
Abstract
Study Design:
Retrospective cohort study.
Objectives:
To investigate the feasibility of inserting pedicle screws in the proximal thoracic (PT) curve in Lenke type 2 idiopathic scoliosis, using post-myelography computed tomography (CT).
Methods:
Post-myelography CT images of 46 Japanese patients, 10 to 30 years old, who underwent surgery for Lenke type 2 idiopathic scoliosis were analyzed. A new parameter “SAPS” (space available for pedicle screw) was introduced, which defines the minimal distance between the lateral cortex of the pedicle and the spinal cord, with a SAPS <4.5 mm being “unacceptable.” All 460 pedicles (T2 through T6) were analyzed. Pedicle diameter was classified according to the Akazawa grading system.
Results:
Most pedicles on the right side at T3 (84.8%) and T4 (97.8%) were unacceptable. The unacceptable rate was 58.7% and 15.2% on the right side at T5 and T6, respectively. A larger Cobb angle of the PT curve was associated with a greater incidence of unacceptable SAPS at these levels. For a Cobb angle of the PT curve >40°, most right T5 pedicles were unacceptable. On the left side, most pedicles from T2 to T5 were acceptable. When T5 was the caudal end vertebra of the PT curve, the left T6 pedicles had an unacceptable SAPS in some cases. When the width of the pedicle channel was ≥2 mm (Akazawa grade 1 or 2), all pedicles from T2 to T6, on both sides, were acceptable.
Conclusions:
Post-myelography CT enabled us to clearly demonstrate the feasibility of inserting pedicle screws in the PT region.
Introduction
Segmental fixation surgery with pedicle screws is widely performed for patients with idiopathic scoliosis, although inserting screws into the pedicles of the rotated vertebrae has potential risk of spinal cord injury. In addition, asymmetrical pedicles and deviation of the spinal cord in the spinal canal in the scoliotic spine increase the difficulty of inserting pedicle screws safely. 1,2 In particular, inserting pedicle screws in the proximal thoracic (PT) region is challenging because pedicles in this region are anatomically narrow. 3 -5 Hence, special attention is needed when the PT curve is included in the area of fusion. However, the potential risk of spinal cord injury by inserting pedicle screws in the PT curve has yet to be fully clarified. Because the PT curve is usually involved in the fusion area in most patients with a Lenke type 2 idiopathic scoliosis, we investigated the safety of inserting pedicle screws in the PT curve of this scoliosis type, using post-myelography computed tomography (CT), which enabled us to accurately assess the relative positions of the pedicles and spinal cord. This study is novel in 2 aspects, being the first to evaluate the safety of inserting pedicle screws in the PT curve of scoliosis cases and the first to evaluate safety of inserting pedicle screws in cases with scoliosis using post-myelography CT.
Materials and Methods
Among 56 Japanese patients with a Lenke type 2 idiopathic scoliosis who underwent surgery between 2006 and 2016, the 46 patients who underwent post-myelography CT were included in this study. These patients were 10 to 30 years old. Post-myelography CT was obtained for the CT-based navigation surgery, with images obtained using a slice thickness of 1.25 mm. In all patients, myelography was performed within 3 months before surgery, and post-myelography CT was obtained approximately 30 minutes after myelography. In order to assess the safety of inserting pedicle screws into the pedicles, we introduced a new parameter, the “SAPS” (space available for pedicle screw), which was defined as the minimal distance between the lateral cortex of the pedicle and the spinal cord, assuming that the pedicle screw is inserted into this gap (Figure 1A). We defined an SAPS of <4.5 mm as being “unacceptable” as we typically use pedicle screws of 4.5 mm or more in diameter. For example, in Figure 1B, the left SAPS is 12.3 mm and is acceptable, while the right SAPS at 3.1 mm is unacceptable. Pedicle diameter was classified according to the Akazawa grading system, which classifies pedicle channels from grades 1 to 4 (≥4 mm, 2-4 mm, 1-2 mm, <1 mm, respectively) 6 (Figure 2). We analyzed all 460 pedicles from T2 to T6 vertebrae included in the surgeries for the 46 patients in our study group. The measurement was primarily conducted by one author (YT). As reliability analysis for the measurements of SAPS, 100 pedicles from 10 randomly selected patients out of the 46 patients were analyzed by 2 attending spine surgeons (YT and YM). Intraclass correlation coefficients (ICC) were calculated for verification of the interobserver reliability. Continuous variables were compared using a t test, with a χ2 test being used to compare categorical data. The threshold for significance was set at P < .05.
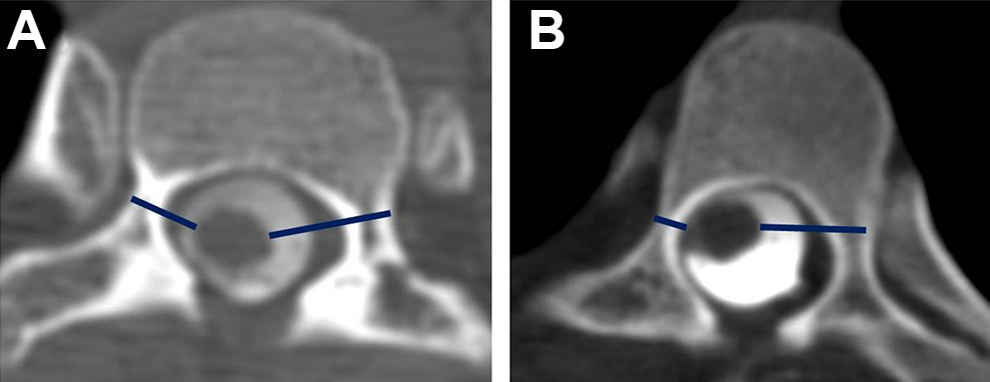
The definition of SAPS (space available for pedicle screw). (A) SAPS is defined as the minimal distance between the lateral cortex of the pedicle and the spinal cord on the post-myelography computed tomography (CT) image. (B) Post-myelography CT at the level of T3 in a 14-year-old girl showing that the right SAPS is 3.1 mm and is unacceptable, while the left SAPS is 12.3 mm and is acceptable.
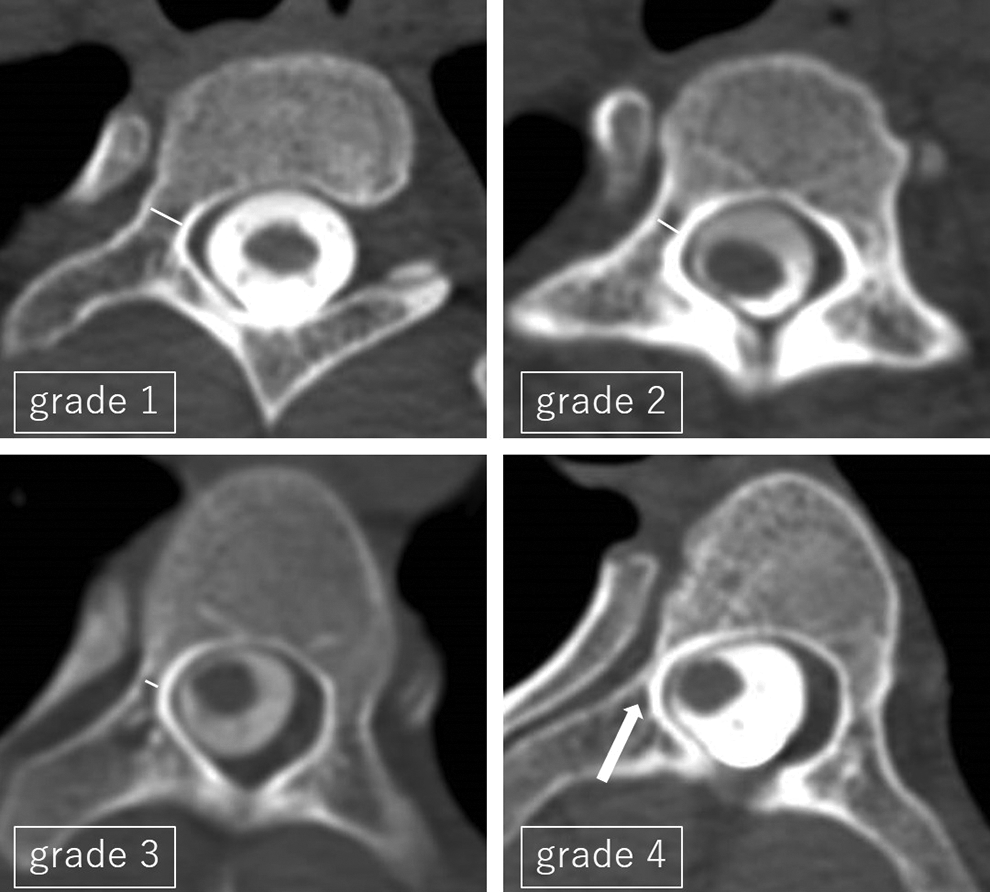
Akazawa grade classification for pedicle channels: grade 1, “large cancellous channel” with an inner diameter of ≥4 mm; grade 2, “moderate cancellous channel” with an inner diameter of ≥2 mm and <4 mm; grade 3, “small cancellous channel” with an inner diameter of ≥1 mm and <2 mm; grade 4, “cortical channel” with an inner diameter of <1 mm.
This study was approved by the research ethics committee of the University of Tokyo.
Results
Demographic data of the patients are shown in Table 1. Our study group included 37 females and 9 males, with the mean age of the study group being 16.1 ± 3.7 years. All PT curves were left curves and the main thoracic (MT) curves were right curves, with a mean Cobb angle of 37.1 ± 7.1° and 57.5 ± 8.8°, respectively. The caudal end vertebra of the PT curve was T5 in 15 patients, T6 in 26, and T7 in 5. The ICC value for the measurement of SAPS between 2 surgeons was 0.962, which confirmed high interobserver reliability.
Demographic Data.
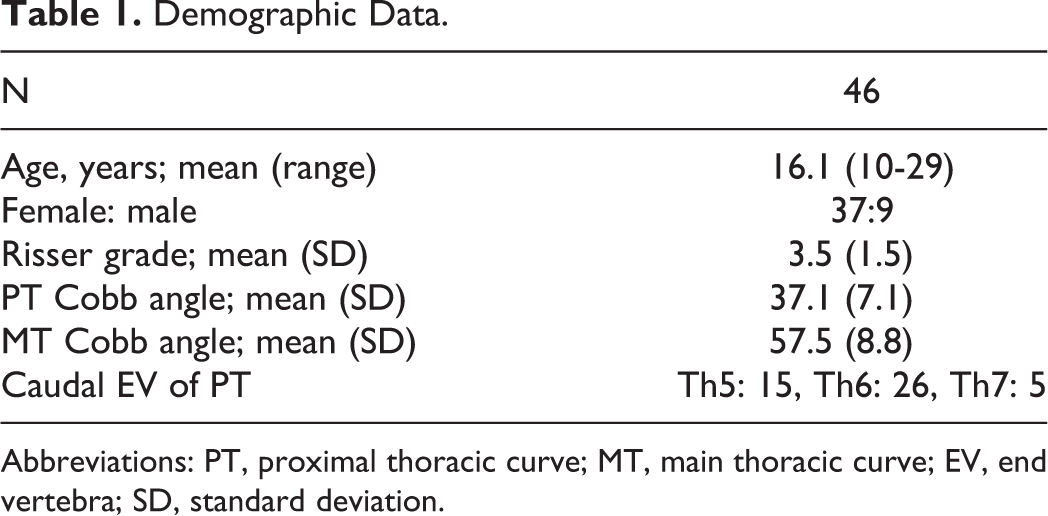
Abbreviations: PT, proximal thoracic curve; MT, main thoracic curve; EV, end vertebra; SD, standard deviation.
On the right side, the mean SAPS from the level T2 through to T6 was 6.9 mm, 3.3 mm, 2.7 mm, 4.5 mm, and 7.4 mm, respectively (Table 2). Most right pedicles at the level of T3 (84.8%) and T4 (97.8%) exhibited a SAPS <4.5 mm and were unacceptable, indicating that insertion of pedicle screws via transpedicular trajectory in the right T3 and T4 pedicles should be avoided in many cases (Table 2). Twenty-seven (58.7%) pedicles at the level of T5 and 7 (15.2%) at T6 were unacceptable (Table 2). For both right T5 and T6 pedicles, a larger Cobb angle of the PT curve was associated with unacceptable SAPS, which may have been due to a greater deviation of the spinal cord with a larger PT curve (Tables 3 and 4). More specifically, when the Cobb angle of the PT curve exceeded 40°, the SAPS of the right T5 pedicle was less than 4.5 mm in most cases (Figure 3). At all levels, from T2 to T6, unacceptable right pedicles, with a SAPS <4.5 mm, had Akazawa grade 3 or 4 pedicle channels (Table 2).
Right Pedicles.
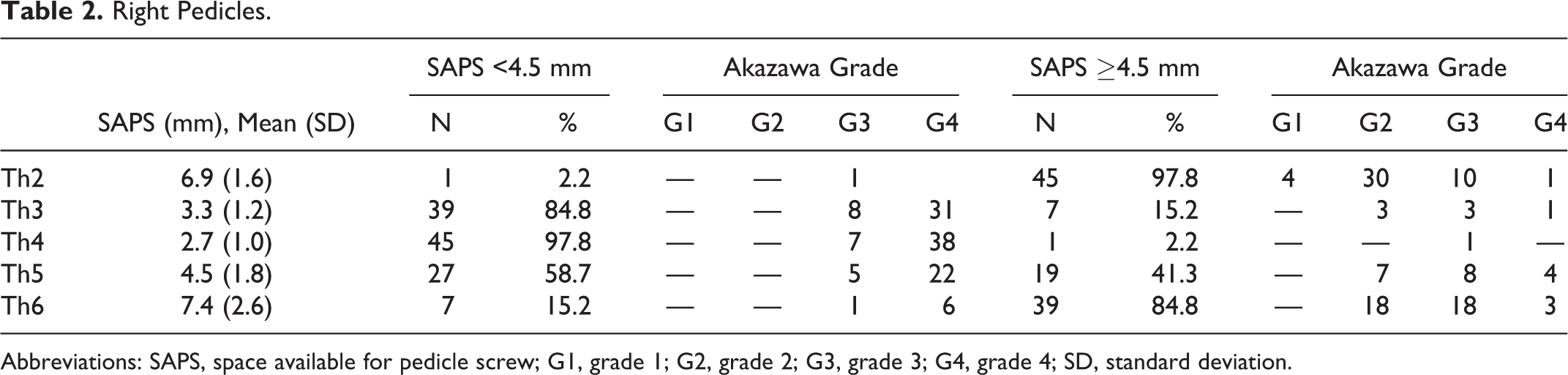
Abbreviations: SAPS, space available for pedicle screw; G1, grade 1; G2, grade 2; G3, grade 3; G4, grade 4; SD, standard deviation.
Findings of the Right Th5 Pedicle.
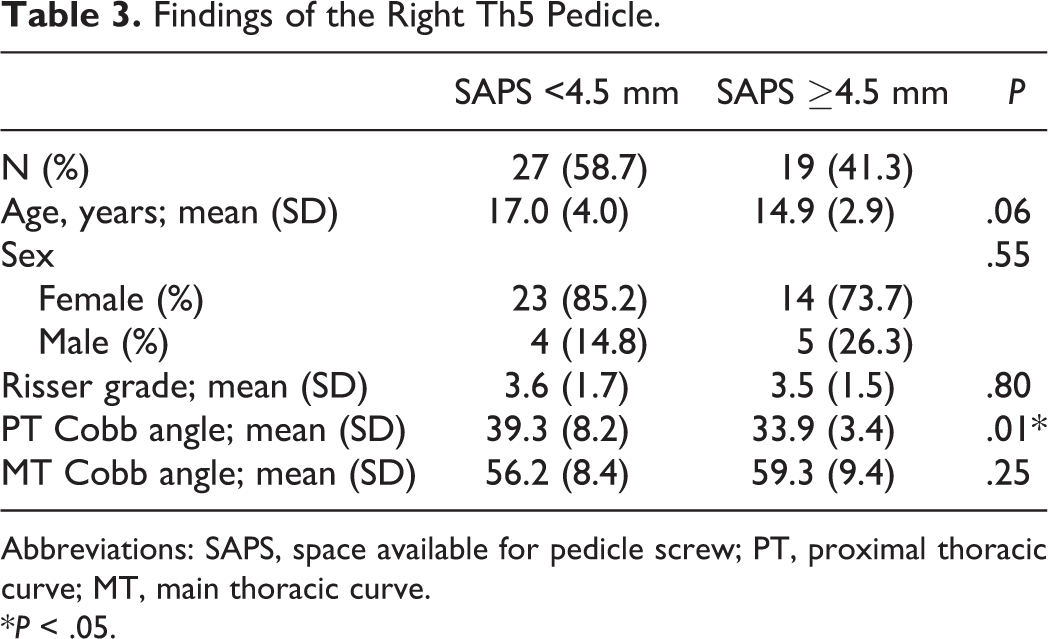
Abbreviations: SAPS, space available for pedicle screw; PT, proximal thoracic curve; MT, main thoracic curve.
*P < .05.
Findings of the Right Th6 Pedicle.
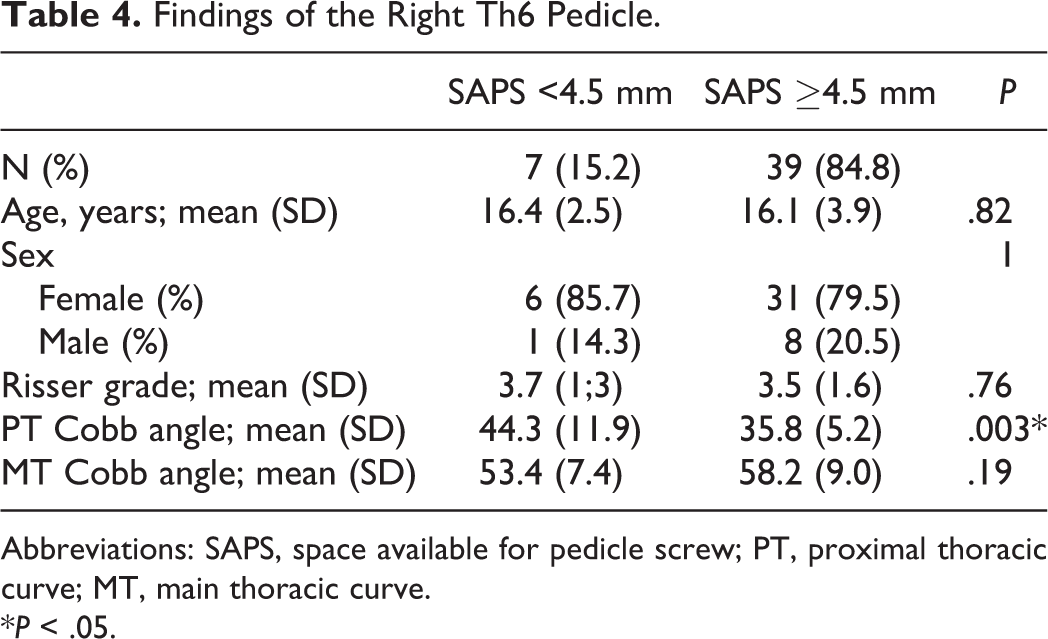
Abbreviations: SAPS, space available for pedicle screw; PT, proximal thoracic curve; MT, main thoracic curve.
*P < .05.
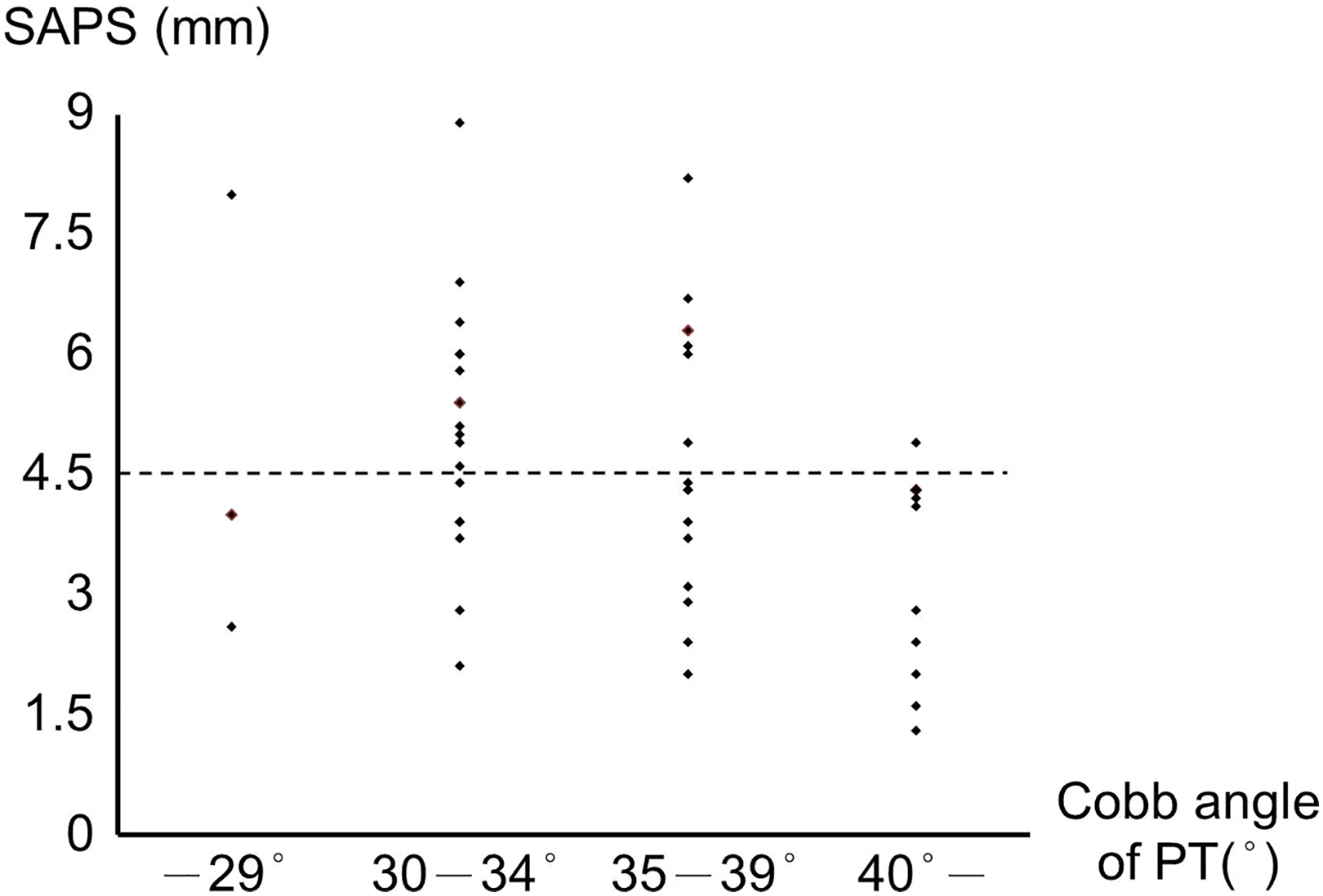
The relationship between the Cobb angle of the proximal thoracic (PT) curve and the space available for pedicle screw (SAPS) at the level of the right T5 pedicle. When the Cobb angle of the PT curve exceeds 40°, the SAPS becomes <4.5 mm in most cases at this level and is, therefore, unacceptable.
On the left side, most pedicles from T2 to T5 were acceptable (Table 5). At the level of T6, 7 pedicles (15.2%) were unacceptable. In all 7 of these cases, the caudal end vertebra of the PT curve was T5, which indicated that in these cases, T6 was involved in the MT curve, and thus, the spinal cord was deviated to the left side at this level. As well as on the right side, at all levels from T2 to T6, the left unacceptable pedicles, with a SAPS <4.5 mm, exhibited pedicle channels with Akazawa grade 3 or 4, although the number of unacceptable pedicles on the left side was much smaller than those on the right side (Table 5).
Left Pedicles.
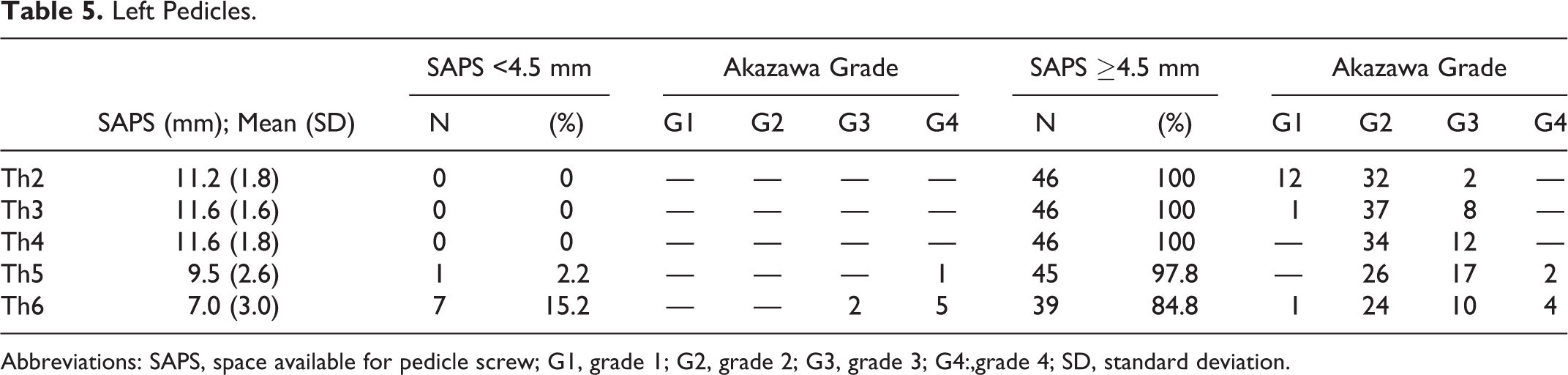
Abbreviations: SAPS, space available for pedicle screw; G1, grade 1; G2, grade 2; G3, grade 3; G4:,grade 4; SD, standard deviation.
Discussion
This is the first study that investigated the feasibility of inserting pedicle screws in the PT region in cases with Lenke type 2 idiopathic scoliosis in detail. The results of this study can be summarized in 4 points. First, we should avoid inserting pedicle screws into the right T3 and T4 pedicles in most cases via transpedicular trajectory. Second, at the right T5 and T6 levels, an unacceptable SAPS was associated with a large Cobb angle of the PT curve. Specifically, when the Cobb angle of the PT curve exceeds 40°, transpedicular insertion of a screw in the right pedicle of T5 should be avoided. Third, in most cases, left pedicles of the PT region in cases with Lenke type 2 idiopathic scoliosis are acceptable, although we should pay attention when inserting a screw into the left T6 pedicle in cases where T5 is the caudal vertebra of the PT curve. Fourth, on both sides, from T2 to T6, unacceptable pedicles, with an SAPS <4.5 mm, had Akazawa grade 3 or 4 pedicle channels. In other words, when the pedicle channel is wider than 2 mm, which corresponds to an Akazawa grade 1 or 2, we can insert pedicle screws safely in terms of the position of the spinal cord.
When the pedicle channel is wider than the diameter of the planned pedicle screw, the risk of spinal cord injury due to insertion of a pedicle screw is quite low. However, the pedicle channel is not always wide enough for a pedicle screw. In such cases, the safety of inserting pedicle screws into pedicles is determined by 2 factors, namely, the width of the pedicle channel and the degree of deviation of the spinal cord (Figure 1B). Regarding the pedicle channels, previous studies have described the anatomical features of the pedicles in cases with or without scoliosis. Kim et al and McLain et al have shown that pedicle channels are anatomically narrow in the PT region. 3,4 Abul-Kasim et al and Davis et al reported that pedicles on the concave side of a curve are narrower than those on convex side in cases of idiopathic scoliosis. 2,7 These results indicate that pedicle channels on the right concave side of the PT curve are potentially too narrow for pedicle screw insertion. Hence, in this region, pedicle screws can easily violate the spinal canal and damage the spinal cord. Thus, when we try to insert pedicles screws on the right side of the PT curve, determining the position of the spinal cord in the spinal canal is quite important. Previous studies that have examined the deviation of the spinal cord in cases of scoliosis have used magnetic resonance (MR) imaging. 1,8,9 Although MR imaging is a very powerful modality for visualization of the spinal cord, MR imaging is inferior to CT in some aspects. First, MR imaging is not suitable for thin slice analysis as we used in our study. Second, MR imaging is also not suitable for visualizing the cortical bone, which includes the thin pedicles of the vertebrae. For these reasons, previous studies have not reported on pedicle channels in relation to the spinal cord. To overcome this limitation, we used post-myelography CT in our study, which allowed us to define the SAPS parameter to simultaneously assess the width of the pedicle channel and the degree of deviation of the spinal cord using a single modality.
No previous study has focused on the safety of pedicle screw insertion for the PT curve in cases with Lenke type 2 idiopathic scoliosis. Our findings show that inserting pedicle screws into the right concave side of the PT curve carries a potential risk of compressing the spinal cord. One solution might be to use the in-out-in technique, although the extrapedicular screw has inferior pull-out strength compared to a transpedicular screw. As such, there is doubt regarding whether extrapedicular screws would have sufficient strength to resist the lateral force exerted on the concave side. 10 Hence, surgeons have to be familiar with other anchoring methods, including hooks or sublaminar wires, for acquiring good correction and secure fixation of the PT curve, although segmental pedicle screw instrumentation remains the most powerful technique for curve correction.
When the pedicle channel is <2 mm, which corresponds to an Akazawa grade 3 or 4, more than 70% (119/168 = 0.71) of pedicles are at risk for spinal cord injury on the right concave side of the PT curve (Table 2). This indicates that if the pedicle channel is very narrow, the spinal cord is also probably deviated very closely to the inner wall of the pedicle. This relationship between the width of the pedicle channel and the position of the spinal cord implies that narrow pedicles on the concave side of scoliosis may result from a scalloping mechanism caused by pulsation of the spinal cord.
This study has a few limitations. First, we investigated the safety of inserting pedicle screws only in terms of spinal cord injury and did not consider other organs at risk for injury, including the aorta or esophagus. 11 -14 Second, the post-myelography CT was obtained in the supine position in all patients, although segmental fixation surgery for scoliosis is performed in prone position. Therefore, the actual position of the spinal cord in the spinal canal during surgery may be different from that seen on the post-myelography CT images.
In conclusion, we investigated, for the first time, the feasibility of inserting pedicle screws in the PT region in cases of Lenke type 2 idiopathic scoliosis, defining a new parameter, the SAPS. Post-myelography CT enabled us to accurately assess the morphometry of the pedicles and deviation of spinal cord at the same time, and clearly demonstrated the feasibility of inserting pedicle screws in the PT region.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the research ethics committee of the University of Tokyo.