
Abstract
Study Design:
Prospective matched cohort study
Objective:
To evaluate the sensitivity and specificity of Gene Xpert in the diagnosis of spinal tuberculosis.
Methods:
From January 2016 to August 2018, Gene Xpert results were prospectively studied in 68 patients of clinicoradiologically suspected spinal tuberculosis (STB) and a control group (CG) of 92 patients, all of whom underwent computed tomography–guided/C-arm-guided/open surgical biopsy. Sensitivity, specificity, positive predictive value, and negative predictive value are obtained using standard equations.
Results:
Out of 68 cases of STB, Gene Xpert was positive in 62 (true positive: 62/68) and negative in 6 (false negative: 6/68). Gene Xpert was negative for all 92 cases of CG (true negative: 92/92, false positive 0/92). Thus, in our series, sensitivity of Gene Xpert is 91.18%, specificity is 100%, positive predictive value is 100%, and negative predictive value is 93.88%. Out of all cases of STB, 62/68 (91.18%) were Gene Xpert positive, but only 35/64 (54.69%) was acid-fast bacilli (AFB) culture positive and 53/60(88.33%) was histopathologically conclusive of TB. Also, Gene Xpert was positive in 7/7 (100%) cases of STB in which histopathology were inconclusive and 25/29 (86.21%) cases of STB in which AFB culture was negative.
Conclusion:
In STB, Gene Xpert clearly outperforms AFB culture and histopathology due to its high sensitivity and specificity apart from being rapid in diagnosis. Hence it is justified to diagnose spinal tuberculosis by Gene Xpert though histopathology is confirmative and AFB culture remains the gold standard.
Introduction
Mycobacterium tuberculosis is the most common microbiological agent that causes granulomatous, chronic infection in India and many developing countries. The spine is the most common site of skeletal tuberculosis and accounts for 50% of cases. 1 Early diagnosis and management of spinal tuberculosis (STB) have special importance in preventing serious complications including the neurological deficit, irreversible disability, and spinal deformity.
Confirmation of M tuberculosis by positive culture takes 6 to 8 weeks, which limits its usefulness. 2 Histopathology is an important diagnostic tool but is technically demanding and time consuming. 3 Xpert MTB/RIF assay (Gene Xpert) is a rapid automated molecular test with high accuracy for pulmonary 4 and various extrapulmonary samples of TB such as cerebrospinal fluid, urine, lymph node and other tissues. 5,6 However, adequate data regarding sensitivity and specificity in samples collected from spinal tuberculosis is not available and comparable control group is not available in studies in published literature. We tried to evaluate sensitivity and specificity of Gene Xpert in relation to patients with spinal tuberculosis diagnosed on clinicoradiological parameters, HP (histopathology) and AFB (acid-fast bacilli) culture and compared it to a control group of patients who were diagnosed to be nontubercular lesions based on histopathological and/or microbiological diagnosis.
Methods
After approval from institutional review board, we prospectively studied 68 patients with clinicoradiologically suspected STB who underwent biopsy procedures by computed tomography (CT)–guided, percutaneous C-arm-guided, or open surgical procedures from January 2016 to August 2018. All samples were tested for AFB stain, standard AFB culture, histopathology, and Gene Xpert. Similarly, a control group (CG) of 92 patients was studied, who were clinicoradiologically and histopathologically non-TB lesions who had similar investigations from a biopsy procedure. The results of Gene Xpert were analyzed in relation to histopathology and AFB culture report at 42 days.
Patients’ clinical details, procedure details, and follow-up data were recorded in electronic medical record system along with case sheet. Radiological studies, including X-ray, magnetic resonance imaging (MRI) and CT scan were studied using PACS (picture archiving and communication system). CT-guided biopsy was performed under local anesthesia and all percutaneous C-arm-guided biopsy were done under general anesthesia using standard protocols. The rest of the samples were obtained by open surgical procedures.
All samples underwent following laboratory examinations,
Microscopic smear examination for AFB by Ziehl–Neelsen technique and examined under 100× oil immersions lens.
TB culture was done using incubating culture for 42 days using BaCT/ALERT 3D mycobacterial detection system (Culture bottles—BaCT/ALERT MP medium-enriched middle brook 7Hg broth and LJ media [Lowenstein-Jensen medium] containing p-nitrobenzoic acid [PNB]).
Gene Xpert (Xpert MTB/RIF assay) (Cepheid Inc, Sunnyvale, CA, USA) was done with adherence to the protocol in a real-time format using 6 fluorescent probes called molecular beacons (real-time PCR-CBNAAT—cartridge-based nucleic acid amplification test—completely closed system—Sensitivity of the test 131 test CFU/mL).
Tissue samples were grounded first followed by treatment by N-acetyl-
Post decontamination another treatment was done with the buffer provided in the kit. The sample was then inoculated in cartridge taking care that no particulate matter entering the cartridge.
Pus sample did not need prior treatment and was directly treated with the buffer provided in the kit.
Histopathology study: Tissue was stained with hematoxylin and eosin stain and was seen under a microscope for AFB and epitheloid cell granuloma, Langerhans cell with or without caseation (except for abscess/liquid samples—where histopathology was not possible for practical purposes).
All laboratory investigations—AFB stain, standard AFB culture, histopathology, and Gene Xpert—were done in the same LABORATORY. All reports were confirmed by the concerned senior pathologist.
Diagnostic accuracy was first assessed by simple comparison of results of Gene Xpert in relation to confirmation by histopathological evidence of granulomatous inflammation and/or isolation of M tuberculosis bacilli by culture. Additionally, clinicoradiological presentation and response to antitubercular therapy at follow-up were added for further confirmation of the diagnosis of tuberculosis. In addition, the results of Gene Xpert in the STB group were further analyzed in relation to histopathology and AFB culture.
Results
This study included 160 specimens, all of which were sent to the same laboratory between January 2016 and August 2018. Among the 160 tissue samples, CT-guided fine-needle aspiration cytology (FNAC) was done in 29 cases, percutaneous wide bore needle biopsy in 65 cases, and open surgical biopsy was done in 66 cases (Table 1).
Types of Biopsy Procedures.
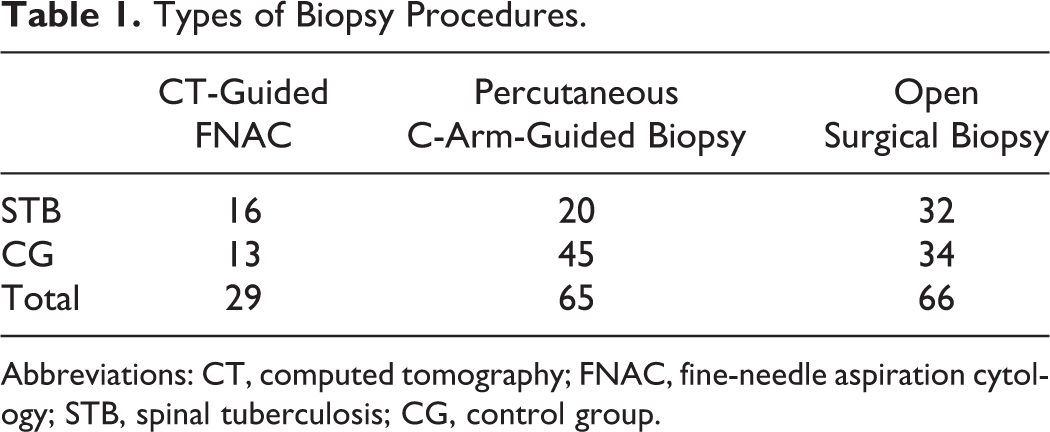
Abbreviations: CT, computed tomography; FNAC, fine-needle aspiration cytology; STB, spinal tuberculosis; CG, control group.
Out of 68 cases of STB confirmed by either histopathology or AFB culture or both, in 62 cases Gene Xpert detected M tuberculosis (true positive: 62/66) and in 6 cases M tuberculosis was not detected by Gene Xpert (false negative: 6/68). Gene Xpert was negative for all 92 cases that were clinicoradiologically and histopathologically non-TB lesions (true negative: 92/92, false positive 0/92). Thus, the sensitivity of Gene Xpert for spinal tuberculosis in our series is 91.18%, specificity is 100%, a positive predictive value is 100%, and negative predictive value is 93.88% (Table 2). CT-guided FNAC was done in 16 cases of STB and 13 cases of CG. Because of such limited sample size in these subgroups, we could not analyze sensitivity and specificity of each biopsy method.
Results of Gene Xpert in STB and CG.a
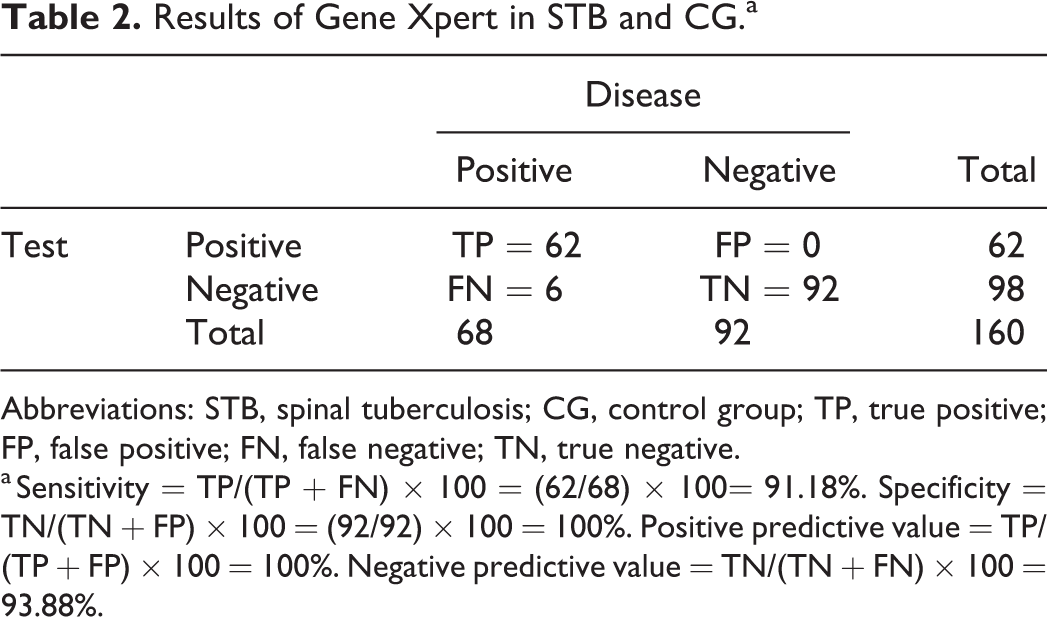
Abbreviations: STB, spinal tuberculosis; CG, control group; TP, true positive; FP, false positive; FN, false negative; TN, true negative.
a Sensitivity = TP/(TP + FN) × 100 = (62/68) × 100= 91.18%. Specificity = TN/(TN + FP) × 100 = (92/92) × 100 = 100%. Positive predictive value = TP/(TP + FP) × 100 = 100%. Negative predictive value = TN/(TN + FN) × 100 = 93.88%.
Out of 68 cases of spinal tuberculosis, 8 were pus samples and hence histopathology was not feasible—in the remaining 60 cases, the sample was obtained for histopathology, which was positive in 53 cases (53/60=88.33%) and was inconclusive in 7 cases (7/60 = 11.67%). Similarly, out of 68 cases of spinal tuberculosis, in 4 cases AFB culture could not be done—out of the remaining 64 cases, AFB culture grew M tuberculosis in only 35 cases (35/64 = 56.69%) (Table 3). Thus, the sensitivity of Gene Xpert, histopathology, and AFB culture with regard to comprehensive final diagnosis is 91.18%, 88.33%, and 56.69%, respectively.
Gene Xpert Results Compared With Histopathology and Acid-Fast Bacilli Culture.

On further subgroup analysis, among 53 patients in whom histopathology was positive for tuberculosis, Gene Xpert was positive in 47 cases (47/53 = 88.68%) and Gene Xpert was negative in 6 cases (6/53 = 11.32%). Similarly, among 29 cases in which AFB culture grew M tuberculosis, Gene Xpert was positive in 33 cases (33/35 = 94.29%) and negative in 2 cases (2/35 = 5.71%). Also, Gene Xpert was positive in all 7 cases of STB in which histopathology was inconclusive (7/7 = 100%). Similarly, out of 29 cases of STB in which AFB culture was negative, Gene Xpert was positive in 25 cases (25/29 = 86.21%) (Table 4).
Results of Gene Xpert, Histopathology, and AFB Culture in the Study.
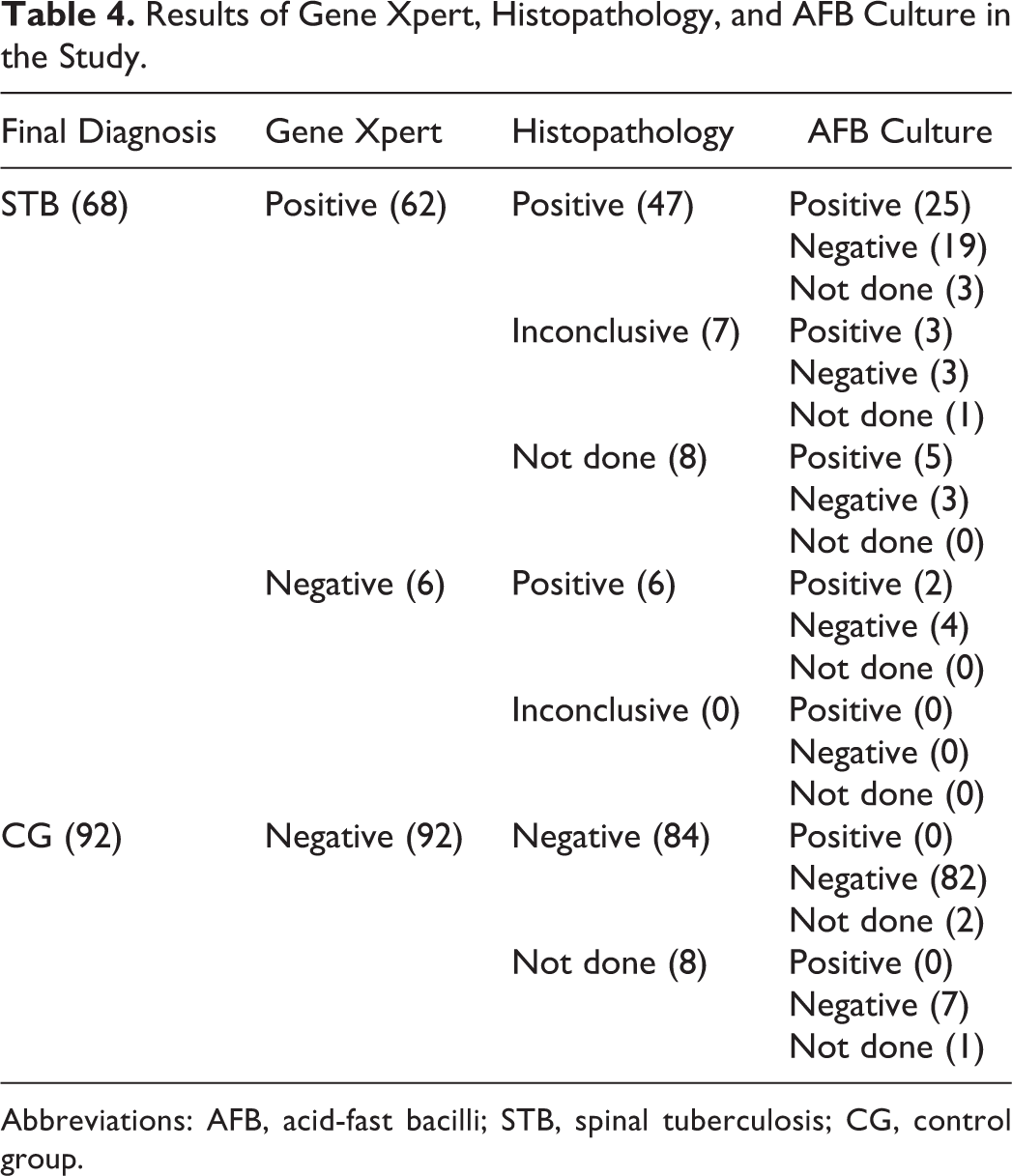
Abbreviations: AFB, acid-fast bacilli; STB, spinal tuberculosis; CG, control group.
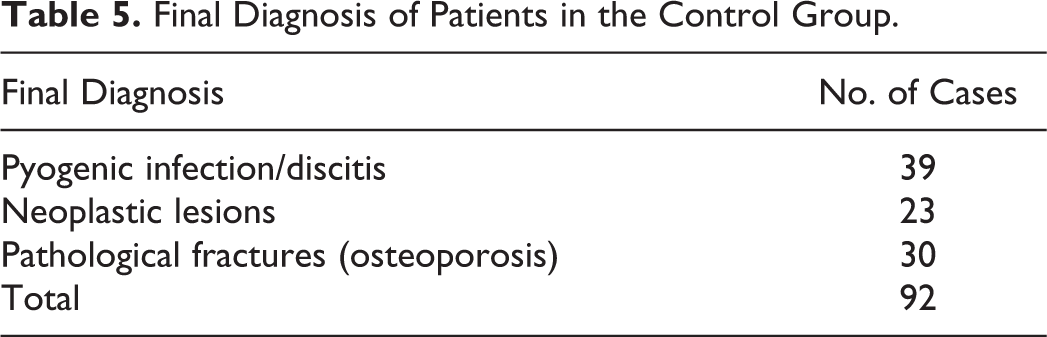
Out of all the samples in which Gene Xpert was positive to M tuberculosis, rifampicin resistance was detected in only 1 case and was replicated in the drug sensitivity report. The patient was put on appropriate second-line antitubercular drugs (ATD) and responded well to therapy. The final diagnosis of patients in the CG is presented in Table 5.
Final Diagnosis of Patients in the Control Group.
Discussion
Tuberculosis of the spine requires prompt diagnosis and early initiation of treatment, otherwise patient may develop kyphosis and/or neurological complication (paraplegia) and other adverse consequences. 2 For diagnosis of osteoarticular tuberculosis, no single modality like AFB culture, AFB staining, histopathology is definite of ascertaining it.
The sensitivity of AFB staining in various published studies was reported in the range of 20% to 60%, which can be increased to a small extent using special physical and/or chemical methods of sample processing and special equipment like fluorescent microscopy/LED fluorescent microscopy. 7 Lakhanpal et al 8 reported 49.53% positivity by AFB culture and a range of 48.6% to 80% has been reported in the literature. Various factors accounted for low AFB culture sensitivity such as paucibacillary as nature of disease, 9 type of species, stain used, experience of the technical person, and so on. In addition to these, it has other limitations like the requirement of live organisms, the long incubation period of 2 to 8 weeks, and biosafety issues. 10 These causes delay in diagnosis and result in poor disease control and increased health care cost. 11 Newer rapid culture techniques like BACTEC and BACTEC-alert are better alternatives compared with conventional culture methods. 12
CT/fluoroscopic-guided FNAC biopsy technique is a useful diagnostic for spinal lesions with accuracy in between 88.5% and 96.4%. 13 Mondal 14 reported 38 cases of vertebral tuberculosis with histopathological features suggestive of TB. With the cytological and morphologic recognition of a granulomatous process, a presumptive diagnosis of tuberculosis in skeletal tissues can be made (excluding other processes), and thus initiation of relatively early appropriate antitubercular treatment can be started but is technically demanding.
The Gene Xpert (Xpert MTB/RIF assay) has been described as a potential “game changer” for TB control. 15 This is a new approach to DNA sequence analysis that uses fluorogenic reporter molecules—nucleic acid hybridization probes—called molecular beacons. 16,17 The Gene Xpert detects M tuberculosis and rifampicin resistance by PCR amplification of the rifampin resistance determining region (RRDR) of the M tuberculosis rpoB gene and subsequent probing of this region for mutations that are associated with rifampicin resistance. 18
This multifunctional diagnostic platform has many advantages over other diagnostic tools. It is an automated, closed system that requires minimal technical expertise, providing a diagnosis of TB and at the same time assessment of rifampicin resistance within 2 hours as opposed to 1 day for smear microscopy, 16 days using liquid culture and 20 days using solid culture. 19 The test reduces the time to start definite treatment from 56 days (interquartile range [IQR] 39-81) to 5 days (IQR, 2-8). 20 It has an analytic sensitivity of 5 genome copies of purified DNA and 131 CFU/mL of M tuberculosis spiked into sample Also it has less cross-contamination, requires much less biosafety infrastructure and minimal training. 21
Molecular techniques have been a great revolution in the diagnosis of tuberculosis providing rapid results while being highly sensitive in pulmonary tuberculosis detection and drug-resistant cases. 4 Also role of Gene Xpert has been established in many types of extrapulmonary samples, such as for lymph node samples, sensitivity ranged from 50% to 100% whereas for cerebrospinal fluid (TB meningitis), the pooled sensitivity was 62.8% (95% CI 47.7%-75.8%) and pooled specificity was 98.8 (95% CI 95.7%-100%). 3,5,22,23 For diagnosis of joint tuberculosis, sensitivity, specificity, accuracy, positive and negative predictive values of PCR were 82.65% (81/98), 91.00% (91/100), 86.87% (172/198), 90.00% (81/90), and 84.26% (91/108), respectively as demonstrated by Sun et al 24 in their study.
In this study, we have tried to find sensitivity and specificity of Gene Xpert in spinal tuberculosis cases, for which adequate literature data is not available yet. This is a prospective study and observed sensitivity of Gene Xpert is 91.18% and specificity is 100%, which correlates well with similar study by Held at al 25 showing sensitivity of 95.6% and specificity of 96.2% and for STB and study done by Arockiaraj et al 26 demonstrating sensitivity of 71.2% and specificity of 100% compared with composite reference standard. Positive predictive value is 100% and negative predictive value is 93.88% in our study, that is, negative result reliably excludes TB. This is the only study that compares Gene Xpert results in TB spine with controlled group of established non-TB cases.
However, these tests are not suitable for patient monitoring as these tests detect DNA from both viable and nonviable bacilli. 20 In our series, out of 6 patients of STB group in which Gene Xpert was negative (false negative), all 5 patients were on ATD (2 weeks to 1.5 years) before biopsy procedure, which might have affected the result of Gene Xpert. But, in the same STB group there were another 12 patients who were on ATD for a different duration (1 week to 2 years) before biopsy procedure but their Gene Xpert was positive. So, starting of ATD before sample collection cannot be solely attributed to negative results of Gene Xpert, nor can it be used as an ideal tool for monitoring the treatment as per this study. But, role of Gene Xpert after treatment with ATD in diagnosis and monitoring cases of STB will be of interest to learn in future studies.
Thus, from a purely technical perspective, no test for TB is perfect. Microscopy, conventional culture, and drug sensitivity test (both phenotypic and genotypic) all have shortcomings and limitations related to accuracy and effectiveness, operator dependency, training and resource requirements, and biosafety. Gene Xpert clearly outperforms microscopy and should be used as the initial diagnostic test but clinicoradiological presentation; culture and histopathology should be rechecked before excluding the diagnosis of STB. Patients identified positively by Gene Xpert without rifampicin resistance should receive appropriate first-line ATD immediately. Rapid drug sensitivity testing for rifampicin is recommended by the World Health Organization. 27,28
Patients at risk of drug resistance in whom rifampicin resistance is detected by Gene Xpert should be placed on an appropriate multidrug-resistant TB regimen immediately and isoniazid continued until the drug sensitivity test result for isoniazid is available. Additional specimen should be provided for conventional culture and DST against other first- and second-line drugs according to World Health Organization recommendations 29,30 and their treatment adjusted accordingly.
Conclusion
In STB, Gene Xpert outperforms AFB culture and histopathology due to its high sensitivity and specificity apart from being rapid in diagnosis. Hence it is justified to diagnose spinal tuberculosis by Gene Xpert though histopathology is confirmative and AFB culture remains the gold standard. It might be useful to have confirmation by clinicoradiological features, histopathology, and AFB culture before excluding the diagnosis of spinal tuberculosis.
Footnotes
Acknowledgments
The authors thank Dr. Roy & Tribedi Diagnostic Laboratory.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.