
Abstract
Study Design:
Retrospective cohort study.
Objective:
As hospital compensation becomes increasingly dependent on pay-for-performance and bundled payment compensation models, hospitals seek to reduce costs and increase quality. To our knowledge, no reported data compare these measures between hospital settings for elective lumbar procedures. The study compares hospital-reported outcomes and costs for elective lumbar procedures performed at a tertiary hospital (TH) versus community hospitals (CH) within a single health care system.
Methods:
Retrospective review of a physician-maintained, prospectively collected database consisting of 1 TH and 4 CH for 3 common lumbar surgeries from 2015 to 2016. Patients undergoing primary elective microdiscectomy for disc herniation, laminectomy for spinal stenosis, and laminectomy with fusion for degenerative spondylolisthesis were included. Patients were excluded for traumatic, infectious, or malignant pathology. Comparing hospital settings, outcomes included length of stay (LOS), rates of 30-day readmissions, potentially preventable complications (PPC), and discharge to rehabilitation facility, and hospital costs.
Results:
A total of 892 patients (n = 217 microdiscectomies, n = 302 laminectomies, and n = 373 laminectomy fusions) were included. The TH served a younger patient population with fewer comorbid conditions and a higher proportion of African Americans. The TH performed more decompressions (P < .001) per level fused; the CH performed more interbody fusions (P = .007). Cost of performing microdiscectomy (P < .001) and laminectomy (P = .014) was significantly higher at the TH, but there was no significant difference for laminectomy with fusion. In a multivariable stepwise linear regression analysis, the TH was significantly more expensive for single-level microdiscectomy (P < .001) and laminectomy with single-level fusion (P < .001), but trended toward significance for laminectomy without fusion (P = .052). No difference existed for PPC or readmissions rate. Patients undergoing laminectomy without fusion were discharged to a facility more often at the TH (P = .019).
Conclusions:
We provide hospital-reported outcomes between a TH and CH. Significant differences in patient characteristics and surgical practices exist between surgical settings. Despite minimal differences in hospital-reported outcomes, the TH was significantly more expensive.
Keywords
Introduction
With increased emphasis on pay-for-performance and bundled payment compensation models, health care is shifting to value-based models. The value of health care is defined by the outcomes per dollar spent, 1 and hospitals seek ways to reduce costs while improving quality of care. A part of the Affordable Care Act, the Hospital Readmission Reduction Program, penalizes hospitals with higher than expected 30-day readmission rates. 2,3 Additionally, potentially preventable complications (PPC) were estimated to cost the United States $88 billion in 2006. 4 These metrics, in addition to hospital length of stay (LOS), have served as targets for hospitals to reduce costs and improve quality.
Extensive literature has presented such hospital-reported outcomes for 3 common lumbar spinal procedures: microdiscectomy, laminectomy, and laminectomy with fusion. 5 -17 Many of these studies used national administrative databases, and authors have cautioned the interpretation of the data because of coding errors and a variable patient population. 18 -20
Although previous research has focused on variations in spinal care according to the anatomic region, individual surgeon, and surgical approach, 18,19,21 little emphasis has been placed on the effect of the hospital setting. Krumholz et al 20 showed that hospital quality is correlated with outcomes by dividing hospitals into quartiles based on performance, demonstrating hospitals in the top quartile outperformed hospitals in the lowest quartile with regard to readmission risk. Fuller et al 22 also found that large tertiary hospitals have differences in payer mix and disease severity that can directly affect quality outcome measures.
We sought to investigate the differences in patient populations, hospital-reported outcomes, and costs associated with performing common lumbar surgeries at a tertiary hospital (TH) versus community hospitals (CH) within a single medical system. This information can help hospital systems optimize at-risk patient populations and serve as a benchmark to improve the quality and cost of care.
Materials and Methods
Patient Population
After obtaining approval from the institutional review board, we performed a retrospective review of prospectively collected data from a single medical system consisting of 1 TH (757 beds) and 4 CH (110-320 beds). The TH is in an urban US city, and the CH are in suburban settings within 10 to 70 miles of the TH. In general, tertiary referral centers are large, often academic, hospitals with full specialty and subspecialty services. Patients are often referred or transferred to these hospitals as they have the resources to care for patients of higher acuity and those with more comorbid conditions. Community hospitals are usually stand-alone hospitals with the primary aim to care for local patients, but lack resources to care for highly complex patients and do not have as many readily available subspecialty services. Community hospitals often refer complex patients to tertiary referral centers. 22 Eight orthopedic spine surgeons (TH, n = 4; CH, n = 4) and 10 neurosurgeons (TH, n = 2; CH, n = 8) performed 3 common primary, elective lumbar procedures between January 1, 2015 and January 1, 2016. Surgeon experience ranged from 6 to 33 years.
The treating surgeon prospectively identified adult patients (18-90 years of age) undergoing elective lumbar microdiscectomy for disc herniation, laminectomy without fusion for spinal stenosis, and laminectomy with fusion for degenerative spondylolisthesis. Patients with incomplete hospital records, nonlumbar spine pathology, nonprimary lumbar surgery, or traumatic, infectious, or malignant lumbar pathology were excluded from the study. For patients undergoing laminectomy with fusion, all procedures were performed via a posterior midline incision, and no patients undergoing anterior lumbar interbody fusion were included in the study.
Data Collection and Outcome Measures
The treating surgeon determined whether patients met the inclusion and exclusion criteria and manually entered specific surgical details into the physician-maintained prospective database. In addition to surgical variables, patient characteristics were analyzed according to hospital location (TH vs CH): age, sex, race, primary insurance provider, comorbid conditions, surgeon specialty (orthopedic spine vs neurosurgery), and surgery performed as an inpatient versus outpatient procedure (for microdiscectomy and laminectomy only). Preoperative comorbid conditions included cardiac (congestive heart failure or coronary artery disease), pulmonary (chronic obstructive pulmonary disease), renal (chronic kidney disease and renal failure), diabetes, hypertension, smoking status, and obesity (body mass index ≥30 kg/m2). The All-Patient Refined Diagnosis-Related Groups severity of illness score (lowest severity = 1, highest severity = 4) was recorded. 23,24 This score has been used in multiple studies to estimate disease severity. 9,17,23,24
Stratified by surgical procedure and hospital setting, outcome measures included baseline patient and surgical characteristics, in-hospital LOS, the rates of PPC and readmissions, discharge disposition to home versus a facility (inpatient rehabilitation or skilled nursing facility), and hospital costs. Costs between the TH and CH were defined as the primary outcome measure. With 3M PPC Grouping Software (2015; Salt Lake City, UT), we used discharge coding to identify conditions not present on admission that were potentially preventable based on interrelationships between patient comorbidities at the time of admission, the reason for admission, the severity of the patient’s illness, and procedures performed. 25 Each identified PPC was confirmed by the treating surgeon. Readmission rates included 30-day all-cause, all-payer readmissions to the same hospital at which the index surgery had been performed. The logic follows the same algorithm as the Centers for Medicare and Medicaid Services (CMS) all-condition, hospital-wide readmission measure but includes all payers. 26
Hospital costs, rather than charges, were obtained from the billing database from a single medical system for single-level microdiscectomy, 1- or 2-level laminectomy, and laminectomy with single-level fusion. Costs were reported for the following: total, drug, laboratory, operating room, imaging, patient room, supply (including implant), therapy (physical and occupational), and intraoperative neurophysiological monitoring costs. The various cost categories were derived directly from our billing database, which is consistent across all hospitals within our single medical system. Items or services are billed according to similar “charge buckets” for each hospital in the medical system, creating consistency in billing. This itemized list of supplies and services are then billed to the patient’s insurance payer as charges. Payment to the hospital from the insurance payer is defined as the cost of an item or service. The operating room costs were further broken down into labor, supply, and fixed costs. The fixed costs are those related to the infrastructure and overhead to run the facility where the procedure was performed.
Statistical Analysis
Descriptive statistical analysis was performed for patient characteristics and surgical data. Independent-sample t tests were calculated for continuous variables, and chi-square and Fisher’s exact tests were calculated for categorical variables. Then we performed univariate and multivariable stepwise linear regression models for cost data to adjust for patient characteristics, including age, sex, race, comorbid conditions, insurance, surgeon specialty, surgical factors, and discharge disposition. All independent variables that could have affected cost were included in the univariate analysis. Variables with a P value of .20 or less were then included in the multivariable stepwise linear regression analysis. Using an alpha error of 0.20, variables at or below this level of significance were included in the multivariable stepwise linear regression model using stepwise elimination. All statistical analyses were performed using SPSS version 22.0 (IBM Corp, Armonk, NY, USA). An alpha error of 5% was used as a cutoff to determine statistical significance.
Results
A total of 217 (TH, n = 49; CH, n = 168) patients underwent microdiscectomy for disc herniation, 302 (TH, n = 89; CH, n = 213) underwent laminectomy for spinal stenosis, and 373 (TH, n = 83; CH, n = 290) underwent laminectomy with fusion for degenerative spondylolisthesis. Significant differences in patient characteristics and operative variables were observed between hospital settings (Table 1).
Characteristics of Patients Undergoing Elective Lumbar Procedures at Tertiary and Community Hospitals.a
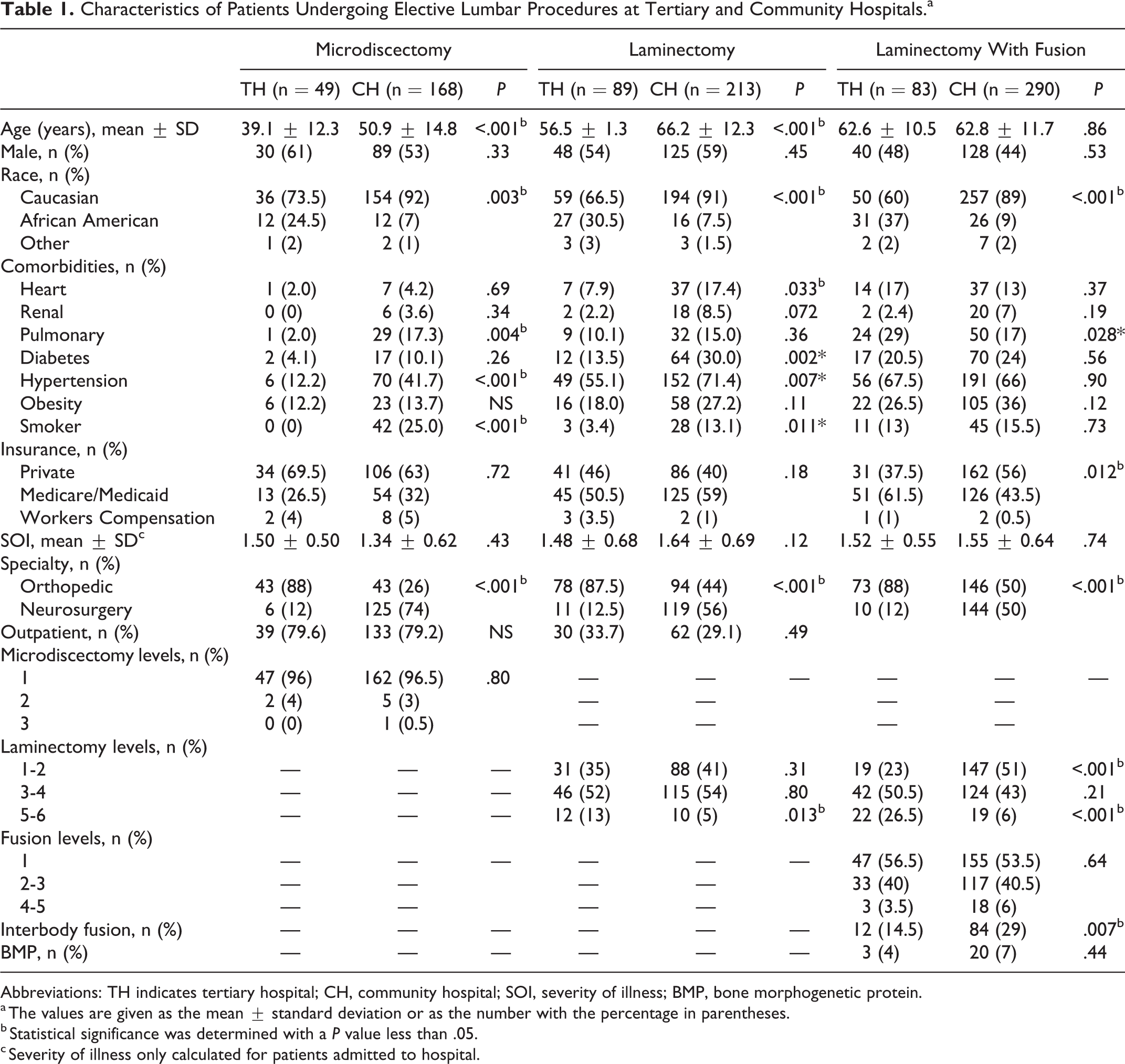
Abbreviations: TH indicates tertiary hospital; CH, community hospital; SOI, severity of illness; BMP, bone morphogenetic protein.
a The values are given as the mean ± standard deviation or as the number with the percentage in parentheses.
b Statistical significance was determined with a P value less than .05.
c Severity of illness only calculated for patients admitted to hospital.
The TH had significantly longer LOS for laminectomy with (P < .001) and without (P = .001) fusion (Table 2). No difference in PPC or readmission rates existed between hospital settings (Table 2). Patients undergoing laminectomy without fusion at the TH were significantly more likely to be discharged to a facility (P = .019; Table 3).
Outcomes of Elective Lumbar Procedures at Tertiary and Community Hospitals.a
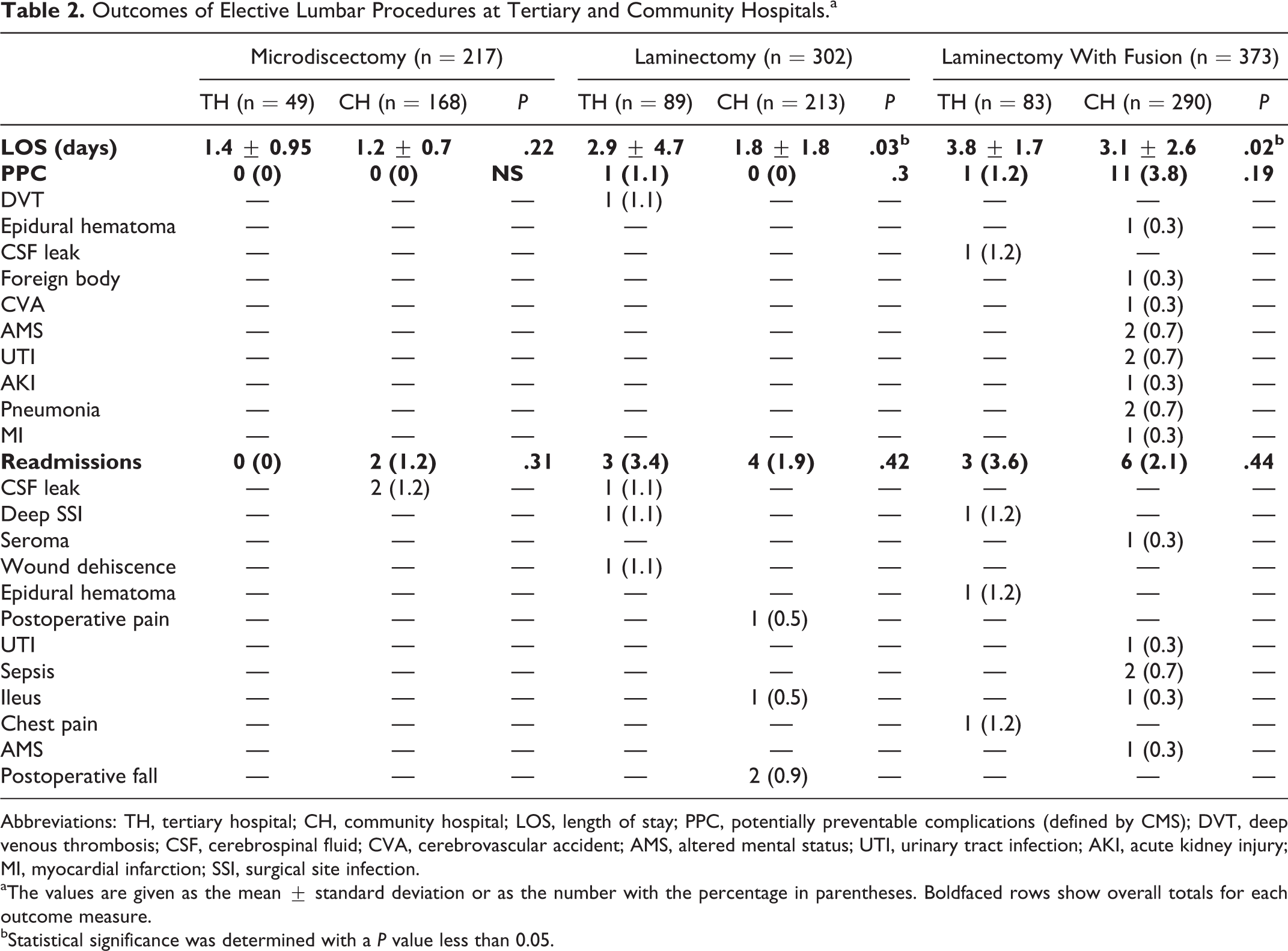
Abbreviations: TH, tertiary hospital; CH, community hospital; LOS, length of stay; PPC, potentially preventable complications (defined by CMS); DVT, deep venous thrombosis; CSF, cerebrospinal fluid; CVA, cerebrovascular accident; AMS, altered mental status; UTI, urinary tract infection; AKI, acute kidney injury; MI, myocardial infarction; SSI, surgical site infection.
aThe values are given as the mean ± standard deviation or as the number with the percentage in parentheses. Boldfaced rows show overall totals for each outcome measure.
bStatistical significance was determined with a P value less than 0.05.
Discharge Disposition for Elective Lumbar Procedures at Tertiary and Community Hospitals.
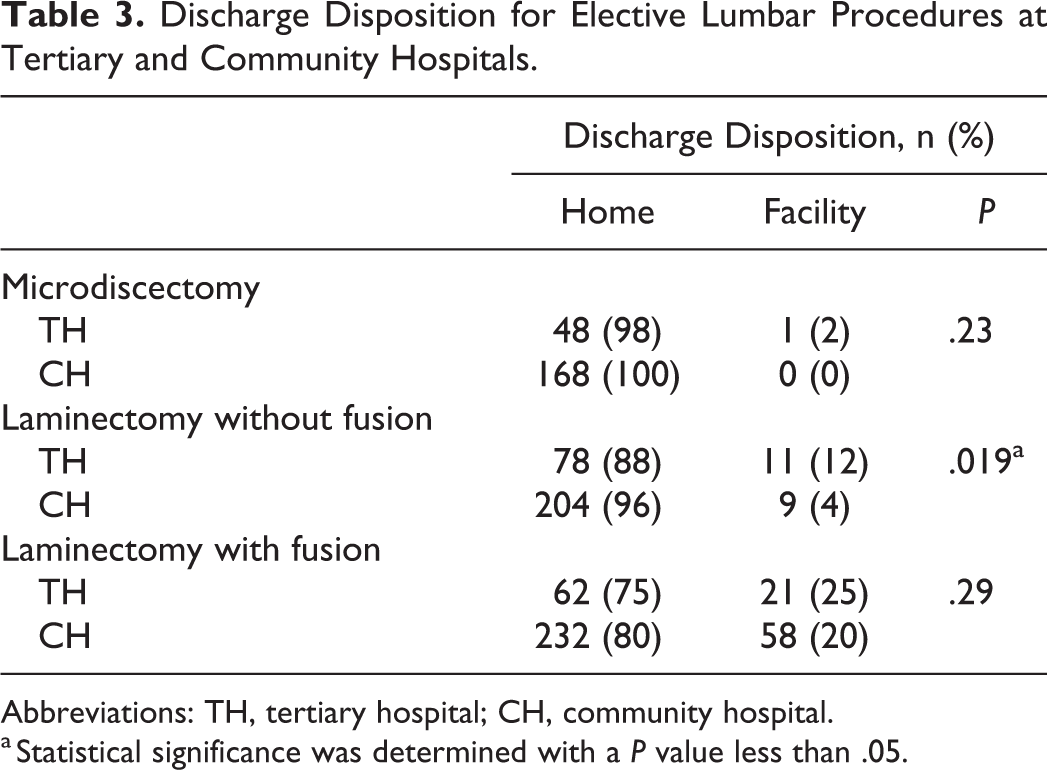
Abbreviations: TH, tertiary hospital; CH, community hospital.
a Statistical significance was determined with a P value less than .05.
The total cost of undergoing a single-level microdiscectomy was significantly higher at the TH (US$9707.83 ± 4012.57) versus the CH (US$4961.34 ± 2701.09; P < 0.001), as was the cost of undergoing a 1- or 2-level laminectomy at the TH (US$18 511.89 ± 16 084.36) versus the CH (US$10 173.41 ± 11 048.43; P = 0.014) before controlling for covariates (Table 4). The total cost of undergoing a one-level fusion with variable level decompression was not significantly higher at the TH (US$35 705.99 ± 10 032.02) versus the CH (US$32 547.73 ± 12 899.32; P = 0.094) before controlling for covariates (Table 4). Table 5 shows the univariate predictors of increased total costs for the 3 lumbar procedures. After adjusting for univariate factors, undergoing a microdiscectomy (P < .001) or laminectomy with fusion (P < .001) at the TH was significantly more expensive, while undergoing a laminectomy without fusion trended toward significance (P = .052; Table 6). The appendix (available online) shows the baseline patient characteristics for patients included in the cost analysis.
Cost (USD) of Elective Lumbar Procedures at Tertiary and Community Hospitals.a
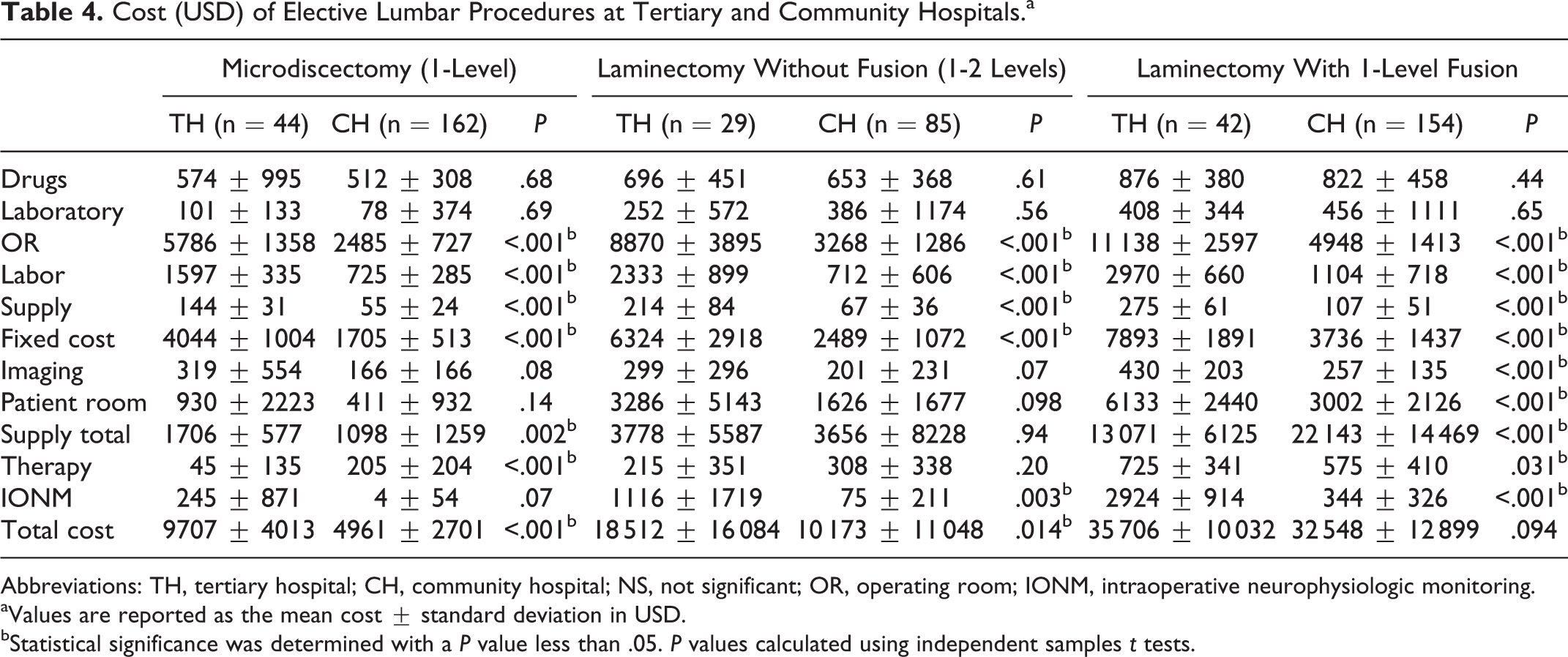
Abbreviations: TH, tertiary hospital; CH, community hospital; NS, not significant; OR, operating room; IONM, intraoperative neurophysiologic monitoring.
aValues are reported as the mean cost ± standard deviation in USD.
bStatistical significance was determined with a P value less than .05. P values calculated using independent samples t tests.
Univariate Analysis for Predictors of Total Cost for Elective Lumbar Procedures in USD.
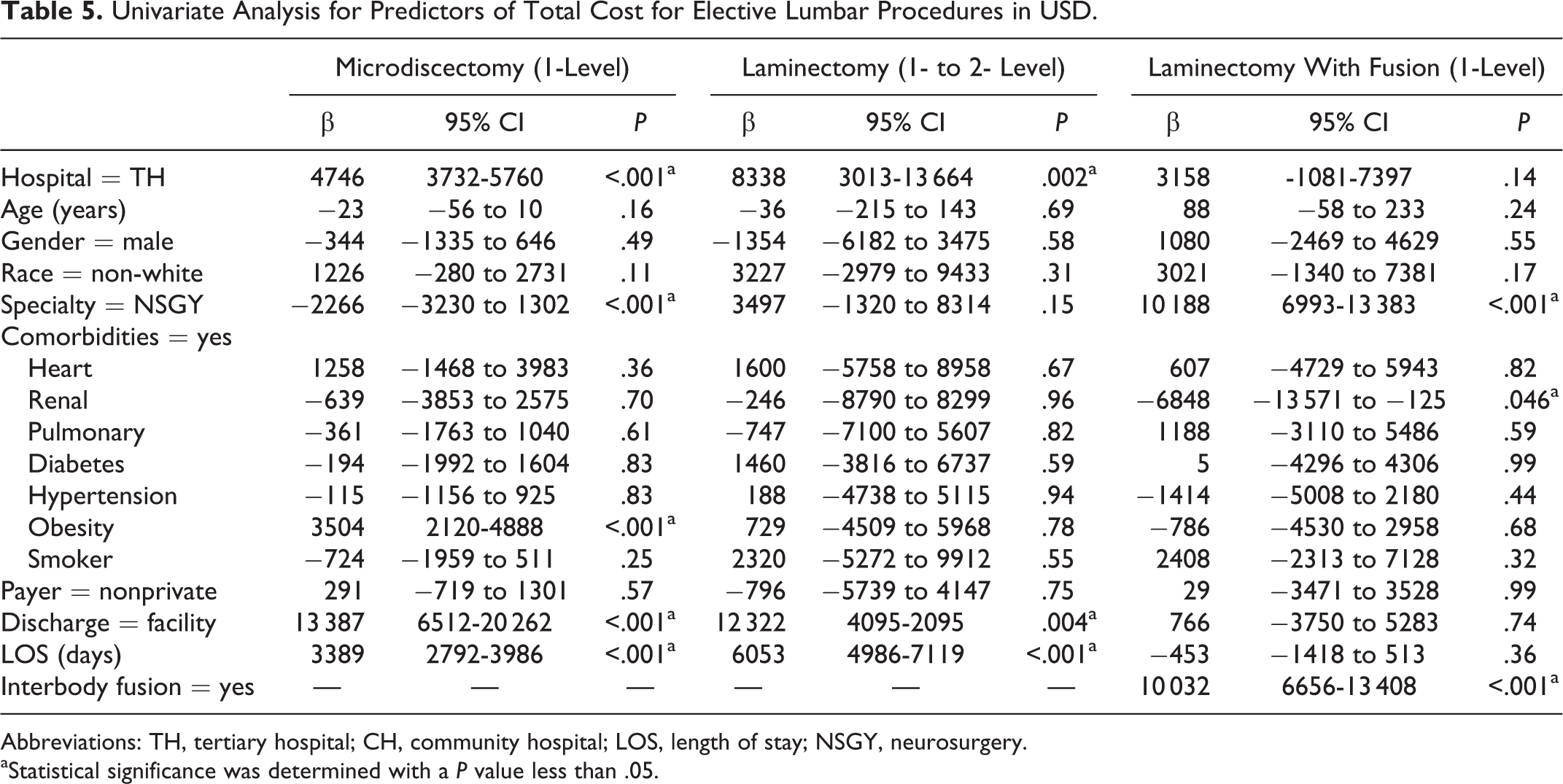
Abbreviations: TH, tertiary hospital; CH, community hospital; LOS, length of stay; NSGY, neurosurgery.
aStatistical significance was determined with a P value less than .05.
Multivariable Stepwise Linear Regression Analysis for Total Cost of Elective Lumbar Procedures in USD.a
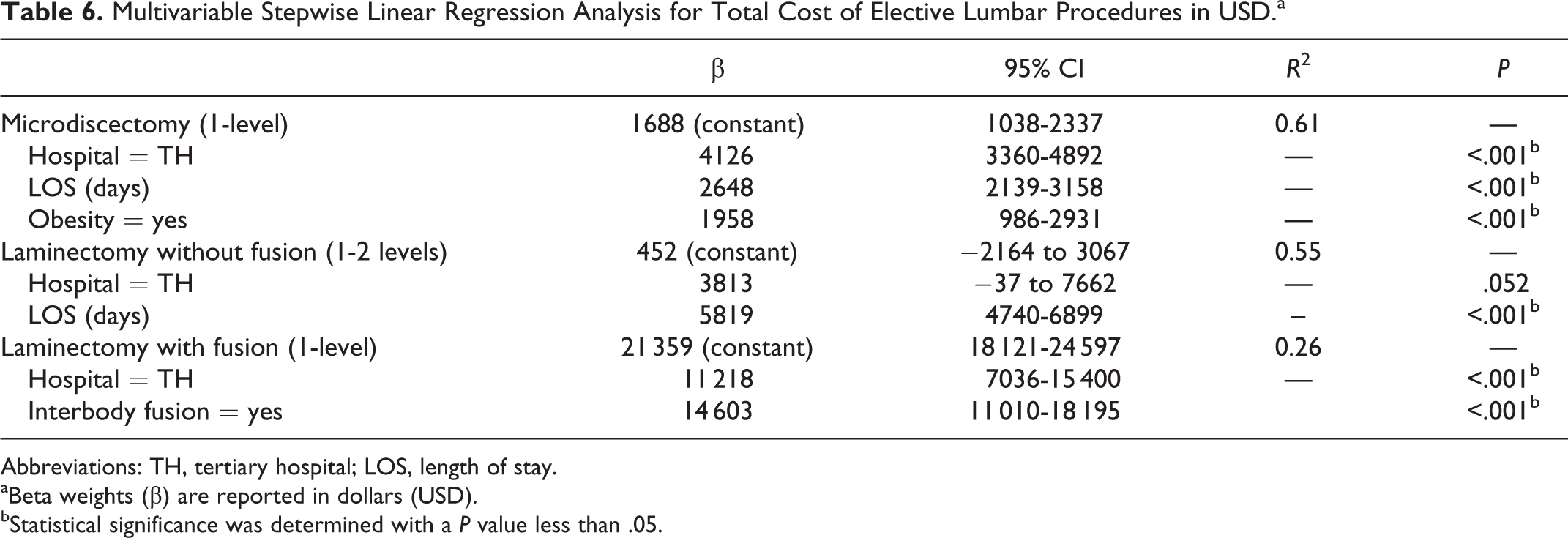
Abbreviations: TH, tertiary hospital; LOS, length of stay.
aBeta weights (β) are reported in dollars (USD).
bStatistical significance was determined with a P value less than .05.
Discussion
With increased emphasis on health care value, we aimed to evaluate differences between hospital settings in which primary, elective lumbar spinal procedures are performed. Most of the hospital-reported outcomes for 3 elective lumbar spinal procedures (microdiscectomy, laminectomy, and laminectomy with fusion) were not significantly different when comparing a TH and CH, but the costs of the procedures were significantly higher at the TH.
The patient population and surgical factors significantly differed between hospital settings. The TH generally served a younger patient population with a higher proportion of African Americans and fewer comorbid conditions. Patients undergoing microdiscectomy and laminectomy procedures at the TH were, on average, 10 years younger than those undergoing procedures at the CH. This difference was not observed for patients undergoing laminectomy with fusion, possibly because of the natural history of degenerative spondylolisthesis. 27 Of note, patients undergoing laminectomy with fusion procedures had significantly more Medicare/Medicaid payers at the TH (61.5%) versus the CH (43.5%). Fuller et al 4 showed that Medicaid enrollees have a 25% greater likelihood of readmission compared with commercial enrollees. Additionally, Seicean et al 28 showed that African Americans undergoing laminectomy with or without fusion had more preoperative comorbidities, longer LOS, and greater odds of major complications and discharge with continued care. Interestingly, the TH seemed to have younger, healthier patients with similar disease severity, but patients undergoing laminectomy without fusion were discharged to a facility significantly more at the TH. We were not powered to determine predictors of discharge disposition, but further studies should examine this between hospital settings. Although socioeconomic factors were not significantly associated with hospital-reported outcomes in the present study, understanding the demographics between hospital settings can assist surgeons in optimizing at-risk patient populations to improve outcomes.
The number of microdiscectomy and laminectomy levels were similar between hospital settings, but the TH performed more decompressions for a given number of fusion levels and the CH performed more interbody fusions. Considering similar baseline patient characteristics, the observed differences in surgical technique for patients undergoing laminectomy with fusion may be due to spinal surgeon preferences and training background. Irwin et al 29 showed the greatest disagreement between orthopedic spine surgeons and neurosurgeons regarding the treatment of degenerative spondylolisthesis. Our results suggest, however, that variation exists between specialties and between surgical settings. For example, orthopedic spine surgeons performed interbody fusions more often at the CH versus the TH (37.7% vs 20.1%) and performed more multilevel decompressions at the TH. This shows the complexity of assessing hospital-reported outcomes, where systematic and individual choices affect outcomes and costs.
Overall, we showed minimal differences in hospital-reported outcomes between surgical settings. Prior literature has reported longer LOS and higher complication and readmission rates compared with the values in the present study (Table 2). 6,7,9,11,12,16,30 -32 The low complication and readmission rates in our study are largely due to coding according to the CMS provider preventable conditions and 30-day all-cause, all-payer readmissions to the same hospital. Since our study sought to determine the effect of hospital setting on these hospital-reported outcomes, which affect hospital reimbursement, our complication and readmission rates may not reflect a fair comparison to values available in the literature. For example, cerebrospinal fluid (CSF) leaks are commonly noticed intraoperatively and are repaired. CSF leaks that are reportable to CMS are those that require a return to the operating room during the same hospital stay (a PPC) or those that would require a readmission and possible return to the operating room within 30 days (a readmission). Both events would significantly affect the cost of the perioperative course, and are reportable to CMS, affecting hospital reimbursement. Therefore, one would expect the complication and readmission rates to be lower than that reported in the literature.
With small differences in hospital-reported outcomes, the TH had significantly higher costs than the CH, even when controlling for covariates. To eliminate possible confounders in our cost analysis, we chose to compare only patients undergoing 1- or 2-level procedures. By shifting the TH patients to the CH setting, our medical system would have saved an average of US$4747 per single-level microdiscectomy, US$8338 per 1- or 2-level laminectomy, and US$3158 per multilevel laminectomy with single-level fusion for a total cost savings of US$583 308 (for 115 patients) during the year. The TH was more expensive by factors of 1.96 for microdiscectomy, 1.82 for laminectomy, and 1.10 for laminectomy with fusion. Surprisingly, the cost of performing an outpatient 1-level microdiscectomy at a TH (US$8050) was nearly equal to the cost of performing an inpatient microdiscectomy at a CH (US$8378). This shows that the TH provides more value for more invasive procedures, whereas the CH provide more value for the less invasive procedures. 1
Nearly all cost categories were significantly more expensive at the TH, but operating room costs contributed the most to the observed differences between surgical settings. The fixed costs associated with running a large tertiary referral center accounted for the largest proportion of the operating room costs, but labor and supply costs were also significantly higher at the TH. Length of surgery has been associated with increased operating room costs with lumbar surgery, but this variable was not evaluated in the present study. 33 The TH had significantly lower total supply costs compared with the CH (−US$9072) for laminectomy with fusion. The total supply costs include implant costs, and the observed cost difference likely reflects the higher use of interbody fusions in the CH setting. In addition to performing surgery at a TH, the use of interbody fusion was a significant predictor of increased costs for laminectomy with fusion procedures (Table 6). Regardless of the higher supply costs in the CH, the overall costs were significantly lower due to reduced fixed costs in other areas. The multivariable linear regression was less predictive of total costs between for laminectomy with fusion procedures, accounting for only 26% of the cost variability. This shows that factors outside the scope of our study likely contribute to increased costs, and further study should elucidate these variables. While the overall cost of performing a microdiscectomy or laminectomy without fusion was significantly greater at the TH on univariate analysis (Table 4), microdiscectomy and laminectomy with fusion were significantly more costly at the TH when controlling for covariates (P < .001; Table 6). The costs associated with performing a laminectomy without fusion at a TH trended toward significance (P = .052), but an increased LOS overshadowed the effect of the hospital setting. This is likely because laminectomy without fusion generally has a short LOS, as does microdiscectomy, and any increase in LOS strongly affects the perioperative costs of these procedures (P < .001). The TH had significantly longer LOS for patients undergoing laminectomy with and without fusion for the whole cohort, but only those undergoing fusion in the cost analysis had a significantly increase LOS (Table 2, appendix). Although previous studies have focused on the surgeon to reduce costs, 21,34 our study highlights significant hospital-level differences that the surgeon cannot directly control.
Our study had several limitations. Although it was a goal of the study to elucidate differences in patient and operative characteristics between surgical settings, conclusions for hospital-reported and cost outcomes should be made with caution. We controlled for such differences by performing multivariable stepwise linear regression models for cost data but were not powered to do so for categorical data. Propensity scores were considered but would have eliminated rare outcomes, such as readmission and complication rates. It is also possible that our readmission rates are understated considering that the hospitals in our medical system are surrounded by other medical systems where patients may have sought care. 4 Missing readmissions was minimized by encouraging patients to contact our call center if they experienced postoperative problems, and multiple hospitals in our medical system provided a larger catchment area for readmissions. Using multiple hospitals in our cost assessment increased the variability of how certain items were categorized, but this variability was reduced by analyzing information within a single medical system. Our medical system also provided cost rather than charge data, which is much more accurate and consistent between payers. Assessing the costs associated with complications, readmissions, and discharge to a facility was beyond the scope of the study and should be assessed in future studies.
To our knowledge, this is the first study to compare hospital-reported outcomes and costs at a large TH and CH within a single medical system for patients undergoing primary elective lumbar procedures. We found that the surgical settings served distinct patient populations with variable baseline patient characteristics. Minimal differences in hospital-reported outcomes existed, but the cost of performing any lumbar procedure was significantly higher at the TH. Larger, multicenter studies are needed to detect differences in complication and readmission rates and to evaluate patient-reported and functional outcomes.
Supplemental Material
Supplemental Material, GSJ848666_suppl_mat - Effect of Surgical Setting on Hospital-Reported Outcomes for Elective Lumbar Spinal Procedures: Tertiary Versus Community Hospitals
Supplemental Material, GSJ848666_suppl_mat for Effect of Surgical Setting on Hospital-Reported Outcomes for Elective Lumbar Spinal Procedures: Tertiary Versus Community Hospitals by Tristan B. Weir, Neil Sardesai, Julio J. Jauregui, Ehsan Jazini, Michael J. Sokolow, M. Farooq Usmani, Jael E. Camacho, Kelley E. Banagan, Eugene Y. Koh, Khalid H. Kurtom, Randy F. Davis, Daniel E. Gelb and Steven C. Ludwig in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Gelb is a board member and fellowship committee chair for AOSpine NA. He receives payment for lectures and for development of educational presentations from AOSpine NA. He receives royalties from DePuy Synthes Spine and Globus Medical. He has stock in the American Society for Investigative Pathology. Dr Koh receives payment for consultancy from Biomet. His institution receives RO1 grant money from the National Institutes of Health. Dr Ludwig is a board member for Globus Medical, the American Board of Orthopaedic Surgery, the American Orthopaedic Association, the Cervical Spine Research Society, and the Society for Minimally Invasive Spine Surgery. He is a paid consultant for DePuy Synthes, K2M, and Globus Medical. He receives payment for lectures and travel accommodations from DePuy Synthes and K2M. He receives payment for patents and royalties from DePuy Synthes and Globus Medical. He has stock in Innovative Surgical Designs and the American Society for Investigative Pathology. He receives research support from AO Spine North America Spine Fellowship support, Pacira Pharmaceutical, and AOA Omega Grant. He is a board member of Maryland Development Corporation. He receives royalties from Thieme, Quality Medical Publishers. He is on the governing board of Journal of Spinal Disorders and Techniques, The Spine Journal, and Contemporary Spine Surgery. The authors have no further potential conflicts of interest to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.