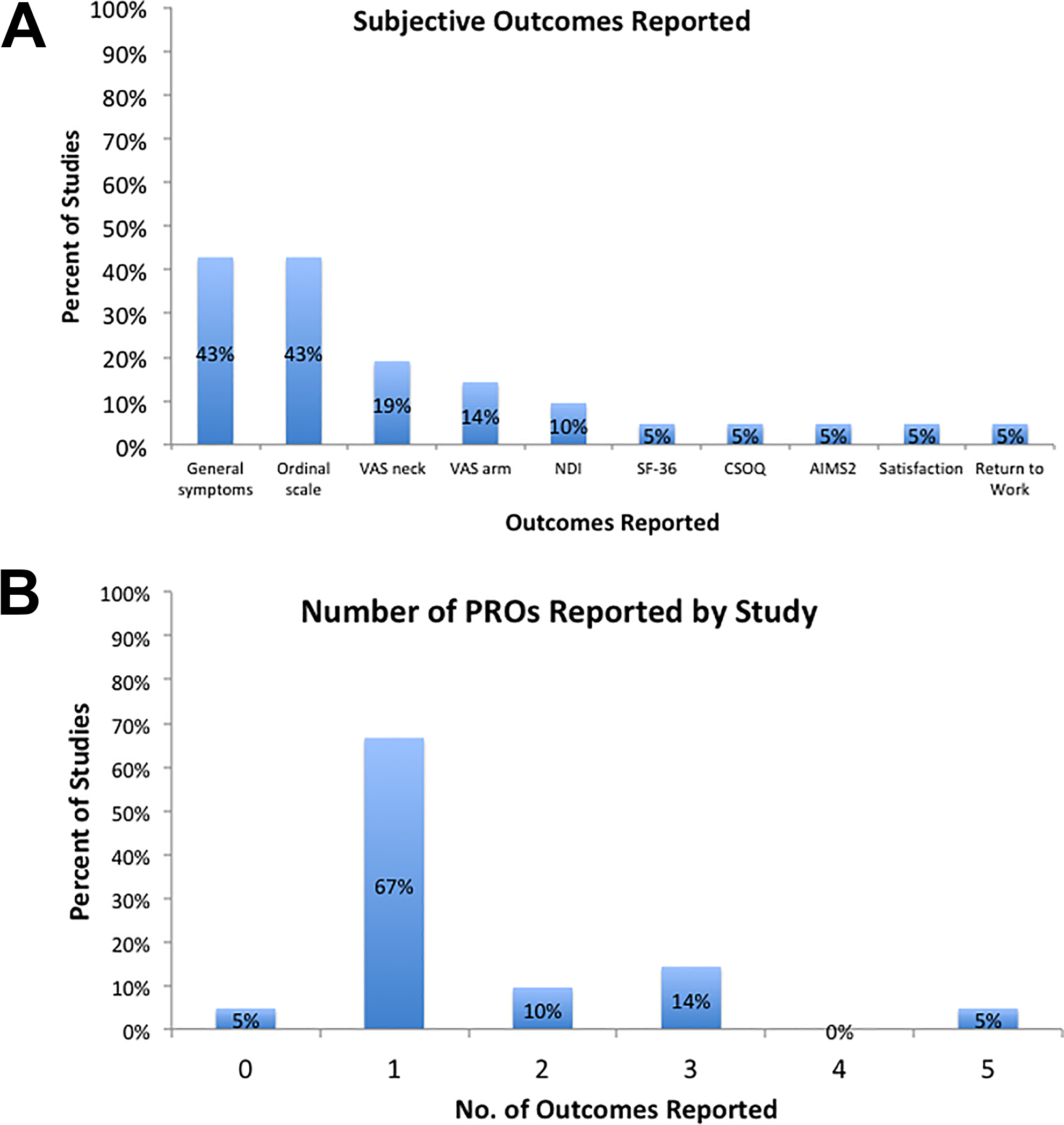
(A) Subjective outcomes reported: The most common subjective outcomes reported were general symptoms assessments and ordinal scales (each in 43%), followed by VAS neck (19%), VAS arm (14%), and NDI (10%) scales. Other outcomes were found in 1 study each. VAS, visual analog scale; NDI, Neck Disability Index; SF-36, Short Form 36; CSOQ, Cervical Spine Outcomes Questionnaire; AIMS2, Arthritis Impact Measurement Scales 2. (B) Patient-reported outcomes reported by study: The majority of studies (67%) document 1 subjective outcome measure, with 5 studies reporting 2 (n = 2 studies) and 3 (n = 3 studies) outcomes. One study reported 5 subjective measures and one reported none.
Discussion
Based on the results of this study, patients undergoing posterior fusion for symptomatic pseudarthrosis after ACDF can expect to have improvements in NDI and VAS Neck pain at 6 months and 1 year postoperatively. At a mean follow-up of 12.3 months, NDI scores were 54.4 and 36.6 at preoperative and 6-month time points (P = .004), respectively, and VAS Neck scores were 8.1 and 5.0 at preoperative and 6-month time points, respectively (P = .038). These outcomes are statistically significant as well as clinically important, with both exceeding minimally clinically important differences. 46 -49 Furthermore, these outcomes were attained with acceptable perioperative risk, with mean intraoperative blood loss of 130 mL (not including 3 patients with “minimal” blood loss), procedure duration of 131 minutes, and length of stay of 2.9 days. All patients went on to fusion postoperatively based on radiographic criteria.
To our knowledge, this is the first report on clinical outcomes in patients undergoing posterior instrumented fusion with a screw/rod construct alone for pseudarthrosis after ACDF. The results of our cohort are important, suggesting that these patients exhibit clinically meaningful improvements in NDI and neck pain within the first 6 months postoperatively. While many have noted improvements after revision for pseudarthrosis, few studies have reported on validated instruments in cervical pathology. Kuhns et al 10 studied 33 patients undergoing lateral mass plating and/or wiring, reporting postoperative Short Form–36 (SF-36), Cervical Spine Outcomes Questionnaire (CSOQ), and Arthritis Impact Measurement Scales 2 (AIMS2) but no baseline preoperative comparisons to assess change after surgery. Two more recent studies assessed posterior fusion focusing on preparation of the facet joints. Kasliwal et al 44 evaluated posterior fusion using interfacet spacers and lateral mass screws, reporting significant improvements in VAS Neck and Arm pain for 83% and 72% of patients, respectively. 44 They further noted improvement in NDI scores in 67% of patients although this did not reach statistical significance (P < .06). A more recent study by Smith et al 27 assessed tissue-sparing posterior fusion using bilateral facet cages in 25 patients, noting significant improvements in VAS Neck and Arm scores from 7.9 ± 1.5 to 3.8 ± 2.3 and from 7.24 ± 2.2 to 3.12 ± 2.5, respectively, and significant improvements in NDI from 65.1 ± 20.3 to 29.1 ± 17.9 at a mean 18 months postoperatively. These findings are consistent with what was found in our study.
There remains some debate as to whether symptomatic pseudarthrosis after ACDF is best managed with an anterior or posterior approach. In their study of 120 patients with symptomatic pseudarthrosis after ACDF, Carreon et al 23 found similar operative times for anterior (134.9 minutes) and posterior (138.9 minutes) groups, although noted greater estimated blood loss (282.1 vs 102.7 mL) and longer hospital stay (4.4 vs 2.3 days) in those undergoing posterior revision. Similarly, Elder et al 28 note estimated blood loss of 388 mL and mean hospital stay of 4 days in their cohort undergoing posterior revision, whereas in a group of patients undergoing anterior revision, Tribus et al 37 report estimated blood loss of 125 mL and mean hospital stay of 2.2 days. More recent literature has noted a more favorable risk profile for the posterior approach. Smith et al. noted a short length of stay (1.4 days), operative time (104 minutes), and estimated blood loss (88 mL), 27 while in our study we found length of stay of 2.9 days, procedure duration of 131 minutes with 130 mL of blood loss, demonstrating the possibility of achieving a better risk profile than what has been previously reported.
Reviewing the literature, we identified 21 studies, the majority of which included a posterior approach to revise pseudarthrosis after ACDF. Of note, there was substantial heterogeneity in outcomes reporting. The most commonly reported objective variable (length of stay) was noted in 24% of studies, whereas blood loss and operative duration were reported in 19% and 14% of studies, respectively. Similar shortcomings were found in the reporting of patient-reported outcomes. The most commonly noted outcomes were assessments of general symptoms (43%) and ordinal scales (43%), followed by VAS Neck (19%) and VAS Arm (14%) scales. Overall, the quality of the studies was low, with 16 noncomparative studies having a mean MINORS score of 8.9 (range 5-12) of 16, and 5 comparative studies having a mean MINORS score of 9.2 (range 6-13) of 24.
A prior meta-analysis assessed clinical and fusion outcomes to evaluate the optimal approach for revision in the setting of pseudarthrosis after ACDF. 11 Sixteen studies were included in the meta-analysis, with 10 of the studies each reporting on the results after anterior and posterior revision. The authors found a significant difference in fusion success, noting 86.4% success for anterior and 97.1% for the posterior approach (P = .028), but found no difference in terms of clinical outcomes. Nevertheless, the authors note significant heterogeneity and poor overall quality of studies as key factors limiting the accuracy of their conclusions.
Given the overall low prevalence of this condition, it is unlikely that a randomized trial or even a well-powered cohort study would be feasible. Rather, comparing different strategies to treat symptomatic pseudarthrosis may lie in our ability to amalgamate the outcomes of contemporary case series such as this one. However, this systematic review highlights the imposing limitation of this strategy—inadequate use of standardized outcome instruments. The most common patient-reported outcomes noted are general symptoms assessments and ordinal scales—not validated instruments in cervical spine disease—and many of the studies do not distinguish between neck and arm pain, which could represent different underlying pathologies. 11 This lack of standardized outcome measures make results difficult to interpret and compare across interventions.
Our study has several limitations. This series contains a small number of patients treated by a single surgeon without long-term follow-up, limiting the study’s power and ability to draw conclusions about the generalizability and long-term outcomes associated with posterior fusion. In this vein and given the number of patients, a power analysis was not performed and all consecutive patients meeting the inclusion criteria were included in the study. Similarly, as patients underwent revision with a posterior approach and only one with an anterior approach, we are unable to compare across different treatment strategies (anterior vs posterior vs combined). Regarding the systematic review, our inclusion of studies relied on our previously described search strategy and the inclusion of works in the aforementioned databases. To limit the possibility of excluding studies, we used broad search terms as well as multiple databases. Additionally, the results of our study were dependent on data reported in the included studies and were therefore limited by the clarity of reporting in the primary works. Finally, analysis of outcomes reporting is limited by the small number of studies. Yet this is reflective of the current literature on revision for symptomatic pseudarthrosis after ACDF, and this shortcoming is an important reality to highlight as we consider future research in this field.
In conclusion, patient-reported outcomes improve after posterior fusion in the setting of pseudarthrosis after ACDF. These gains are made in the first 6 months postoperatively with an acceptable perioperative risk profile. The current literature for this condition contains substantial variability of outcomes reporting, with few studies documenting validated instruments, limiting our ability to compare results across studies. Randomized trials comparing surgical approaches for symptomatic pseudarthrosis would prove useful but are likely not feasible. In the future, broader adoption of standardized patient-reported outcomes will enable more accurate comparison across studies, informing patients and surgeons about the optimal approach to treat this difficult problem.
Supplemental Material
Supplemental Material, Appendix_-_Search_Strategy - Outcomes of Revision Surgery for Pseudarthrosis After Anterior Cervical Fusion: Case Series and Systematic Review
Supplemental Material, Appendix_-_Search_Strategy for Outcomes of Revision Surgery for Pseudarthrosis After Anterior Cervical Fusion: Case Series and Systematic Review by Michael E. Steinhaus, Philip J. York, Rachel S. Bronheim, Jingyan Yang, Francis Lovecchio and Han Jo Kim in Global Spine Journal
Footnotes
Authors’ Note
Investigation performed at the Department of Orthopaedic Surgery, Hospital for Special Surgery, New York, NY.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.