
Abstract
Study Design:
Anatomical study.
Objectives:
This study was conducted to determine the prevalence of abnormal lumbar vertebrae (4 and 6) and note any differences in pelvic incidence (PI) between spines with 4, 5, and 6 lumbar vertebrae.
Methods:
We screened 2980 dry cadaveric specimens from an osteological collection. Pelvises were reconstructed by articulating the sacra and innominate bones. PI was measured in all specimens via lateral photographs. L6-pelvic incidence (L6PI) was also measured, by articulating L6 to the sacrum and measuring PI from the superior aspect of the L6 vertebral body.
Results:
Of the specimens screened, 969 specimens were evaluated. Average age of death for all specimens was 50.4 ± 15.4 years. The prevalence of 6 lumbar vertebrae was 0.8% (n = 23), and the prevalence of 4 lumbar vertebrae was 1.8% (n = 54). PI measured 38.5° in specimens with 4 lumbar vertebrae, and 46.7° and 47.1° in specimens with 5 and 6 lumbar vertebrae, respectively. PI was significantly different between specimens with 4 and 5 lumbar vertebrae (P < .001) but not between specimens with 5 and 6 lumbar vertebrae (P = .38). For specimens with 6 lumbar vertebrae, when L6 was added to the sacrum, mean L6PI was 27.4°.
Conclusions:
In our large cadaveric study of full spines, we reported a lower prevalence of spines with 4 and 6 lumbar vertebrae compared to previous studies. PI was significantly decreased in subjects with 4 lumbar vertebrae compared with those with normal spines, and special caution should be taken when managing sagittal balance in these patients.
Introduction
Bipedal hominids have evolved to possess 5 lumbar vertebrae. However, the number of lumbar vertebrae has changed throughout evolutionary history. Cadaveric specimens from Old World monkeys consistently had 7 lumbar vertebrae and this number slowly decreased in their evolutionary successors, whose specimens demonstrated thoracization or sacralization of 1 or 2 lumbar vertebrae. 1 Although modern populations of Homo sapiens possess 5 lumbar vertebrae, an abnormal number—4 or 6—is still observed. 2 -7
While modern humans may have 4 or 6 lumbar vertebrae, the manner in which this anatomical aberration affects pelvic balance is unclear. Evolutionary data have suggested that the number of lumbar vertebrae was associated with the type of locomotion of that specific primate. 1,3 Similarly, a modern human with lumbar anomalies may unconsciously alter their locomotion to fit their anatomical profile. Studies to date on the impact of lumbar anomalies and clinical outcomes have focused primarily on lumbosacral transitional vertebrae (LSTV), given their relatively higher incidence. LSTV anomalies may be associated with lower back and gluteal pain 7,8 and even arthritic changes (BS Tucker, DS Weinberg, and RW Liu, unpublished data, 2018), implying that these anomalies do affect function. It is not known whether pelvic balance is affected.
In this study, we sought to determine the relationship between an abnormal number of lumbar vertebrae and the sagittal balance of the pelvis, measured by pelvic incidence (PI). Additionally, we sought to determine the prevalence of cadaveric spines with 4 or 6 lumbar vertebrae. To test the theory that patients with 6 lumbar vertebrae may have a normalized PI when calculated with the addition of L6 to the sacrum, we compared the PI with the addition of L6 in these specimens to specimens with 5 lumbar vertebrae.
Materials and Methods
A total of 2980 specimens were screened from the Hamann-Todd Human Osteological Collection at the Cleveland Museum of Natural History (Cleveland, OH). Specimens were excluded if there was significant bony wear or articular damage found in the sacra, innominate bones, or associated vertebrae that prevented re-articulation of the specimens.
The pelvis was reconstructed by articulating the sacrum with innominate bones and reinforced by a series of rubber bands (Figure 1A). A 12-mm piece of compressible foam was inserted as an artificial pubic symphysis, which has been verified in previous studies. 9 After each specimen was articulated, lateral photographs were obtained (Figure 1A). Two authors (MVA and JRT) measured PI independently in ImageJ 1.49v (National Institutes of Health, Bethesda, MD), using a previously validated method (Figure 1B). 9 To obtain the number of lumbar vertebrae for each specimen, all 2980 cadavers’ vertebrae were screened 3 times. Vertebrae were counted from C1 caudally, with the assumption of 7 cervical and 12 thoracic vertebrae. 10 Attention was given to the presence or absence of costal facets in determining thoracic vertebrae. 10
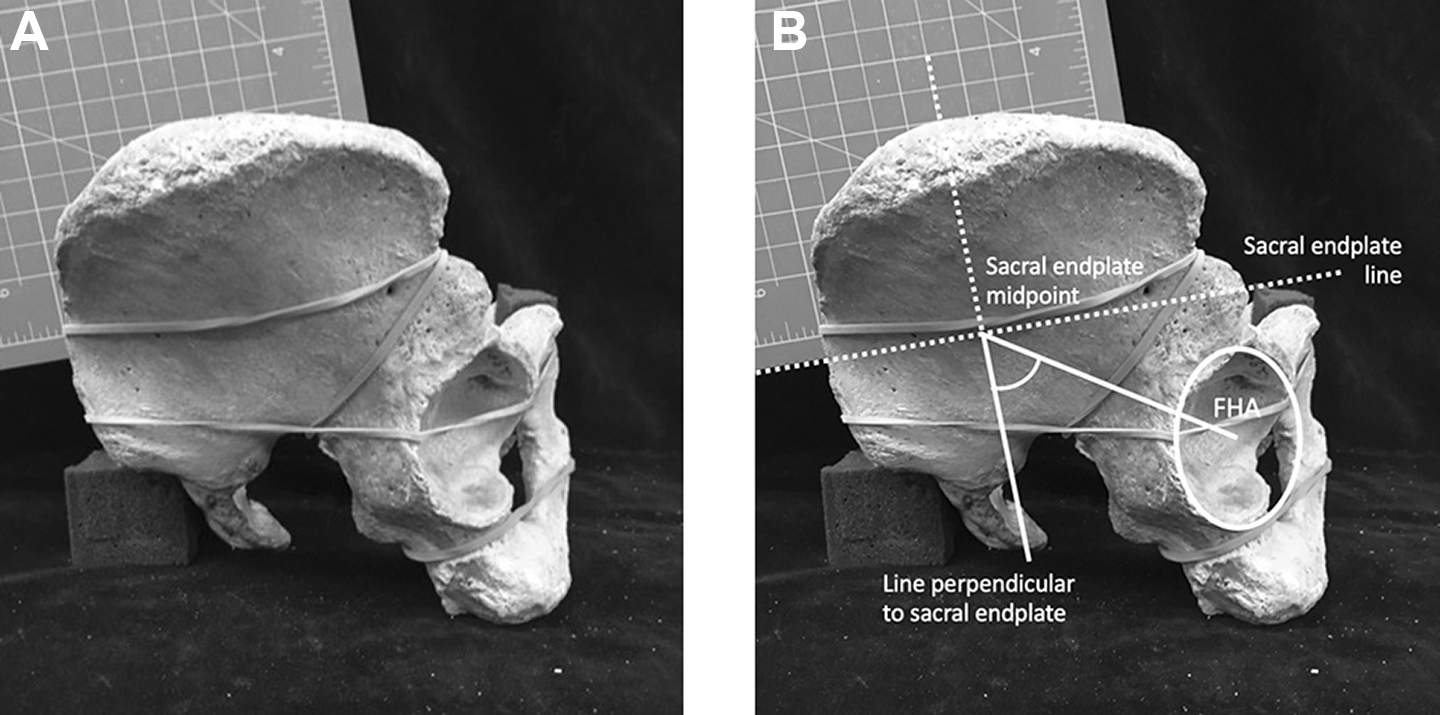
(A) Lateral photographs were obtained of each re-articulated pelvis. A square ruler was placed to mark the midpoint and plane of the sacral endplate. (B) Measurements were superimposed on images obtained of the reconstructed pelvises. One side of a square ruler was placed along the sacral endplate and a designated mark on the ruler was aligned with the midpoint of the sacral endplate. Pelvic incidence is defined as the angle formed by a line perpendicular to the sacral endplate and a line connecting the midpoint of the sacral endplate and the femoral head axis (FHA). We used the midpoint of an ellipse over the acetabular rim to approximate the femoral head axis.
Eight hundred and ninety-two pelvises with 5 lumbar vertebrae were previously measured for PI and served as a control group. For cadavers with 4 lumbar vertebrae, PI was measured using the method described above. For cadavers with 6 lumbar vertebrae, PI was measured both without and with the sixth lumbar vertebra attached (Figure 2A and B). We calculated L6-PI, which we defined as a PI measured from the superior aspect of an articulated L6 vertebral body instead of the sacral endplate. Orientation of the sixth lumbar vertebrae was verified by articulation of bilateral facet joints and sacral endplate alignment (Figure 3A and B).
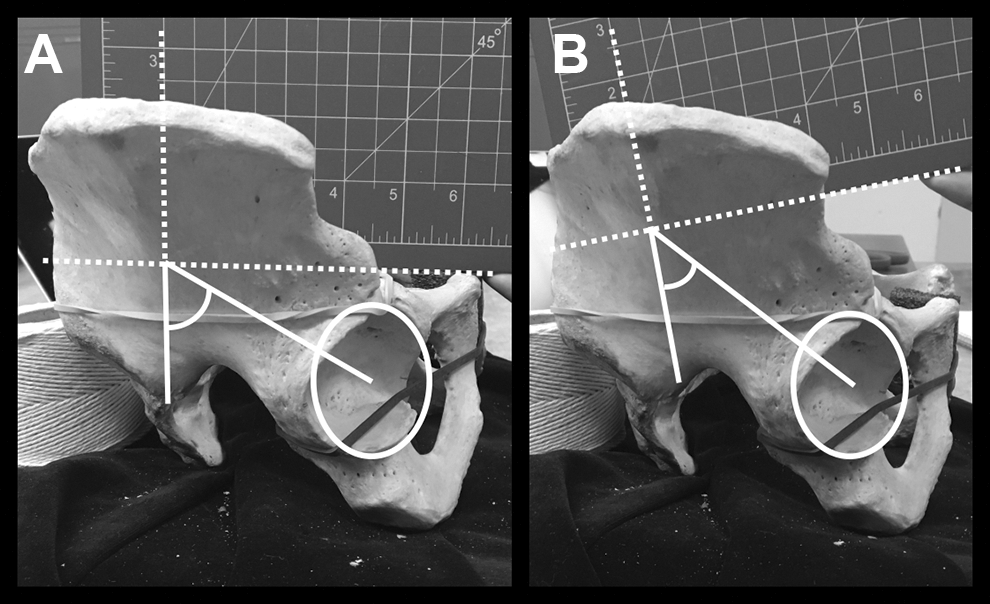
(A) Pelvic incidence without L6 added. (B) Pelvic incidence with L6 added (aka L6-PI).
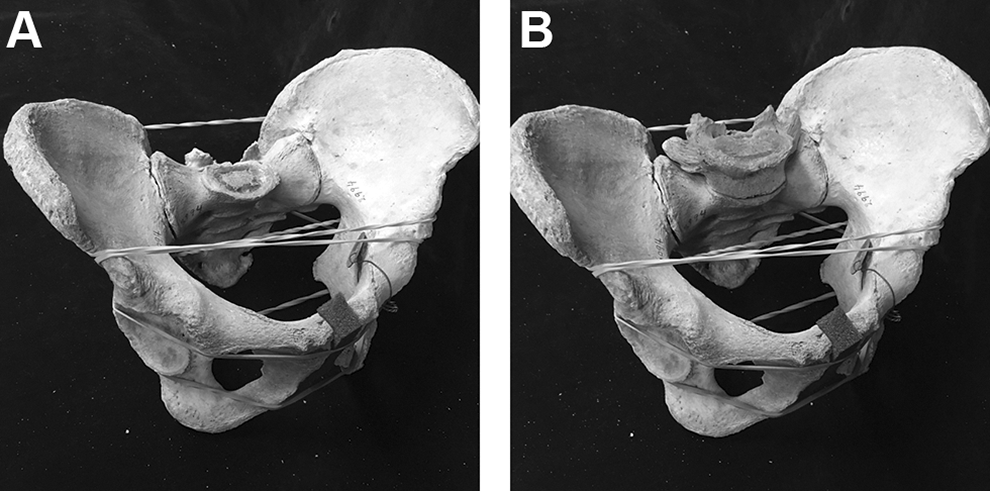
Reconstructed pelvis without (A) and with (B) L6 added. Articulation of L6 was verified with bilateral facet joint and full sacral endplate alignment.
All statistical analysis was performed using SPSS v22 (IBM Corporation, Armonk, NY). ANOVA and χ2 analysis was used to evaluate differences in means and categorical frequency, respectively, between groups. Multivariate regression models were used to determine the differences between PI among specimens while minimizing confounding from demographic parameters. Statistical significance was determined at an α level equal to .05. Interclass correlation coefficient (ICC) was calculated between each author’s PI measurements. ICC of <0.40 was considered poor, 0.40 to 0.75 good, and >0.75 excellent. 11 This study was exempt from institutional review board approval as it did not involve human subjects.
Results
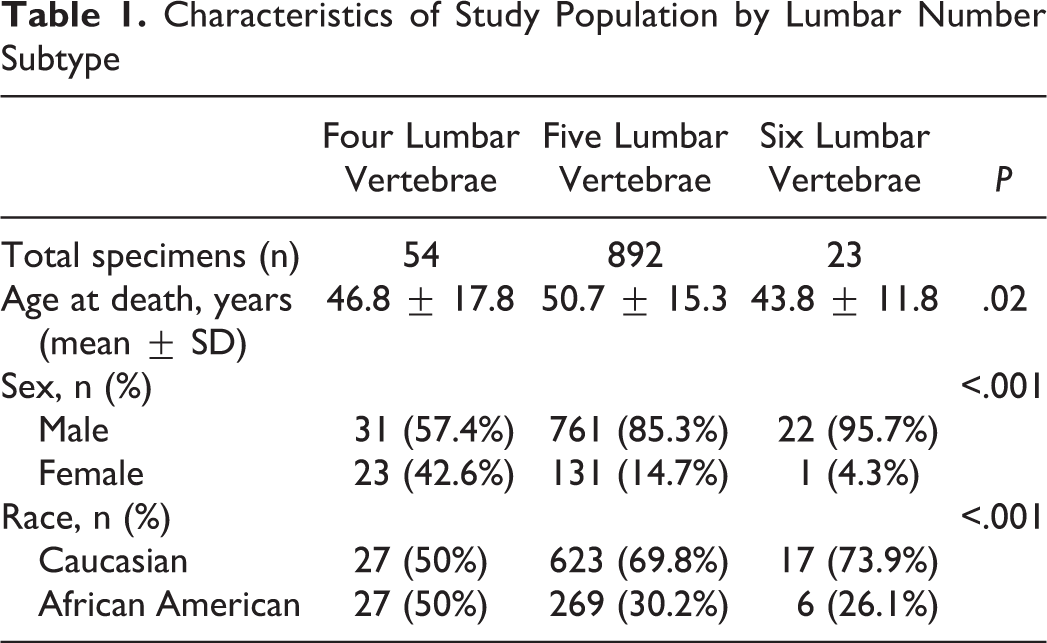
Of the 2980 specimens screened, 969 specimens were evaluated. Average age at death for all specimens was 50.4 ± 15.4 years. In our study population, 84% (n = 814) were male and 69% (n = 667) were Caucasian. Further study population characteristics are detailed in Table 1.
Characteristics of Study Population by Lumbar Number Subtype
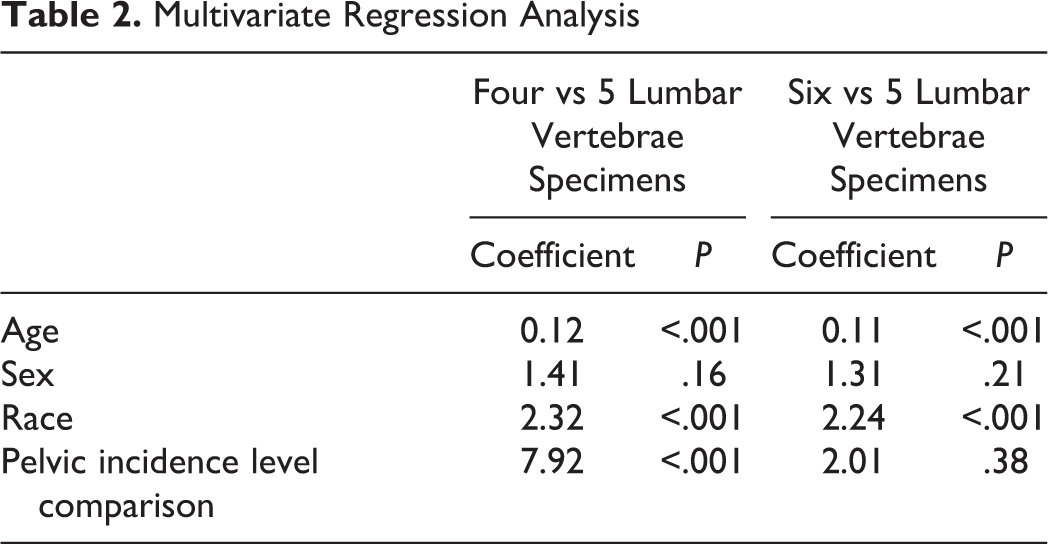
The authors calculated a total prevalence of 1.8% for 4 lumbar vertebrae and 0.8% for 6 lumbar vertebrae. The mean PI of the study population was 46.2 ± 21.1°. Average PI was calculated as 38.5° for specimens with 4 lumbar vertebrae, 46.7° for specimens with 5 lumbar vertebrae, and 47.1° for specimens with 6 lumbar vertebrae. Multivariate regression analysis showed PI was significantly different between specimens with 4 and 5 lumbar vertebrae (β = 7.92, P < .001) but not between specimens with 5 and 6 lumbar vertebrae (β = 2.01, P = .38; Table 2). For 6 lumbar vertebrae specimens, when L6 was added to the sacrum, mean L6-PI was 27.4 ± 8.0° and was significantly different from specimens with 5 lumbar vertebrae (P < .001). Additionally, PI with and without L6 added was significantly different (P < .001).
Multivariate Regression Analysis
This suggests a relative lordosis through the L6/S1 disc space and L6 vertebra of 19.3°. ICC between 2 authors for all measurements was excellent (ICC > 0.85).
Discussion
This study sought to calculate the prevalence of spines with 4 and 6 lumbar vertebrae and to evaluate any differences in PI between groups. Our study found an overall prevalence of 2.6% of anomalous number of lumbar vertebrae: 1.8% of specimens with 4 lumbar vertebrae and 0.8% with 6 lumbar vertebrae. PI in specimens with 4 lumbar vertebrae was significantly decreased compared with specimens with 5 vertebrae. Specimens with 6 lumbar vertebrae did not have significantly different PI compared to those with 5 lumbar vertebrae. With the addition of L6, L6PI was significantly decreased compared with the PI of normal spines.
In this study, we reported a lower prevalence of spines with 4 (1.8%) and 6 (0.8%) lumbar vertebrae compared with previous studies. In an examination of 591 dry cadaveric specimens from Kampala, Uganda, Luboga found 8 (1.4%) of the specimens possessed a sixth vertebrae. 2 In another study, Price et al identified 4.1% of patients with a sixth vertebrae in an evaluation of the radiographs of 268 asymptomatic patients. 4 In certain subpopulations, the prevalence of 6 lumbar vertebrae is much higher. In an article by Ibrahim et al, who evaluated 364 patients undergoing surgery for adolescent idiopathic scoliosis (AIS), 20 patients (5.5%) had 6 lumbar vertebrae and 4 patients (1.1%) had 4 lumbar vertebrae within the cohort. 12 In a separate study by Hu et al studying the radiographs of 657 patients with AIS, 14 patients (2.1%) were noted to have 4 lumbar vertebrae and 34 patients (5.2%) had 6 lumbar vertebrae. 13 Our study of cadaveric specimens showed a prevalence of 1.8% and 0.8% for spines with 4 and 6 lumbar vertebrae, respectively, which were both significantly lower than what has been reported in the literature. Our study used a similar method of counting vertebrae to that of prior studies and utilized a larger cohort of specimens.
Pelvic incidence was not observed to be significantly different in specimens with 6 lumbar vertebrae compared with those with 5 lumbar vertebrae, and prior literature on this has been inconclusive. In an evaluation of radiographs from 268 asymptomatic patients, Price et al measured PI and lumbar lordosis in patients with and without a sixth lumbar vertebrae. 4 The authors reported a significantly increased PI (mean of +22° difference) and significantly increased lumbar lordosis (mean of +8° difference) in the 11 (4.1%) with 6 vertebrae. 4 The study was limited by a small sample size and by the ethnic heterogeneity of a French and Japanese study population, particularly due to the phenotype’s unknown genetic predisposition. In contrast, in a study of early hominids by Whitcome, cadavers with 6 lumbar vertebrae showed a similar lumbar lordosis to spines with 5 vertebrae. 14 The conclusions from this study are limited as Whitcome only included early hominid cadaveric specimens who demonstrated different postures and bipedal gaits than modern Homo sapiens. 14 Our study improves upon the prior literature with a larger sample size of specimens with 6 lumbar vertebrae (n = 23).
Our finding that L6PI was significantly decreased compared to the PI in patients with 5 lumbar vertebrae was not unexpected. Lumbar vertebrae are naturally lordotic, which would translate into a decreased measured PI. This observation, in conjunction with our finding that PI in 6 lumbar vertebrae specimens matched controls when L6 was not incorporated, suggests that L6 behaves more like a lumbar vertebra than a sacral vertebra.
Pelvic incidence was observed to be different in patients who had 4 lumbar vertebrae. To our knowledge, this study is the first report of PI in patients with 4 lumbar vertebrae. However, the PI observed in this study group was similar to what has been observed in asymptomatic patients with a fused LSTV, who also possess 4 lumbar vertebrae. In a radiographic evaluation of 10 patients with L5 sacralization, Dominguez et al reported a mean L5-PI of 32.75°, measured from the superior aspect of the L5 vertebral body. 15 The results from Dominguez et al and the present study (PI = 38.5 ± 12.1) suggest patients with 4 lumbar vertebrae have a decreased PI relative to patients with 5 lumbar vertebrae and future studies should correlate this finding with symptomatology and clinical outcomes. Overall, the decreased PI in specimens with 4 lumbar vertebrae questions whether what would have been an L5 vertebra somehow sacralized during spine formation. This may have important implications when restoring appropriate lumbar lordosis in lower lumbar or lumbopelvic fusions to more accurately reconstruct correct sagittal balance in patients with 4 lumbar vertebrae.
Our study was limited by several constraints. First, the skeletal specimens were dry and as such did not possess any soft tissue or ligamentous structures. The authors, however, do not believe this to severely affect the manner in which the pelvises were reconstructed or measured as the technique has been previously validated. Additionally, in calculating the L6PI measurement used in this study, the lack of intervertebral disc may skew the results. However, the authors carefully re-articulated each L6 based on the uncovertebral and facet joints in the same manner to avoid misalignment and subsequent mismeasurement. This study had the advantage of direct anatomical investigation of the bony specimens, avoiding errors inherent in radiographs such as positioning issues and magnification. Finally, our study is limited by the reconstruction of the pelves with rubber bands for stabilization and compressible foam to approximate the symphysis. We feel that this limitation is acceptable given the reliability found in this study and our previous reports of this technique, and the fact that our conclusions are based on comparative differences rather than absolute measurement values.
Conclusions
Our study of 969 cadavers demonstrated that PI was not different between specimens with 5 and 6 lumbar vertebrae but was significantly lower in those with 4 lumbar vertebrae. Careful evaluation of spinopelvic parameters should be considered particularly in patients with 4 lumbar vertebrae, where decreased PI was noted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.