
Abstract
Study Design
Systematic Review.
Objectives
Identify risk factors for mechanical instability in thoracolumbar gunshot wounds to develop a new classification system.
Methods
A systematic review following PRISMA 2020 guidelines was conducted across multiple databases from January 1, 1990, to September 12, 2024 (PROSPERO: CRD42023458804).
Results
Of 2400 records, 33 studies (3195 patients) met inclusion criteria, mostly retrospective and single-center, with varying definitions of instability. Direct comparison was limited due to clinical heterogeneity. Only 12 studies defined mechanical instability, mainly using the Denis three-column theory. Instability was reported in less than 10% of cases, except for one higher-rate outlier. The main markers included vertebral body comminution and potential ligamentous injury. Management was mainly conservative, with a low fixation rate (1.5-9.7%). Imaging relied on CT and static X-rays, with some studies advocating for dynamic radiographs.
Conclusion
There is a lack of standardized definitions for mechanical instability in civilian thoracolumbar gunshot injuries. Four recurrent unstable patterns were detected, with vertebral body comminution as the most consistent marker. The need for a standardized classification system and further prospective studies is evident.
Introduction
Patients with civilian spinal gunshot wounds exhibit a broad range of clinical manifestations upon admission, ranging from isolated, stable vertebral fractures to severe polytrauma cases that require complex and challenging treatment. 1 The surgical management of these injuries remains a subject of ongoing debate, with significant discussions in the literature concentrating on factors such as neurological decompression, removal of bullets from the vertebral canal, repair of cerebrospinal fluid leaks, and management of spinal instability. 2
Although spinal gunshot wounds are often viewed as inherently stable, a clear consensus on the definition or classification of unstable fracture patterns is lacking. It has been suggested that gunshot injuries leading to fractures of both pedicles or facet joints should be deemed unstable and managed with fixation.1-3 However, existing classification systems, such as the AO Spine Thoracolumbar Injury Classification System, were not designed for penetrating injuries. 4 Spinal gunshot wounds possess unique biological and mechanical characteristics that demand a different approach. The absence of a specific classification system and a clearly defined concept of mechanical stability further complicates clinical decision-making. 2
This systematic review aims to identify risk factors associated with mechanical instability in civilian thoracolumbar gunshot wounds, providing evidence to support the development of a new classification system for these injuries.
Materials and Methods
We conducted a systematic review of the literature in the PubMed, Embase, Lilacs, and Cochrane Library databases to identify factors associated with mechanical instability in civilian thoracolumbar gunshot wounds. This review was conducted according to the PRISMA 2020 Statement and registered in PROSPERO (CRD42023458804). All deviations or amendments to the registered protocol have been documented to ensure transparency.
A clinical question based on the patient, intervention, comparison, outcome model (PICO) was developed to clarify the scientific issue and assess eligibility: “In patients with civilian thoracolumbar gunshot wounds, what risk factors are associated with the development of mechanical instability?”
Criteria for Considering Studies for This Review
To address this question, we investigated the risk of mechanical instability and related factors in studies examining civilian thoracolumbar gunshot wounds based on the criteria outlined below.
We included both randomized and non-randomized trials, as well as prospective and retrospective comparative cohort studies, including case-control studies. We excluded case reports, case series, cadaveric studies, diagnostic studies, register-based studies (because they lack the radiological and clinical detail required to classify fracture patterns and evaluate mechanical instability), and reviews (systematic and narrative) from the review.
Patients
This study involved men and women with thoracolumbar gunshot wounds located between the T1 and L5 vertebrae. We excluded studies that focused solely on pediatric patients or cervical injuries. Additionally, we excluded studies concentrating on military injuries or high-velocity gunshot wounds due to significant differences in soft tissue and bone injury patterns, as well as varying mechanisms of injury, especially in military contexts. Civilians typically sustain gunshot wounds from lower-velocity handguns, which cause less tissue damage and spinal instability compared to injuries from high-powered rifles and explosives. High-energy weapons, with muzzle velocities exceeding 2000 feet per second, can lead to serious indirect injuries, such as cavitation.
Intervention
We reviewed studies that examined non-operative management of thoracolumbar gunshot wounds.
Comparator
Studies on surgical treatment served as comparators; however, in line with our review’s objective, studies lacking a comparison group were also included.
Outcome
Mechanical instability. Because no standardized definition exists for thoracolumbar gunshot injuries, we established an a priori operational definition. Mechanical instability was considered present when studies:
Applied a recognized classification system like Denis three-column theory (instability defined as damage in two or more columns), Thoracolumbar Injury Classification and Severity Score System (TLICS) with a score of five or higher, or other recognized classification frameworks, or reported qualitative features compatible with instability. These features include severe vertebral body comminution, posterior element or ligamentous disruption, progressive deformity, neurological deterioration, or failure of conservative management requiring stabilization.
This operational definition was applied consistently across study screening, data extraction, and synthesis. Variations in definitions or diagnostic criteria used by individual studies were systematically documented for comparative analysis.
Language and Time
We included articles in English, Portuguese, or Spanish published between January 1, 1990, and September 12, 2024.
Search Methods for Identifying Studies
Information Sources
We searched the MEDLINE (PubMed), Embase (OVID), Lilacs, and Cochrane Library databases, along with the reference lists of included studies and relevant reviews identified in the search (snowball strategy).
Search Strategy
Our literature search focused on Medical Subject Headings and terms related to thoracolumbar gunshot wounds. We developed the following search strategy for MEDLINE: (spine [mesh] OR “spinal”:ti,ab OR column [tiab] OR columns [tiab] OR vertebra [tiab] OR vertebral [tiab] OR vertebrae [tiab]) AND (wounds, gunshot [mesh] OR gunshot [tiab] OR firearm [tiab] OR firearms [tiab] OR gun [tiab] OR guns [tiab] OR shotgun [tiab] OR shotguns [tiab]). The search was not restricted by study design or language; however, due to resource limitations, only studies in English, Portuguese, or Spanish were included. We searched for studies published between January 1, 1990, and September 12, 2024. The MEDLINE search strategy was adapted for each database by using the corresponding controlled vocabulary and by adjusting field tags and operators to match the database-specific syntax. Free-text terms were preserved across databases to maximize sensitivity (Supplemental Table S1). After identifying relevant studies, the reviewers also manually screened the reference lists of included articles to identify additional pertinent studies (snowball strategy). Two independent reviewers conducted this process, and any disagreements regarding the inclusion of additional studies were resolved through discussion or, when necessary, adjudication by a third reviewer.
Data Management
The search results were uploaded to Zotero Reference Manager (Corporation for Digital Scholarship, 2023), an internet-based software program that facilitates collaboration among reviewers during the study selection process. Duplicates were removed. Before the formal screening process, we trained new review team members who were unfamiliar with citation management software.
Selection Process
The selection process involved four reviewers who were divided into two groups, each independently screening the titles and abstracts according to the inclusion criteria. Disagreements were resolved through discussion or by consulting an expert researcher who was not part of the screening and selection process. Articles chosen for full-text review were sourced from the library. Each group of reviewers then examined the full-text articles selected by the other group and vice versa (crossover design) to minimize potential selection bias. During the full-text review, the references of the studies were also assessed for eligibility (snowball strategy). Any potential conflicts among the reviewers were resolved or referred to a third party.
Data Collection and Analysis
Data Extraction
The data were extracted into two different tables: one containing the descriptive characteristics of the studies and the other summarizing the findings. Study characteristics included the first author’s name, year of publication, country, study design, participant data, intervention/comparator data, definitions or criteria for mechanical instability, study period, mean follow-up, and funding/conflict of interest data. We documented the definitions and criteria for mechanical instability resulting from thoracolumbar gunshot wounds among the included studies. We analyzed the synthesis of mechanically unstable injuries, which encompassed those classified as unstable upon arrival and those that did not respond to non-operative management with new posterior neurological injury or pain. Data extraction for definitions of instability was performed independently by two reviewers. Any discrepancies were resolved through discussion, and when consensus could not be reached, a third reviewer adjudicated.
Risk of Bias Assessment
The included studies were evaluated for risk of bias using the ROBINS-E tool (Risk Of Bias In Non-randomized Studies of Exposures), which is specifically designed to evaluate non-randomized studies investigating exposures or risk factors. 5
For the ROBINS-E assessment, we prespecified a set of key confounders relevant to mechanical instability in spinal gunshot injuries. These included patient-related factors (age, sex, comorbidities, baseline neurological status), injury-related characteristics (spinal level, number of vertebrae involved, projectile trajectory and energy, associated injuries), treatment-related aspects (management approach, timing of surgery, initial external stabilization), radiological/definitional issues (imaging modality, definition of instability, pre-existing spinal disease), and study context (type of center, historical period, follow-up adequacy). Studies that did not consider these confounders were deemed to be at a “very high risk” of bias regarding the confounding domain.
Effect Measures and Statistical Analysis
Descriptive statistics summarized the characteristics of the included studies, such as the proportion of mechanically unstable injuries, treatment methods, and patterns of unstable injuries. Data analysis and synthesis were performed using RevMan 5.4.1 (The Cochrane Collaboration, 2020).
Strategy for Data Synthesis and Quality Assessment
The results from individual reviewers were combined into a single data table. This table was discussed with the entire team of reviewers to reach a consensus on the outcomes of the review. The data were also assessed for suitability for quantitative meta-analysis. The Grading of Recommendations, Assessment, Development, and Evaluations approach was employed to evaluate the certainty of the evidence. 6
Results
Study Selection
A total of 2400 records were identified through the database searches. After removing duplicate records, 2381 titles remained. A total of 47 full-text articles were screened for eligibility,7-53 of which 17 were excluded.31,32,39-53 4 additional records were found through citation searching,54-57 of which one was excluded.
55
Thus, 33 articles were included in the systematic review (Figure 1).7-30,33-38,54,56,57 Studies were excluded for the following reasons: registry-based studies (n = 5)39,40,43,44,47; lacking sociodemographic data (n = 1)
41
; excluding unstable cases (n = 1)
42
; not differentiating the spinal region (n = 5)45,49,51,52,55; being descriptive studies (n = 3)46,48,50; duplicating data from other studies by the same research group (n = 2)31,32; including high-velocity gunshot wounds (n = 1).
53
*Consider, if Feasible to do so, Reporting the Number of Records Identified From Each Database or Register Searched (rather than the Total Number Across all Databases/Registers). **If Automation Tools Were Used, Indicate How Many Records Were Excluded by a Human and How Many Were Excluded by Automation Tools. Source: Page MJ, et al. BMJ 2021;372:n71. doi: 10.1136/bmj.n71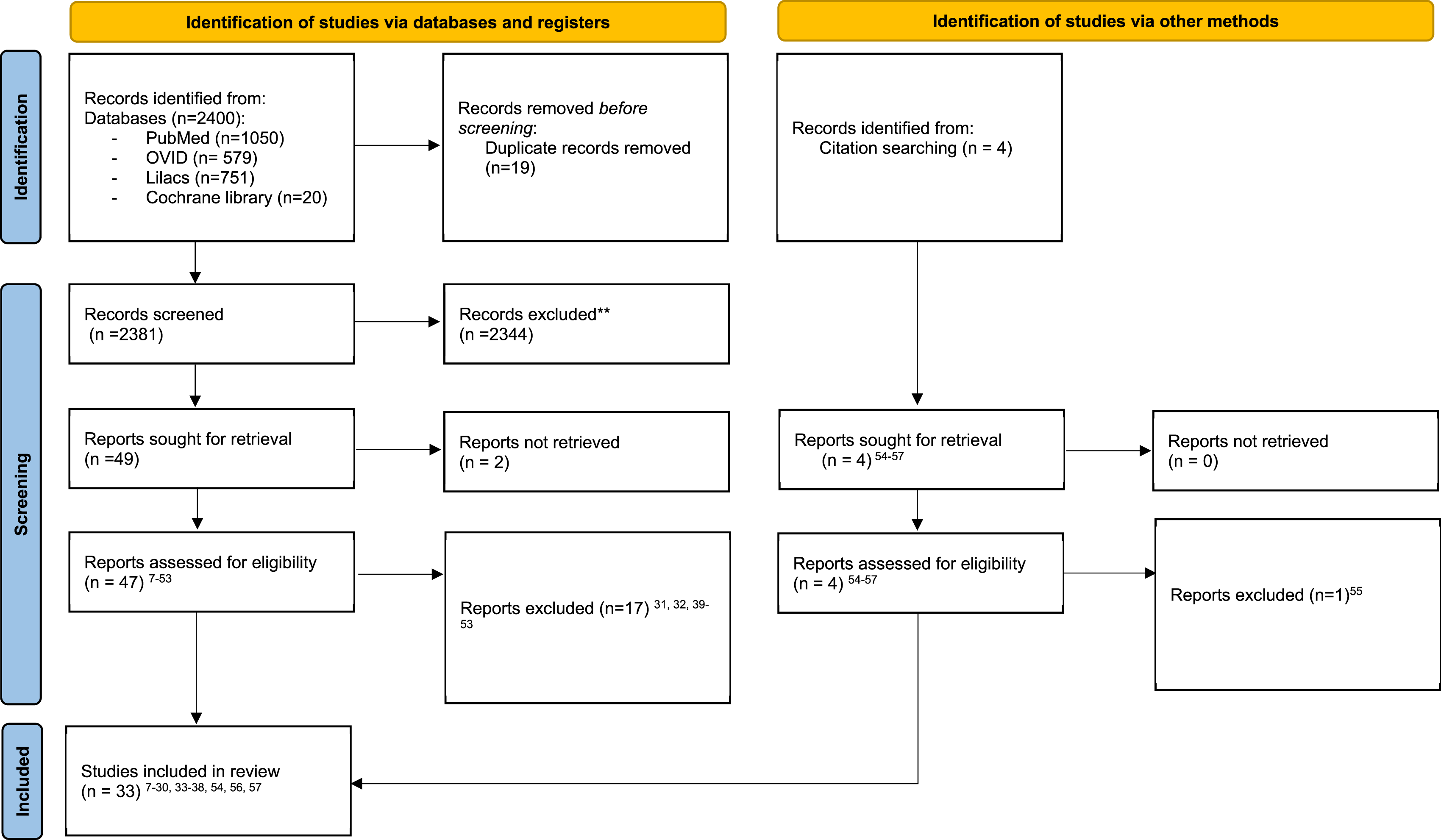
Study Characteristics
Study Characteristics
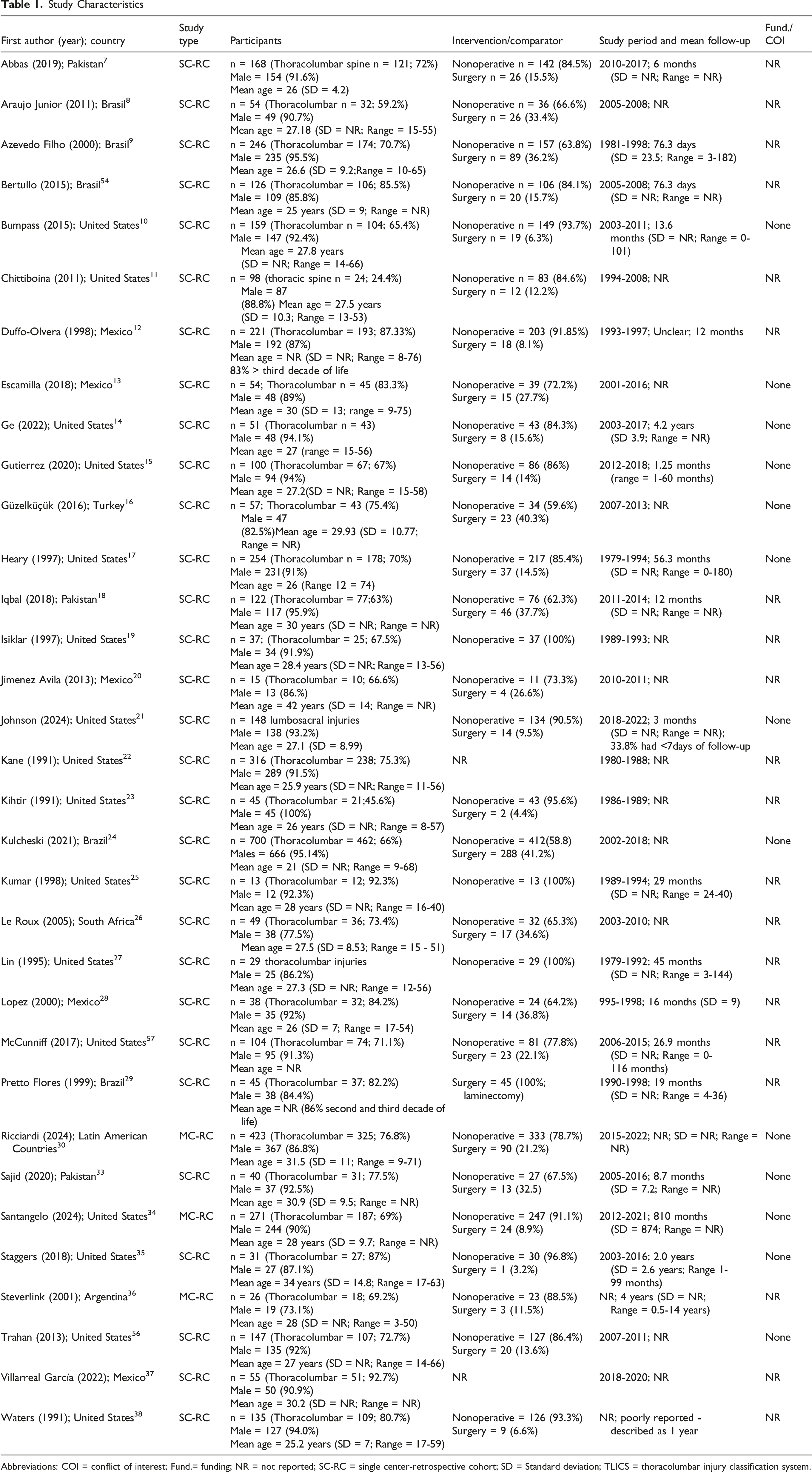
Abbreviations: COI = conflict of interest; Fund.= funding; NR = not reported; SC-RC = single center-retrospective cohort; SD = Standard deviation; TLICS = thoracolumbar injury classification system.
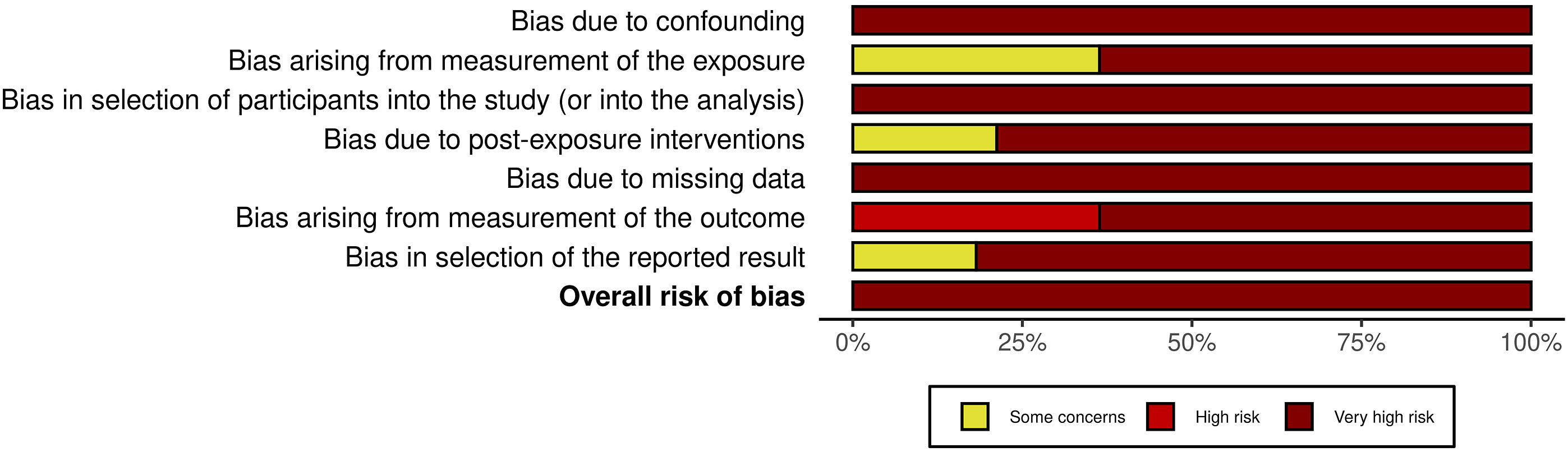
Risk of Bias Assessment
Assessment using the ROBINS-E tool indicated that all studies had an overall very high risk of bias (Figures 2 and 3). Traffic light plot of risk of bias in included studies using the ROBINS-E tool. Each column represents a specific domain of bias: D1, bias due to confounding; D2, bias arising from measurement of the exposure; D3, bias in selection of participants into the study (or into the analysis); D4, bias due to post-exposure interventions; D5, bias due to missing data; D6, bias arising from measurement of the outcome; D7, bias in selection of the reported result. Colors indicate judgment: red circle with exclamation mark, very high risk; red “X”, high risk; yellow dash, some concerns. Summary bar chart of risk of bias domains across all included studies. The horizontal bars show the proportion of studies judged to have very high risk (dark red), high risk (red), or some concerns (yellow) for each bias domain. Overall, most studies exhibit very high risk of bias in multiple domains, highlighting the limitations of the current literature.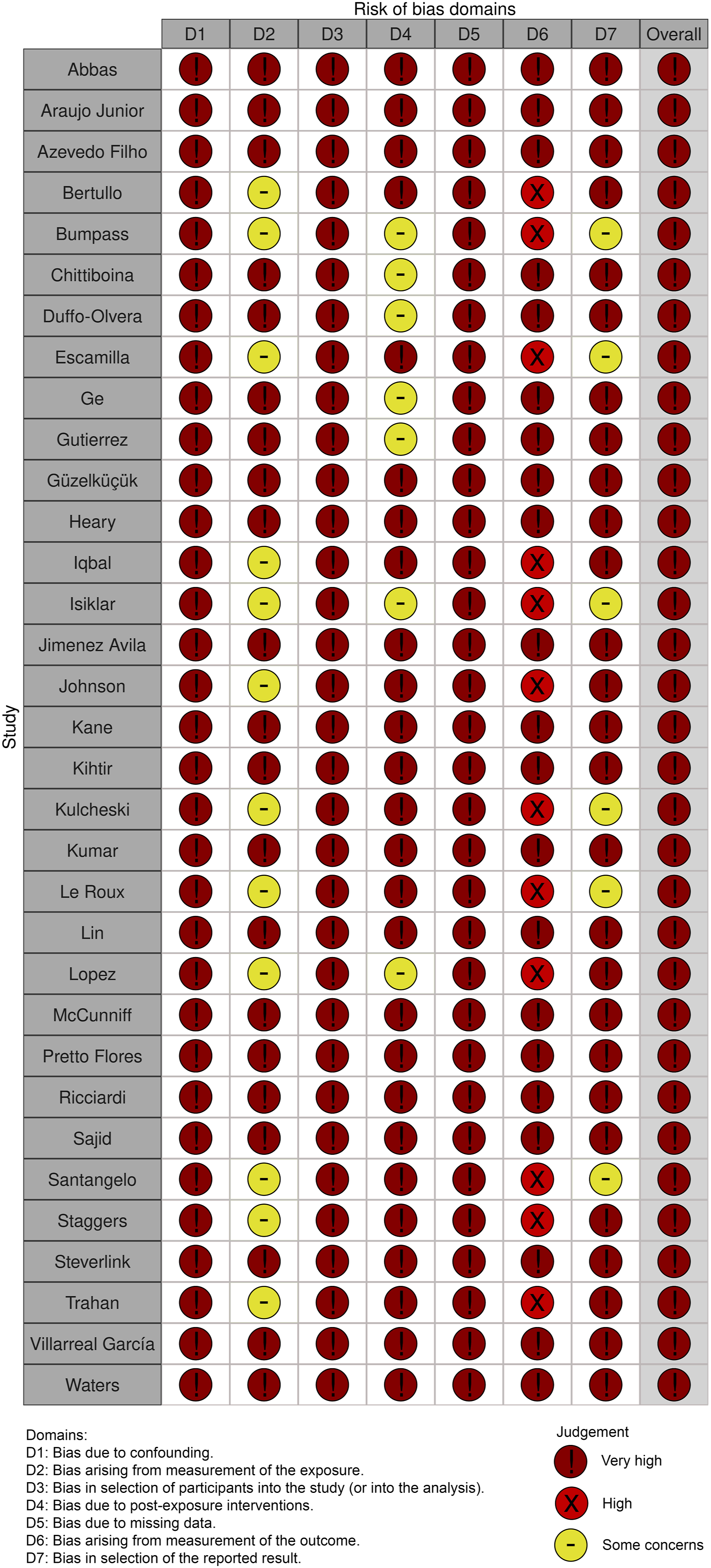
None of the included studies applied appropriate methods to control for confounding factors (e.g., stratification, regression, matching, standardization, or inverse probability weighting). This limitation is probably related to the predominantly small sample sizes, which lacked sufficient statistical power to allow for such analyses. Only a minority of studies provided precise descriptions of fracture patterns to estimate potential determinants of mechanical instability. As a result, exposure measurement was heterogeneous, with most studies relying on radiographs and CT scans, but without consistent or universal application across studies.
Selection bias is a common issue in retrospective, single-center studies. The follow-up periods were often underreported, typically short-term, and poorly defined, with frequent omissions regarding the trauma-to-evaluation interval (such as referral times). This suggests that the exposure window varied significantly among patients with similar injuries. Additionally, probably case selection tended to favor more severe patients, including those with neurological deficits or multiple traumas. As a result, there was an underrepresentation of isolated fracture patterns in patients who did not have neurological or systemic complications.
Additional concerns included post-exposure intervention bias. For example, patients assessed with CT scans had more detailed characterization of fracture morphology than those assessed only with plain radiographs, potentially leading to differential accuracy in exposure classification. The absence of a universally accepted or consistently reported use of orthoses precludes determining the true impact of such interventions in potentially unstable injuries. Similarly, concomitant neurological injury requiring decompression surgery may have influenced the indication for fixation, thereby limiting the ability to discriminate clearly between cases rated as unstable vs stable.
Handling of missing data was also inadequate across studies. Neither complete case analyses nor imputation methods were performed, leading to a high risk of bias. Outcome assessment was further limited by the absence of standardized criteria for instability, reliance on short and poorly documented follow-up, and inconsistent imaging strategies (with CT being used more frequently, while MRI or dynamic radiographs were rarely reported).
Finally, none of the included studies provided a pre-specified analysis plan for evaluating mechanical instability associated with particular injury patterns, making selective reporting difficult to exclude.
Definition of Mechanical Instability
Unstable Thoracolumbar fracture Distribution, management, and Risk Factors
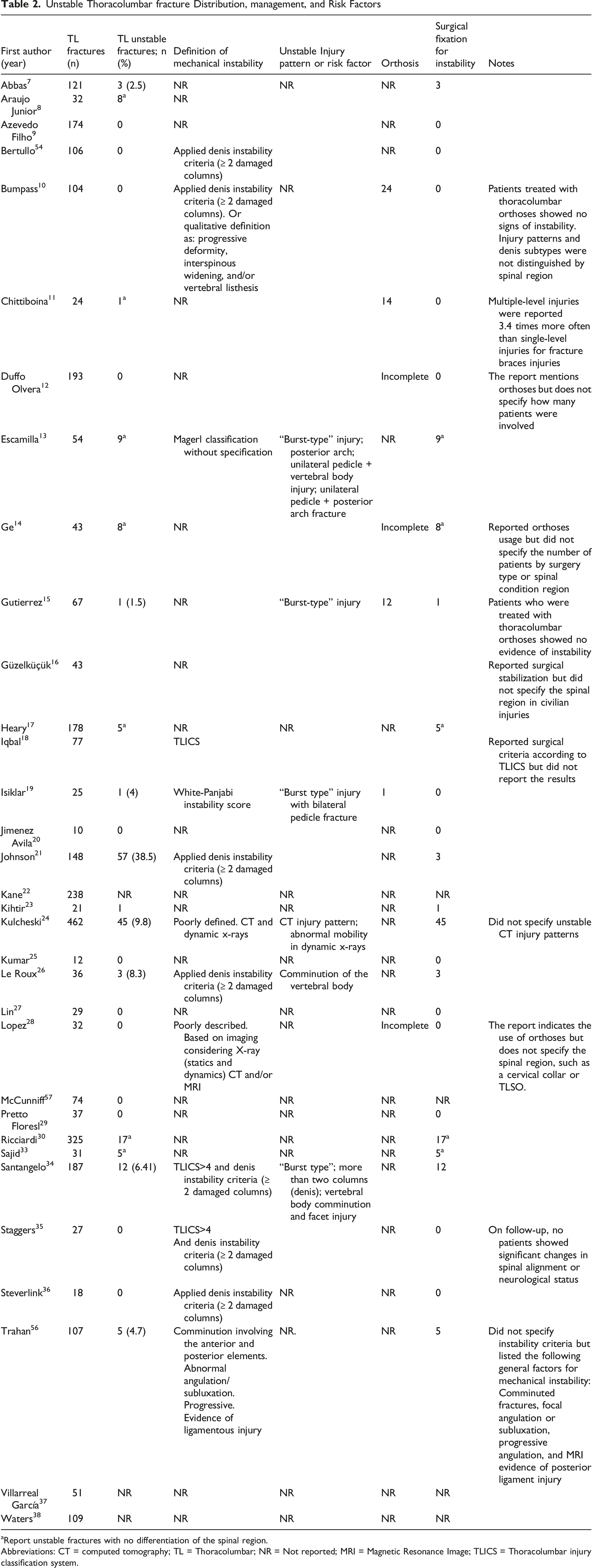
aReport unstable fractures with no differentiation of the spinal region.
Abbreviations: CT = computed tomography; TL = Thoracolumbar; NR = Not reported; MRI = Magnetic Resonance Image; TLICS = Thoracolumbar injury classification system.
Although all referenced papers considered mechanical instability as a study variable or at least an essential criterion in treatment decision-making for spinal gunshot wounds, only 12 of the 33 studies documented definitions or criteria for mechanical instability. Of these 12, 10 classified mechanical instability according to a previously published spinal blunt trauma classification system. The most frequently reported systems were the Denis three-column spinal theory (n = 4),21,26,36,54 followed by the thoracolumbar injury classification system score >4 (n = 3),18,34,35 the White and Panjabi instability score (n = 1), 19 and the Magerl classification system (n = 1). 13 On the other hand, some articles inadequately described the criteria for instability, considering progressive deformity, vertebral listhesis, comminution, and evidence of ligamentous injury, either indirectly (e.g., interspinous widening) or directly (e.g., MRI).10,24,28,56 The majority of the studies accepted the notion that computed tomography imaging and static X-rays are the most effective methods for determining unstable injury patterns. Two studies suggested using dynamic X-rays as a complementary diagnostic method.24,28 However, the available evidence does not provide sufficient detail to clarify their role in this context. Specifically, patient selection criteria, safety concerns in the presence of retained projectiles, and the magnitude of angular or translational change that should be regarded as clinically significant remain undefined.
Unstable thoracolumbar fractures were documented in 21 articles.7,8,11,13-19,21-24,26,30,33,34,37,38,56 With the exception of Johnson et al. 21 injuries involving unstable thoracolumbar fractures accounted for less than 10% of the cases. Johnson et al reported a higher rate of unstable injuries according to the Denis classification; however, they did not stabilize these injuries according to this theory.
Unstable Injury Patterns
The most common risk factor for mechanical instability was the injury patterns involving severe comminution of the vertebral body,13,15,19,26,34,56 either in isolation or in conjunction with fractures of the posterior arch (pedicle or facet fractures).13,19,34 Some authors referred to this pattern as “burst-type” despite the lack of compressive force in the injury mechanism. Evidence of ligament injury, whether indirect or direct (e.g., MRI), was also suggested as an instability factor.10,56 In cases where MRI is not feasible due to retained projectiles, ligamentous injury may be suspected through CT by reconstructing the projectile trajectory. However, this approach remains indirect and should be interpreted with caution.
Figure 4 describes four types of unstable injury patterns predominantly reported. Escamilla identified 3 patterns of unstable fractures.
13
The most frequent was comminution of the vertebral body (n = 12; 24.5%), followed by fractures involving the posterior elements. These included unilateral pedicle or facet fractures with associated vertebral body comminution (n = 6; 12.2%), and bilateral pedicle or facet fractures (n = 3; 6.1%). Isiklar et al reported a single case of bilateral pedicle fracture with vertebral body comminution as the only unstable pattern in their series.
19
Le Roux et al documented 3 patients (8.3%) who required surgery due to severe vertebral body comminution.
26
Santangelo et al. reported 12 patients treated for unstable patterns, including 4 with vertebral body comminution, 6 with involvement of two of the 3 Denis columns, and 1 with severe posterior arch comminution (unspecified).
34
Finally, Trahan et al described five patients treated for mechanical instability, applying broader criteria whereby instability should be suspected in comminuted fractures involving both anterior and posterior elements, particularly when associated with abnormal focal angulation, subluxation, or progressive deformity; MRI evidence of posterior ligamentous injury was also considered supportive. However, specific criteria were not detailed for each case.
56
Unilateral pedicle or facet fractures are generally considered stable in the literature. Fractures that involve the vertebral body and posterior wall, when not comminuted, are not regarded as inherently unstable.13,15,19,26,34,56 Schematic representation of the four basic patterns of unstable civilian thoracolumbar gunshot injuries. From left to right: (1) severe comminution of the vertebral body, (2) unilateral facet/pedicle fracture with associated vertebral body comminution, (3) bilateral facet/pedicle fracture, and (4) posterior ligament injury.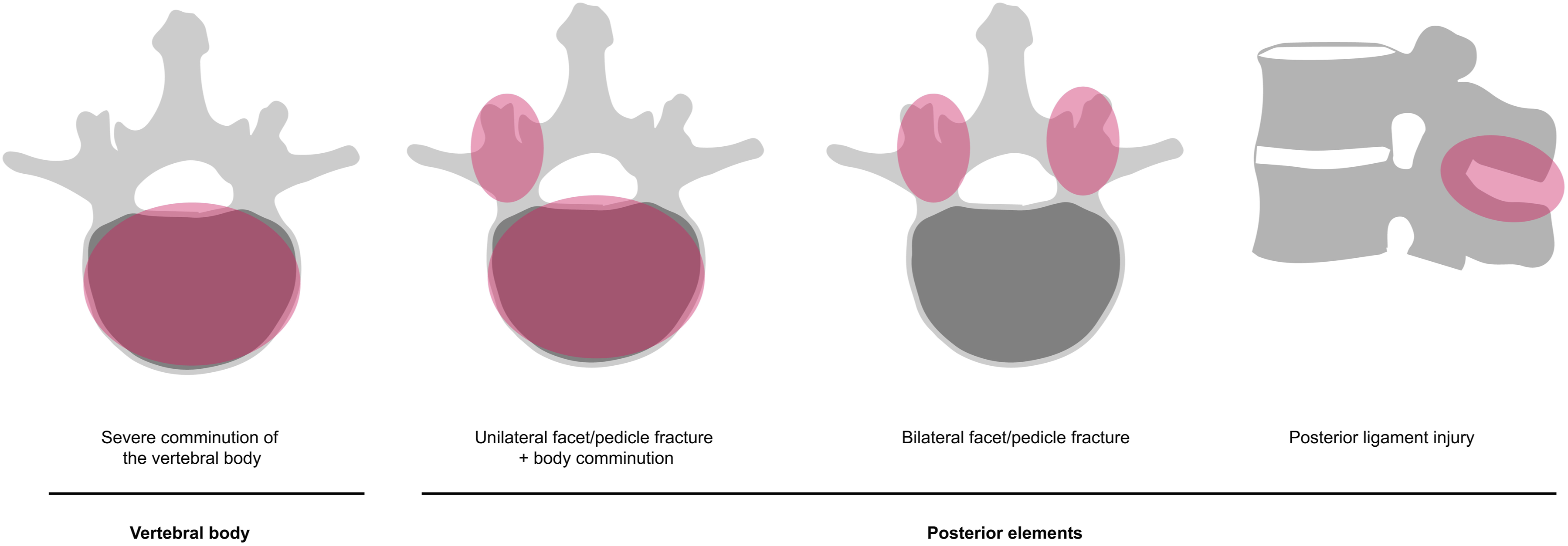
In this systematic review, it was not possible to specify operational thresholds for the four injury patterns, including the extent of vertebral body comminution, clinically meaningful cut-offs for kyphosis angle and translation, and the diagnostic standard for posterior ligamentous complex injury, because the retrieved literature did not provide sufficient or consistent data. This gap highlights a persistent clinical uncertainty that warrants further investigation. To address this issue, a future Delphi consensus study is planned, aiming to establish clinically relevant thresholds and standardized definitions.
Isolated non-structural and stable injury patterns were predominant, including structures such as the transverse process, spinous process, posterior arch, unilateral pedicle injury, and unilateral facet injury.
It is important to note that many of the studies included did not provide a comprehensive and accurate description of injury patterns. Furthermore, some studies did not differentiate between spinal regions, which is a crucial factor in understanding the complexity of these injuries.
In the present review, surgical fixation for unstable mechanical injuries was infrequently indicated (1.5%-9.7%),7,13-15,17,21,23,24,26,30,33,34,56 nor the use of orthoses.10-12,14,15,19,28 However, existing literature lacks detail on variation in fixation or orthosis use based on spinal level, projectile path, ligament findings, or multilevel involvement. This highlights ongoing clinical uncertainty and the need for consensus criteria to guide future practice. The distribution, management, and risk factors for unstable thoracolumbar fractures are summarized in Table 2.
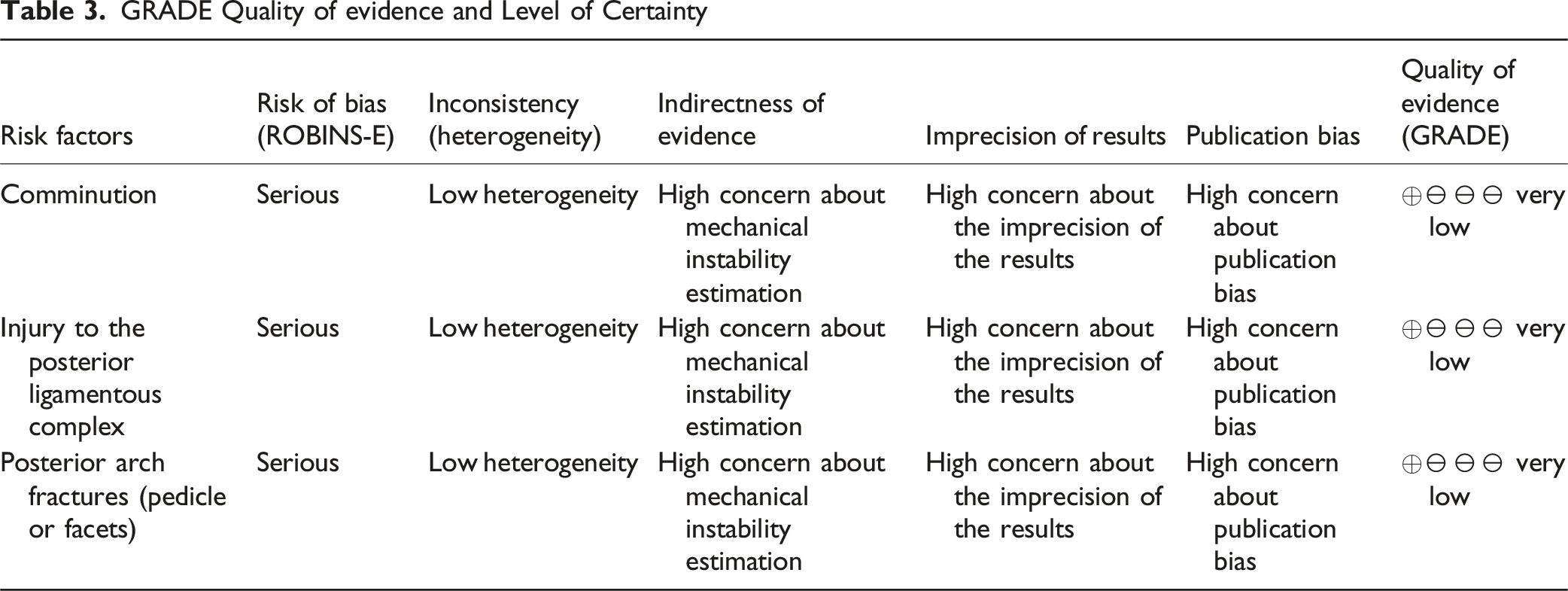
Certainty of Evidence
GRADE Quality of evidence and Level of Certainty
Discussion
Although gunshot wounds to the thoracolumbar spine share some similarities with blunt trauma, the unique biological and mechanical factors involved classify these patients as a distinct group. This difference necessitates a different approach in the initial decision-making process compared to patients with non-penetrating spinal injuries.
Unlike blunt trauma, spinal gunshot wounds are affected by ballistics, which include the type of firearm, the projectile’s trajectory, the bullet’s size and speed, and the distance from the firearm to the target. These factors influence the severity of the trauma and the extent of damage to bones and soft tissues through various mechanisms such as direct impact, cavitation, shock wave effects, and fragmentation and migration of the bullet.1-3
It is widely accepted that the injury mechanisms from gunshot wounds are affected by the factors mentioned earlier. Low-velocity weapons mainly cause damage through direct impact, leading to a range of injuries from minor fractures to severe comminuted vertebral injuries or spinal cord transections. In contrast, high-velocity weapons create additional injury mechanisms, resulting in more complex tissue damage. Other critical biological factors include issues related to retained bullets (such as location, neurological compression, and toxicity), neurological prognosis (such as spinal cord transection), associated hollow viscous injury, and the primary focus of this review, vertebral column instability.1-3,7-53
Spinal gunshot wounds are generally considered stable injuries, although the literature inadequately assesses mechanical stability.7-30,33-38,54,56,57 Despite consensus among most studies that mechanical instability is essential in deciding treatment, our systematic review, which included 33 studies involving 3195 patients with thoracolumbar gunshot wounds, could not find a clear definition. Only 12 studies provided some criteria for assessing instability. Most of the included studies used previously established classification systems or frameworks, initially developed for blunt spinal fractures, a type of injury involving significantly different indirect forces, such as compression or flexion/distraction.13,18,19,21,26,34-36,54
The injury patterns of thoracolumbar gunshot wounds exhibit distinctive characteristics. For example, bilateral pedicle or facet fractures, such as those caused by a gunshot wound with a lateral projectile trajectory, are notably rare in cases of blunt trauma.13,19,34
Despite the lack of high-quality studies providing definitive insights into the risk factors for mechanical instability in civilian thoracolumbar gunshot fractures, we observed a clear tendency for specific injury patterns to be classified as unstable. These patterns often involve severe comminution of the vertebral body, which increases the risk of kyphosis, as well as injuries to the pedicle or the facets.13,15,19,26,34,56 Additionally, the evaluation of the posterior ligamentous complex through indirect computed tomography imaging has been emphasized.10,56 In cases of blunt trauma injuries, a significant kyphosis deformity resulting from compression failure of the anterior and middle columns should raise concerns about potential posterior ligament complex injuries. Conversely, in instances of penetrating trauma, it is crucial to consider the trajectory of the projectile. A straightforward vertebral body injury could potentially be accompanied by direct damage to the posterior ligament along the projectile’s path. 10
Importantly, previous efforts to classify spinal gunshot wounds have been documented, although they lacked validation and widespread dissemination.1,36 We believe that existing blunt trauma classifications are not effective for civilian thoracolumbar fractures, especially those that focus on the mechanism of injury, such as the Magerl/TLICS system (which classifies injuries as compression, distraction, or translation). Additionally, the Denis three-column model may not be applicable, as a projectile’s path can affect two columns without causing significant comminution or instability, unlike compression burst fractures. As evidence of this, many articles that consider Denis for classifying injuries show a discrepancy between the rate of fractures with injury to two or more columns and those stabilized due to mechanical instability.21,26,36,54
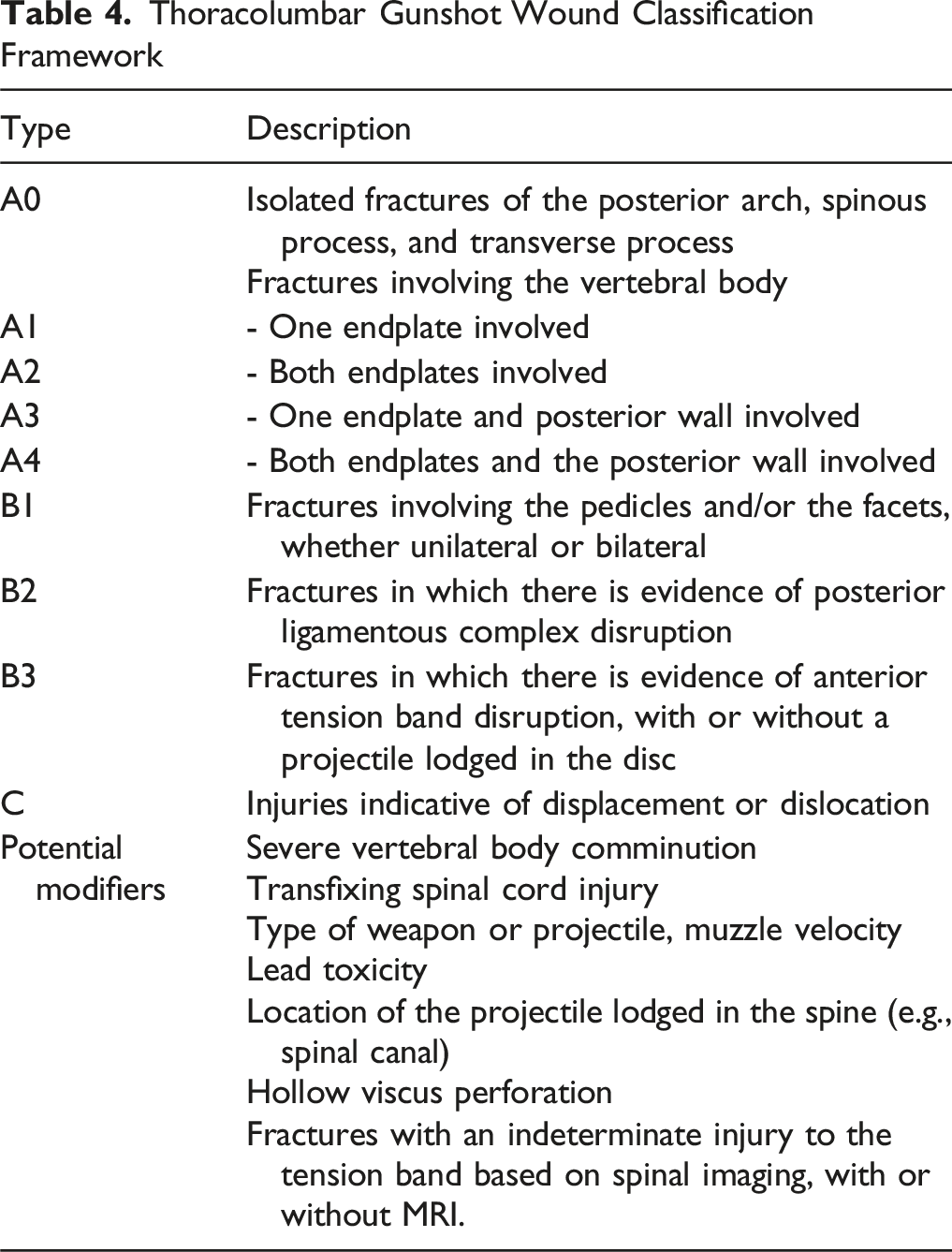
To develop a framework that effectively characterizes these injuries, we believe the AOSpine system is a suitable choice. This system emphasizes morphology, stability, and hierarchical organization and allows for the inclusion of clinical modifiers, providing a flexible platform for describing these specific injuries. Although the AOSpine system was originally designed for blunt trauma injuries, we hypothesize that the injury patterns associated with these cases may fit within its hierarchical structure.
To improve the classification system for civilian thoracolumbar spinal gunshot wounds, it is crucial to combine mechanical factors with biological and ballistic considerations. Possible modifiers to include are the amount of vertebral body comminution, the type of weapon or projectile, muzzle velocity, perforation of hollow viscera, bullet trajectory (especially transfixing injuries, which have the worst neurological prognosis), the location of the projectile lodged in the spine, and lead levels.
Thoracolumbar Gunshot Wound Classification Framework
The present study faces several limitations, primarily the variability among the included studies and the retrospective design of most of the evidence. The absence of a standardized definition of mechanical instability complicates direct comparisons and reduces the generalizability of the findings, similar to the high risk of bias in the included studies. Additionally, the use of single-center retrospective cohorts introduces selection and information bias. Formal interrater agreement (e.g., kappa) was not calculated. The inability to perform a meta-analysis due to clinical and methodological differences prevents a thorough quantitative synthesis, and the lack of long-term follow-up data limits the ability to make definitive treatment recommendations. Further research is needed to establish consensus and improve the best available evidence to develop a new classification system. We believe that standardizing according to the hierarchical structure of the AOSpine system would be a reasonable step toward achieving this goal.
Conclusions
Our review highlights a lack of clear definitions for unstable civilian gunshot injuries to the thoracolumbar region. Four recurring patterns were identified: severe vertebral body comminution, unilateral pedicle or facet fractures with vertebral body involvement, bilateral pedicle or facet fractures, and disruption of the posterior ligamentous complex. Vertebral body comminution was the most consistently reported feature indicating instability, although overall certainty remains very low. Due to significant heterogeneity and methodological limitations, definitive conclusions cannot be drawn. Future research should ideally focus on prospective, morphology-based cohorts with predefined instability criteria, standardized imaging, and blinded outcome assessment. As an alternative approach, structured consensus methods such as Delphi studies could utilize the patterns identified here to create a reproducible, evidence-informed classification system.
Supplemental Material
Supplemental Material - Mechanical Instability After Civilian Thoracolumbar Gunshot Injuries: A Systematic Review to Support Classification Development
Supplemental Material for Mechanical Instability After Civilian Thoracolumbar Gunshot Injuries: A Systematic Review to Support Classification Development by Guillermo Alejandro Ricciardi, Ignacio Cirillo, Juan Pablo Cabrera, Otávio Vitório Alvarenga Pereira, Emiliano Neves Vialle, Charles Carazzo, Michael Dittmar, Alfredo Guiroy, Ratko Yurac, Gregory D. Schroeder in Global Spine Journal.
Footnotes
Acknowledgement
This study was organized by the AO Spine Latin America Trauma Study Group. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through AO Spine Latin America regarding data collection, data analysis, and proofreading. The authors would like to thank Idaura Lobo and Carla Ricci (AO Spine) for their administrative assistance. The authors also extend their gratitude to all investigators and healthcare professionals involved in the management and study of spinal gunshot wounds, whose valuable contributions were essential to the completion of this research, including Dr. Jorge Cabrera Escamilla, Dr. Victor Davila, Dr. Sebastian de la Torre, Dr. Omar Hernandez, Dr. Cristobal Herrera Palacios, Dr. José María Jimenez Avila, Dr. Arturo Rodriguez Montalvo, Dr. Janicke Rodriguez, Dr. Alvaro Rocchietti, Dr. Luis Saavedra, Dr. David Servin, and Dr. Hugo Tejerina.
ORCID iDs
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.