
Abstract
Study design:
Systematic review.
Objective:
In 1994, the Load Sharing Classification (LSC) was introduced to aid the choice of surgical treatment of thoracolumbar spine fractures. Since that time this classification system has been commonly used in the field of spine surgery. However, current literature varies regarding its use and predictive value in relation to implant failure and sagittal collapse. The objective of this study is to assess the predictive value of the LSC concerning the need for anterior stabilization to prevent sagittal collapse and posterior instrumentation failure.
Methods:
An electronic search of PubMed, Medline, Embase, and the Cochrane Library was performed. Inclusion criteria were (1) cohort or clinical trial (2) including patients with thoracolumbar burst fractures (3) whose severity of the fractured vertebrae was assessed by the LSC.
Results:
Five thousand eighty-two articles have been identified, of which 21 articles were included for this review. Twelve studies reported no correlation between the LSC and sagittal collapse or instrumentation failure in patients treated with short-segment posterior instrumentation (SSPI). Seven articles found no significant relation; 5 articles found no instrumentation failure at all. The remaining 9 articles experienced failure in patients with a high LSC or recommended a different surgical technique.
Conclusions:
Although the LSC was originally developed to predict the need for anterior stabilization in addition to SSPI, many studies show that SSPI only can be sufficient in treating thoracolumbar fractures regardless of the LSC. The LSC might have lost its value in predicting sagittal collapse and posterior instrumentation failure.
Keywords
Introduction
The choice of treatment of spinal fractures is based on a thorough clinical workup and imaging. This enables a complete understanding of the morphology of the fracture and possible ligamentous injury, including a neurological examination to determine any possible presence of neurological deficit. In contrast to the clear diagnostic criteria, the optimal treatment of these injuries remains a subject of ongoing debate. Among the many available treatment options, the short-segment fixation through a posterior approach is the most performed surgical procedure in the treatment of thoracolumbar spine fractures. 1 It offers little morbidity and has a straightforward approach. However, postoperative anterior collapse and posterior implant failure are reported by several authors. 2,3 Some of these failures are thought to be caused by a lack of support from the anterior columns and could be prevented by providing additional anterior spinal support through a separate or combined intervention. 4
To decide whether posterior fixation alone is sufficient or additional anterior stabilization is required, the Load Sharing Classification (LSC) can be used. 5 This is a 3-factor point-value system, which grades vertebral comminution in 3 planes, from 1 to 3 (1 being mild, 3 being severe). The amount of vertebral involvement, the amount of apposition or displacement, and the amount of correction of kyphotic deformity are assessed. 6 Six points or less on the LSC is considered to represent little comminution, whereas scores from 7 to 9 portray high to severe vertebral comminution.
High comminution (corresponding to an LSC of 7 points or more) might result in loss of anterior support. Less anterior support can lead to an increase in loading of the pedicle screws and therefore in a higher chance of instrumentation failure. According to the original study from 1994 by McCormack et al, 5 fractures with an LSC score of 7 or more should therefore be supported with an anterior stabilization, in addition to a 4-screw short-segment posterior stabilization (one level above and one level below the fractured vertebra). Due to changes in technique and implants in the last decades, it remains unclear whether the LSC still has its value in predicting the need for anterior fixation. 1
The current literature varies substantially regarding the predictive value of the LSC. 7 -10 Therefore, this study performs a systematic review of the literature to assess the predictive value of the LSC concerning sagittal collapse and posterior instrumentation failure with a specific interest for patients with thoracolumbar burst fractures with a high LSC score, treated with a posterior stabilization only.
Methods
A comprehensive systematic review of the literature on the predictive value of the LSC concerning sagittal collapse and posterior instrumentation failure was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement. 11
Search Strategy
For this review, PubMed (from the original article of McCormack in 1994 to November 9, 2018), Medline (1994 to November 9, 2018), Embase (1994 to November 9, 2018), the Cochrane Database of Systematic Reviews (CDSR), and the Cochrane Central Register of Controlled Trials (1994 to November 9, 2018) were searched. Only articles written in the Dutch, English, and German language were reviewed. For any other language, restrictions were applied. A flow chart of the included articles is shown in Figure 1.
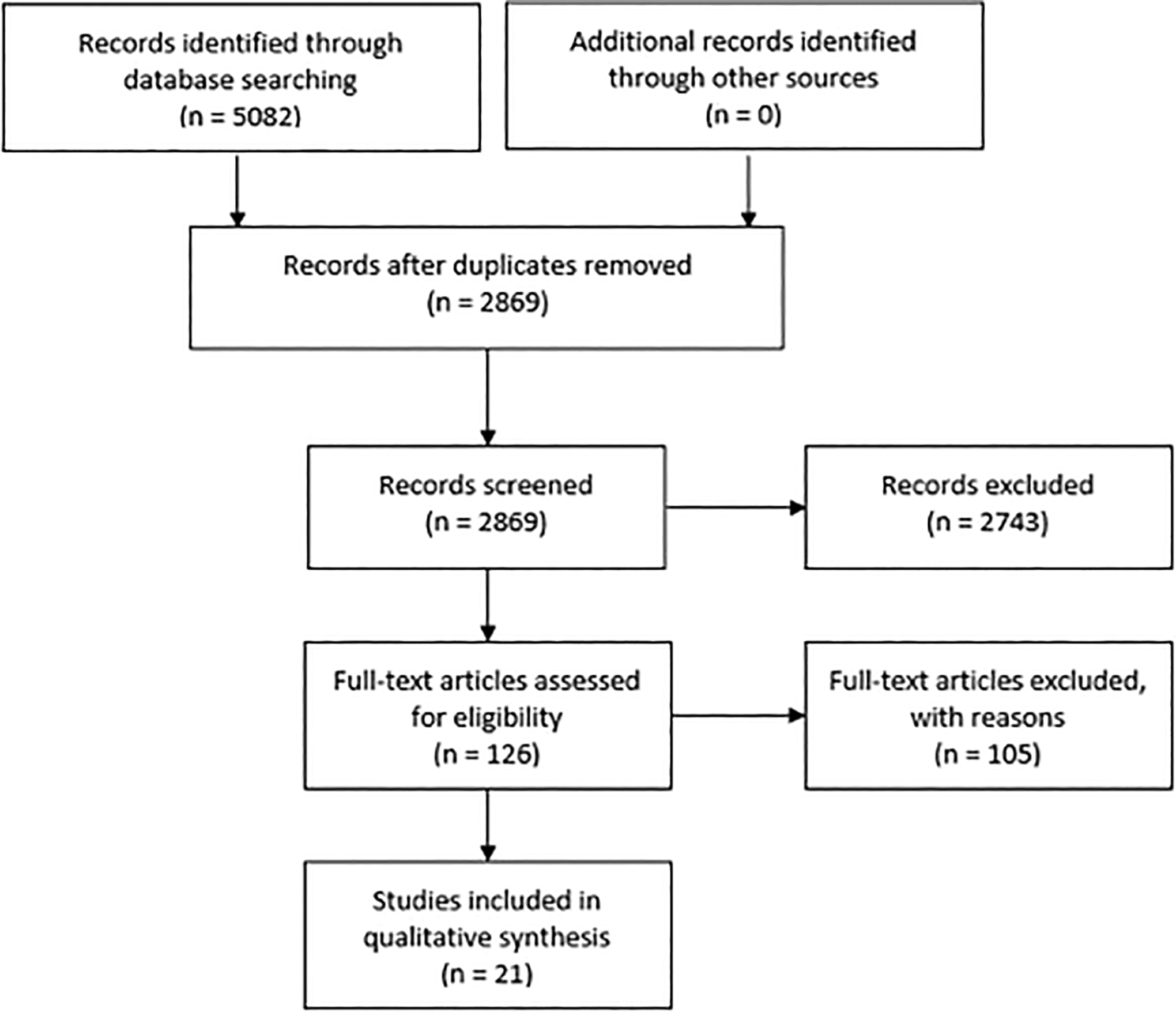
Flowchart of selected articles according to the PRISMA statement.
Inclusion and Exclusion Criteria
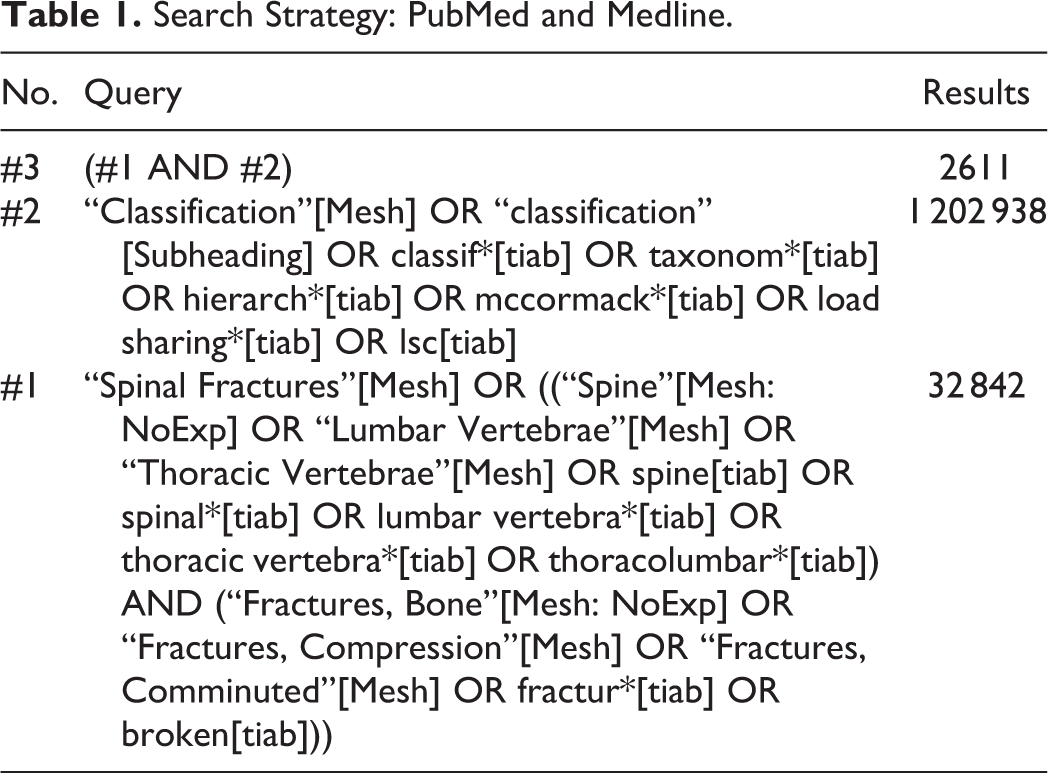
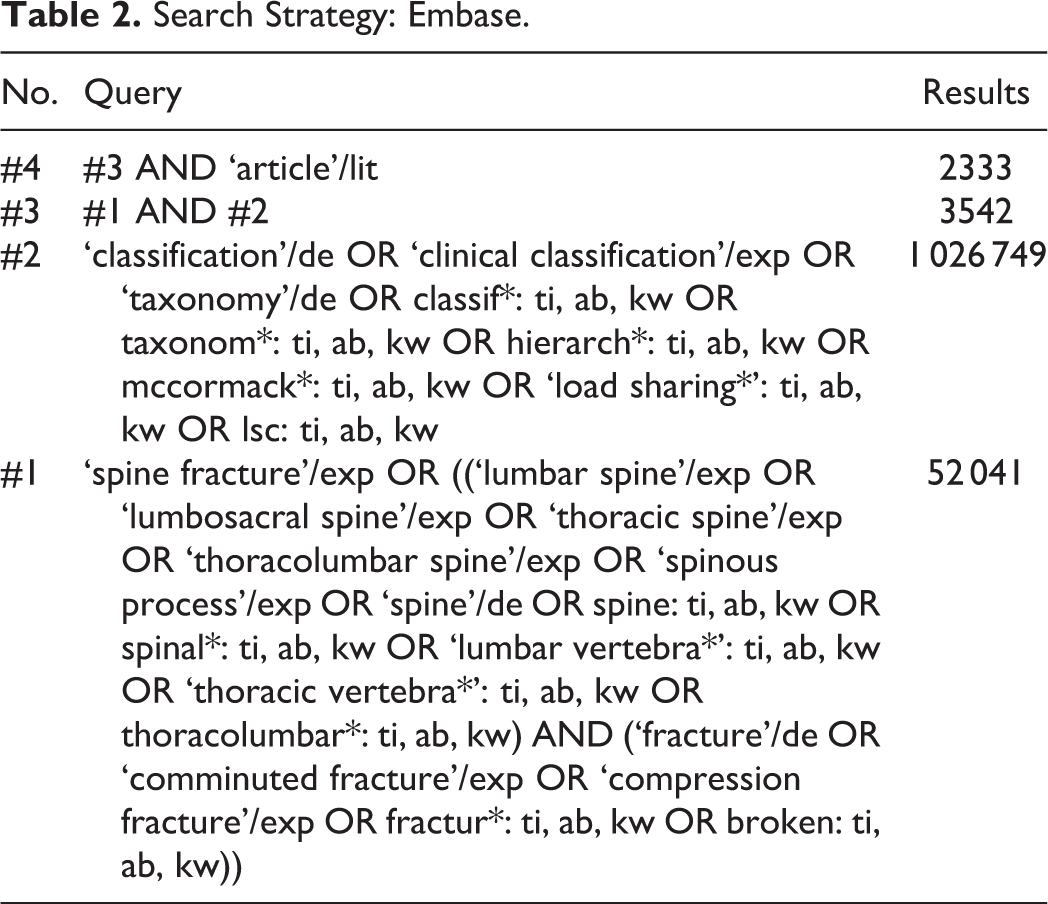
The search entailed medical subject headings (Mesh terms) and also alternatives for these words. Inclusion criteria for articles were (1) cohort or clinical trial, (2) including patients with thoracolumbar burst fractures and (3) who were evaluated by the LSC for the severity of the fractured vertebrae. Exclusion criteria were fractures caused by osteoporotic or pathogenic reasons. Also, fractures in patients over 80 and under 15 years old were excluded. The search strategy can be found in Tables 1, 2, and 3.
Search Strategy: PubMed and Medline.
Search Strategy: Embase.
Search Strategy: Wiley/Cochrane Librarya.
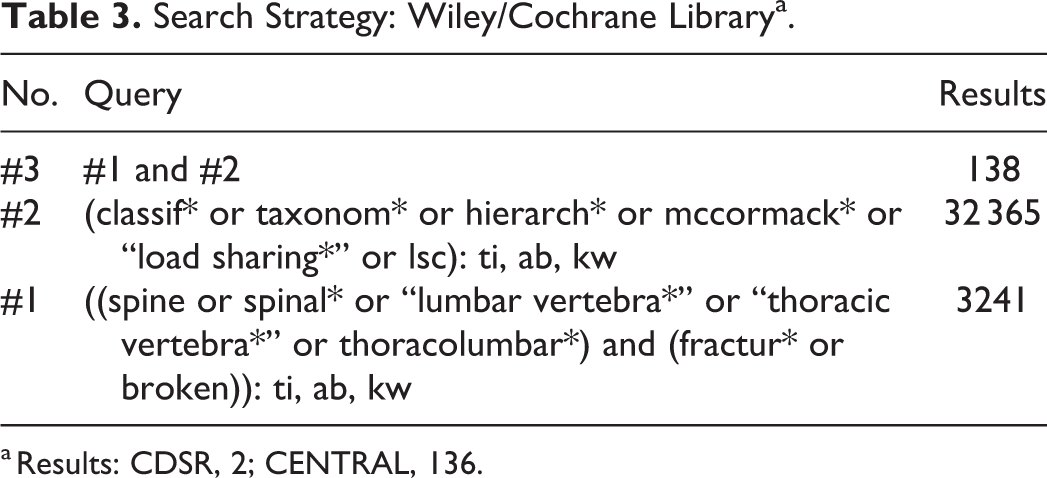
a Results: CDSR, 2; CENTRAL, 136.
Screening
After removal of the duplicates in EndNote, 2 authors (WT, MJ) independently determined the relevance of each article to this review based on the abstracts and titles. A second selection was made based on the full text, where after the final articles were included.
Data Collection
Extracted data from the included articles was (1) the study design, (2) patients demographics, (3) received surgical method, (4) LSC scores, and (5) outcomes after follow-up, in particularly related to complications as loss of correction, instrumentation failure, and/or sagittal collapse. Furthermore, the level of evidence (Centre of Evidence Base Medicine, University of Oxford) was determined.
Results
Five thousand eighty-two articles were identified through the databases. After removal of the duplicates, 2869 articles were screened. A total of 2743 articles were excluded based on title and abstract. Of the remaining 126 articles, 105 did not meet the inclusion criteria based on the full text. The remaining 21 articles met the inclusion criteria. All 21 articles reviewed reported the surgical technique, the severity of the fracture evaluated by the LSC, and occurrence of instrumentation failure. In 12 of the 21 articles (57%), no effect of the LSC was found on the outcome. The remaining 9 studies found a relation between a high LSC and instrumentation failure or loss of correction or already chose the surgical approach based on the LSC score. A comprehensive summary of the results is presented in Table 4.
Summary Results of the Included Studies.
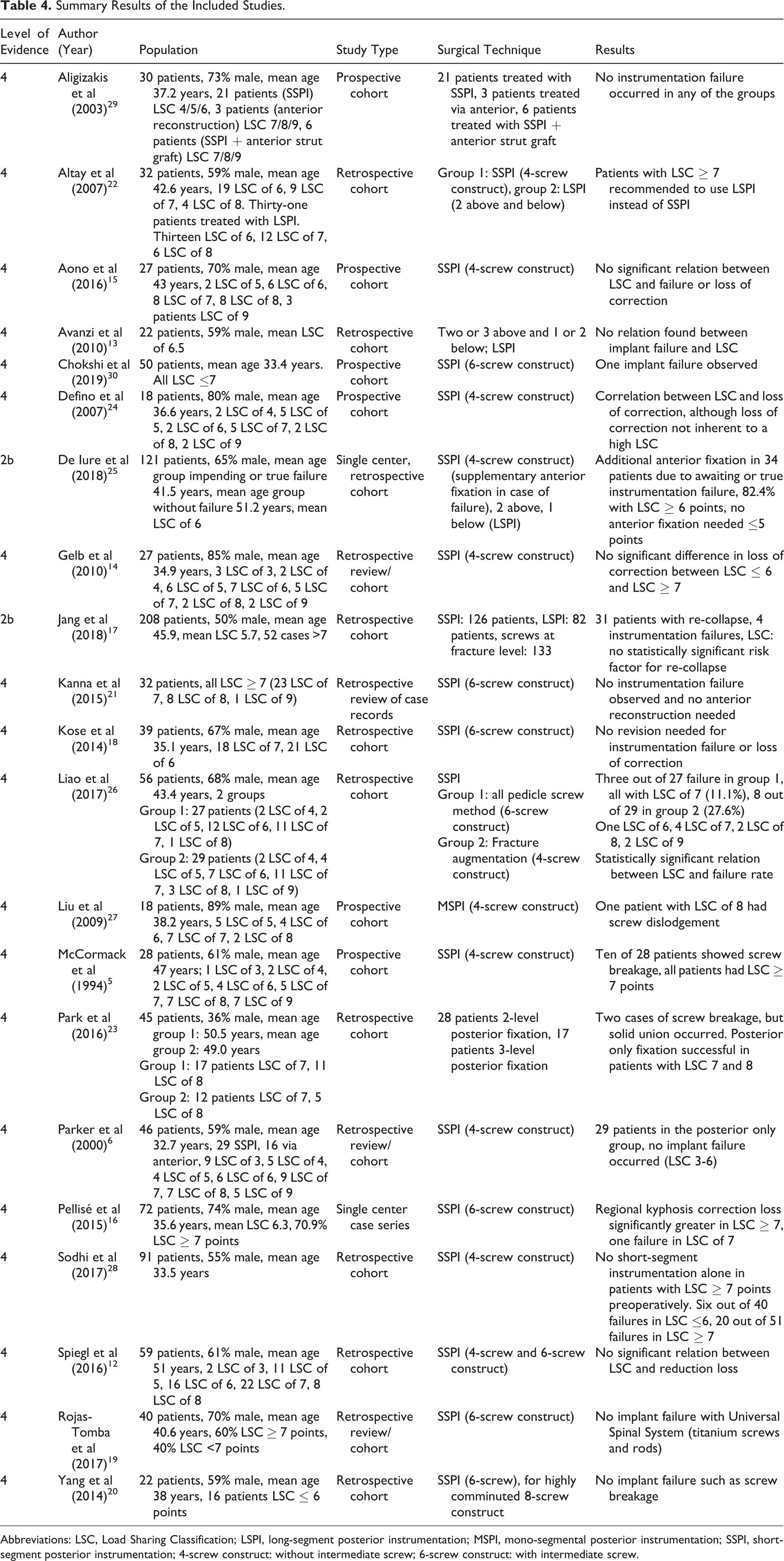
Abbreviations: LSC, Load Sharing Classification; LSPI, long-segment posterior instrumentation; MSPI, mono-segmental posterior instrumentation; SSPI, short-segment posterior instrumentation; 4-screw construct: without intermediate screw; 6-screw construct: with intermediate screw.
No Relation Between LSC and Instrumentation Failure
Of the 12 articles that found no effect of the LSC on loss of correction or implant failure, 6 reported no significant relation between the LSC and instrumentation failure. 12 -17 Four did not find instrumentation failure at all. 18 -21 One reported no instrumentation failure but recommended to use long-segment posterior instrumentation (LSPI) instead of short-segment posterior instrumentation (SSPI) for patients with a high LSC score. 22 The last one reported instrumentation failure, but stated that SSPI only can be used successful in patients with a high LSC. 23 Of the 656 patients that were described in these 12 studies, 317 had a high LSC score and 317 had a low LSC score. Of the remaining patients the score was not specified. One patient in the high score group experienced instrumentation failure; none experienced failure in the low score group. This, however, was not reported in every study. Within this group, it was stated that anterior reconstruction is not necessary in most fractures and that a 2-level (6-screw construct) posterior fixation can be used successfully in patients with a high LSC score. 15,16 Pellisé et al 16 found a statistically significant relation between LSC scores ≥7 and loss of correction. However, no correlation was found between the LSC score and instrumentation failure. In addition to that, the loss of correction observed was not associated with significant differences in clinical outcomes and further surgery due to correction loss was not required in any case.
Relation Between LSC and Instrumentation Failure
Six studies reported a relation between a high score and instrumentation failure. 5,24 -28 Of the 332 patients that were described in these 6 studies, 112 had a high LSC score and 99 a low LSC score. In the remaining patients the score was not specified. Of these patients 63 in the high score group and 13 in the low score group experienced failure. This, however, was not reported in every study. Liao et al 26 concluded that a high LSC causes higher failure rates. Liu et al 27 used mono-segmental posterior instrumentation and conclude that an LSC of 8 correlated with a high incidence of loss of reduction or implant failure.
Use of LSC Score to Decide Surgical Technique
Two articles already based their surgical approach on the LSC score 6,29 and one study only included low LSC scores in order to prevent the need for anterior reconstruction. 30 Of the 126 patients described in these 3 studies, 30 had a high score and 96 a low score. One failure occurred in the group with a low score; no failure occurred in the group with a high score. Aligizakis et al 29 stated that the LSC is a helpful adjunctive tool that can complement but not replace other forms of classification.
Discussion
When treating thoracolumbar fractures, there is no universal agreement on the best type of surgical treatment to achieve and maintain stabilization. The 21 studies reviewed used the classification system since the introduction of the LSC in 1994 and additionally looked at complications such as instrumentation failure. Of these 21 studies, 6 studies actually report a relation between the LSC and failure. Those 6 studies, including the study of McCormack et al, 5 reported instrumentation failure in patients who had an LSC of 7 or more. The remaining 15 studies showed that there was no significant correlation between instrumentation failure and the number of points scored on the LSC. Two studies only showed an association between loss of correction and the LSC, 16,24 although this did not appear to be entirely inherent to a high score. 24
The classification system of McCormack et al 5 has been used intensively over the past 20 years. However, their article has some limitations. In their retrospective study only 28 patients were included, treated with an older generation screws and rods. The conclusions drawn by the authors can be debated nowadays and these thoughts are not new. Several studies already reported the questionable value of the LSC regarding instability and instrumentation failure. 13,21,25,31 Jang et al 17 discussed that another critical limitation of the original article is that no patient-related parameters were considered. In their study, age (>43 years old) and gender were related to re-collapse and not the LSC score. Pishnamaz et al 32 compared different spine fracture classification systems and concluded that other systems have a higher reliability. Therefore, the role of the LSC in clinical practice is arguable.
In the past decades, new insights and numerous improvements have modified the approach on spinal trauma care. McCormack et al 5 stated that with a high LSC score anterior stabilization is necessary in order to prevent failure. However, anterior stabilization is less desirable due to the potentially increased morbidity and the desired preservation of spinal motion, especially in younger patients. 19,21 Therefore, the wish to obtain sufficient stabilization via a posterior only approach is present.
Main differences seen in the reviewed articles in comparison with the article of McCormack et al 5 are concerning the surgical technique. In the article of McCormack et al, 5 an SSPI with 4 screws was used. Most spinal surgeons did not use this technique and are using various modifications to improve the stiffness of the posterior construct. The modifications used are extending the SSPI, using cement augmentation at fracture level or, in most cases, the use of intermediate screws at the level of the fractured vertebra. Besides the changed techniques, great improvements have been made regarding the materials used. In 1994, only stainless steel screws and rods were used. Nowadays, all constructs are made of titanium, which is said to have twice the strength and elasticity of stainless steel. Therefore, it can bear more weight and is less likely to break. 15 Modern surgical techniques and more sophisticated instrumentation may have contributed to the reduction in instrumentation failure. 14,19,20 Few studies were comparable to the original article of McCormack et al. 5 The studies that had used the same technique either did not mention the materials used or used titanium screws and rods which makes it incomparable to the stainless steel constructs used by McCormack et al. 5 Due to these improvements the LSC has not managed to maintain itself in present time. Therefore, it has lost its predictive value and thus its reliability for predicting clinical outcomes. 19 Wood et al 33 discussed in a comprehensive view on the management of thoracolumbar spine fracture that there still remain many uncertainties regarding the best approach to the treatment of spinal fractures. Numerous classification systems have been proposed of which the AOSpine classification, as described by Reinhold et al, 34 has been used widely and is thought to be most applicable in clinical practice. 32 However, further research is still necessary to asses which system or which combination of systems is best in predicting instrumentation failure and the need for anterior stabilization.
Limitations
A limitation of this review is that in case of instrumentation failure, only the number of points on the LSC was considered and no other possible contributors. McCormack et al 5 reported that the stability of the vertebral body and the clinical outcome is not only dependent on the degree of comminution, but is largely determined by ligamentary damage. 26,29 Because ligamentary damage plays a major role in the indication for surgery, no surgical decision can be made based on the LSC only. Other causes that contribute to instrumentation failure may, among other things, include age, gender, lifestyle, muscle strength, and previous fractures or surgery. These were not considered in this review. Another limitation is that the results of the studies reviewed may be difficult to compare due to the fact that the studies have small populations, the fracture types can be different, and a variety of techniques is used. There is a possibility that the LSC has more influence on one technique than the other. In addition, some studies showed a relation between instrumentation failure and the LSC, thus not significant. This occurred in studies with a small sample size. 12,14,15,24 Due to differences in study design and various cutoff values for a high LSC score it was impossible to perform a meta-analysis.
Conclusions
Although McCormack et al 5 describe that anterior stabilization in addition to SSPI is necessary in patients with a high LSC score, many studies show that SSPI only can be sufficient and safe enough in treating thoracolumbar fractures regardless of the LSC. Therefore, the LSC might be losing its predictive value concerning sagittal collapse and posterior instrumentation failure.
Footnotes
Acknowledgment
The authors thank Mr J. C. F. Ket from the Medical Library of the VU University of Amsterdam for performing the database searches.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.