
Abstract
Study Design:
Retrospective database review.
Objectives:
To determine factors associated with unplanned readmission, complications, and mortality in patients undergoing operative management for C2 fractures.
Methods:
The American College of Surgeons–National Surgical Quality Improvement Program (ACS NSQIP) was queried between 2007 and 2014. Unplanned readmission, any complication, and mortality were the outcomes of interest. Bivariate statistics were calculated, and multivariate regression models were estimated.
Results:
A total of 285 patients were enrolled. Readmission data was available for 199 patients and 11 patients (5.5% of 199 patients) had an unplanned readmission. Overall, 60 patients (21% of 285 patients) had at least 1 complication and 15 patients (5.3% of 285 patients) died. Five factors were associated with complications: transferred from another facility (odds ratio [OR] 3.00, 95% confidence interval [CI]1.51-5.98; P < .01); operative time ≥180 minutes (OR 2.43, 95% CI 1.11-5.36; P = .03); at least 1 patient comorbidity (OR 2.50, 95% CI 1.01-6.18; P < .05); American Society of Anesthesiologists (ASA) class 3 (OR 4.86, 95% CI 1.19-19.88; P = .03); and ASA class 4 (OR 7.24, 95% CI 1.66-31.66; P = .01). The only factor associated with unplanned readmission was having at least one postoperative complication (OR 7.10, 95% CI 1.04-48.59; P < .05), while patients who were partially or totally dependent from a functional standpoint were at increased odds of death (OR 3.98, 95% CI 1.12-14.08; P = .03).
Conclusions:
Patients with functional limitations have increased odds of death, while patients with postoperative complications have increased odds of unplanned readmission. Being transferred from an outside facility, having an operative time ≥180 minutes, having at least one comorbidity, and being classified as ASA class 3 or 4 increase patient odds of complication.
Introduction
Among the elderly, cervical spine fractures are common, especially compared with other age brackets. 1,2 Of all cervical spine fractures, C2 level fractures have been shown to be most common and have demonstrated an increasing incidence over recent years. 1,3,4 One recent study demonstrated a 135% increase in the rate of C2 fractures from 2000 to 2011. 3 As the population continues to age, it is likely that this trend could continue into the foreseeable future. 5 Thus, a robust analysis of risk factors that may impact outcomes—complications, mortality, and unplanned readmission—is warranted.
To date, much of the literature has focused on specifically on the outcomes after odontoid fractures within a predetermined age range (eg, octogenarians) and has compared outcomes stratified by nonoperative and operative intervention. 6 -8 Additional research has evaluated patients with odontoid fractures presenting for care irrespective of treatment approach. 9 However, much of the research includes only small cohorts (eg, 26 consecutive patients). 10 With the increasing incidence of these fractures, there is an unmet need to better understand the factors associated with complications, mortality, and unplanned readmission for those patients undergoing surgical intervention for such fractures among all age ranges.
Using the American College of Surgeons–National Surgical Quality Improvement Program (ACS NSQIP) database, this study aimed to answer the following 3 study questions: (1) What factors (patient and care delivery characteristics) are associated with unplanned readmission within 30 days of surgery? (2) What factors (patient and care delivery characteristics) are associated with at least one complication within 30 days of surgery? (3) What factors (patient and care delivery characteristics) are associated with mortality within 30 days of surgery?
Materials and Methods
Data Source
In this retrospective study, the ACS NSQIP database was used. 11 In order to ensure the database remains as accurate as possible, trained and certified Surgical Clinical Reviewers gather the data and audits of selected participating sites are conducted. 11 Prior research has further shown that the ACS NSQIP is better at identifying complications than other databases, such as the University HealthSystems Consortium. 12 Readmissions, complications, and death up to 30 days following surgery are captured in ACS NSQIP.
Inclusion Criteria and Outcome Data Classifications
From 2007 to 2014, patients undergoing surgical management for a C2 fracture were identified using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis (805.00 805.02, 805.12) and primary CPT (20 660, 20 661, 20 664, 20 665, 22 310, 22 315, 22 318, 22 319, 22 326, 22 595, 22 841, 22 590, 63 001) codes. In total, 285 patients fit our inclusion criteria.
The outcomes of interest were unplanned readmission, any complication, and mortality within 30 days of surgery. The unplanned readmission variable consists of instances in which patients were readmitted to the hospital when it was not planned at the time of the principal procedure. Also, unplanned readmission was only captured from 2012 onward in ACS NSQIP. Complications included need for transfusion, failure to wean off oxygen, pneumonia, unplanned intubation, urinary tract infection, cardiac arrest, cerebrovascular accident, organ/space surgical site infection, deep surgical site infection, superficial surgical site infection, deep vein thrombosis, myocardial infarction, pulmonary embolism, renal insufficiency, sepsis, and shock. Complications were coded as “1” or “0,” where “1” indicated that at least one instance of the complication occurred, while “0” indicated the complication did not occur.
Covariates
A total of 10 covariates were included in both the complications and mortality multivariate regression models. The covariates included age, gender, race, and ethnicity, admission source, functional status, operative time, surgeon specialty, at least one preoperative comorbidity, American Society of Anesthesiologists (ASA) class, and body mass index (BMI). These covariates were included in the multivariate regression models based on clinical experience, theory, 13 and literature suggesting that they may be confounders—that is, they help in explaining the variation in the outcome. Indeed, current research demonstrates that age, 14 gender, 15 race and ethnicity, 16,17 operative time, 14,18 surgeon specialty, functional status, 14 comorbidities, 15 ASA class, 14 and BMI 18 can be associated with spine surgery outcomes. While a number of previous studies have not demonstrated that admission source 14 or surgeon specialty 19 are associated with spine surgery outcomes, the inclusion of such covariates in previous studies suggest that they are acceptable covariates to include in this study. The same covariates plus the addition of at least one postoperative complication were used in the readmission multivariate regression model.
For all models, the following covariates were categorical: age (years; <60, 60-69, 70-79, ≥80); gender (male or female); race and ethnicity (non-white/non-Hispanic, white/non-Hispanic, Hispanic); admission source (admitted from home or transferred from another facility); functional status (independent or partially/totally dependent); surgeon specialty (orthopedic surgery or neurosurgery); at least one preoperative comorbidity (yes or no); and ASA class (1 and 2, 3, or 4). For the any complication model, BMI was a categorical variable (underweight, normal, overweight and obese, or missing), while it was a continuous variable for the unplanned readmission and mortality models. For the unplanned readmission model, operative time (minutes) was continuous, but operative time was categorical (<120, ≥120 but <180, or ≥ 180 minutes) for the any complication and mortality models. For the unplanned readmission model, at least one postoperative complication was categorical (yes or no). The differences in certain variables being specified as categorical or continuous are due to the distribution of the covariates for the particular outcome and are based on an understanding that models need to converge to be of value.
Statistical Analysis
The frequency and percentages of each main outcome of interest (readmission, any complication, mortality) were calculated and reported (Table 1). The specific complications were also determined (Table 1). Bivariate analyses were conducted to compare differences between patient characteristics (eg, age; preoperative comorbidities) and care variables (eg, surgical approach, surgeon subspecialty) (Table 2). Multivariate logistic regression models were used to determine factors that placed patients at increased risk of unplanned readmission, any complication, or mortality within the first 30 postoperative days, accounting for all other factors. Because we worked with a sample and not the full population (or a sample approximating the full population) in this study, we neither used set P value cutoffs in the bivariate analyses, nor any form of stepwise selection methods, to determine the final set of covariates included in the regression models. Significance was set a priori at P < .05.
Patient Outcomes (n = 285).
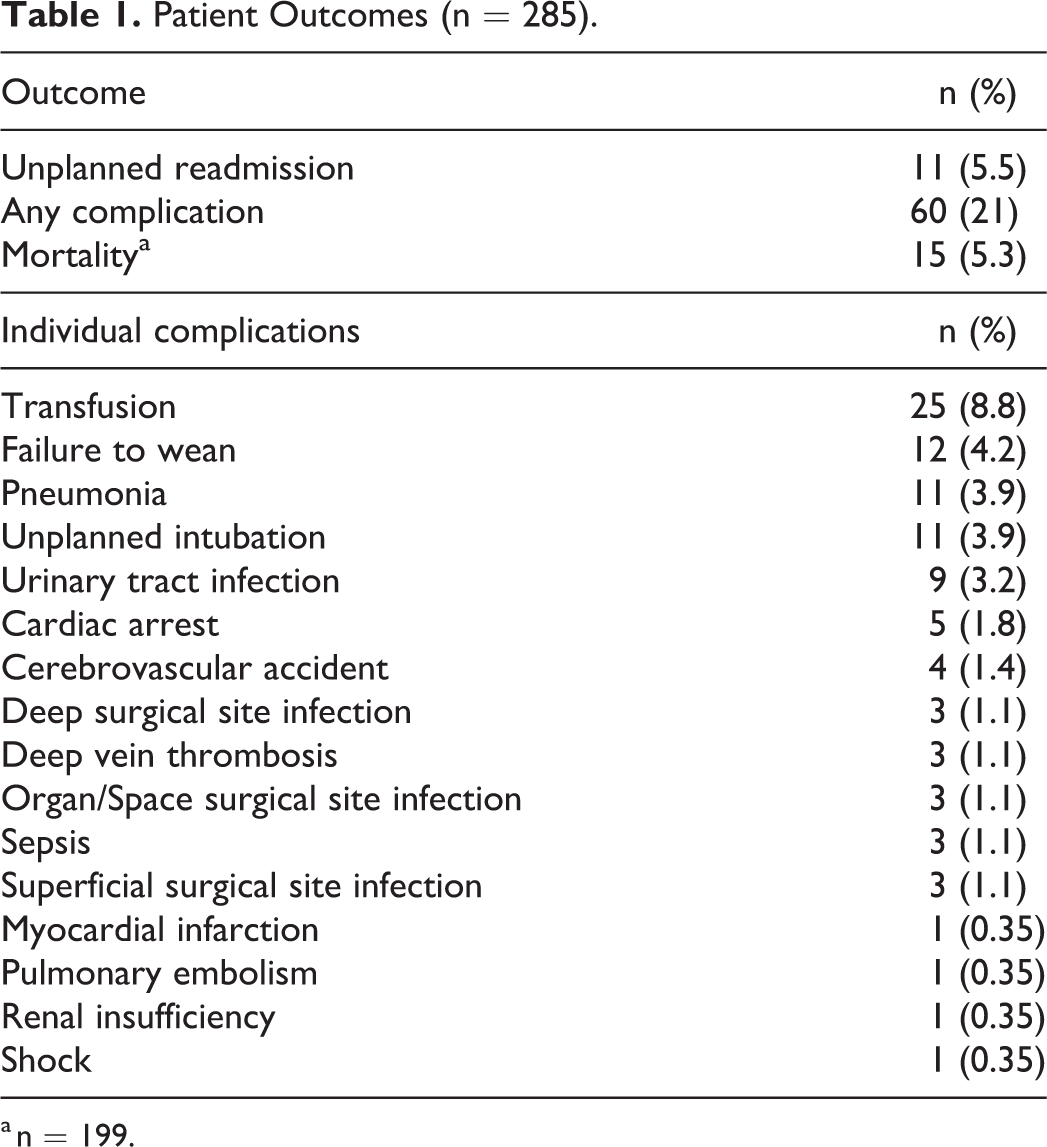
a n = 199.
Bivariate Analysis Comparing Patient and Surgery Factors in Those With and Without One or More Complication or Mortality.
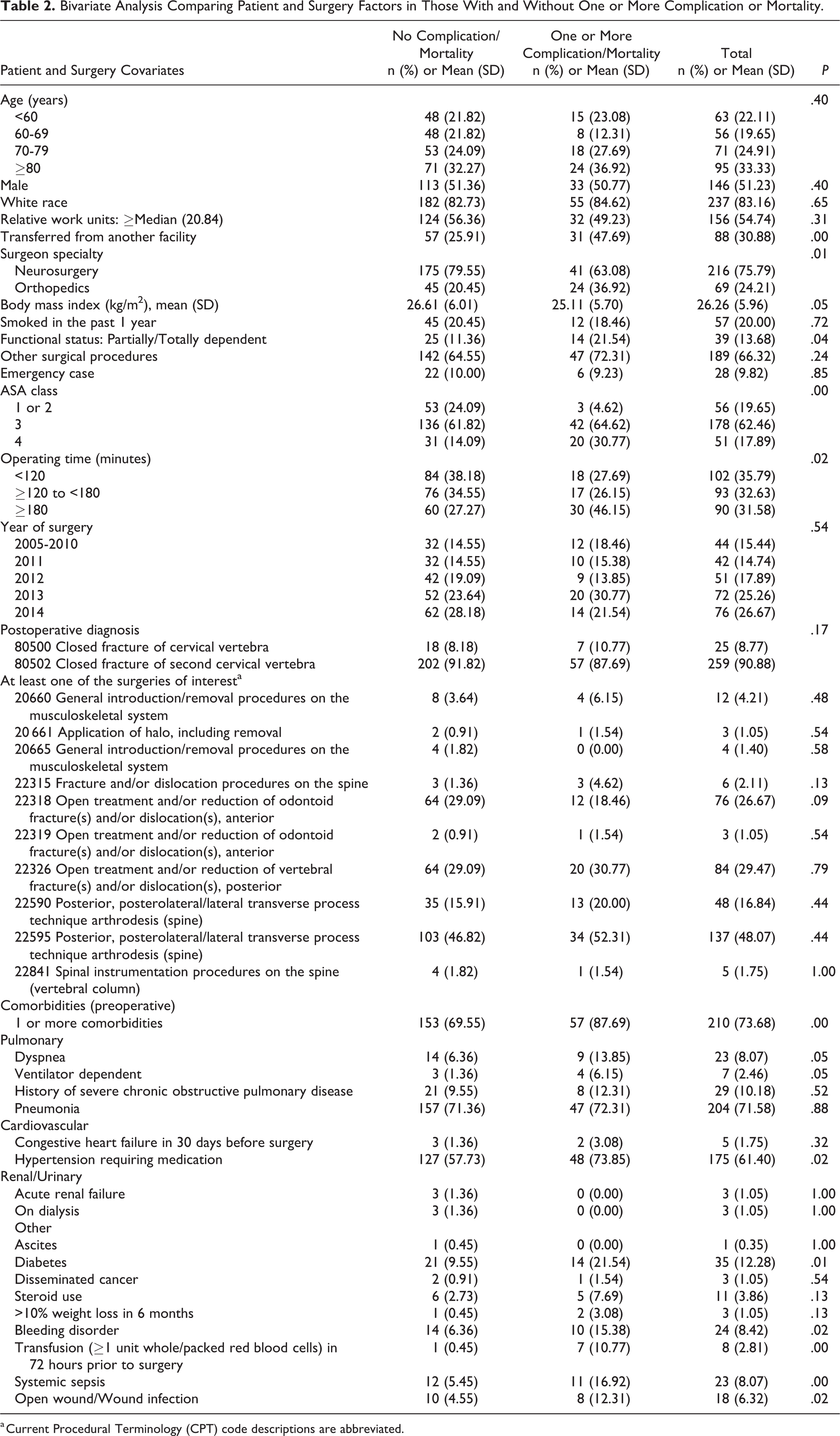
a Current Procedural Terminology (CPT) code descriptions are abbreviated.
Results
Of the 285 patients meeting inclusion criteria over the entire study time frame, nearly one quarter of patients (60; 21%) had a complication, while 15 patients (5.3%) died over the initial 30 postoperative days (Table 1). In the subset of the patient sample (199 patients) that could be analyzed for unplanned readmission (2012 onward), a total of 11 patients (5.5%) had an unplanned readmission within the initial 30 postoperative days (Table 1). The most common complication was the postoperative need of blood transfusion (25 patients; 8.8%), while myocardial infarction, pulmonary embolism, renal insufficiency, and shock were similar for the least common complication (1 patient each; 0.35%) (Table 1).
A significantly higher percentage of patients who had at least one complication or died within the initial 30 postoperative days were transferred from another facility (47% vs 26%, P < .01); partially or totally functionally dependent (22% vs 11%, P = .04); and/or had one or more comorbidities (88% vs 70%, P < .01) (Table 2). Additionally, a significantly higher percentage of patients designated as ASA class 4 (31% vs 14%, P < .01) and/or had operations of longer duration (≥180 minutes) (46% vs 27%, P = .02) had at least one complication or died (Table 2).
In multivariate analysis, the following factors were associated with increased odds of at least one complication: transferred from another facility (odds ratio [OR] 3.00, 95% confidence interval [CI] 1.51-5.98; P < .01); operative time ≥180 minutes (OR 2.43, 95% CI 1.11-5.36; P = .03); at least one patient comorbidity (OR 2.50, 95% CI 1.01-6.18; P < .05); ASA class 3 (OR 4.86, 95% CI 1.19-19.88; P = .03); and ASA class 4 (OR 7.24, 95% CI 1.66-31.66; P = .01) (Table 3). In multivariate analysis, the following factors were associated with decreased odds of at least one complication: age of 60 to 69 years (OR 0.27, 95% CI 0.09-0.83; P = .02) and age ≥80 years (OR 0.33, 95% CI 0.12-0.91; P = .03) (Table 3).
Multivariate Analyses for Complications, Unplanned Readmission, and Mortality in Patients Receiving Operative Care for a C2 Fracture.
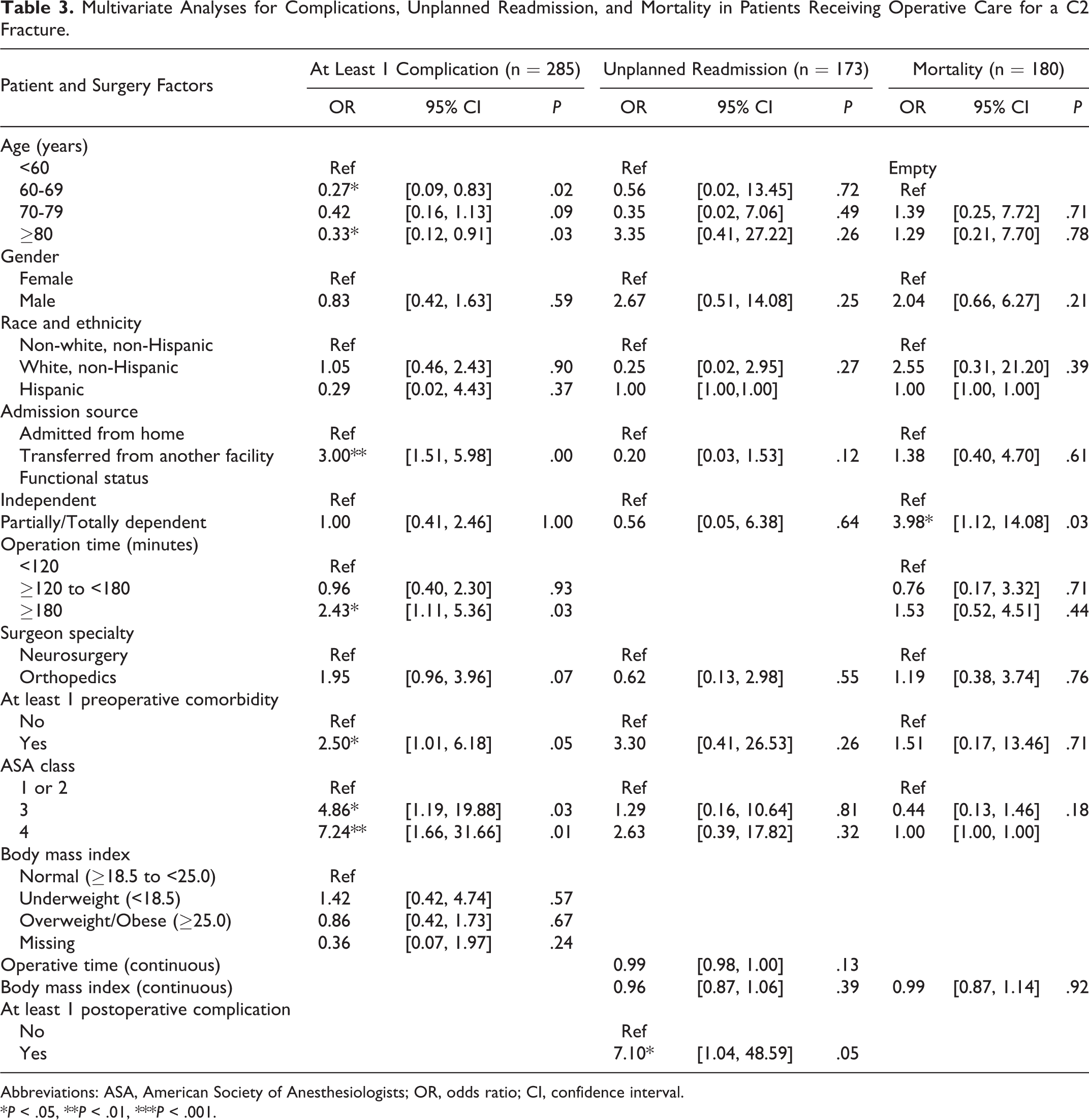
Abbreviations: ASA, American Society of Anesthesiologists; OR, odds ratio; CI, confidence interval.
*P < .05, **P < .01, ***P < .001.
When accounting for other factors in a multivariate analysis, the only factor that significantly increases the odds of unplanned readmission is at least one postoperative complication (OR 7.10, 95% CI 1.04-48.59; P < .05) (Table 3). When accounting for other factors in the multivariate analysis, patients who were either partially or totally functionally dependent were at increased odds of death (OR 3.98, 95% CI 1.12-14.08; P = .03).
Discussion
This study uses a large, high-quality database to offer insight into factors associated with unplanned readmission, complications, and mortality in patients undergoing surgical intervention for C2 spine fractures. Such understanding is lacking in the current literature. We found that having at least one postoperative complication was the only factor associated with unplanned readmissions. However, our results demonstrate that being transferred from another facility for surgery, extended operating time, at least one patient comorbidity, and worse ASA class increased the odds of a complication occurring within 30 days of surgery. In contrast, certain age ranges have decreased odds of complications. Only poor patient functional status is associated with increased odds of death.
There is very limited research analyzing factors associated with unplanned readmission following a C2 fracture. Indeed, most of the current literature has compared surgical approaches or operative versus nonoperative approaches, not specifically what factors affect readmission following surgical intervention. In one study by Patterson et al, 20 data between 2005 and 2013 from the ACS NSQIP were used to compare outcomes of odontoid stabilization using an anterior versus posterior approach in a cohort of 141 patients. The authors found that patients undergoing an anterior approach were more likely to have a readmission than patients undergoing a posterior approach. 20 Patterson et al 20 also found that a surgery via an anterior approach was shorter in duration than surgery via a posterior approach. Despite our bivariate analysis demonstrating that patients with longer surgeries had a higher percentage of at least one complication or mortality, our multivariate analysis found no increased odds between duration of surgery and unplanned readmission. In another study of the Medicare claims database from 2000 to 2011, Pearson et al 3 found that older patients (80-85 years and >85 years) had increased odds of 30-day unplanned readmission. However, we did not find similar results, which may be due to the fact that we included more and different covariates and included all age ranges, not simply those who qualify for Medicare. Indeed, the younger patients who had C2 fractures may have other severe health comorbidities and/or other characteristics that no longer make age a predictor of unplanned readmission when all age groups are taken into account. Overall, because our work demonstrates that the only factor associated with increased unplanned readmission is having at least one postoperative complication, we suggest focusing on optimizing patients preoperatively or taking steps to assess and minimize intraoperative and postoperative complications to reduce unplanned admissions as much as possible.
We found a number of factors associated with increased complication risk that is consistent with prior reports in the literature. In a retrospective review of 225 consecutive patients, Bokhari et al 21 found that neurological deficits, comorbidities, and presence of other injuries were predictors of complications and death. Similarly, we also found that the presence of at least one comorbidity increased the odds of having at least one complication. Further, we found that worse ASA class (ASA class 3 of ASA class 4) and transfer from another facility also increased the odds of having at least one complication. Higher ASA class and transfer from another facility likely indicate patients with more health complexity, potentially consistent with neurological deficits and presence of other injuries. Another study by Yue et al 22 showed that bleeding disorder/coagulopathy and intensive care unit (ICU) admission following traumatic C2 fracture surgery were associated with increased odds of complication. Again, these are similar to our findings, which show that at least one preoperative comorbidity, overall worse health status, as measured by ASA class, and transfer from another facility are associated with increased odds of at least one complication. While the factors associated with increased odds of complications are not easily addressed preoperatively, these findings do suggest that there is value in attempting to optimize patient comorbidity status as much as possible prior to surgery and then increasing surveillance postoperatively to try to reduce complication risk. However, such knowledge can also be used to discuss patient and family expectations and have more robust shared decision-making discussions.
In addition to determining predictors of unplanned readmission and complications in all patients undergoing surgical intervention in a large database, we also found that partially or totally dependent functional status was the only predictor of 30-day postoperative mortality. Similar to the predictors of complications, this is a challenging factor to optimize prior to surgical intervention. Woods et al 23 showed that while a difference in mortality favors surgical treatment in the short term, there are no long-term mortality benefits to surgical intervention. Additionally, other work has shown unlikely differences in mortality based on treatment approach for older patients (eg, octogenarians). 7 Furthermore, Perry et al 6 found no difference in mortality rate for patients undergoing operative versus nonoperative intervention at 3 years follow-up in patients with type II odontoid fractures. Similarly, Radovanovic et al 24 found no difference in mortality based on treatment approach. Therefore, it is critical for surgeons to have honest and open dialogue regarding surgical and nonsurgical treatments options including surgical risk and benefits. Perhaps, it may be of the best interest of patients with partially or totally dependent functional status to discuss potentially nonoperative treatment whenever possible.
The limitations of our study must be considered when evaluating its findings. First, many of the limitations are from the inherent limits of using the ACS NSQIP database. While there are quality controls to ensure accurate data entry, including data abstraction by trained clinic reviewers, errors may still be possible. Furthermore, procedure-specific complications are unavailable in the ACS NSQIP database. For example, while we are able to determine complications (eg, blood transfusion) that occurred during an admission for a C2 fracture in which surgery was performed, we cannot exactly pinpoint the reason for the complication. However, we can state that the blood transfusion occurred within the first 72 hours of the surgery start time. 11 In addition, the ACS NSQIP contains a great deal of data from academic medical centers; thus, our findings may not be generalizable to nonacademic medical centers. The database is also created via an opt-in approach, so it is likely to not be a true national representation. Last, the database only reports our outcomes of interest (readmission, any complication, mortality) within a 30-day timeframe postoperatively; therefore, we may be underestimating the true rates of readmission, any complication, and mortality. Nevertheless, it is a large database with many participating institutions; therefore, we feel it is a reliable and value database worthy of analysis. Second, there are number of different C2 fractures; the predictors for unplanned readmission, complications, and mortality of each individual fracture type may differ. Unfortunately, we are limited in conducting such an analysis because of our small overall sample despite the use of a large database. In our clinical practice at a level-I trauma center, we routinely manage nondisplaced C2 fractures (odontoid, hangman’s) nonoperatively with either a hard collar or a halo. 25 -29 However, in the setting of fractures with neurological deficits or displaced fractures, we perform posterior-based decompression and stabilization.
The current study provides insight into risk factors associated with increased odds of unplanned readmission, complications, and mortality in patients with C2 fractures undergoing surgical intervention. The predictor or predictors for each outcome are challenging to address. We believe that working to optimize known patient comorbidities and functional status prior to surgical intervention, if necessary, may improve outcomes. If surgery is offered to a patient with a C2 fracture, the surgeon should minimize the surgical time to less than 3 hours. Additionally, in patients with comorbidities (eg, ASA class 3 or 4) the surgeon should have a frank discussion regarding the increased rate of postoperative complications and mortality as compared with healthier patients. Indeed, prior research within the orthopedic surgery literature demonstrates that preoperative optimization of modifiable risk factors can lead to improved outcomes, including decreased readmissions. 30 Keeping in mind the results of our study, we recommend caution in proceeding with surgical intervention. In the senior author’s practice, stable C2 fractures are managed with a hard collar, while unstable C2 fractures are managed with a halo vest immobilization. Operative intervention is considered for C2 fractures with neurological compromise or C2 fractures in the setting of a hyperostotic spine. If surgical intervention can be avoided in patients with poor health, functional status, and/or comorbidities, it may be an acceptable management approach. Our work can help surgeons, patients, and families have open and honest discussions about reported benefits and risks associated with surgical intervention for C2 fractures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DNB reports grants from Alpha Omega Alpha (AOA), outside the submitted work. ENM reports personal fees from Evolution Spine, personal fees from Globus Medical, outside the submitted work. AM reports grants from Globus, grants from LES Society, grants from Corelink, grants from AO Spine, grants from OMeGA, outside the submitted work. All other authors (CT, BR, RWM) have no disclosures.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.