
Abstract
Study Design:
This was a systematic review and meta-analysis.
Objectives:
Degenerative cervical myelopathy (DCM) with spondylolisthesis remains not well defined, poorly studied, and underreported and plays a minor role in the therapeutic decision-making. Spondylolisthesis, however, is not uncommon and may result in dynamic injury to the spinal cord. We aim to describe the impact of spondylolisthesis in DCM severity and postoperative outcomes.
Methods:
Two independent reviewers conducted a Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA 2015)-based review between 1970 and May 2020 for articles reporting outcome of DCM in patients with degenerative cervical spondylolisthesis. Patient clinical and radiological data was recorded at baseline and during postoperative follow-up (FU). A meta-analysis comparing surgical outcome between DCM patients with and without spondylolisthesis assessed by the regular/modified Japanese Orthopaedic Association Assessment Scale (mJOA) recovery ratio was completed.
Results:
A total of 3 studies were included (1 ambispective and 2 retrospective cohorts); 607 patients with DCM were identified, 102 (16.8%) of whom also had spondylolisthesis. DCM patients with spondylolisthesis were significantly older (P < .05), presented with worse baseline mJOA and Nurick grades (P < .05 in 2 studies), and were more commonly operated via posterior approaches (P < .05). All groups experienced a (m)JOA and/or Neck Disability Index score improvement during FU. In the pooled meta-analysis, spondylolisthesis patients showed a significantly lower functional recovery ratio at 2 years compared with other DCM patients (P = .05).
Conclusions:
Spondylolisthesis is frequent in older DCM patients and may be a predictor of a more advanced degeneration and subsequent worse baseline conditions and postoperative outcome.
Keywords
Introduction
Contrary to lumbar spondylolisthesis, degenerative cervical spondylolisthesis (DCS) remains poorly studied and lacks understanding in terms of clinical relevance. Based on the existing literature, DCS is underreported and still plays a minor role in the therapeutic decision tree. 1 -4
Despite a first description made by White et al 5 stating as abnormal horizontal translation greater than 2.7 mm between the vertebrae and later by Woiciechowsky et al, 6 Dean et al, 7 and Suzuki et al 8 among others, 1,9 the literature still does not offer a consensual quantitative definition of DCS. 2,4 Furthermore, studies reporting on natural history of DCS (risk of progression, instability, and space available for the cord) are limited. 4 On the other hand, numerous articles discussed specific pathological criteria (for instance, ossification of the posterior longitudinal ligament, age, magnetic resonance imaging [MRI] signal change) 10,11 within the domain of degenerative cervical myelopathy (DCM) and their impact on baseline severity, surgical outcome, and management strategies. Given that DCS is a consequence of the degeneration cascade (including disc degeneration and hypertrophic arthropathy of the facet joints and ligaments), which is also true for other subsets of DCM, and typically manifests in the ageing spine, it is tempting to postulate that presence of DCS can directly influence the severity of DCM and outcome (Figure 1). 12 Moreover, presence of DCS can be associated with instability and dynamic spinal canal stenosis, thereby affecting the severity of symptoms. 12 It has been reported that DCS occurs in 12% of DCM patients, presenting most commonly at C4-C5 8 ; however, epidemiological data remain limited.
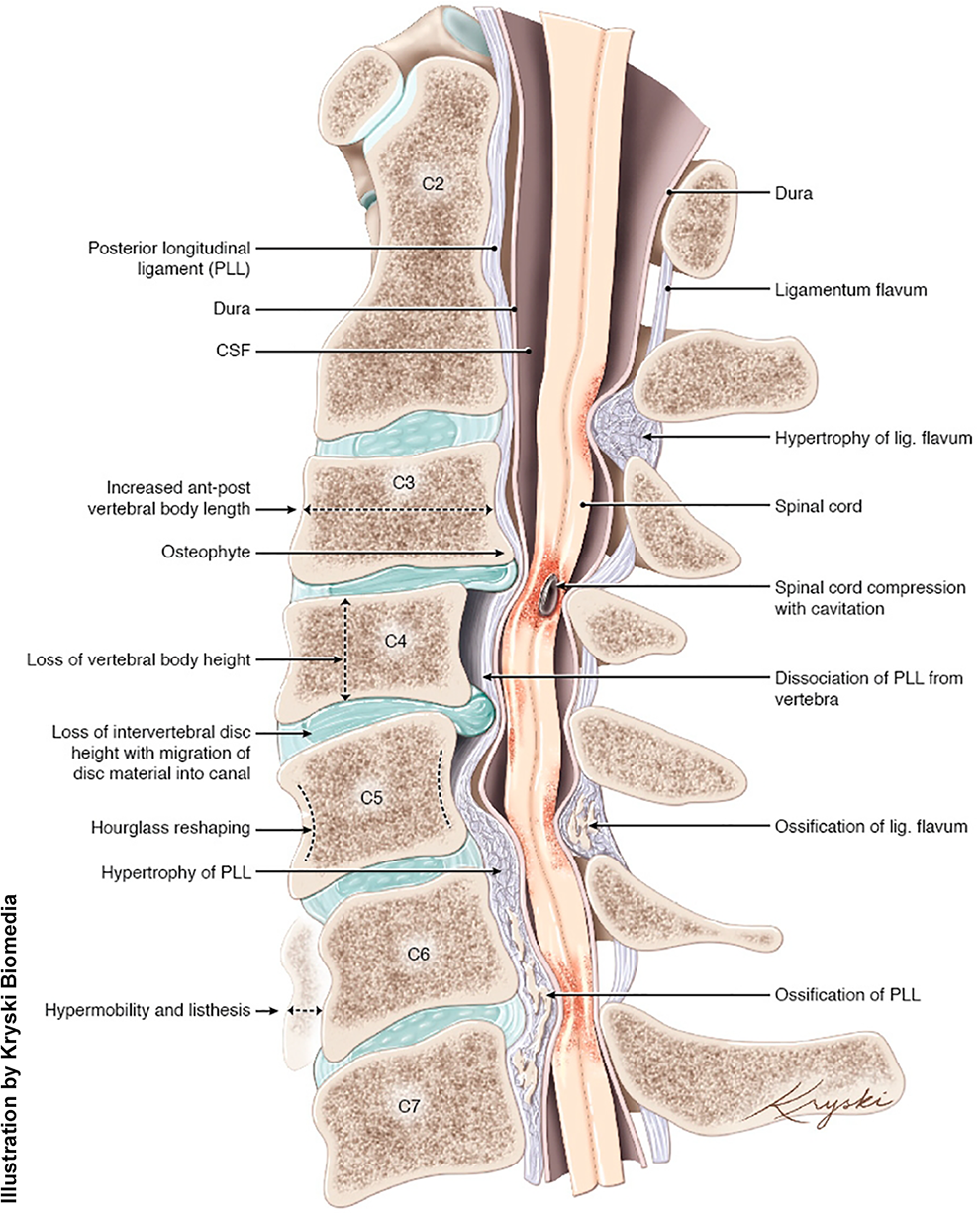
Degenerative changes that can be seen in patients with DCM and DCS (concept, Aria Nouri; edits, Michael G. Fehlings; artwork design, Diana Kryski).a
With the growing interest to identify factors that can influence the neurological severity and surgical outcome of DCM, we conducted a systematic review to evaluate the impact of DCS on the severity and outcome of patients presenting with DCM.
Methods
Search Strategy and Information Sources
This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA-P) 2015 guidelines. 13 Given the nature of the study, no research ethics board approval was needed.
To test our hypothesis that DCS may influence the clinical severity and postoperative outcome of DCM, we performed a restricted search using the keywords (spondylolisthesis AND degenerative cervical myelopathy) OR (cervical spondylolisthesis AND myelopathy) OR (listhesis AND cervical spondylotic myelopathy) OR (listhesis AND cervical myelopathy) on May 5, 2020, on the databases EMBASE, Cochrane Library, PubMed, Google Scholar, and Web of Science, resulting in a list of 154 references. We only targeted studies written in English, French, German, or Portuguese and did not restrict our search for the date of publication.
Eligibility Criteria
The following inclusion criteria were used to select studies among the above-mentioned 154 references: (1) studies reporting comparison of surgical outcome of DCM patients with and without spondylolisthesis and (2) studies providing one or more of the following outcome measurements: regular or modified Japanese Orthopaedic Association Assessment Scale (mJOA), 14,15 Nurick grades, 16 Neck Disability Index (NDI), 17 Visual Analog Scale (VAS), 18 Numeric Rating Scale (NRS), 19 36-Item Short Form (SF-36) Physical Component Summary, 20 pseudarthrosis or other complications, and sagittal balance parameters. Articles that did not meet the inclusion criteria were ruled out. In addition, editorials, letters, review articles, case reports, and finite element and animal experimental studies were excluded. References of the included studies were also reviewed.
Data Management and Selection Process
Titles and abstracts were screened by 2 independent reviewers, and full-text copies of all relevant articles were acquired. In the case of discrepancy, a third reviewer would arbitrate until there was a consensus among the authors (Figure 2). Three studies met the selection criteria, 21 -23 and data was extracted separately by the same reviewers and double-checked by a senior author.
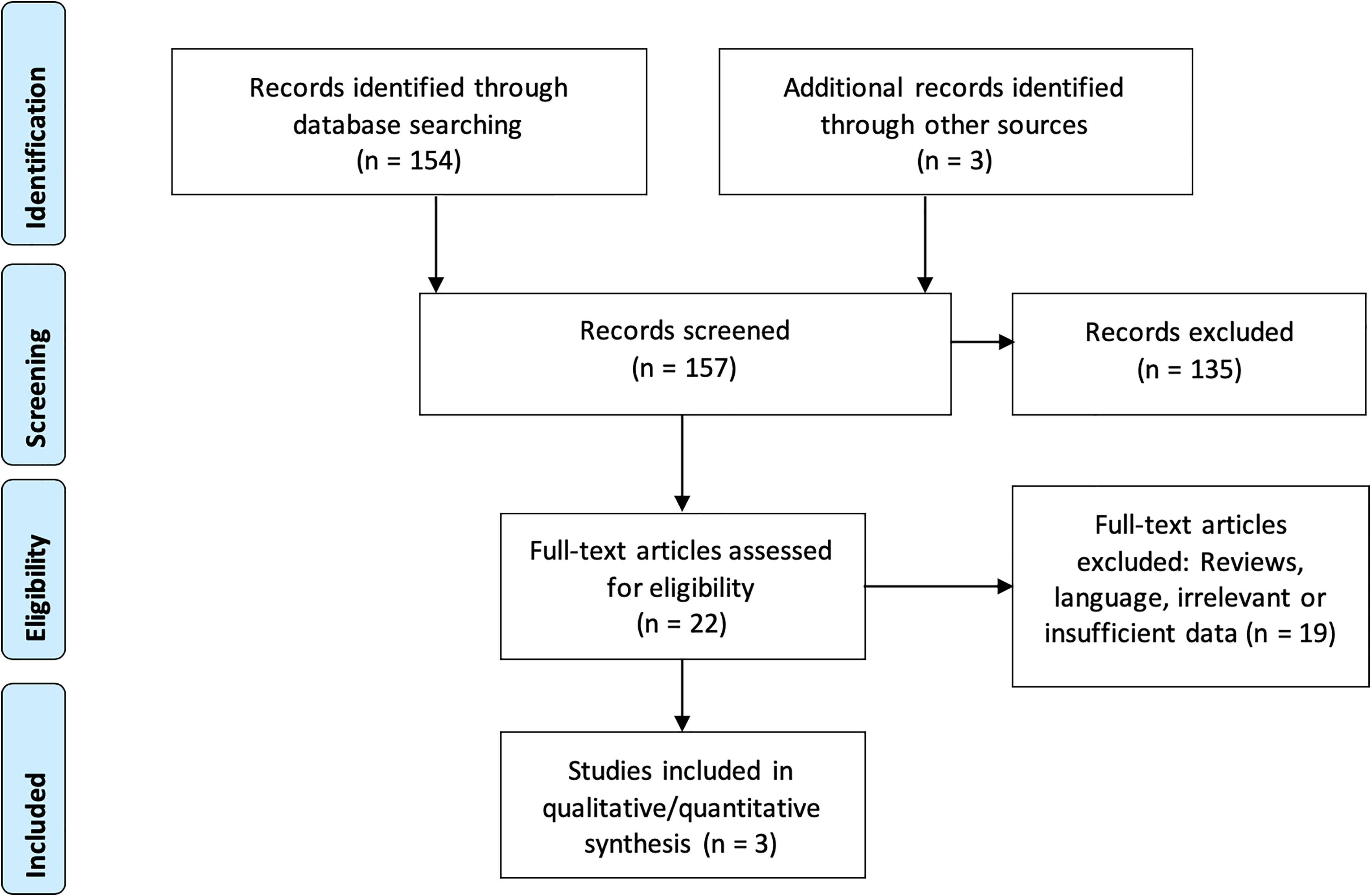
PRISMA-P flowchart and search strategy.
Data Collection Process and Data Items
The full text of each article was carefully reviewed, and data extraction was performed independently by the 2 first authors. The following data items were considered: (1) study design; (2) patient demographics; (3) surgical approach; (4) sample size; (5) duration of symptoms; (6) follow-up (FU) time; (7) patient-related outcome measurements (PROMs), considering disability, NDI, Nurick grades, SF-36, and mJOA scores/recovery rate and VAS/NRS pain scores; (8) fusion rates, adjacent segment disease, pseudarthrosis, and sagittal/coronal imbalance; and (9) parameters concerning intraoperative and postoperative complications (complications, estimated blood loss, and duration of surgery). Additional raw data for computing the recovery ratio was obtained directly from the authors of one of the articles.
Risk of Bias in Individual Studies
The 3 included articles were graded according to the Newcastle-Ottawa Quality Assessment Scale for quality assessment of nonrandomized studies 24 before being approved for further report in their results. The level of evidence for each study was evaluated using the Oxford Centre for Evidence Based Medicine guidelines. 25
Statistical Analysis of Outcomes, Prioritization, and Quantitative Synthesis
Overall, the results are presented in subgroups of patients suffering from DCM with or without spondylolisthesis. Results for continuous variables are reported as mean ± SD and were compared using independent t-tests. For those articles that did not report mean and SD, we estimated the mean and SD according to the methodology described by Hozo et al. 26
Categorical variables are presented as proportions and were assessed using the χ2 and Fisher exact tests. We conducted a meta-analysis (Review Manager version 5.3, Cochrane, London, United Kingdom) using a random-effects model (level of significance, P = .05) focusing on the only significant parameter available in all 3 studies (recovery rate from JOA or mJOA). The recovery rate was calculated according to Hirabayashi’s method: Recovery rate (%) = (Postoperative JOA − Preoperative JOA)/(17 [Full score] − Preoperative JOA) × 100. 27 The heterogeneity between other measured outcomes and the small number of articles included prevented further comparisons.
Results
Search Results and Included Articles
The initial search strategy identified 157 articles (Figure 2). After abstract screening, 135 articles were excluded and 22 were fully read. Only 3 were selected for inclusion. 21 -23 One ambispective study with a geographically diverse cohort and propensity matching by age, baseline mJOA, mJOA recovery rate, and surgical approach was identified. 21 In addition, 2 retrospective cohorts from Japan were also included. 22,23
The international ambispective cohort 21 presented 2 groups of DCM patients, one without (n = 404, 88.2%) and one with signs of spondylolisthesis (n = 54, 11.8%), and defined listhesis as “an anterior or posterior displacement of a rostral vertebra in relation to the adjacent caudal vertebra on MRI and only if the entire vertebral body was displaced.” 21(p3) The cohort from Suzuki et al 23 included 117 patients, with spondylolisthesis being defined as “more than 2 mm slip compared with adjacent vertebrae on plain radiographs in a neutral position,” 23(p1809) and found in 33 (28.2%) patients. The cohort from Shigematsu et al 22 included 32 patients (n = 15 or 46.9%, with spondylolisthesis defined as more than 2.5 mm of slippage displacement observed on flexion/extension radiographs at least at 1 level), all of them receiving laminoplasty. Patient groups and respective demographics, surgery-related data, and PROMS are summarized in Table 1.
Study and Patient Characteristics for Each Cohort.a
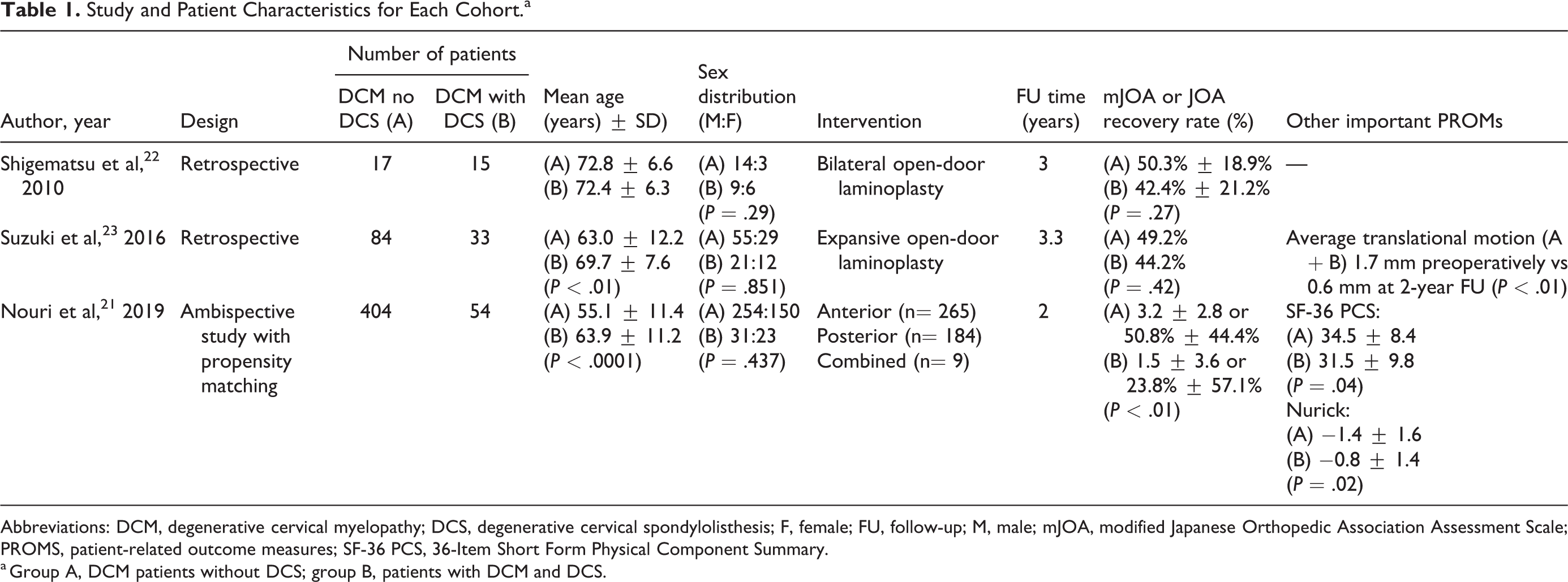
Abbreviations: DCM, degenerative cervical myelopathy; DCS, degenerative cervical spondylolisthesis; F, female; FU, follow-up; M, male; mJOA, modified Japanese Orthopedic Association Assessment Scale; PROMS, patient-related outcome measures; SF-36 PCS, 36-Item Short Form Physical Component Summary.
a Group A, DCM patients without DCS; group B, patients with DCM and DCS.
Demographic Results
A total of 607 patients in 3 studies had detailed data about preoperative and postoperative clinical presentation. Of these, 102 (16.8%) had spondylolisthesis. This disease constellation (both DCM and DCS) was more frequent in adult men (n = 61, 59.8%), with a mean age varying between 63.9 ± 11.3 years in the international cohort 21 and 72.4 ± 6.3 years in the smaller Japanese cohort. 22 Two out of 3 studies showed that DCM patients with spondylolisthesis were significantly older by an average of 8.8 years (P < .0001) 21 and 6.7 years (P < .01). 23 DCS occurred mostly at the C4-C5 level (21, 17.9%) for Suzuki et al 23 and equally at C3-C4 and C4-C5 levels (9, 28.1%) for Shigematsu et al. 22
Clinical Presentation and Outcomes
Nouri et al 21 described a worse baseline disease severity when presenting with spondylolisthesis. This was assessed by the mJOA (11.72 ± 3.05 vs 12.79 ± 2.74; P = .008), Nurick grades (2.78 ± 1.59 vs 1.74 ± 1.57; P = .008), and SF-36 Physical Component Score (35.22 ± 9.24 vs 41.23 ± 11.17; P = .01). Other measured parameters such as the SF-36 Mental Component Score and NDI were not significantly different (P > .05).
Suzuki et al 23 also found a significantly lower baseline average JOA score (P < .05) in the DCS group, and Shigematsu et al 22 showed a small nonsignificant difference in the same direction (6.5 ± 3.4 vs 6.8 ± 3.8; P = .82).
Postoperatively, patients with DCS presented a significantly lower mean improvement at the FU period in only 1 study, 21 even after propensity matching, for both mJOA (1.5 ± 3.6 vs 3.2 ± 2.8, P < .01) and Nurick scores (−0.8 ± 1.4 vs −1.4 ± 1.6; P = .02). However, Suzuki et al 23 only documented a worse postoperative average JOA in the DCS group (P < .05) without any difference with regard to recovery rates (44.2% vs 49.3%; P = .42). Pain VAS scores also improved consistently in both groups. Similarly, Shigematsu et al 22 found no difference in measured clinical outcomes (average JOA or recovery rate) but demonstrated that all patients significantly improved.
Putting together the recovery ratio findings of the 3 studies 21 -23 in the meta-analysis (Forest plot, Figure 3) showed that patients with spondylolisthesis presented with worse outcome based on the JOA or mJOA recovery ratio than DCM patients without spondylolisthesis (P = .05).

Meta-analysis distribution of postoperative outcomes for Japanese Orthopedic Association Assessment Scale (JOA) or modified JOA recovery rate in the presence or absence of degenerative cervical spondylolisthesis (DCS). It is shown that patients with spondylolisthesis presented with worse neurological recovery than degenerative cervical myelopathy patients without spondylolisthesis (P = .009, fixed effect model; P = .05, random effects model).
Radiological Outcomes
Different radiological parameters were reported according to the different imaging modalities used. Shigematsu et al 22 presented a broader analysis with no difference in cervical sagittal alignment, cervical lordotic angle, or range of motion between groups. 22
Nouri et al 21 had an MRI for each patient and observed the following in the DCS group: a higher frequency of ligamentum flavum enlargement (81.5% vs 53.5%; P < .0001) was found; a trend toward more compressed levels (3.48 vs 3.08; P = .052) was found; and ossification of the posterior longitudinal ligament tended to be less common (3.7% vs 11.4%, P = .098).
Surgical Strategy and Complication Rate
Each study reflected different surgical approaches, with the Japanese-derived cohorts only receiving laminoplasties, generally via open-door technique from C3 to C6 23 or double-door (midsagittal spinous splitting) technique from C3 to C7. 22 Posterior approaches also prevailed in the ambispective cohort (P = .0002) for DCS patients, and anterior surgery was more commonly performed in patients without DCS. It was also found that DCS patients received surgery for a greater number of levels on average (4.3 ± 1.4 vs 3.6 ± 1.2; P = .0002) and tended to have longer operations (196.6 ± 89.2 vs 177.2 ± 75.6 minutes; P = .087). No data was available on complication rate or reoperation rate.
Discussion
Summary of Evidence
To date, little is known about cervical spondylolisthesis and its impact on DCM. DCS is probably underreported and has not received the same attention as degenerative lumbar spondylolisthesis, despite possibly being as common. 4 Although the number of studies included in this review is limited to 3 articles, there are some general conclusions that can be made: (1) spondylolisthesis in DCM presents in patients with older age; (2) criteria for defining DCS are lacking; (3) DCS seems to affect baseline severity and surgical outcome of DCM and, therefore, deserves a more consistent approach, classification, and consideration in the surgical timing and strategy.
It also appears that spondylolisthesis is frequently accompanied by yellow ligament enlargement/infolding, hypertrophic facet arthropathy, osteophytes, and facet subluxation, all of which represent frequent signs of cervical degeneration (Figure 1). 12,28 As is known, these changes are part of a chain of events where disc degeneration also occurs, resulting in a loss of motion and increased stress during movement.
Prevalence and Demographics of DCS
There is only limited data regarding the prevalence of DCS, with no clear diagnostic criteria. It has been estimated that its prevalence in the general population ranges between 5% and 20%. 6,8 On the other hand, studies reporting on patients with cervical symptoms have shown higher prevalence rates (up to 26.4%). 8 The 3 included studies 21 -23 showed an average prevalence of 16.8%. Two of these 22,23 described C3-C4 and C4-C5 as the levels more frequently involved, which is in line with previous findings. 2,7 The preferential location of spondylolisthesis in the midcervical segments has been suggested to be a result of their higher mobility and their ligamentary laxity, far from the proximal insertion of the strong ligaments of the cervical axis. 5 Suzuki et al 8 also showed that disc degeneration was significantly higher at levels, with DCS as part of the same motion-related degenerative process. These authors went even further, studying the degree of translational motion in these patients and showing a proportional trend between the amplitude of motion and the magnitude of DCS. Ultimately, a distinction was proposed between stable and unstable DCS, defined as movement less than or greater than 2 mm, respectively, correlating higher translational motion in dynamic imaging with higher DCS values. 8,23 It is interesting to note that the most common levels suffering from symptomatic disc degeneration are C5-C7, which does not exactly correlate with previously discussed DCS epidemiology. 29 The main hypothesis for DCS being more common in levels adjacent to disc degeneration is that ankylosis and rigidity increase stress on the adjacent discs and facets, especially during flexion and extension of the cervical spine. The increased stress may stretch the disc and ligaments, allowing slippage to occur. 2,3,7
Diagnostic Tools
Plain radiographs remain the gold standard in the diagnosis of lumbar spondylolisthesis, and dynamic imaging allows the assessment of instability. 2,4 However, there is neither clear guidance as to which imaging modality should be used to assess DCS nor are there specific cutoff values for its diagnosis and categorization. Cervical radiographs provide the benefit of imaging in the standing position with standard weight-bearing, but they do not provide information regarding its impact on spinal cord compression. It is also cheaper and easily available.
Dynamic radiographs also play a role in the assessment of cervical spine instability. The correspondent mobility of each segment is measured in terms of translational anteroposterior motion of the superior and inferior vertebrae relative to each other at rest or between flexion and extension positions, whereas the angular motion is the difference of intervertebral angles between 2 adjacent vertebrae from flexion to extension or in the resting position. White et al 5 defined instability as “inability under physiologic loads to maintain relationships between vertebrae in such a way that there is neither initial damage nor subsequent irritation to the spinal cord or nerve roots and, in addition, there is no development of incapacitating deformity or pain due to the structural changes.” 5,30,31(p93) White et al 5 further elaborated on quantitative cutoffs for instability (more than 3.5 mm of horizontal translation or 11° of angular motion between vertebrae), 5 whereas the Panjabi criteria remain focused on lumbar instability assessment. 31
On the other hand, MRI enables a 3-dimensional evaluation suppressing artefactual measurements given by 2-dimensional superposals. It also allows for better image resolution and more accurate measurements while evaluating the influence of DCS on spinal canal stenosis, DCM, and neurological tissue outcomes. 32 -34 Evidence suggests that dynamic MRI can elucidate changes in the disc width and cord compression with higher sensitivity. 34 -36 Using dynamic supine MRI, it has been shown that new appearance or increased cord compression can be identified in more than 20% of patients and that the average narrowing of the cervical canal was 20% in comparison with the neutral position. 34 Although not all of this movement-related compression is related to DCS, it highlights the importance of incorporating dynamic factors in the diagnostic and surgical decision-making process. However, the effectiveness of incorporating dynamic MRI in everyday clinical practice for assessment of DCS remains unclear.
Among the 3 included studies, one made the diagnosis based on static MRI (12% of DCS prevalence), 21 another did it based on plain radiographs in a neutral position, 23 and Shigematsu et al 22 added dynamic radiographs to plain acquisitions. The current state of affairs reflects this same uncertainty, and no single modality is complete on its own.
Classification Issues
To date, 3 classification proposals have been made. Recently, Suzuki et al 8 divided DCS into grade 1 and grade 2 (respectively 2-3 mm or >3 mm of slippage in neutral radiographs), on a quantitative gradient scale. Back in 2009, Dean et al 7 presented 2 categories of DCS: adjacent to a stiffer spondylotic segment (59.7%) or within spondylotic segments (40.3%). Type 1 is normally associated with other degenerative changes and coexists with horizontally oriented facet joints that allow for more translational motion. Type 2 relies more on disc degeneration. Finally, Woiciechowsky et al 6 categorized DCS into 3 types: type 1 with degeneration of the facet joints; type 2 with degeneration of facet joints and vertebral bodies; and type 3 with severe cervical spine deformity. The applicability of this classification is questionable because it does not clearly correlate with a growing proportional severity range. Suzuki et al 8 were able to demonstrate a narrower space available for the cord in levels with DCS >2 mm, with a higher incidence of severe cord compression and deformity at such levels. Despite establishing radiologically relevant DCS >2 mm, they failed to correlate grade 1 and grade 2 with progressive clinical and radiological damage.
As opposed to lumbar spondylolisthesis, DCS cannot be classified according to the Meyerding classification. 37 It is easy to conceive that the cervical equivalent to a Meyerding grade 2 or more would result in severe neurological compromise because of spinal cord compression.
Influence of DCS on Surgical Outcome
Despite using different PROMs, all the studies included in our meta-analysis found worse baseline clinical myelopathy in DCS patients. Only Shigematsu et al 22 did not reach significant values, probably because of the small sample size. Furthermore, DCS seems to not only correlate with worse preoperative clinical status, but also to affect postoperative outcomes. Nouri et al 21 (significantly lower mean mJOA [P < .01] and Nurick grade improvement at the end of the FU period [P = .02]) showed a significant difference, even after propensity matching. The 2 Japanese studies indicated worse mJOA recovery ratios that were not significant. 22,23 The reason again is likely attributable to smaller sample sizes and insufficient statistical power. When putting the studies together in the meta-analysis (Forest plot, Figure 3), the presence of DCS results in significantly worse neurological recovery (P = .05).
Does DCS influence a poorer result in DCM patients? This question can be coupled with the following: shall surgical treatment and timing be more aggressive in DCM patients also presenting with DCS? The answer depends on both the natural history of DCS and the direct proportional ratio between DCS magnitude and DCM severity.
Park et al 4 stated that a 7-year FU is probably too short to fully understand DCS natural history and also supported the findings from Oichi et al 1 stating that anterolisthesis seems more deleterious for surgical outcome than retrolisthesis in patients with DCM and concluded that a patient’s age was a risk factor for DCS progression.
Concerning the link between DCS displacement and DCM severity, less data exist. Suzuki et al 8 pointed out that the space available for the spinal cord was smaller and cord compression grade higher in cervical levels with more than 2 mm listhesis, but this finding was not connected with any clinical score. Among the 3 included studies we also did not find any specific data.
In addition to already known factors (duration of symptoms, baseline neurological status, and T1 hypointensity on MRI), our study highlights that presence of DCS also negatively influences the outcome of DCM. 11
Limitations
Few studies met our selection criteria, and 2 out of 3 were geographically limited and with relatively small samples (low quality of evidence, level 4). This rendered our meta-analysis (Forest plot, Figure 3) less powerful. Furthermore, it was also limited to the assessment of neurological recovery rates, because of the lack of equivalent outcome measures among the 3 studies. The FU time could have been longer for all the studies.
Another important difference between studies concerns the different available imaging tools. Whereas the static MRI probably underreports minor DCS that show themselves only in dynamic studies, plain or dynamic radiographs can also underestimate because they lack resolution and 3-dimensional representation. Also, the explicitness of the lower cervical levels in radiographs is probably suboptimal, causing a selection bias in 2 of our cohorts. Another selection bias for these 2 articles is the limitation of the cohorts to patients having received laminoplasty. On the other hand, the 2 studies lacking dynamic images were not able to report the degree of translation, and therefore, no conclusions were made about the “stable” or “unstable” character of the DCS.
Conclusions
This article is the first systematic review and meta-analysis synthetizing the impact of DCS in DCM patients. Although the level of evidence is limited, some important recommendations can be made. DCS is underreported and only partially understood as a result of poor criteria for diagnosis and classification. Similar to lumbar spondylolisthesis, diagnosis is made through plain radiographs, but this can be debated because millimetric details in the cervical spine are probably more important. It occurs more frequently at the C3-C4 and C4-C5 levels and at older age.
Multiple findings suggest a path connecting DCS and poorer DCM outcome, such as smaller space available for the cord in DCS patients and higher cord compression, significantly worse baseline and postoperative JOA and mJOA recovery rates for DCS patients in our quantitative analysis, and shorter duration of symptoms until surgery. This parameter and its magnitude shall then be considered in the surgical decision.
To address this knowledge gap about DCS epidemiology and outcome, we plan to develop and validate a standard DCS severity classification based on listhesis to canal diameter ratio as the major contributor instead of using an absolute listhesis value as a single measurement. This could reflect the impact of the DCS in the space available for the cord and in DCM development as well as predict surgical outcomes more accurately.
Footnotes
Authors’ Note
RG: project draft, literature review, data analysis, and manuscript writing; AN: literature review, data analysis, and manuscript writing; GJ: data analysis and manuscript review; KS: manuscript writing; ET: project draft, writing of the manuscript, and overall supervision. ETtraining fees were obtained from Medtronic, Depuy Synthes, Spineart.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.