
Abstract
Study Design:
Literature review.
Objectives:
Posterior cervical interfacet cages are an alternative to lateral mass fixation in patients undergoing cervical spine surgery. Recently, a percutaneous, tissue-sparing system for interfacet cage placement has been developed, however, there is limited clinical evidence supporting its widespread use. The aim was to review studies published on this system for patient reported outcomes, radiographic outcomes, intraoperative outcomes, and complications.
Methods:
Four electronic databases (PubMed, EMBASE, Scopus, and MEDLINE) were queried for original published studies that evaluated the percutaneous, tissue-sparing technique for posterior cervical fusion with interfacet cage placement. All studies reporting on open techniques and purely biomechanical studies were excluded.
Results:
The extensive literature search returned 7852 studies. After systematic review, a total of 7 studies met inclusion criteria. Studies were independently classified as retrospective or prospective cohort studies and each assessed by the GRADE criteria. Patient reported outcomes, radiographic outcomes, intraoperative outcomes, and complications were extracted from each study and presented.
Conclusions:
Tissue-sparing, posterior cervical fusion with interfacet cages may be considered a safe and effective surgical intervention in patients failing conservative management for cervical spondylotic disease. However, the quality of evidence in the literature is lacking, and controlled, comparative studies are needed for definitive assessment.
Introduction
Foraminal stenosis in the cervical spine occurs as a result of intervertebral disc degeneration and spondylosis which elicits the clinical presentation of cervical radiculopathy. 1 Although many patients improve with conservative management, a cohort of patients may require surgical intervention and decompression for refractory symptoms. The neural foramen in the cervical spine may be decompressed either directly or indirectly through a variety of techniques.
Cervical interfacet spacers (CIS) or cages are a relatively new advancement in the treatment of cervical spondylotic and radicular disease. Through distraction of the facet joint, these implants increase foraminal height and volume allowing indirect decompression of the exiting nerve root. 2 -4 Because the facet joint correlates with center of range of motion and fulcrum of spinal movement in the cervical spine, interfacet distraction implants may have a distinct biomechanical advantage and less significant ability to generate kyphosis. 3 Additionally, the facet distraction arthrodesis technique, as originally described by Goel, 5 may be a straightforward and robust method of spinal stabilization. After joint preparation and decortication, these implants are press-fit into the interfacet region to facilitate fusion. 3 Given their relatively large footprint in relation to the facet surface area and their placement under compression, these devices may allow for rapid arthrodesis. 3,5
There have been a number of studies reporting on the open technique of interfacet allograft cages or spacers; however, these methods require extensive subperiosteal muscular dissection lateral to the facet joints, which may result in muscle denervation, delayed wound healing, poor cosmesis, and infection. 2,3,6,7 Recently, a percutaneous system (DTRAX) has been designed to mitigate the morbidity associated with the open, posterior cervical approach and allow interfacet instrumentation through minimal access incisions. 2 The system takes advantage of the orientation of the cervical facets, such that distraction opens the neural foramina. Under fluoroscopic guidance, a series of rasps and decorticators are used to prepare the facet joint surface and promote bony healing. 7,8 A titanium shim with windows for insertion of bone graft is inserted percutaneously into the facet, thus stabilizing the facet with instrumented distraction. 8
Although a number of morphometric and biomechanical studies exist regarding the technique, 3,4,9,10 there is limited clinical evidence supporting its widespread use. The purpose of the current study was to rigorously and systematically evaluate the clinical and radiographic outcomes of percutaneous cervical fusion with interfacet cages based on the currently available literature.
Methods
Literature Search and Study Identification
A comprehensive search of the literature was performed based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines on September 30, 2018. The databases used included PubMed, EMBASE, MEDLINE, and Scopus. Our goal of the search was to identify clinical studies reporting on percutaneous posterior cervical fusions with interfacet cages. All published articles were retrieved without a search constraint on publication date. The key words and phrases used are found in Table 1. A manual search of reference lists of included studies and previous reviews was also performed to find any additional suitable citations.
Keywords and MeSH Terms Used in the Query of PubMed, EMBASE, Scopus, and MEDLINE Databases.
Quality Assessment
Studies were independently assessed for quality by 2 investigators (J.L. and K.G.) using the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) criteria. 11 Only 1 discrepancy existed in the quality assessment process resulting from misunderstanding of the methods in a study. The discrepancy between the 2 reviewers was resolved by discussion and consensus.
Study Selection and Data Extraction
All potentially relevant publications retrieved from the 4 databases were combined and evaluated. Titles were screened for relevance to percutaneous posterior cervical cages and interfacet fusion devices. Subsequently, the abstracts of selected articles were screened to isolate clinical studies. During the title and abstract screening, if insufficient data was present, the citation was assessed by full-text review. Full-text review was performed on the selected abstracts focused on outcomes related to clinical efficacy and radiographic outcome.
The final inclusion criteria included the following: (1) clinical series of posterior cervical fusion with interfacet cages and (2) percutaneous, tissue-sparing surgical technique. All studies reporting on open techniques and purely biomechanical studies were excluded. No studies were excluded on the basis of the types of outcome measures used or study design.
Two independent investigators (J.L. and K.G.) extracted the following: patient-reported outcomes, radiographic outcomes, fusion rates, complications, and intraoperative outcomes (length of stay, estimated blood loss, and operative time). Patient-reported outcomes included visual analogue scale (VAS) for neck and arm pain, as well as Neck Disability Index (NDI) and Short Form–12 (SF-12) questionnaires.
Results
Included Studies and Quality of Evidence
The extensive literature search returned 7852 studies. After systematic review, a total of seven studies met inclusion criteria (Figure 1). 8,12 -17 All studies were classified as either retrospective cohort or prospective cohort. There were no studies with a control or comparison group. The highest quality evidence was in the form of prospective case series. 8,12,14,16 The quality of evidence for all articles, using the GRADE criteria, was estimated to be low based on the observational nature of the studies. 11 Only 2 of the relevant studies had ≥60 patients (28.6%). 13,15 Clinical and radiographic final follow-up ranged from 12 to 24 months. Four of the included studies included patient reported outcomes (71.4%). 8,14,16,17 One study was a purely radiographic study 12 (14.3%) and another study was an analysis of a medical device registry (14.3%). 13
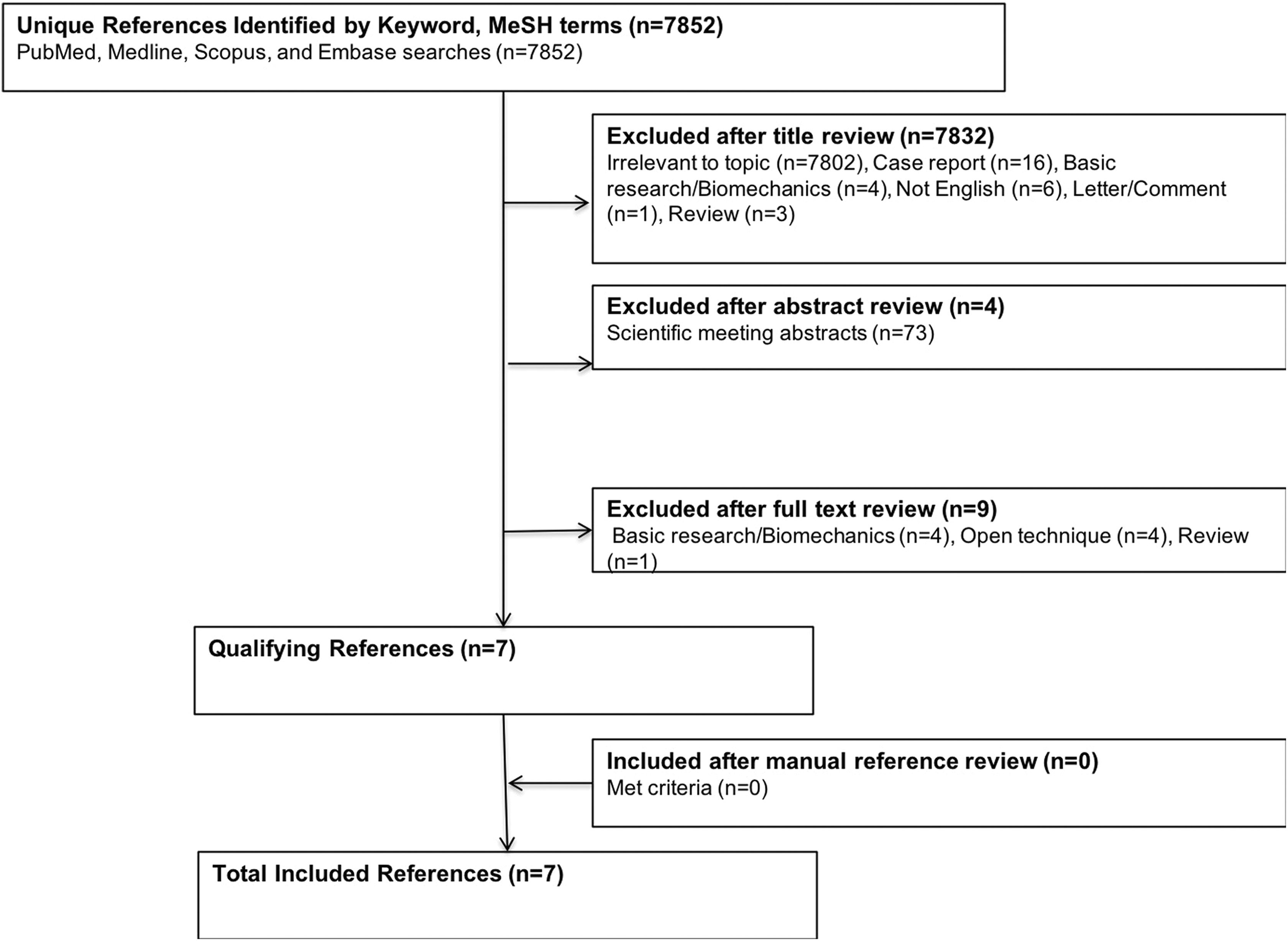
Flow diagram presenting the systematic review process used in this study.
All studies, except 2, were limited to single-level interventions. In the study by Smith et al, 17 the breakdown of levels was single-level (36%), 2-level (24%), 3-level (32%), and 4-level (8%) procedures. In the medical device registry, the breakdown of levels was single-level (36%), 2-level (36%), 3-level (25%), and 4-level (3%) procedures. 13
Intraoperative and Postoperative Outcomes and Complications
Table 2 shows an overall analysis of patient reported outcomes, radiographic outcomes, intraoperative outcomes, and complications analyzed by all articles included in the systematic review. It delineates the specific findings of each study and highlights the heterogeneity that is present in the literature for the commonly reported outcomes and complications.
Complications and Outcomes From Clinical Studies Evaluating Tissue-Sparing, Posterior Cervical Fusion With Interfacet Cages.
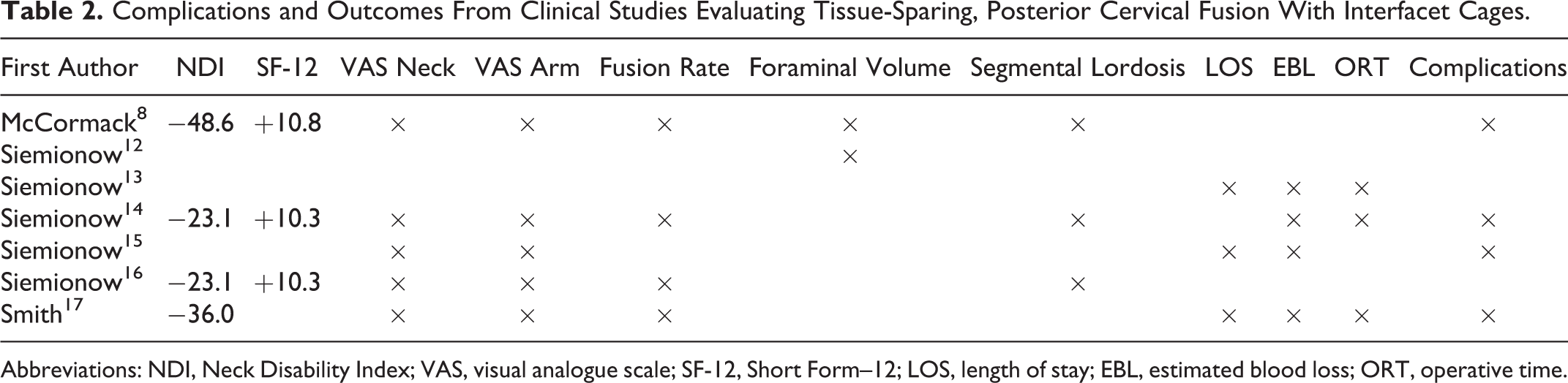
Abbreviations: NDI, Neck Disability Index; VAS, visual analogue scale; SF-12, Short Form–12; LOS, length of stay; EBL, estimated blood loss; ORT, operative time.
Discussion
Patient-Reported Outcome Measures
Patient outcome was assessed with NDI in all studies, except for 3—which used NDI in addition to SF-12. 8,14,16 At 12-month follow-up, the earliest published series in the literature reported significant improvements in the NDI (64.9 to 16.3). Additionally, the SF-12 physical component score (PCS), and SF-12 mental component score (MCS) improved from 34.6 to 45.4 and from 40.7 to 51.4, respectively. 8
At 24 months of follow-up, Siemionow et al 16 reported a significant decrease in NDI from 32.2 to 9.1 ± 7.7 (P < .0001). The authors also showed a significant improvement in the SF-12 PCS and MCS from 34.3 ± 6.0 to 43.7 ± 8.4 and 40.3 ± 7.6 to 51.4 ± 8.8, respectively (P < .0001). 16 In a follow-up study by the same group, the authors reported significant improvements at 24 months in NDI, SF-12 PCS, and SF-12 MCS of 32.2 ± 6.2 to 9.1 ± 7.7, 34.2 ± 6.0 to 43.7 ± 8.4, and 40.3 ± 7.6 to 51.4 ± 8.8, respectively (P < .0001). 14
Smith et al 17 reported on patients treated with percutaneous posterior cervical cage placement for pseudarthrosis after anterior cervical discectomy and fusion (ACDF). The authors showed a significant improvement in NDI from 65.1 ± 20.3 to 29.1 ± 17.9 at a mean of 18 months of follow-up. However, the study included only 25 patients with >1 year of follow-up, and the sample was quite heterogeneous with 36% of those patients required an additional anterior procedure for residual ventral compression or local kyphosis. 17 Overall, in all included studies, both SF-12 and NDI measures improved significantly after surgical treatment. All studies reached the previously described minimum clinical important difference (MCID) criteria for NDI of 7.5%. 18
Pain
With the exception of the device registry study and purely radiographic study, pain was evaluated utilizing the VAS pain score for neck and arm pain. 12,13 McCormack et al 8 reported the most robust improvement in VAS score for neck and arm pain with significant decreases of 5.2 points in both measures at final follow-up. The least robust improvement, although still quite notable, was a decrease in 4.10 and 4.12 for neck and arm pain, respectively (P < .01). 17 The remaining studies reported decreased VAS neck pain by 4.9 to 5.0 points and a decreased VAS arm pain of 4.8 points. 14 -16 Overall, the literature suggests that posterior cervical cage placement results in decreased pain at all time points after surgery. Moreover, all included studies well-exceeded the previously described MCID criteria for VAS of 3 points or greater. 18
Fusion Assessment
Fusion was assessed in a majority of the studies 8,14,16,17 ; however, the methods of radiographic fusion assessment were quite varied. Fusion was either assessed by computed tomography (CT) scans at 1 year or flexion-extension radiographs at final follow-up. Fusion by CT was determined by the presence of bridging bone across the facet joint surface or the overlying lateral masses on sagittal reconstructions. 8,14,16,17 Fusion by flexion-extension radiographs was assessed by translational motion <2 mm, 8,14,16 interspinous distance <2 mm, 8,14,16,17 and/or angular range of motion <5°. 8
There was strong consistency of fusion based on CT imaging across the majority of included studies. Based solely on bridging bone visualized on CT scan at 1 year postoperatively, there was 93% fusion across the treated surgical levels in all studies, except one—which reported 100% fusion. 17 There was significantly less uniformity when assessment was performed based on flexion-extension radiographs. Two studies reported radiographic fusion of 100% when using the criterion of translational motion <2 mm and 98.1% when using the criterion of <2 mm interspinous distance. 14,16 Using a combination of all 3 criteria (angular range of motion <5°, <2 mm translation, and bridging bone on CT scan), McCormack et al 8 reported a pseudarthrosis rate of 23.3%. Conversely, Smith et al 17 reported 100% fusion at the 1-year time point based on both flexion-extension radiographs and CT imaging.
Radiographic Outcomes
One hypothetical concern with using posterior cervical cages placed into the facet joints, however, is the possibility of introducing iatrogenic kyphosis. The placement of the cages between the superior and inferior articular processes causes longitudinal distraction. As a result of the distraction, there may be a reciprocal decrease in lordosis or even generation of kyphosis—particularly in clinical situations where the anterior column remains flexible and multiple levels are treated. 4 In the first series of cervical interfacet spacers, Goel and Shah 2 reported mild loss of lordosis after surgery, however, all patients remained with normal cervical lordosis at final follow-up.
In the first percutaneous series of interfacet cages, McCormack et al 8 reported no significant change in overall lordosis at 1 year compared with baseline (P > .05). Still, segmental lordosis at the treated level decreased by 1.4° and 1.6° at 6 months and 1 year compared with baseline (P < .05). 8 Siemionow et al 14 also reported no significant decrease in overall lordosis at 24 months compared with baseline (P = .40); conversely, in this study, the decrease in segmental lordosis at the treated level in this series was insignificant (P = .83).
Two studies included in our systematic review reported on radiographic changes to the foramen. 8,12 Surprisingly, McCormack et al 8 did not find any significant increase to foraminal height or volume at 12 months after surgery using plain radiographic measurements. However, using postoperative CT imaging, Siemionow et al 12 reported significant increases in foraminal height, area, and theoretical area of 0.35 mm, 0.17 mm2, and 0.29 mm2, respectively (P < .0001). These increases were maintained at 12 months of follow-up. Unfortunately, because of the small sample size, the authors did not perform a correlation between change in foraminal area and clinical outcome. 12
A follow-up study by Siemionow et al 16 evaluated the effect of single-level percutaneous interfacet cages on radiographic adjacent segment degeneration. The authors defined adjacent segment degeneration as a purely radiographic finding and reserved adjacent segment disease for cases where symptoms became clinically apparent. Overall, 5.9% of subjects developed adjacent segment degeneration within 2 years after fusion, but all were quite mild and none developed into adjacent segment disease. There were no statistically significant changes in proximal junctional kyphosis postoperatively (P = .3015). Additionally, there were no reoperations for adjacent segment disease in the 2 years following surgery. The results of this study are promising when compared with ACDF. Comparatively, in a meta-analysis involving 34 716 patients, the prevalence of adjacent segment degeneration was 32.8% (range, 7%- 92%). 19 Furthermore, in a study of Taiwan’s National Health Insurance Research Database (NHIRD) including 241 800 and 725.8 person-years, the 10-year reoperation rate for symptomatic adjacent segment disease was 5.6%. 20
Intraoperative Outcomes
Four studies reported on intraoperative outcomes, including length of stay (LOS), estimated blood loss (EBL), and operative time (ORT). 13 -15,17 Siemionow et al 14,16 reported a mean LOS of 29 hours, EBL of 32.83 ± 16.68 cm3, and mean ORT of 59.15 ± 19.98 minutes in single-level procedures. 7 Similarly, Smith et al 17 reported EBL of 87.8 cm3 (range, 5-200 cm3), ORT of 103.5 minutes (range, 28-282 minutes), and LOS of 1.4 days (range, 0.8-3.4 days), which was averaged across single-level (36%), 2-level (24%), 3-level (32%), and 4-level (8%) interventions. Although the mean and range of blood loss reported by Smith et al 17 may appear exaggerated, the study included anterior-posterior revisions for ACDF pseudarthrosis, which likely increased total blood loss given the revision anterior procedure.
The multicenter device registry likely provides the most pragmatic experience regarding the utilization and performance of the tissue-sparing, posterior cervical interfacet fusion. Including 13 centers and 271 patients, this study reported an average EBL of 74.8 ± 76.1 cm3, ORT of 73.5 ± 32.7 minutes, and LOS of 26 hours (range, 6-336 hours). 13 The mean LOS across our entire systematic review ranged from 26 to 33.6 hours 13 -15,17 and suggests a significant improvement on traditional posterior cervical fusion, which ranges from 4.0 to 7.3 days. 21 -28 Additionally, the mean EBL in this review ranged from 32.83 to 87.8 cm3 for the tissue-sparing, posterior interfacet fusion, 13 -15,17 which compares favorably to open posterior cervical fusions (range, 225-480 cm3). 21 -28
Complications
In light of the wide variety of therapeutic options for cervical spondylotic disease, it is important to understand the burden of percutaneous cervical interfacet fusion on the health care system in terms of intraoperative, perioperative, and postoperative complications. Although at least mentioned in most, 8,14,15,17 only 2 studies reviewed complications with significant detail. 14,15 McCormack et al 8 reported 2 unilateral facet fractures during insertion of the implants (1.7%) and 1 case of implant migration (0.8%). Similarly, there were only two reported complications in the series evaluating single-level, tissue-sparing interfacet cages for ACDF pseudarthrosis—including a recurrent laryngeal nerve palsy that was not related to the posterior procedure. 17
Siemionow et al 14 divided complications into device-related, procedure-related, and serious adverse events. There were no serious procedure or device related complications at two years postoperatively—including no case of device failure or migration. The most common device-related adverse events were shoulder pain and paresthesia, and the most common procedure-related adverse events were postoperative pain, nausea, pain from the bone graft harvest site, and shoulder pain. All these complications were minor and self-limited. 14
One study focused on the evaluation of perioperative complications within 30 days of surgery. 15 The authors reported 3 complications related to posterior cervical fusion with cages (3.4%), which included a patient developing atrial fibrillation postoperatively and another patient with a parietal stroke during the procedure. There were no patients who suffered an inadvertent durotomy, neurologic injury, infection, implant migration, vertebral artery injury or reoperation. Beyond the perioperative period, there was 1 case of a C5 palsy that presented 6 months after the posterior fusion procedure and 1 patient with a pseudarthrosis diagnosed at 12 months postoperatively. 15
The perioperative complications of tissue-sparing, posterior cervical fusion with interfacet cages are also promising when compared to other cervical surgical techniques. Neurologic complications reportedly occur in 4.81% ACDF procedures (range, 0%-32%) and in 9.89% posterior lateral mass screw procedures (range, 0%-20.3%). 29 -39 With posterior cervical cages placed into the facet joints, vascular complications associated with the vertebral artery are likely avoided because of the fact that ventral overadvancement into the foramen transversarium is prevented by abutment into the cephalad cervical pedicle.
Conclusions
The results of our systematic review suggest that tissue-sparing, posterior cervical fusion with interfacet cages may be considered a safe and effective surgical intervention in patients failing conservative management for cervical spondylotic disease. It would certainly be necessary to critically evaluate the literature when evaluating treatment options for cervical spondylotic disease in the determination of cases in which this technique may be best suited. Uniformly, the procedure well-exceeded MCID for all patient reported outcomes, and the complication profile is certainly promising when compared to more traditional cervical surgical procedures.
In select cases, this minimally invasive technique may result in positive clinical outcomes and high fusion rates, however, the level of evidence for the included studies must be not be understated. The limitations of the current study are inherent to those of systematic reviews—the quality of the review is directly proportional to the level of evidence of included studies. The lack of a control and comparison arm in the majority of available studies is a significant limitation of the current review. While there are a number of studies evaluating more traditional, open approaches, the data available on this technique is fairly limited. The heterogeneous nature of the studies reviewed limits generalizability and more pivotal, controlled and comparative studies are required before assessment may be considered definitive, and the technique is widely adopted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Dr Joseph Laratta reports personal fees for consultancy from Spineart, Evolution Spine, and Gerson Lehrman Group, royalties from Spineart and Evolution Spine, intellectual property with Combination Biologic and ICBG/BMAC system, grants from Medtronic, NuVasive, Orthopaedic Science Research Foundation, Orthopaedic Research and Education Foundation, personal fees for travel expenses/meeting accommodations from American Institute of Minimally Invasive Surgery (AIMIS), NuVasive, Stryker, K2M, and Fisher Owen Fund, and is on the editorial board for Spine, Global Spine Journal, and Journal of Spine Surgery. Dr William Smith reports personal fee for consultancy from NuVasive, Spineology, Pediguard, Providence, and Ortho Bio Design, grants from MDT, NuVasive, Providence, and Spineology, ownership interest in NuVasive, Pediguard, and SpineSmith, royalty from NuVasive and Spineology, and is on the speakers’ bureau for NuVasive and Pediguard.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.