
Abstract
Study Design:
In vitro cadaveric biomechanical study.
Objective:
To compare the biomechanics of integrated anchor and blade versus traditional screw fixation techniques for interbody fusion.
Methods:
Fifteen cadaveric cervical spines were divided into 3 equal groups (n = 5). Each spine was tested: intact, after discectomy (simulating an injury model), interbody spacer alone (S), integrated interbody spacer (iSA), and integrated spacer with lateral mass screw and rod fixation (LMS+iS). Each treatment group included integrated spacers with either screw, anchor, or blade integrated spacers. Constructs were tested in flexion-extension (FE), lateral bending (LB), and axial rotation (AR) under pure moments (±1.5 N m).
Results:
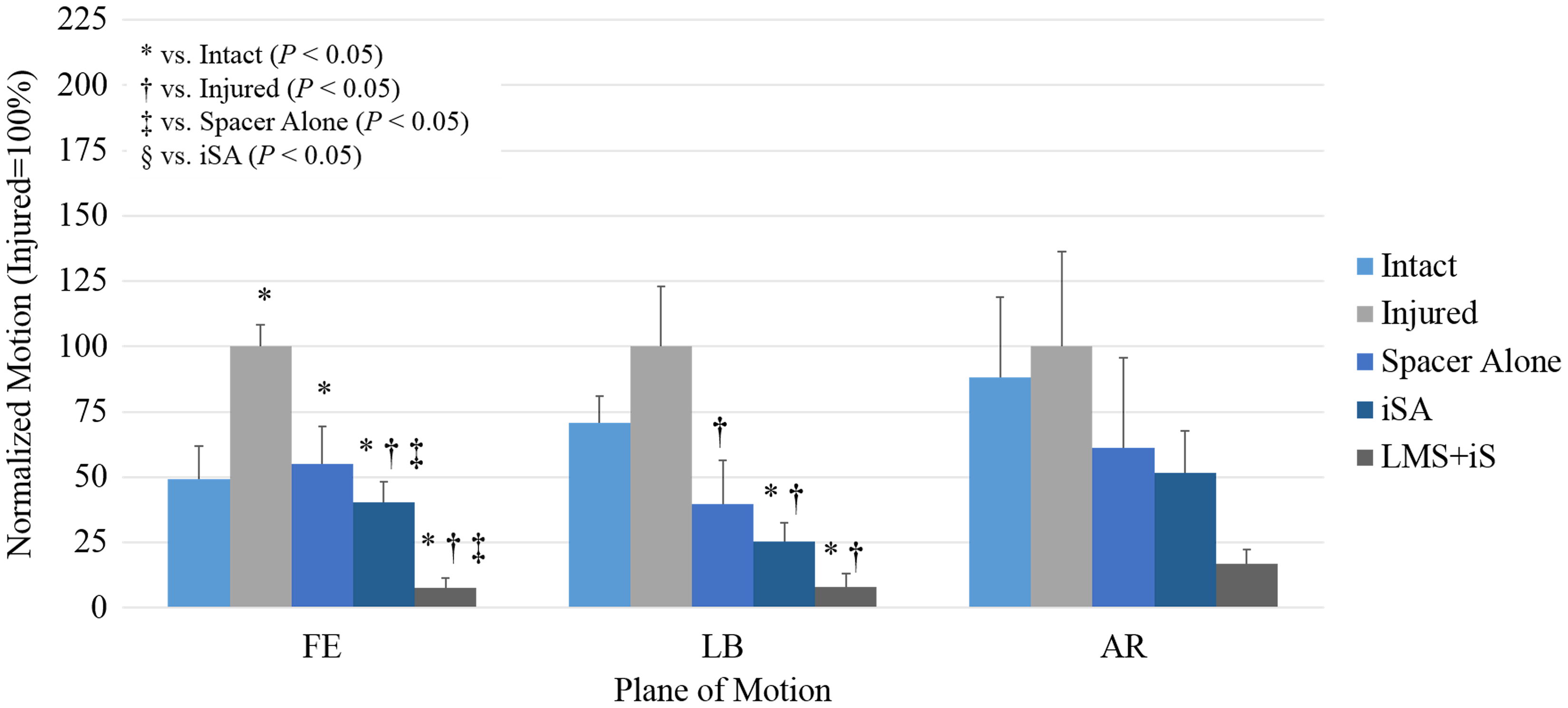
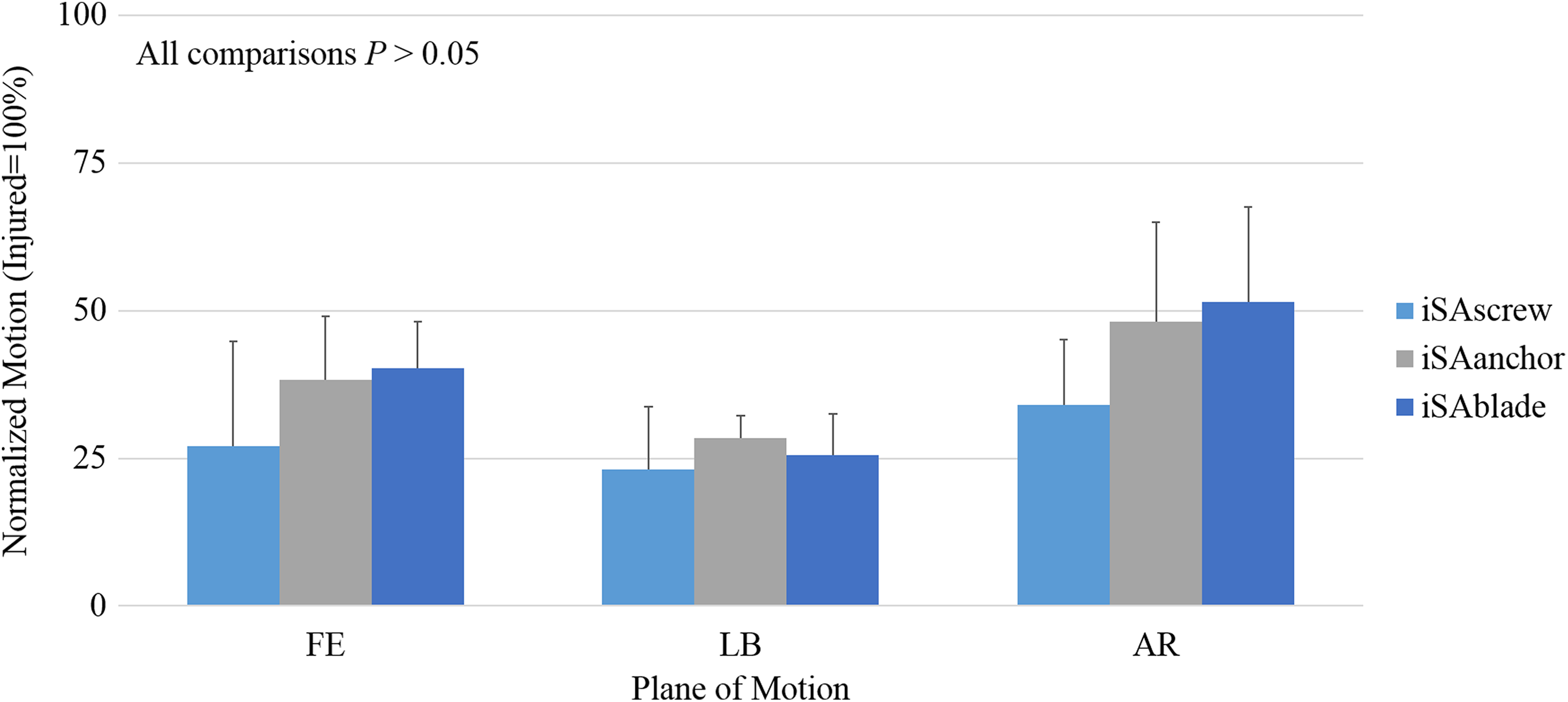
Across all 3 planes, the following range of motion trend was observed: Injured > Intact > S > iSA > LMS+iS. In FE and LB, integrated anchor and blade significantly decreased motion compared with intact and injured conditions, before and after supplemental posterior fixation (P < .05). Comparing tested devices revealed biomechanical equivalence between screw, anchor, and blade fixation methods in all loading modes (P > .05).
Conclusion:
All integrated interbody devices reduced intact and injured motion; lateral mass screws and rods further stabilized the single motion segment. Comparing screw, anchor, or bladed integrated anterior cervical discectomy and fusion spacers revealed no significant differences.
Keywords
Introduction
Anterior cervical discectomy and fusion (ACDF), with or without posterior fixation, is commonly performed to alleviate spondylotic myelopathy and radiculopathy, correct deformity, and restore spinal stability, resulting from traumatic subaxial cervical injury or disc degeneration. 1 -3 Modern low-profile integrated cervical interbody fusion devices include intervertebral body fixation, obviating the need for anterior plating and reducing plate-related complications such as tracheal-esophageal trauma, 4 –6 postoperative dysphagia, 7,8 and adjacent segment degeneration. 7,9 –11 Intervertebral screws remain the gold standard for bone fixation; however, tissue distraction and the cephalad-caudal angulation of the screws may be impeded by soft tissue as well as bony anatomy such as the mandible (at C2-C3) or the sternoclavicular joint (at C6-C7).
Alternatively, novel curved fixation methods have been designed to eliminate cephalad-caudal angulation limitations through an approach inline with the operative disc, thereby minimizing the surgical corridor and the need for periosteal stripping, intraosseous drilling, and/or osteophytectomy for ACDF construction. 12 Commercially available integrated interbody spacers devices include blade fixation (ROI-C with VerteBRIDGE blade fixation, Zimmer Biomet, Warsaw, IN) or anchor fixation (COALITION MIS, Globus Medical, Inc, Audubon, PA; Acapella One, Exactech, Inc, Gainesville, FL; and Aero-C, Stryker, Inc, Kalamazoo, MI). Although extensive biomechanical literature describes integrated screw interbody spacer systems in comparison to anterior plating or posterior fixation options, 13 –17 no in vitro characterization of intervertebral blade or anchor fixation has been reported to our knowledge.
The goal of this study was to quantify stabilization characteristics of 2 uniquely integrated spacer designs before and after posterior fixation. The authors hypothesized that (1) integrated spacers provide stability comparable to circumferential reconstruction and (2) the anchor or blade design offers fixation equivalent to the 2-screw standard integrated device (Figure 1).
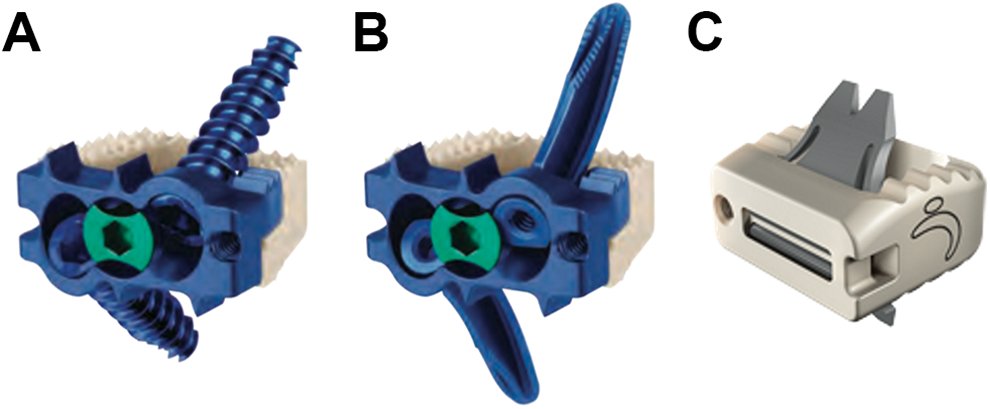
Representative image of tested inline ACDF devices with (A) screw, (B) anchor, and (C) blade intervertebral fixation methods.
Materials and Methods
Specimen Preparation
Investigators used 15 fresh frozen cadaver spines from C2-C7, with the treated level at C5-C6. The medical history of each donor was reviewed to exclude specimens with spinal trauma, malignancy, deformity, or fracture that would otherwise affect the outcome of the test. Standard anteroposterior and lateral plain films were obtained to evaluate the presence of osseous pathology. Cervical spines were thawed to room temperature and were carefully denuded, leaving only ligaments, bones, and intervertebral discs of desired segments. Dual-energy X-ray absorptiometry scans were obtained with a Lunar Prodigy Scanner 8743 (GE Medical Systems, Madison, WI) to evaluate bone mineral density (BMD; g/cm2) according to a water-bathe protocol 18 for the cervical segment in the coronal plane. Specimens were potted at C2 proximally and at C7 distally in a 1:1 mixture of Bondo auto filler (Bondo MarHyde Corp, Atlanta, GA) and fiberglass resin (Home-Solution All Purpose, Bondo MarHyde Corp). All specimens were double-wrapped in plastic bags and were stored at −20°C until testing. Specimens were sprayed with saline (0.9%) throughout testing to preserve viscoelastic properties of the discs and ligamentous structures.
Surgical Constructs
A total of 15 specimens were divided into 3 equal groups (n = 5) such that the average BMD was similar between groups, and were instrumented at C5-C6. All specimens were selected based on vertebral body width and depth, and C5-C6 intervertebral disc height due to limited availability of ACDF devices. All interbody spacers possessed a 12 × 14 mm footprint and 7° of lordosis. Spacer heights (either 5 mm or 6 mm) were selected such that 1 mm of distraction was achieved following insertion. Tested implants included an interbody spacer, and 3.5-mm-diameter titanium (Ti) polyaxial lateral mass screws (LMS) with 3.5-mm-diameter Ti rods (ELLIPSE, Globus Medical, Inc). Integrated polyether-ether-ketone (PEEK) spacers tested included a (1) zero-profile, box-shaped PEEK spacer with integrated plate (12 × 14 mm footprint) and 2 3.6-mm-diameter interbody screws (Sscrew) (COALITION MIS, Globus Medical, Inc); (2) the same spacer-plate system (12 × 14 mm footprint) and 2 curved, 3.7-mm-diameter 3-ridged interbody anchors (Sanchor); and (3) zero-profile, box-shaped PEEK-only spacer (12 × 14 mm footprint) and 2 8.1-mm wide, 9.8-mm long, curved, self-locking blades (Sblade) (ROI-C with VerteBRIDGE blade, Zimmer Biomet), as shown in Figure 1A to C, respectively. Intervertebral screw, anchor, or blade lengths were determined by spacer dimensions, as recommend by each manufacturer. Sscrew constructs were instrumented with either 12 mm or 14 mm long screws to maximize fixation, yet avoid anchoring or penetrating the posterior cortical shell that would otherwise bias kinematic results. Alternatively, Sanchor and Sblade constructs were instrumented with 12 mm long anchors or 9.8 mm long blades, selected in accordance to the height of the implant being used to avoid penetration of the endplates with the curvilinear intervertebral fixation.
Four trained surgeons and a single laboratory researcher were tasked with performing the discectomy and insertion of the ACDF device. All individuals participated in the reconstruction for each technique. The anterior cervical discectomy technique was standardized across all specimens, in accordance with Brigham and Tsahakis. 19 A No. 15 scalpel was used to incise a box outlining the dimensions of the ACDF device. The anterolateral annulus was not resected bilaterally to the uncinated process to avoid traumatic disarticulation of the cervical spine during kinematic testing. Lekscell rongeurs, pituitary tools, and angled Brun curettes were used to remove the complete nucleus pulposus. A high-speed burr with 3 mm side cutting drill bit was used to remove the cartilaginous endplates, and deepen the inferior posterior corners for the rectangular interbody device (when necessary); the cortical vertebral endplates were maintained during the burring process. No specimens used in the study had osteophytes and did not require additional carpentry of the disc space.
The present study aimed to compare novel anchor or blade fixation versus traditional screw fixation techniques used for interbody fusion. Integrated spacers were tested in separate groups to prevent compromise of the bone due to potentially overlapping trajectories. In each treatment group, the following constructs were tested: (1) intact, (2) after discectomy (simulating an injury model), (3) interbody spacer alone (S), (4) integrated interbody spacer (iSA), and (5) integrated spacer with lateral mass screw and rod fixation (LMS+iS). Representative sagittal and coronal radiographic images of lateral mass screws with an integrated spacer (LMS+iS) for each treatment group are shown in Figure 2.
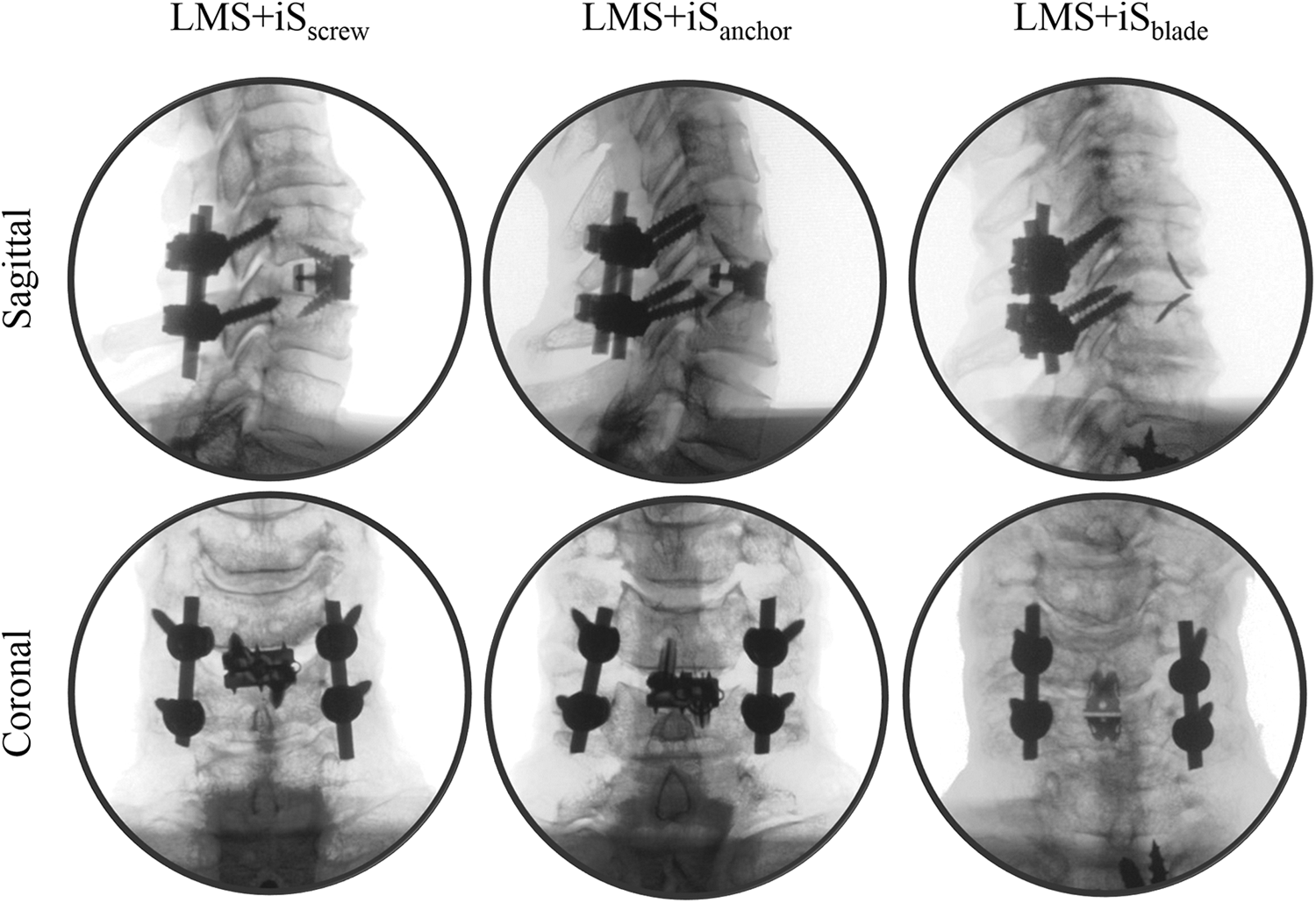
Representative sagittal and coronal radiographs of investigated anterior cervical devices with supplemental fixation.
Biomechanical Testing
Each specimen was thawed overnight and was affixed to a custom 6-degrees-of-freedom (6DOF) motion simulator for range of motion (ROM) testing, as described in the literature, 20 and modeled after the spinal loading simulator proposed by Wilke et al. 21 The cranial (C2) and caudal (C7) portion of the specimen were affixed to a 6DOF motor gimbal assembly, which applied a pure, unconstrained rotational moment independently about the x-, y-, and z-axis corresponding to flexion-extension (FE), lateral bending (LB), and axial rotation (AR). The gimbal assembly is attached to the test platform, which includes linear air-bearing guide rails (x- and z-axis) and pneumatic-controlled linear actuator (y-axis) enabling pure, unconstrained translation. A load control protocol with servomotors will apply a pure, unconstrained bending moment, caudally, at a rate of 1.5°/s, to a maximum moment of ±1.5 N m. 22 Data was collected during the third cycle to minimize the viscoelastic behavior of the tissues.
Plexiglass markers, each with 3 infrared light-emitting diodes, were secured rigidly to C2, C4, C5, C6, and C7 vertebral bodies via bone screws to track motion, and the motion analysis system (Optotrak Certus, Northern Digital, Inc, Waterloo, Ontario, Canada) was placed approximately 6 feet in front of the specimen. Markers denoting a rigid body were aligned along the sagittal curvature of the spine. Optotrak Certus software superimposed the coordinate systems of 2 adjacent vertebral bodies to inferentially determine relative Eulerian rotations in each of the 3 planes, with accuracy of 0.1 mm and resolution of 0.01 mm. 23 Range of motion reported across C5-C6 was normalized to the average injured condition, per group, to determine how each ACDF device stabilizes a simulated collapsed disc. All constructs of each specimen, per treatment group (Sscrew, Sanchor, or Sblade), were normalized to the average injured condition in FE, LB, and AR. The following equation was used: Specimennormalized = [Specimenraw/∑Treatmentraw, injured] × 100.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics (SPSS v22, IBM Corp, Armonk, NY). Following verification of normality of the data using a Shapiro-Wilk test across treatment groups, tested constructs, and planes of motion (Table 1), one-way analysis of variance (ANOVA) with repeated measures and Bonferroni post hoc analysis were performed to discern differences in stability between all tested constructs within each treatment group. 24 Additionally, an independent ANOVA and Bonferroni post hoc analysis was performed to (1) identify differences between raw injured motion that would otherwise bias the normalized results and (2) elucidate differences between ACDF fixation methods. 24 Significance was defined as P < .05.
P Values of Shapiro-Wilk Test of Normality.
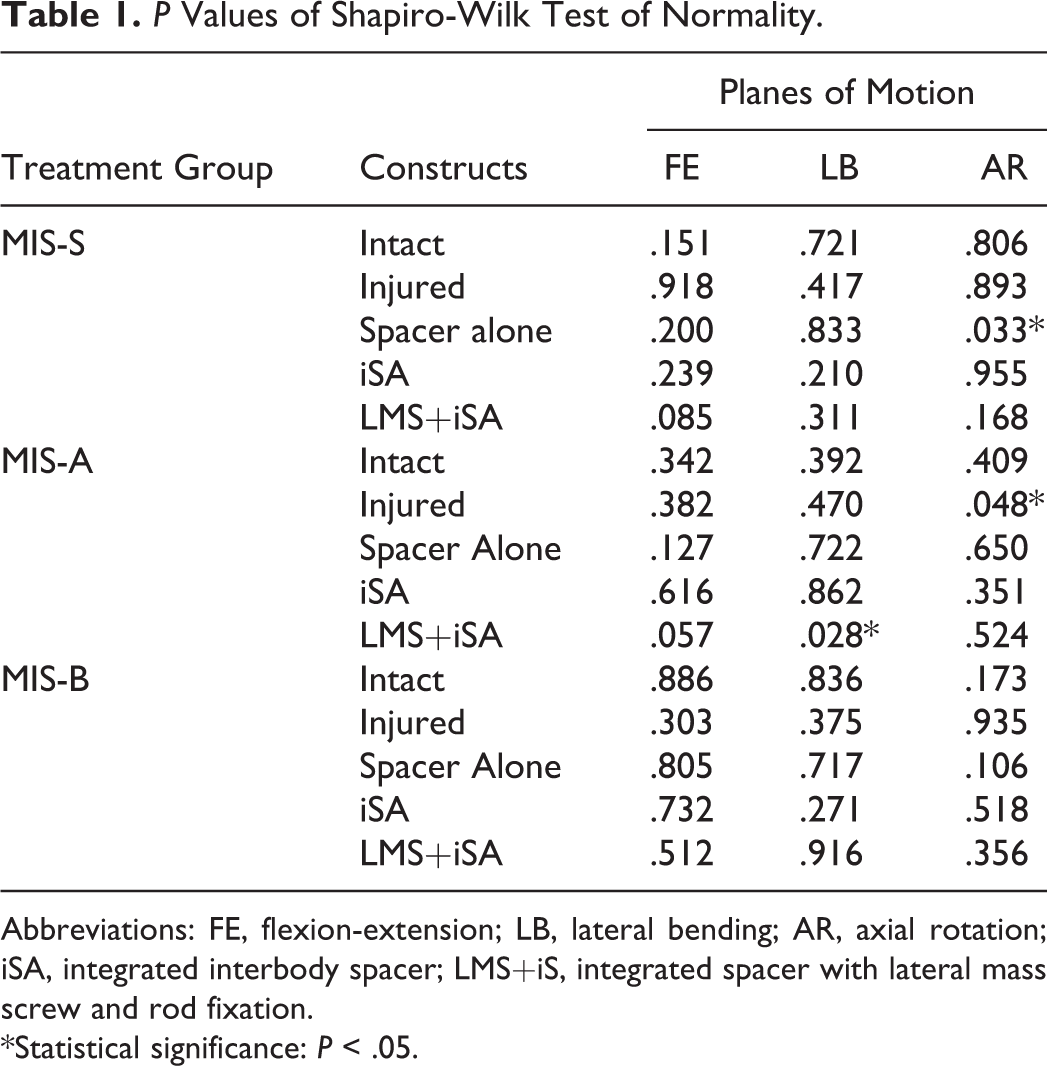
Abbreviations: FE, flexion-extension; LB, lateral bending; AR, axial rotation; iSA, integrated interbody spacer; LMS+iS, integrated spacer with lateral mass screw and rod fixation.
*Statistical significance: P < .05.
Results
P values achieved for the Shapiro-Wilk test across treatment groups, constructs, and planes of motion are presented in Table 1. A summary of treatment group demographics and BMD are presented in Table 2. No significant differences in age and BMD between treatment groups was observed (P = .774 and P = .686, respectively). Raw and normalized ROM (Tables 3 and 4), ROM normalized to the average injured condition with significant relationships (Figures 3 –6), and P values achieved for all constructs within treatment groups (Tables 5 –7) are presented. Comparisons of baseline injury values between treatment groups did not find significant differences between Sscrew, Sanchor, and Sblade groups in FE, LB, and AR (all P = 1.000).
Cadaveric Specimen Demographics (C2-C7) (Average ± SD).
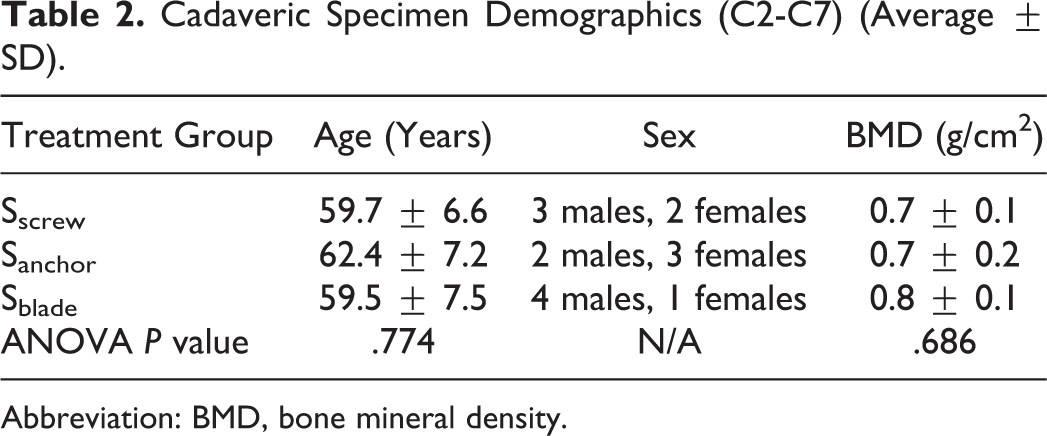
Abbreviation: BMD, bone mineral density.
Raw C5-C6 Motion, ° (Average ± SD).
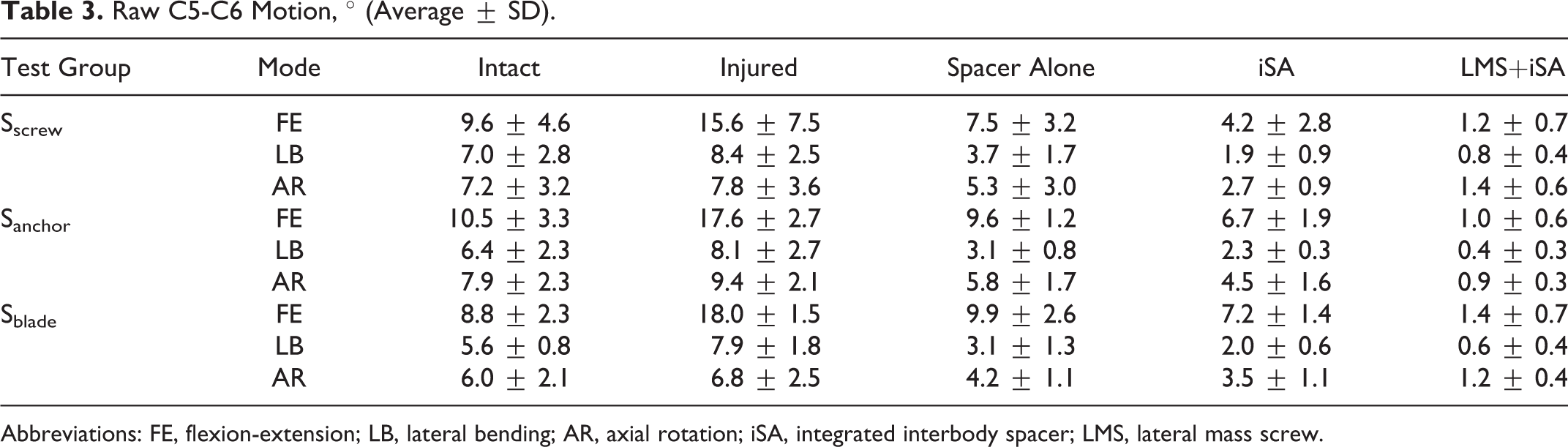
Abbreviations: FE, flexion-extension; LB, lateral bending; AR, axial rotation; iSA, integrated interbody spacer; LMS, lateral mass screw.
Normalized C5-C6 motion, % (Average ± SD).
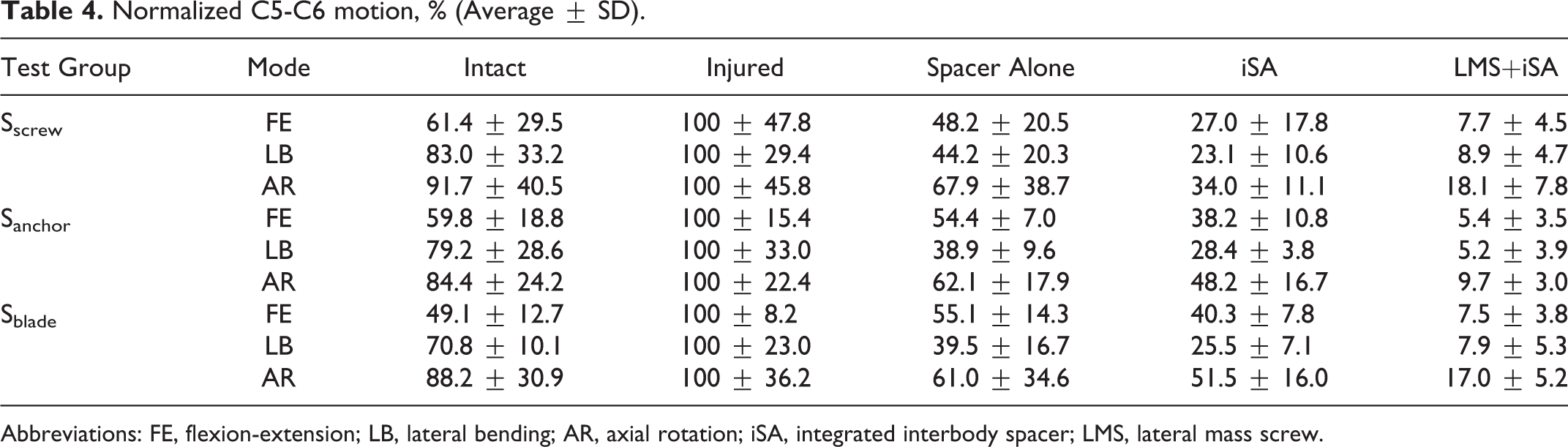
Abbreviations: FE, flexion-extension; LB, lateral bending; AR, axial rotation; iSA, integrated interbody spacer; LMS, lateral mass screw.
Range of motion at C5-C6 for integrated screw (Sscrew) treatment group.
Range of motion at C5-C6 for integrated anchor (Sanchor) treatment group.
Range of motion at C5-C6 for integrated blade (Sblade) treatment group.
Range of motion at C5-C6 for integrated spacers prior to application of supplemental fixation.
Sscrew: P Values of ANOVA.
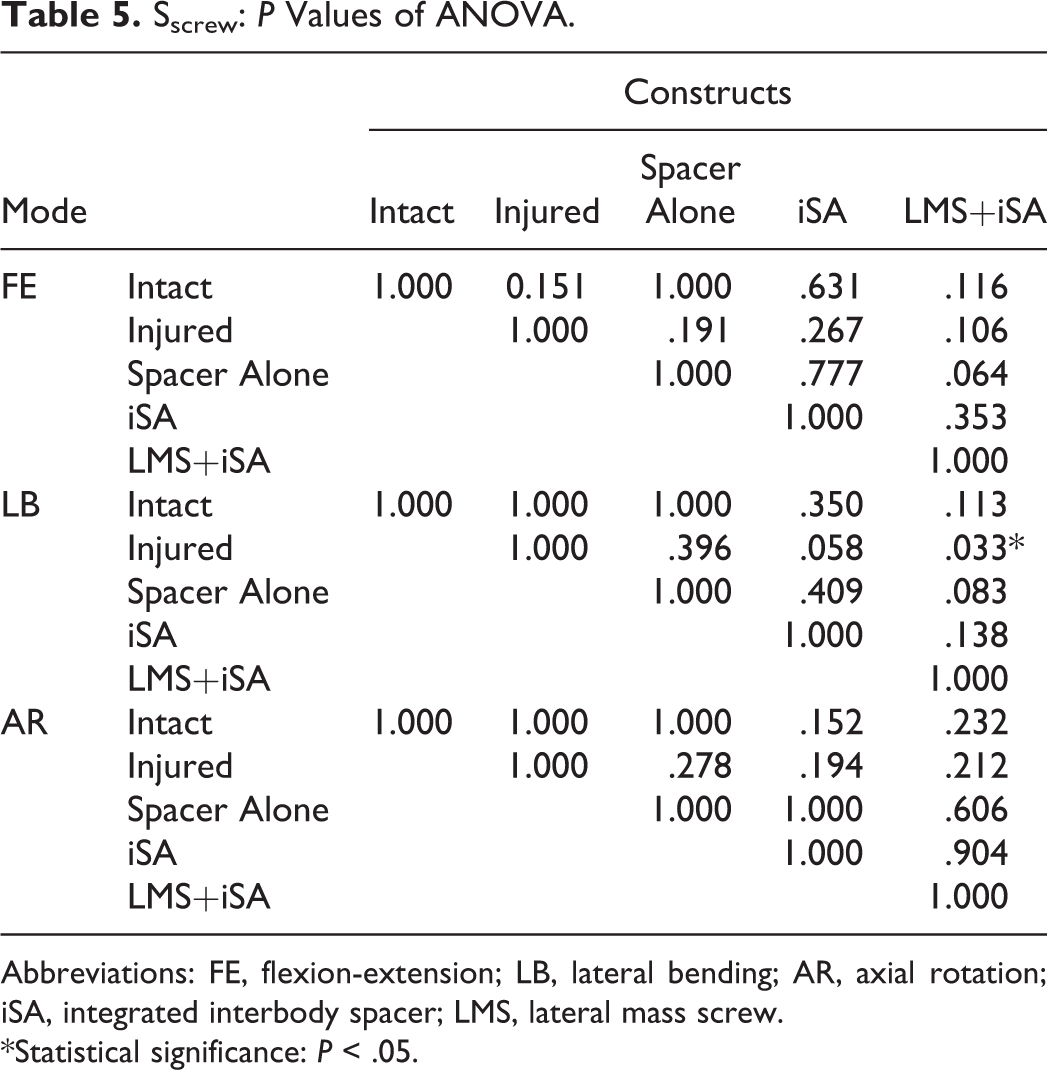
Abbreviations: FE, flexion-extension; LB, lateral bending; AR, axial rotation; iSA, integrated interbody spacer; LMS, lateral mass screw.
*Statistical significance: P < .05.
Sanchor: P Values of ANOVA.
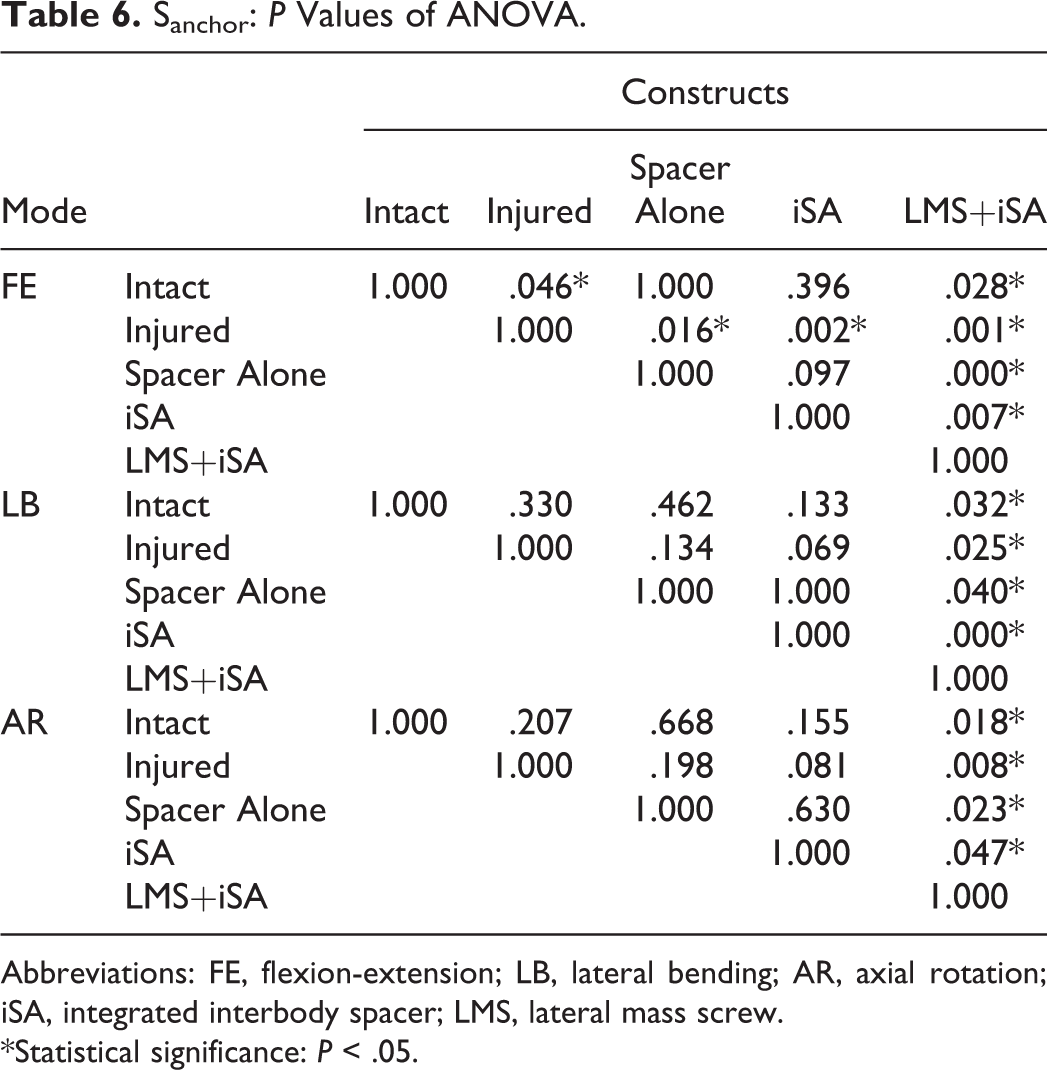
Abbreviations: FE, flexion-extension; LB, lateral bending; AR, axial rotation; iSA, integrated interbody spacer; LMS, lateral mass screw.
*Statistical significance: P < .05.
Sblade: P Values of ANOVA.
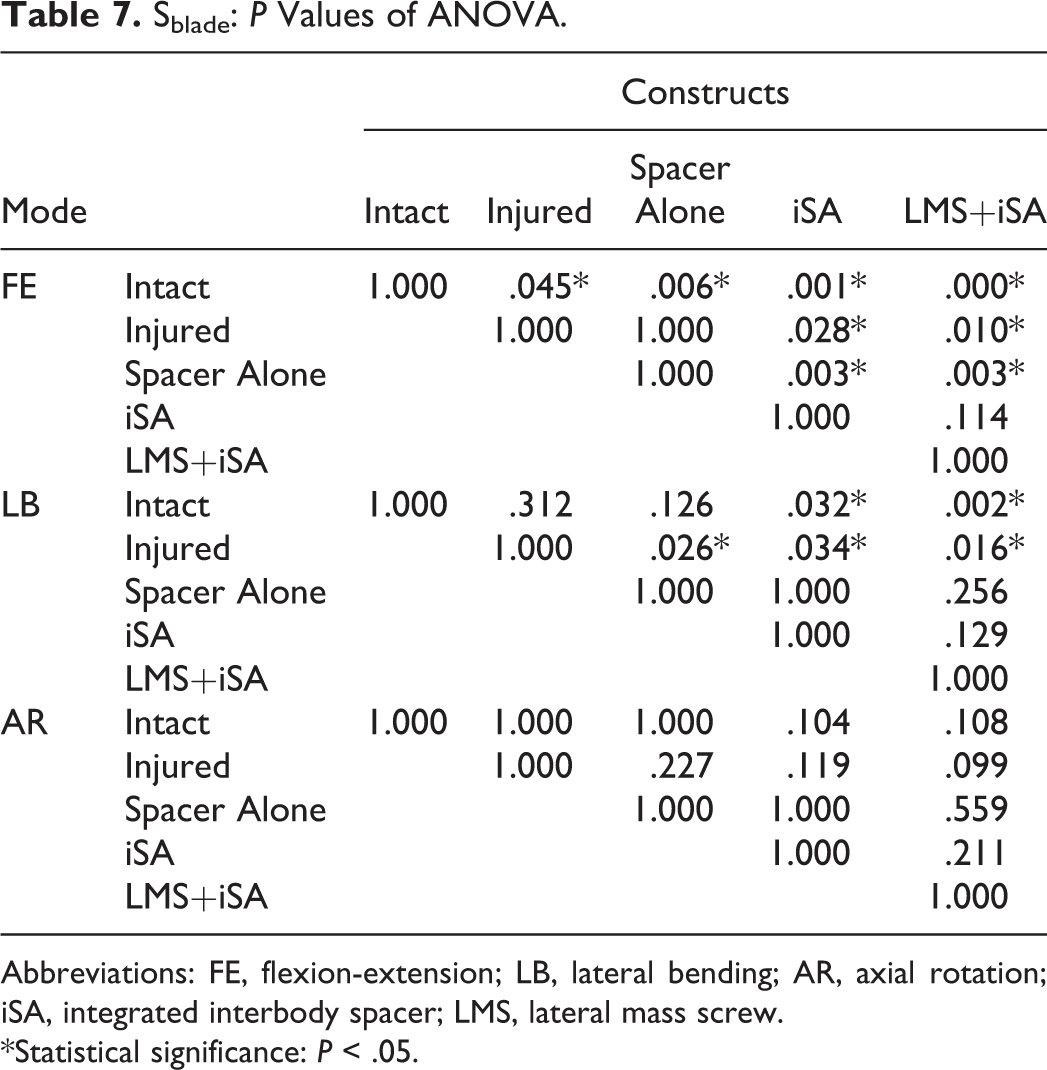
Abbreviations: FE, flexion-extension; LB, lateral bending; AR, axial rotation; iSA, integrated interbody spacer; LMS, lateral mass screw.
*Statistical significance: P < .05.
Traditional ACDF with Screw Fixation
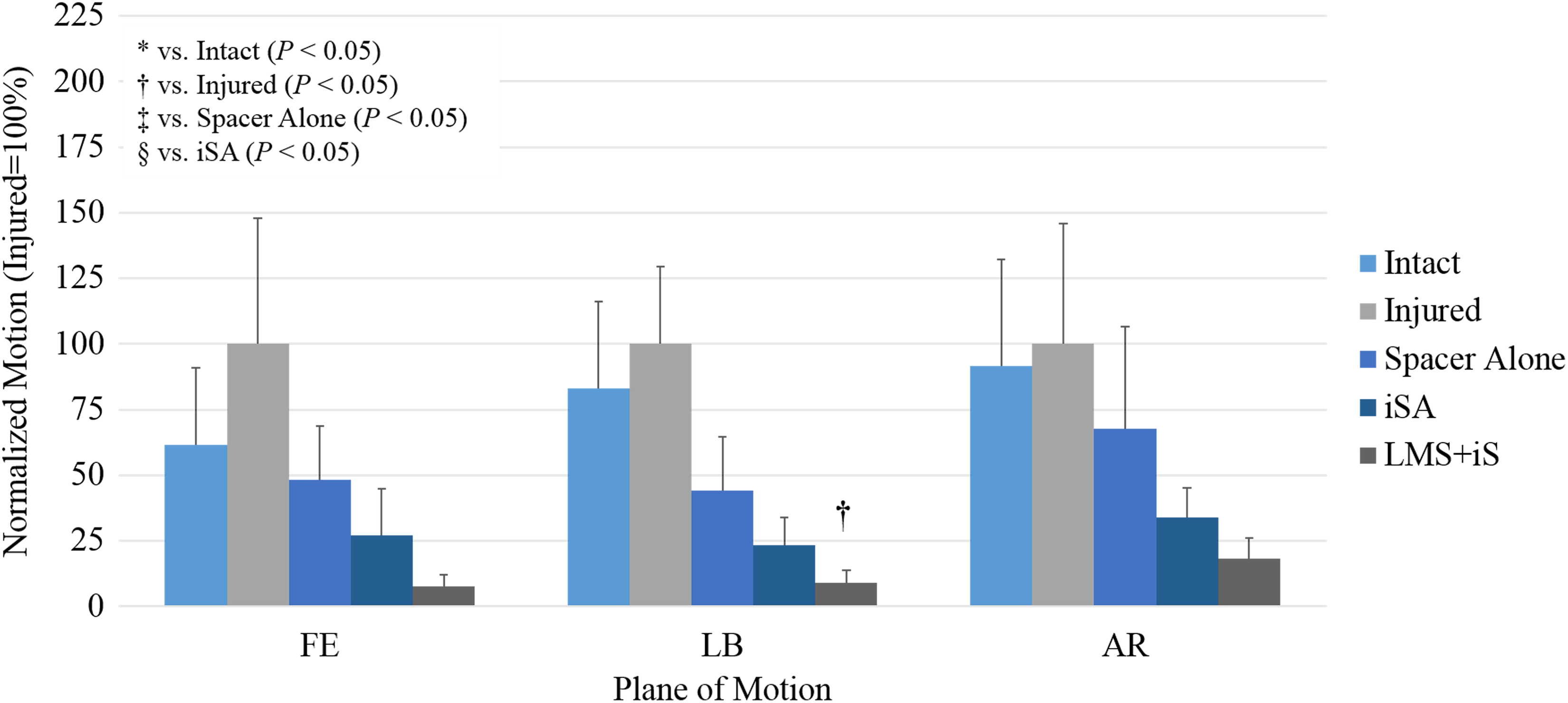
The average age of cadaveric specimens instrumented with Sscrew was 59.7 ± 6.6 years of age (3 males, 2 females) with an average BMD of 0.7 ± 0.1 g/cm2. Raw ROM is shown in Table 3. Range of motion was normalized to injured for all constructs tested (Table 4); significant differences are shown in Figure 3. In all 3 planes, the general trend was observed: Injured > Intact > Spacer Alone > iSA > LMS+iS. Bilateral lateral mass screws in combination with an integrated spacer provided the most rigid fixation in FE, LB, and AR (7.7%, 8.9%, 18.1%, respectively); only in LB did LMS+iS significantly reduced ROM compared to the injury model (8.9% vs 100%; P = .033). No other statistically significant differences were observed (P > .05).
Novel ACDF With Inline Anchor Fixation
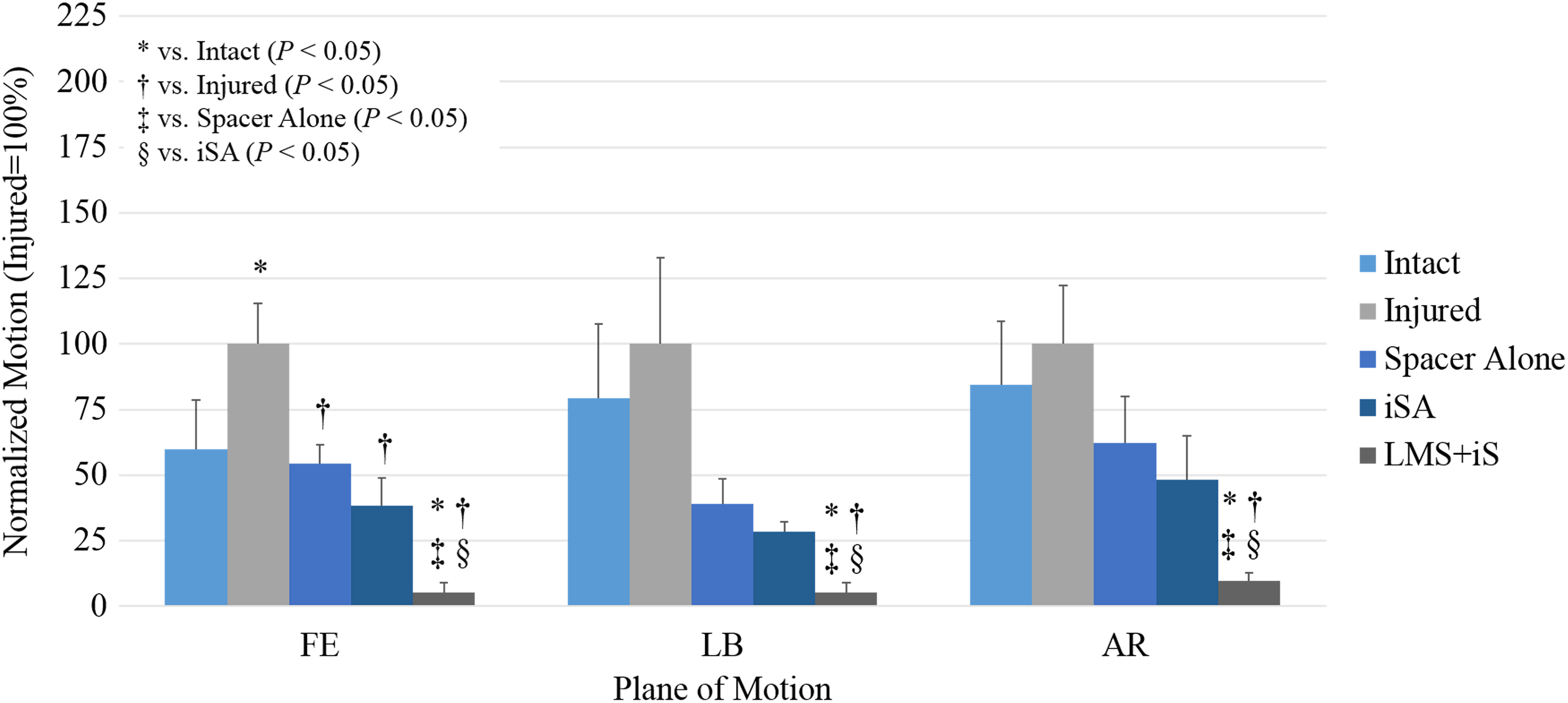
The average age of cadaveric specimens instrumented with Sanchor was 62.4 ± 7.2 years of age (2 males, 3 females) with an average BMD of 0.7 ± 0.2 g/cm2. Raw ROM is shown in Table 3. Range of motion was normalized to injured for all constructs tested (Table 4); significant differences are shown in Figure 4. In all 3 planes, the general trend was observed: Injured > Intact > Spacer Alone > iSA > LMS+iS. In FE, the injury model significantly increased motion compared with intact (100% vs 59.8%; P = .049). Additionally, both spacer alone (54.4%) and iSA (38.2%) constructs significantly reduced motion relative to injured (P = .016 and P = .002, respectively). Lateral mass screws in combination with an integrated spacer provided the largest motion decrease in FE (5.4%); significantly reducing motion compared with intact, injured, S, and iSA (59.8%, P = .028; 100%, P = .001; 54.4%, P = .000; and 38.2%, P = .007, respectively). In LB, LMS+iS (5.2%) significantly reduced motion compared with intact, injured, S, and iSA (79.2%, P = .032; 100%, P = .025; 38.9%, P = .040; and 28.4%, P = .000, respectively). Last, in AR, LMS+iS (9.7%) significantly reduced motion compared with intact, injured, S, and iSA (84.4%, P = .018; 100%, P = .008; 62.1%, P = .023; and 48.2%, P = .047, respectively). No other statistically significant differences were observed (P > .05).
Novel ACDF With Inline Blade Fixation
The average age of cadaveric specimens instrumented with Sblade was 59.5 ± 7.5 years of age (4 males, 1 female) with an average BMD of 0.8 ± 0.1 g/cm2. Raw ROM is shown in Table 3. ROM was normalized to injured for all constructs tested (Table 4); significant differences are shown in Figure 5. Again, in all 3 planes, the general trend was observed: Injured > Intact > Spacer Alone > iSA > LMS+iS. In FE, the injured model significantly increased motion compared with intact (49.1% vs 100%, P = .045). Additionally, S, iSA, and LMS+iS operative constructs significantly reduced motion relative to intact (55.1%, P = .006; 40.3%, P = .001; and 7.5%, P = .000, respectively). Furthermore, both iSA and LMS+iS reconstruction significantly stabilized the operative level in comparison to spacer-alone (S) (P = .003 and P = .003, respectively). In LB, S, iSA, and LMS+iS, operative constructs significantly reduced motion relative to injured (100%) (39.5%, P = .026; 25.5%, P = .034; and 7.9%, P = .016, respectively); only iSA and LMS+iS significantly stabilized the segment in comparison to intact (70.7%) (P = .032 and P = .002, respectively). No other statistically significant differences were observed (P > .05).
Integrated Spacer Device Comparisons
Motion of integrated spacers prior to application of supplemental fixation, normalized to the average injured condition, is presented in Figure 6. No statistically significant differences were found in all planes of motion (P > .05). Intervertebral screw fixation provided the greatest stability in FE, LB, and AR (27.0%, 23.1%, and 34.0%, respectively). In FE, LB, and AR, iSAanchor near identical fixation compared with iSAblade (38.2% vs 40.3%, P = 1.000; 25.5% vs 28.4%, P = 1.000; and 48.2% vs 51.5%, P = 1.000, respectively).
Discussion
Anterior cervical discectomy with fusion using anterior plating has been used for multiple pathologies of the cervical spine. 3,8,11,12,25 Meta-analyses of traditional plate and spacer ACDF conducted by Tabaraee et al 12 and Fraser and Härtl 26 revealed single-level arthrodesis rates of 92.6% and 97.1%, respectively. Despite high reported fusion rates, anterior plating, similar to the effect of spondylotic osteophytes, 27 can affect movement of the pharynx or esophagus along the cervical spine, leading to persistent plate-related complications such as tracheal-esophageal trauma, 4 –6 postoperative dysphagia, 7,8 and adjacent segment degeneration. 7,9 –11
Advances in device design have produced low-profile, integrated cervical interbody spacers to mitigate the complications associated with the use of rigid anterior plating superficial to the symptomatic disc space by reducing the surgical corridor and the need for periosteal stripping, intraosseous drilling, and osteophytectomy. 12 Cadaveric analyses by Majid et al 13 and Stein et al 16 found kinematic equivalence between a single-level integrated interbody spacer with intervertebral screw fixation and plate-spacer ACDF construction in the absence of posterior fixation. Clinically, the use of integrated interbody fusion devices is associated with lower rates of short- and long-term dysphagia, 28 –30 less time for operation, 12,28 diminished operative blood loss, 12,28 reduced length of hospitalization, 12 lower levels of adjacent ossification, 31 and better outcomes as assessed through Japanese Orthopedic Association (JOA) 28 /visual analogue scale 25,30 scores, with reported arthrodesis rates between 92.6% and 98.1%. 12,25,32 –34
Despite technological advances, implantation of modern, integrated cervical interbody devices may be complicated by oblique or challenging cephalad-caudal screw trajectories due to both soft tissue as well as bony anatomy such as the mandible (at C2-C3) or sternoclavicular joint (at C6-C7). Next generation of integrated devices have been designed to accommodate preassembled, self-guided blades or anchors in line with the treated disc, thereby reducing the surgical corridor in comparison to traditional cervical plate or integrated devices instrumented with screws. Use of low-profile instruments in line with the disc space aim to reduce interference with the mandible or sternoclavicular joint at cephalad and caudal levels of the cervical spine. Furthermore, the reduced operative corridor limits periosteal striping and intraosseous drilling, which may help minimize tissue disruption.
Grasso et al 35 were first to provide prospective analyses of next-generation interbody fusion with inline bladed fixation in a single-level treatment of myelopathy and radiculopathy (n = 32 cases), reporting satisfactory fusion rates (100%), and significant increases in intervertebral height (from 4.1 ± 0.7 to 6 ± 0.3 mm) and Cobb angle (from 12.2 ± 4.3° to 21.1 ± 4.1°) at 24-month follow-up (P < .05). Comparisons of inline interbody fusion to traditional spacer and plate construction by Hofstetter et al 36 (n = 70 cases) found that inline devices significantly reduced estimated blood loss (53.8 ± 4.3 vs 103.3 ± 22.3 mL) and dysphagia persisting beyond 3 months (2.9% vs 20%; P < .05). While both integrated spacers and spacer-plate interbody fusion significantly improved JOA scores following surgery, only interbody devices with intervertebral fixation inserted inline to the disc space reduced neurological impairment assessed using the Nurick score (P < .05). Similarly, single-level retrospective analyses by Wang et al 37 (n = 63 cases) found similar clinical outcomes between inline integrated devices with blade fixation and ACDF spacer-plate techniques, noting that integrated interbody fixation inline with the disc space was associated with a lower risk of postoperative dysphagia (0% vs 27.3%), shorter operation time (80.4 ± 12.1 minutes vs 108.7 ± 22.8 minutes), less blood loss (56.8 ± 19.0 mL vs 89.4 ± 29.7 mL), and overall “greater simplicity.”
Despite promising short-term clinical outcomes of inline integrated interbody fusion, to the authors’ knowledge, only one study to date has evaluated characterized stability provided by alternative intervertebral fixation methods. Bucci et al 38 supplement their investigation of fusion status, postoperative complications, and patient reported outcomes of ROI-C with VerteBRIDGE blade with preclinical segmental ROM of 2 cervical spines (C2-C3, C4-C5, and C6-C7; n = 6 segments). The authors report average intact motion of 12.9°, 9.7°, and 10.3° in FE, LB, and AR, respectively; the iSAblade construct significantly reduced motion to 6.6°, 3.8°, and 5.5° (P < .05). Alternatively, the present study observed an average intact motion of 8.8°, 5.6°, and 6.0° in FE, LB, and AR, respectively; the iSAblade construct reduced motion to 7.2°, 2.0°, and 3.5° in FE, LB, and AR, respectively.
Direct comparisons between the 2 studies are difficult due to different testing methodologies. The present study design and technical aspects of biomechanical testing are in compliance with in vitro stability testing of spinal implants guidelines as defined by Wilke et al 21 including use of a spinal loading simulator able to move freely in all 6 degrees of freedom and use of specimens with at least one free segment on either end of the construct length. Bucci et al 38 tested single segments on a uniaxial hydraulic spinal loading system, with a 20 N axial preload to maintain compression.
The present study sought to characterize the aforementioned blade and anchor fixation designs and traditional bone screws through a single-level, in vitro kinematic protocol. In all 3 fixation groups, across all planes of motion, the following trend was observed: Injured > Intact > Spacer Alone > iSA > LMS+iS. Integrated interbody fusion with screws did not significantly reduce motion compared to intact or injured (P > .05); only in LB did LMS+iSscrew significantly decrease motion in comparison to injured (P < .05). The use of anchors (iSAanchor) significantly reduced motion in comparison to injured in FE; LMS+iSscrew significantly decreased motion compared to injured in all planes (P < .05). Integrated implants with blades (iSAblade) significantly reduced motion in comparison to intact and injured in FE and AR (P < .05); the addition of LMS did not significantly stabilize the spine (P < .05). While general trends were observed, broad significant differences in motion with the injured construct were observed for anchor and blade groups, but not the screw group, suggesting differences in the injured model. Additional ANOVA tests were performed to compare the raw injured motion between treatment groups. No statistical significance was observed between Sscrew, Sanchor, and Sblade groups in FE, LB, and AR (all P = 1.000), suggesting the discectomy is not the reason for broad statistical differences between groups. Similarities in motion of constructs, for instance, iSA, between treatment groups suggests that minute differences in standard deviations may contribute to the different statistical trends observed. Last, despite design differences between screw, anchor, and blade fixation, such differences did not lead to statistically significant differences in rigidity, both before and after posterior screws and rods. iSAscrew construction provided the greatest stabilization in FE, LB, and AR (27.0%, 23.1%, and 34.0%, respectively), yet only reduced motion compared with iSAanchor between 5.3% and 14.2% and iSAblade between 4% and 17.6%; the differences between anchor and blade fixation was negligible, ranging from 2.1% to 3.3% during the bending modes.
Integrated cervical spacers tested in the present study have distinct fixation differences that may affect their stability, stress shielding, and anterior-posterior load sharing. It is presently unknown how much stabilization is required for fusion to occur; however, Wolff’s Law states that load transmission through the bone graft is necessary for bone growth and remodeling. The in silica load-sharing investigation of a novel low-profile dynamic integrated cervical plate (InterPlate, RSB Spine, Cleveland, OH) with rotational- and translational-unconstrained screws, and lateral “wings” with teeth creating a partially enclosed bone graft chamber by Palepu et al 39 suggest the potential need for integrated plate-spacer systems with features such as (1) unconstrained intervertebral fixation and (2) titanium teeth to enable load sharing with the graft. Additionally, the implication of differences between unconstrained and static fixed devices on bone graft fusion further emphasizes the differences between the 2 unique interbody devices investigated in the present in vitro study.
The current study investigated 2 devices. The first interbody device tested included an integrated plate-spacer system with a box-shaped PEEK spacer and an integrated Ti plate featuring 3 superior and 3 inferior teeth to penetrate the cortical endplate; 2 rotationally unconstrained Ti screws (iSAscrew) or 3-ridge Ti anchors (iSAanchor) with a blocking-screw to prevent screw/anchor backout. The second interbody device included a convex box-shaped PEEK-only spacer with 2 static self-locking fixed curved Ti blades (iSAblade) projecting into the vertebral body.
Although minimal differences in motion were observed between spacers with unconstrained screw and anchor intervertebral fixation, and static blade fixation, further in vitro or in silica investigation will be needed to determine what effect these different device designs have on stress shielding and load sharing. Even further, multicenter studies are necessary to confirm the implications of device design, stress shielding, and load sharing on patient-reported outcomes, postoperative subsidence, and fusion rates. Initial in vitro analysis by Brodke et al 40 found that static cervical plating lost its ability to share load and limit motion following settling of the device. Clinical investigation by Saphier et al 41 observed significant improvements in patient pain and functionality metrics with use of a load-sharing cervical plate compared to a stress-shielding plating system (P < .05); the load-sharing system exhibited increased fusion rates (96% vs 92%) but was not significant. Nevertheless, it is unknown if these results extend to integrated interbody spacers.
Although the presented work successfully quantified the biomechanical efficacy of novel inline integrated interbody fusion devices aimed at eliminating oblique, challenging intervertebral screw trajectories, this study is not without limitations. First, captured motion data reflect only the immediate postoperative condition and do not account for patient factors such as bone healing and biomechanical features of the final fusion mass. It is within reason to expect the fusion bed formed across the anterior column would further augment the anterior-posterior loading dynamics of the construct. Anatomic differences between specimens could have affected results; however, all motion data was normalized to injured to limit this influence. Similar to other human cadaveric studies, the lack of availability and cost of specimens procured limited sample sizes for this study. Use of a larger sample size may reduce the likelihood of type I and type II errors. Finally, the results of the present study only speak to the biomechanical efficacy of novel inline fixation in a single-level construct, not their use in multi-level construction as recently introduced in literature.
Conclusions
Cadaveric biomechanical investigation found that integrated cervical interbody fusion devices and lateral mass screws offered the greatest stability, regardless of spacer and intervertebral fixation design. Comparison of commercially available screw, anchor, and bladed intervertebral fixation techniques revealed no significant differences in all 3 planes of motion, both before and after supplemental posterior fixation. Long-term multicenter studies of the presented integrated interbody fusion constructs are needed to determine the clinically relevant differences between techniques.
Footnotes
Authors’ Note
Anterior interbody spacer with intervertebral screws examined in this study (COALITION MIS, Globus Medical, Inc, Audubon, PA) is FDA cleared for use without lateral mass fixation; if anchors are employed, supplemental posterior fixation is required. Anterior interbody spacers with blade fixation is FDA cleared for use without lateral mass fixation (ROI-C with VerteBRIDGE blade, Zimmer Biomet, Warsaw, IN).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors would like to disclose that the study was performed at Globus Medical, Inc (GMI), using its 6-degrees-of-freedom motion simulator. Surgeons PMA, IC (Globus Medical—royalties, Nuvasive—royalties, Stryker Spine—consultant, SpinalCyte—stock, Spine Innovations—stock, Cytonics—stock, Spine Wave—royalties, SpineCraft—consultant), CZ, and BK have no conflict of interests related to the devices examined in this study; none were compensated for their efforts in the present study. Cadaveric specimens and related materials were provided by GMI, at which JAH, MM, and BSB are employees.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.