
Abstract
Study Design:
Retrospective case series.
Objective:
To describe the early implementation of an inpatient spinal surgery unit and measure the impact on cost and length of stay (LOS).
Methods:
A retrospective case review was performed for frequent spine-related diagnosis-related groups (DRGs) cared for by a dedicated multidisciplinary team: combined anterior/posterior (AP) spinal fusion with major complicating or comorbid condition (MCC), combined (AP) spinal fusion with CC, combined (AP) spinal fusion without complicating or comorbid (CC)/MCC, cervical spinal fusion with MCC, cervical spinal fusion with CC, and cervical spinal fusion without CC/MCC. Four time periods were compared: historical control, initial pathway implementation, full pathway implementation, and spine unit opening. Mean hospital LOS, mean and median total costs (USD), and ratio of costs-to-charges were analyzed.
Results:
The number of spine cases per interim ranged from 219 to 258. The mean overall hospital LOS and mean cost varied from 3.8 to 4.3 days for all DRGs across the time periods and was not significant. Cost also did not vary significantly throughout. Median variable cost per anterior/posterior spinal fusion procedure with a CC or MCC declined by 16 311, first with the institution of a spine pathway protocol by USD8738 and then USD7423 with the establishment of a spine care unit but did not reach significance.
Conclusions:
The use of a standardized, inpatient spine care pathway implemented by a multidisciplinary team may reduce the hospital length of stay and decrease overall costs.
Keywords
Introduction
The treatment of spinal disorders in the United States has been estimated to cost over 100 billion dollars annually, as of 2006 reports. 1 The multifactorial nature of low back pain (LBP) may be a contributing factor itself in tandem with its high point prevalence in the US population leading to widespread disparity in diagnostic workup as well as surgical and nonsurgical treatment measures. 2 A 2008 analysis by the US Congressional Budget Office found widespread regional variation in the per capita Medicare spending that could be attributed more to disparity in physician practice than regional variation in health care prices. 3 Recent high-quality randomized clinical trials evaluating the surgical utility of lumbar stenosis are inconclusive. 4,5 As such, the need for cost-saving strategies for the diagnosis and management of costly spinal disorders is growing.
Cost containment in the treatment of most spinal disorders has proven challenging. The movement to restructure medical care by grouping health professionals based on their common spine skillset to optimize and streamline care is underway. This so-called spinal care pathway can function in a variety of settings, both inpatient and outpatient. 6 More recently, spine-centered care pathways have seen increased development as a method for improving outcomes and cutting costs. 7 Another merit of pathways, particularly relevant to the diagnosis and treatment of spinal disorders, is in addressing the inconsistency between evidence-based practice guidelines and clinical practice. Recent reviews published in the literature found the majority of spine-related clinical pathways to be centered on the reduction of costs pertaining to the nebulous treatment of LBP, which can often carry high costs when straying from evidence-based guidelines. Moreover, the majority of studies lacks any quantifiable outcome measures studying the efficacy of spine pathways. 8
The authors perform a retrospective cost analysis of the implementation of a spine-centered pathway at a regional academic spine center to assess the impact of standardized spine care on inpatient elective and nonelective spine admissions and the impact on overall hospital costs and length of stay (LOS).
Methods
Clinical Care Pathway Formation
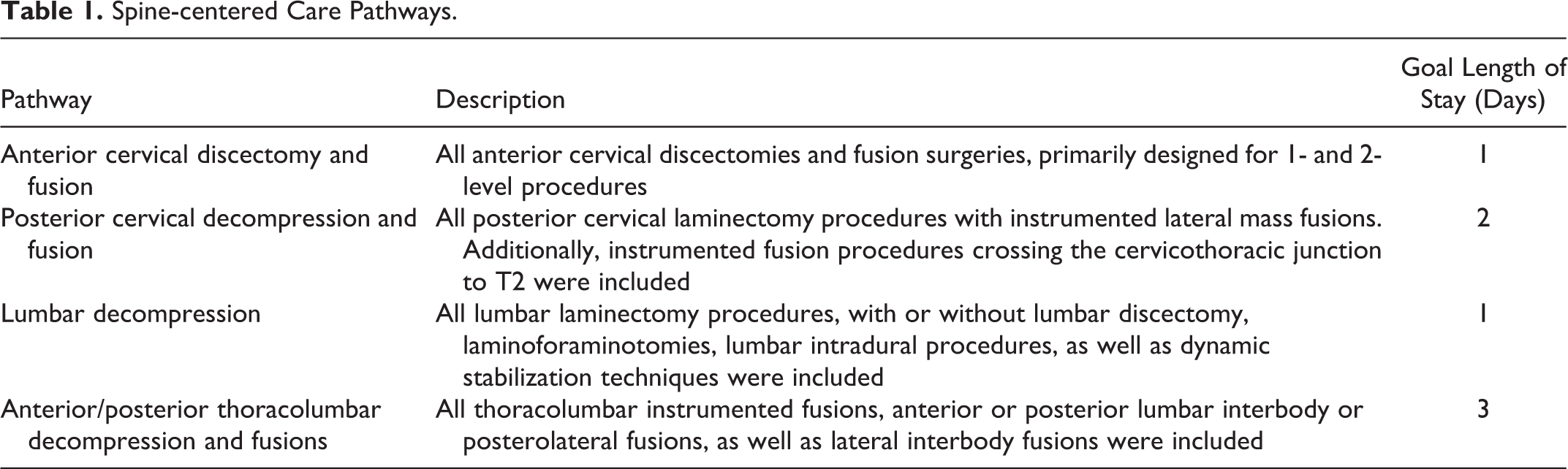
Clinical care pathways for the postoperative spinal surgery patient were created as a result of the collaboration among neurosurgical and orthopedic spinal surgeons, hospitalists, nursing staff, rehabilitation staff, unit managers, as well as hospital administrators so as to maximize efficiency and reduce redundancy of care. The overall goal was to standardize postoperative medical treatment such that consistency of care and communication was established among health providers. In addition to standardized postoperative order sets between the orthopedic and neurological surgeons, a 24-bed dedicated spine unit was created to centralize care of spine patients. Four clinical spine pathways were jointly developed based on the most common spine relevant surgical procedures performed with the overall goal to standardize both pre- and postoperative patient management (Table 1). These four common pathways initially addressed included the anterior cervical discectomy and fusion, posterior cervical decompression and fusion, lumbar decompression, and anterior/posterior thoracolumbar decompression and fusion. Each pathway contained key electronic orders designed to encourage early postoperative mobilization, aggressive physical therapy and early rehabilitation discharge, with the collective aim at limiting in patient postoperative morbidity.
Spine-centered Care Pathways.
Retrospective Review of Cases
A retrospective review was performed from October 1, 2014 through September 30, 2015 of an adult spinal surgery administrative database, with data collected at a single academic center. In an attempt to limit direct costs of rising United States health care, payments to hospitals from Medicare or an insurance company have utilized diagnosis-related groups (DRGs). Rather than a traditional aggregation of direct costs for inpatient care, payments were standardized for groups of diseases, and then further adjusted according to complicating and comorbid conditions. For this study, the following DRGs were queried for analysis: 453 combined anterior/posterior spinal fusion with major complicating or comorbid condition (MCC), 454 combined anterior/posterior spinal fusion with CC, 455 combined anterior/posterior spinal fusion without complicating or comorbid (CC)/MCC, 471 cervical spinal fusion with MCC, 472 cervical spinal fusion with CC, and 473 cervical spinal fusion without CC/MCC.
System-wide Spine-centered Pathway Implementation
With patient safety in mind, systematic changes were incrementally made to surgical spine patient care by 8 academic spine surgeons across the neurosurgery and orthopedic surgery departments at a single tertiary care institution. The spinal care pathway trial implementation period was designated from January 1 through March 31, 2015 and instituted as an electronic order set for postoperative patients. For the spine pathway order set, the above 4 general pathway choices were provided, with each subset of orders being designated for each general category of spinal procedures with a target number of days for each group (supplemental tables). The spine surgery pathway was officially online and designated for all spine patients on April 1; however, during the initial 3-month run-in period, patients were not admitted to a standardized spinal unit. The designated “Spine Unit” was established and opened on July 1. This unit is composed only of spinal patients, undergoing elective or nonelective surgery for traumatic, degenerative, deformity, infectious, or oncologic spine-related pathology. The purpose of this unit was to optimize patient care by designating a specialized team of nurses, physical therapists, occupational therapists and hospitalists, all familiar with the designated pathways as well as the care of spinal patients.
Outcomes
Four specific time periods (designated interims 1-4) were compared during this period. A baseline period prior to the use of pathways was designated as October 1, 2014 through December 31, 2014. This was followed by sequential 3-month intervals for the trial, full pathway implementation, and spine unit opening, with the dates for these intervals listed above. Mean hospital LOS, mean and median total costs (USD), and ratio of costs-to-charges were analyzed for each time period. These outcomes measures were analyzed for each aforementioned interim period for each spine DRG.
Statistical Analysis
Mean hospital LOS, total charges and total collections for the overall cohort, and DRG were compared. Means for each of the 6 individual procedures over the 4 time periods were analyzed using 1-way analysis of variance. Statistical analysis was performed using SAS version 9.4 (Cary, NC). A P value of .05 was designated as being statistically significant.
Results
The total number of spine cases were analyzed by DRG, for each of the 4 study periods, ranging from 219 to 258. Total case data overall and across the 6 individual DRGs was collected (Table 2). The mean overall hospital LOS and mean cost with establishment of spine unit were calculated, ranging from 3.8 to 4.3 days for all DRGs, and did not vary significantly (Table 3). Mean (Table 4) and median variable costs (Table 4) were analyzed by DRG during the 4 study periods.
Procedure Description and DRG Case Distribution.
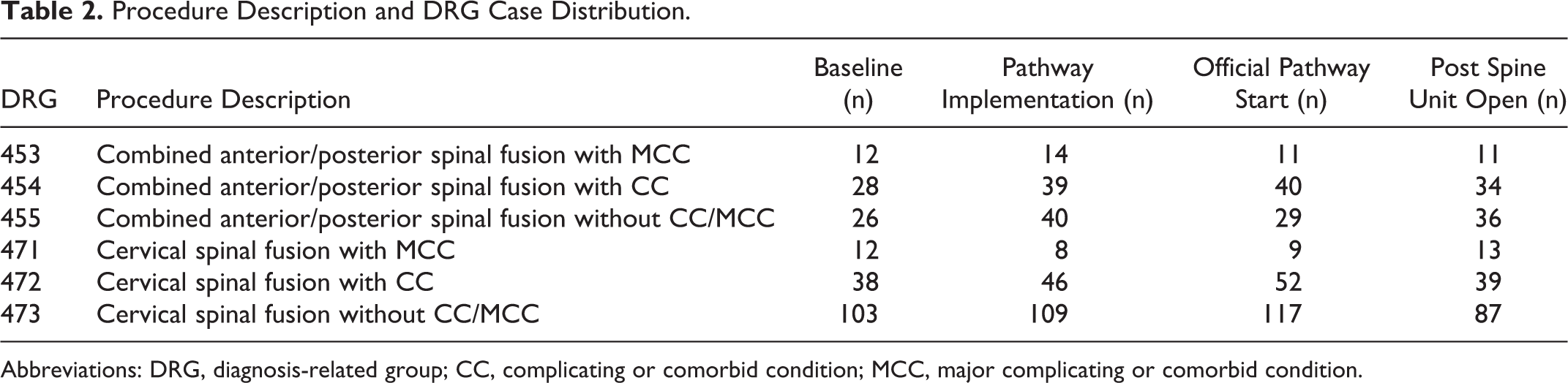
Abbreviations: DRG, diagnosis-related group; CC, complicating or comorbid condition; MCC, major complicating or comorbid condition.
Mean Overall Hospital Length of Stay and Mean Cost With Establishment of Spine Unit.
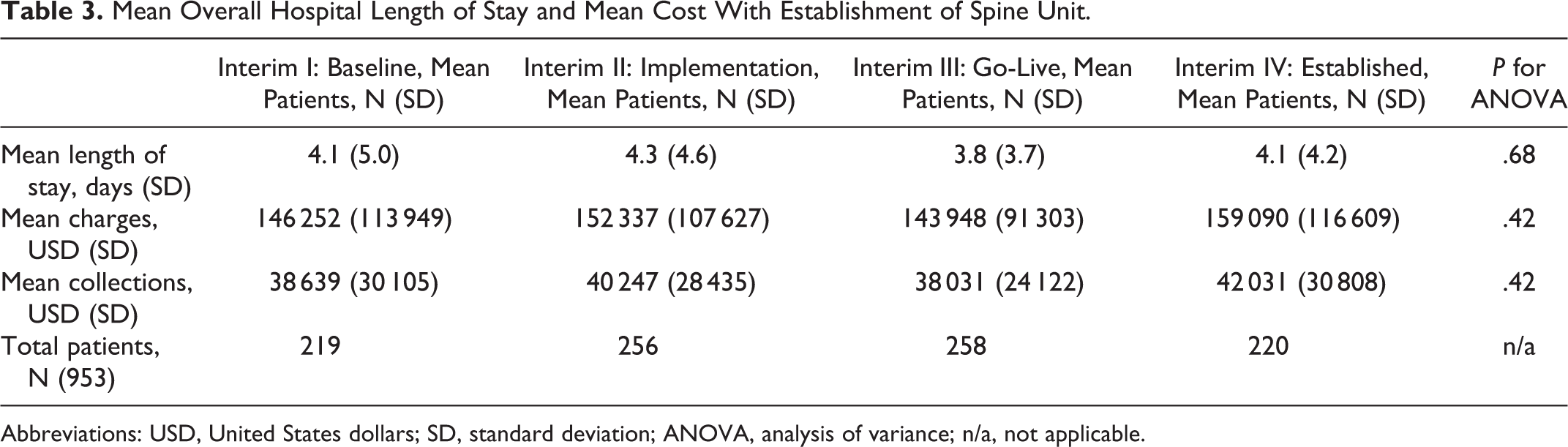
Abbreviations: USD, United States dollars; SD, standard deviation; ANOVA, analysis of variance; n/a, not applicable.
Hospital Length of Stay and Mean Cost by Procedure With Establishment of Spine Unit.
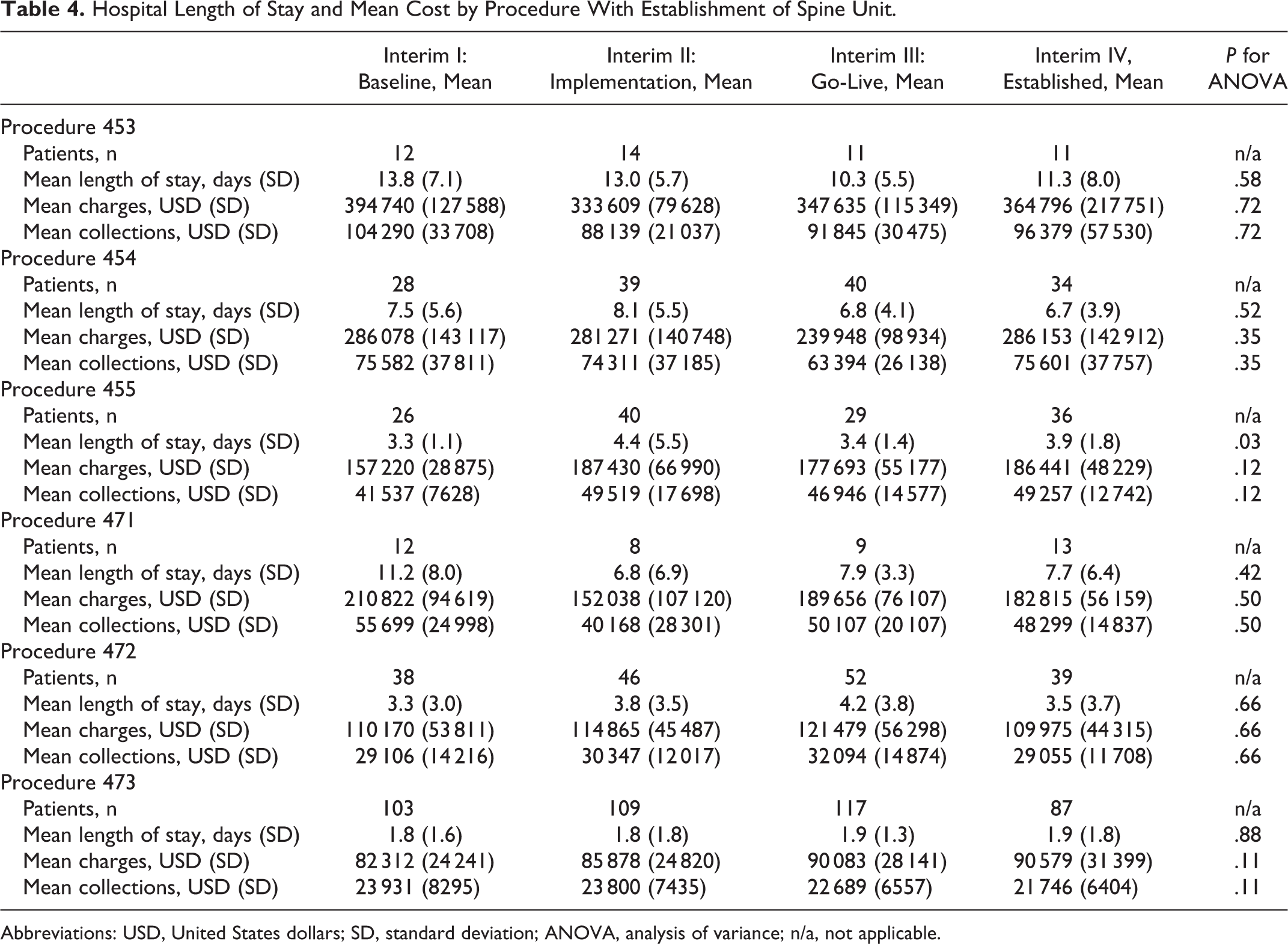
Abbreviations: USD, United States dollars; SD, standard deviation; ANOVA, analysis of variance; n/a, not applicable.
Cervical spine fusions without a CC or MCC were the least expensive on average, ranging from USD10 521 to USD11 492. Anterior/posterior spinal fusions with an MCC were the most expensive DRG with a baseline median variable cost of USD54 893. Overall, both average and median variable costs declined for all procedures with a CC or MCC but did not reach significance. The median variable cost of an anterior/posterior spinal fusion procedure with a CC or MCC declined by 16 311, first with the institution of a spine pathway protocol by USD8738 and then USD7423 with the establishment of a spine care unit (Table 4).
Discussion
Spine-centered pathway protocols, implemented at our institution, focused on streamlining the postoperative care of patients with the goal of lowering hospital LOS and costs. However, this present implementation failed to achieve a significant reduction in these measures (Tables 2 and 4). When analyzing the groups of patients by DRG, a positive relationship between surgical complexity and positive impact of the spine pathway is observed. When comparing the least complicated DRG analyzed, a cervical spine surgery without comorbidity to the most complex spine DRG, an anterior/posterior fusion with an MCC, the maximum benefit to the patient is observed through reduction in cost. Specifically, in the anteroposterior fusion group with an MCC, a 29.7% decline in median variable costs is observed. We hypothesize that this relationship relates to the fact that patients with more extensive procedures, are more aggressively mobilized earlier on postsurgery as compared with previous, leading to reduced length of stay and lower cost. This question among others will drive further studies of the impact of an organized inpatient spine pathway. This finding highlights the difficulty of interpreting retrospectively collected data, which did not account for unpredicted variation in changes in patient disease complexity and surgical costs. A more fruitful comparison might arise from prospectively analyzing direct costs in an effort to assess the cost-effectiveness of a spine surgery pathway.
Early ambulation has been shown to lead to improved outcomes in numerous studies across a range of orthopedic procedures. 9,10 Moreover, early ambulation has been correlated with decreased LOS, particularly in the elderly. 11,12 In all DRGs together, the average decline in LOS was 1 day, with up to a 2.5- to 3.5-day decline in the most complex patients with the use of a spine-centered pathway. This can be most likely attributed to the multidisciplinary team focus of early ambulation for all groups. Even with anterior/posterior thoracolumbar fusions patients are mobilized on the same day postoperatively. Then, on postoperative day 1, the patient then participates in rigorous physical therapy, ambulating out of bed.
Numerous studies have previously conceptualized spinal pathways with the goals of improving productivity and limited expense. 7,13 -16 Paskowski et al 7 have reported the use of spine pathways for the reduction in costs for LBP diagnosis and treatment. They do, however, lack any detailed analysis on the ability of these pathways to improve outcomes.
Limitations
The present study unfortunately is felt to lack the necessary data to demonstrate a significant reduction in LOS and either total costs or ratio of cost-to-charges. Furthermore, future study should correlate functional outcomes measures with the implementation of this spine service line. This is undoubtedly, the goal of future care in addition to lowering cost through the maximization of evidence-based therapies while minimizing the use of unsupported measures. 17 To the author’s knowledge, this is the first report in the literature detailing the successful incorporation of a spinal surgery-centered inpatient pathway and standardized postoperative care.
Conclusion
Although the current study did not show a significant decrease in overall cost, the use of a standardized, spine care pathway in the inpatient setting and implemented by a multidisciplinary team may reduce the hospital length of stay and decrease overall costs. Further study is required to determine the relative impact of specific care initiatives on postoperative outcomes as well as reducing procedural morbidity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was supported by funding from AO Spine North America.