
Abstract
Primary spinal chondrosarcoma (CS) is rare. Only a few previous case reports have included a detailed description of the surgical process used to treat the CS. In addition, a paucity of documentation exists comparing differences in the outcomes between the approaches in en bloc resection. Here, we present a case of CS in the lumbar (L) spine treated with two-stage (anterior and posterior approach) en bloc surgery and analyze the differences between one-stage and two-stage approaches in the treatment of primary lumbar CS. A 30-year-old male patient with an L3 vertebral body CS presented with back pain and lower limb weakness. Lumbar spine magnetic resonance imaging (MRI) showed an L3 vertebral body tumor with cord and root compression. Two-stage surgery comprising posterior total laminectomy and transpedicular screw fixation over L2–L4 in the first stage, with subsequent anterior corpectomy, cage implantation, and anterior lumbar interbody fusion was performed to achieve total tumor removal and stabilization. The patient’s symptoms improved postoperatively, with no recurrence as of the 2-year follow-up. The analysis of previous similar cases showed that two-stage surgery, compared with one-stage surgery, appears to be beneficial in lumbar spine multisegment disease, providing a lower recurrence rate.
Introduction
A chondrosarcoma (CS) is a malignant tumor comprising transformed cells producing a cartilaginous matrix, 1 and such tumors account for approximately 10% of all bone tumors. 2 However, primary spinal CS is relatively rare, with a reported prevalence rate of less than 10%. 3 Up to 60% of spinal CSs occur in the thoracic spine, with the remaining incidences variously occurring in the cervical spine, lumbar (L) spine, and sacrum.4,5
Several surgical approaches for achieving en bloc resection have been mentioned in previous studies. Both one-stage surgery (using only a posterior or anterior approach) and two-stage surgery (using a combination of posterior and anterior approaches) have been mentioned.2,5–7 To our knowledge, few prior case reports have included detailed descriptions of the surgical methods used during the two-stage approach.8–10 We described our method, in this report, and compared the surgical outcomes between one-stage and two-stage en bloc surgical approaches for the treatment of rare primary lumbar CS.
Case report
A 30-year-old man without known systemic disease presented with low back pain radiating to the left anterior thigh for 4 months, accompanied by progressive left lower limb weakness. Symptoms presented without diurnal variation and were exaggerated with flexion and relieved with stretching. The patient’s medical history revealed no known cancer and no history of radiation or surgical treatment. No traumatic accident or previous infectious disease was reported. Neurological examinations revealed decreased left lower limb muscle strength, with a positive straight-leg raising test (SLRT). Sensory function was intact, but the patient complained of tingling, numbness, and soreness related to motion. L-spine X-ray, computed tomography (CT), and magnetic resonance imaging (MRI) revealed an L3 vertebral body osteolytic lesion with epidural expansion and compression of the spinal cord and nerve root (Figures 1 and 2). No elevated tumor markers were observed, and a technetium 99m-methylene diphosphonate (Tc-99m MDP) whole-body bone scan did not reveal any abnormal uptake, except in the L-spine (Figure 3a). No evidence of metastasis was found elsewhere in the body on positron emission tomography (PET) (Figure 3b and 3c). Owing to the remarkable neurological deficit during disease progression, a malignant tumor was highly suspected. Thus, surgical intervention was arranged.
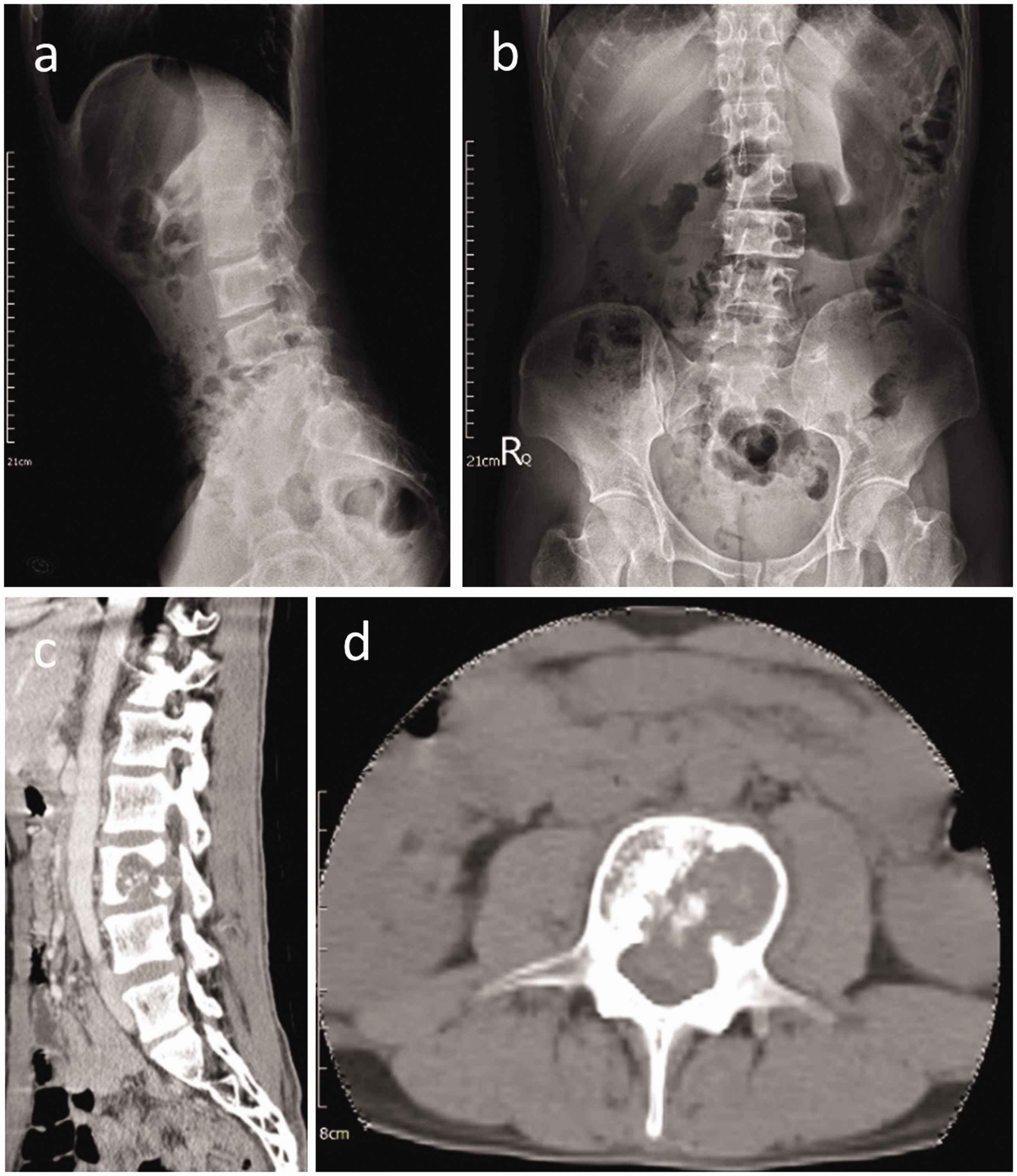
Lumbar (L)-spine X-rays; lateral view (a) and anterior–posterior view (b). Computed tomography (CT) showing the osteolytic characteristic of the lesion over the L3 vertebral body in the sagittal view (c) and axial view (d). Spinal canal invasion is noted in the axial view.
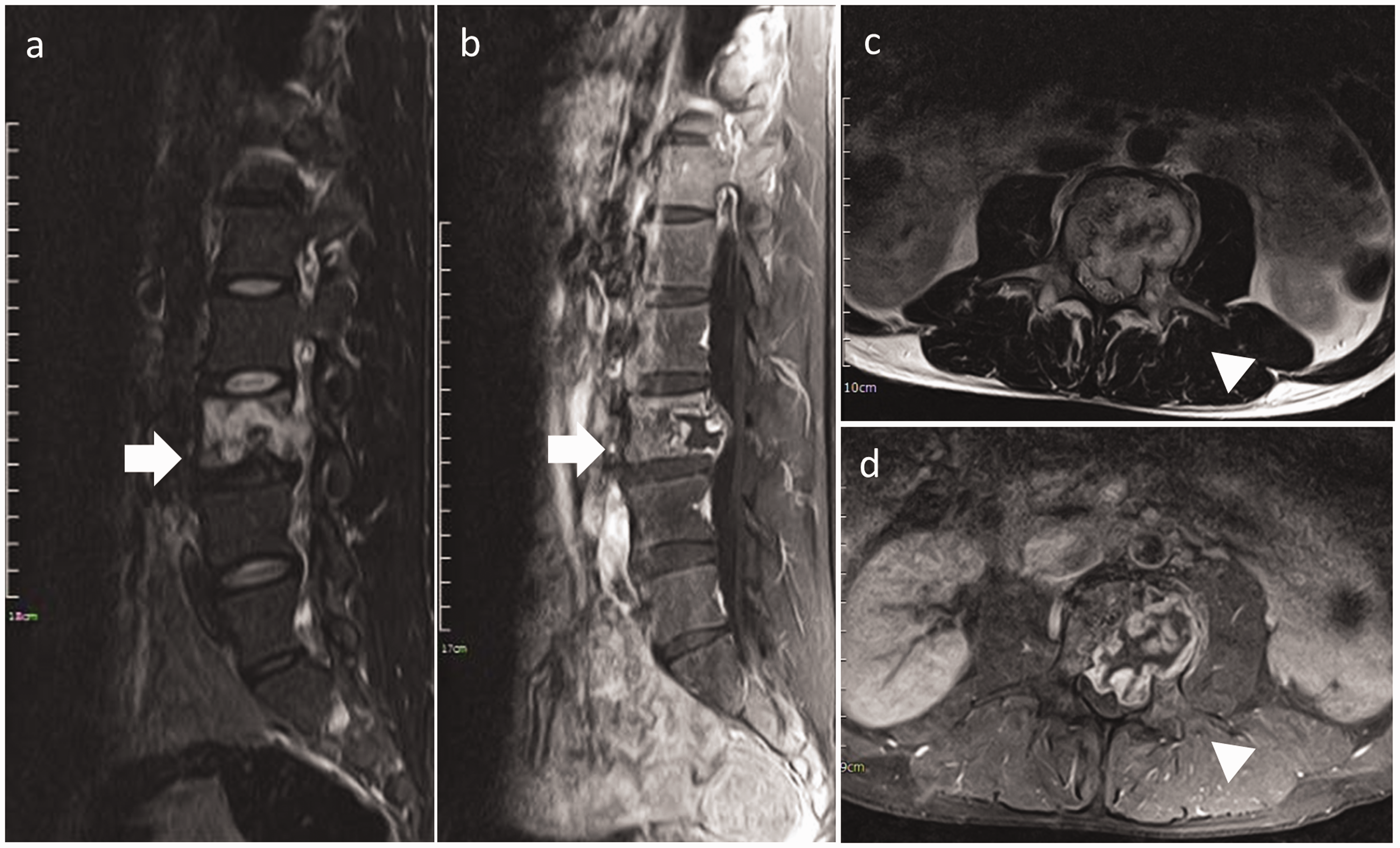
Magnetic resonance images (MRI) showing a lesion in the third lumbar (L3) vertebral body. (a) Sagittal T2-weighted image showing a lobulated lesion with heterogeneous signal intensity (arrow). (b) Sagittal T1-weighted image with contrast showing a lesion with heterogeneously high signal intensity (arrow). Axial T1-weighted (c) and T2-weighted (d) images with contrast, showing the epidural expansion of the tumor, associated with cord and root compression (arrowhead).
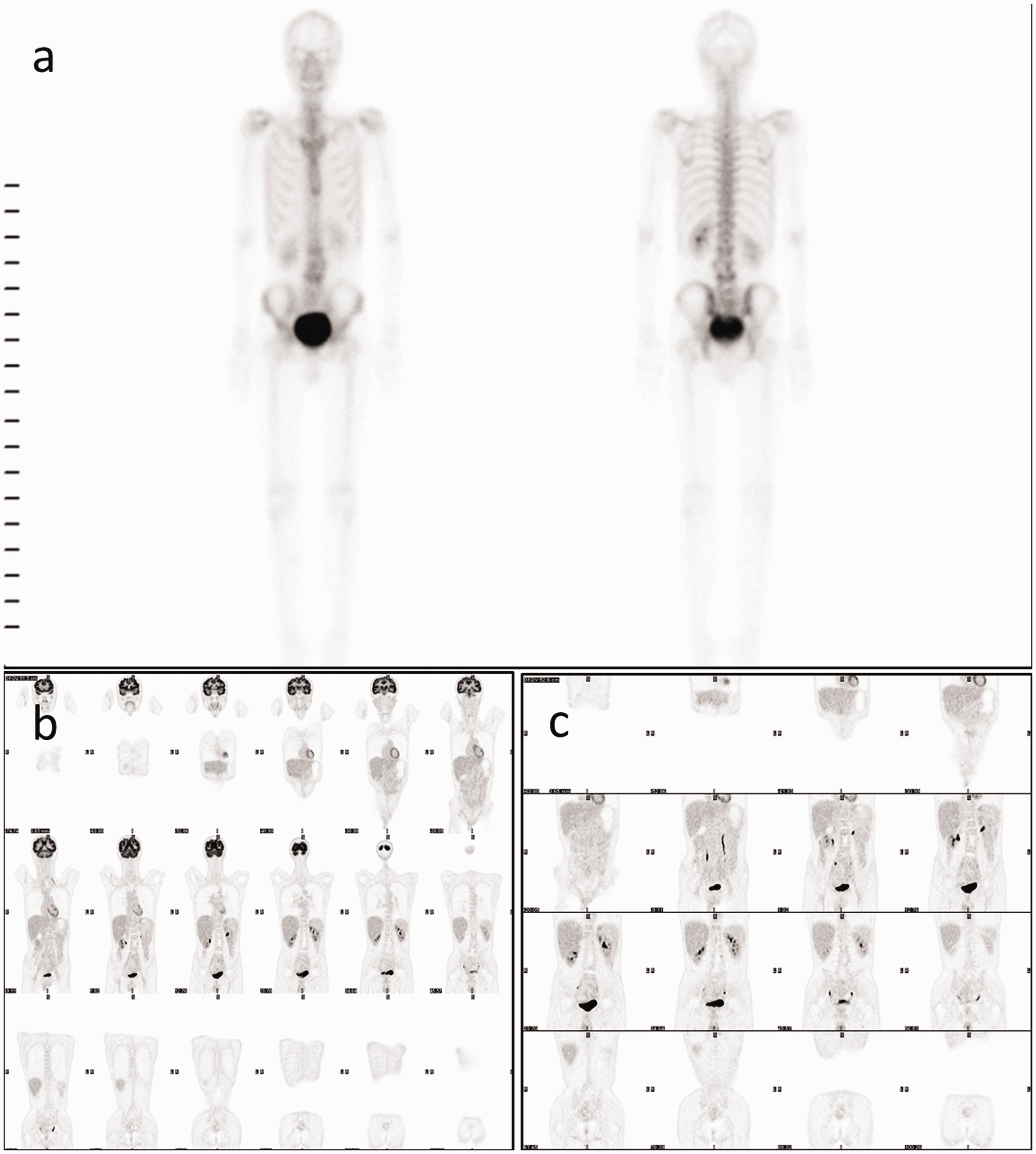
Additional imaging (a) Technetium 99m-methylene diphosphonate (Tc-99m MDP) whole-body bone scan showing no remarkable abnormal uptake, except in the lumbar (L)-spine, suggesting primary lumbar chondrosarcoma without metastasis. (b) and (c) Postoperative whole-body positron emission tomography (PET) scan showing no evidence of metastasis.
Two-stage surgery was performed. Posterior laminectomy of L3 with transpedicular screw fixation over L2 and L4 was performed first (Figure 4a and b). A frozen section was obtained from the en bloc excised specimen and was assessed intraoperatively, revealing a cartilaginous tumor (data not shown). Four weeks after the first-stage surgery, an anterior approach was performed. The L3 level was located with fluoroscopic imaging. A longitudinal incision was made over the left abdomen, and the rectus was retracted toward the midline. An incision on the posterior sheath was made using blunt dissection, entering the retroperitoneal space. The peritoneum was elevated medially and away from the psoas muscle, and the ureter was identified and moved away from the psoas muscle. Upon identifying the psoas muscle and medial L3 body, descending aorta, and inferior vena cava, located medially to the psoas muscle, a 23-gauge needle was inserted into the disc space, and the level was confirmed with fluoroscopic imaging. To mobilize the great vessels for improved exposure of the L3–L5 vertebral bodies, blunt dissection with a peanut dissector and suction tip was performed, followed by transection of the segmental vessels and the iliolumbar and ascending lumbar veins. The great vessels, retroperitoneum, and rectus muscle were held in place using a Harrington retractor, and the blunt dissection continued from left to right until the right lateral edge of the vertebral body was palpable. A table-held retractor with a reverse lip was used to engage the bladder on the right side of the body rather than a Harrington retractor, to provide an anchor to prevent slipping owing to tension. Corpectomy at L3 was then performed, and subsequent anterior lumbar interbody fusion (ALIF) was performed with implantation of a distractible titanium cage as well as anterior plate fixation using a 76-mm VECTRA-T® (DePuy Synthes Inc., West Chester, PA, USA) (Figure 4c and d), achieving both total resection of the tumor and reconstruction.

Postoperative plain radiographs after the two-stage surgery. The lateral view (a) and anterior–posterior (AP) view (b) of the lumbar (L)-spine after the first-stage surgery showing L2 and L4 transpedicular screw fixation. The lateral view (c) and anterior–posterior (AP) view (d) show the reconstruction and anterior lumbar interbody fusion (ALIF) after L3 corpectomy.
Pathology revealed lobules within the cartilaginous tumor containing a blue-gray cartilage matrix, focal increased cellularity, and minimal to focal mild nuclear atypia, suggesting a diagnosis of grade I CS with clean tumor margins (Figure 5).

Intraoperative frozen section and post-operative pathological (hematoxylin and eosin staining, ×200) images showing tumor permeating and entrapping the pre-existing lamellar bone trabeculae (a) and mildly increased cellularity of the normal cartilage component (b). (c) Specimen showing the tumor-free margins. The scale bar indicates 100 µm.
The patient’s symptoms improved after the operation, and he also reported improved quality of life. No recurrence was noted with MRI or CT at the 2-year follow-up (Supplementary information). The patient agreed to the publication of this report and provided written informed consent. The China Medical University & Hospital Research Ethics Committee waived the requirement for ethics approval because of the nature of this study (case report).
Discussion
The most common symptom of spinal CS is back pain, with neurological signs related to spinal cord or nerve root compression. 4 A palpable mass has also been mentioned in cases of outward extending spinal CS. CT usually reveals a lytic, destructive, lesion of varying density, and CT is helpful in defining the tumor location and characterizing the tumor growth. 4 MRI is used to estimate the extent of soft tissue invasion. T1-weighted images often demonstrate a hypointense lesion, whereas T2-weighted images are hyperintense. 4 The World Health Organization grading system for CS ranges from low-grade (grade I) to high-grade (grade IV) tumors, with the grade determined according to histologic features, such as tumor cellularity, nuclear atypia, stromal content (i.e., chondroid or myxoid), and mitoses. 11 CSs can be divided into conventional and variant subtypes, including clear cell CSs, mesenchymal CSs, and dedifferentiated CSs.3,5 The last two subtypes indicate high malignancy and a poor prognosis. 4 Biopsy before definitive surgery has been suggested in some articles, and CT-guided biopsies performed with a large-bore trocar instead of a fine needle have also been suggested. 4 The biopsy path should be contained in the excision margin in case of contamination. 3 Surgical resection is the definitive treatment for a spinal CS, with en bloc resection without entering the tumor capsule contributing to better overall survival and lower recurrence rates.2,5–7 Other risk factors related to survival rates are age, histologic subtype, tumor grade, tumor size, and the extent of the disease.1,12 Because spinal CS is resistant to chemotherapy and conventional radiation therapy, adjuvant radiation therapy is used for any residual tumor after incomplete resection, and this therapy has been found to improve the prognosis of metastatic patients.1,5 The overall survival rate varies across different histological gradings. 11 The 10-year survival rates are 90% and 30% to 40% for Grade I CS and high-grade CS, respectively. 11
A literature search was performed on 1 August 2020 of the PubMed, Medline, and Cochrane Library databases, with the search covering studies published from 1990 to 2019, according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines 13 (Figure 6). The eligibility criteria specified studies and case reports describing patients with primary intraosseous CS involving the L-spine who received surgical interventions. Articles including descriptions of the surgical methods, follow-up time, recurrence, and outcomes were further selected and investigated manually. We searched the databases using three keywords, namely, “primary”, “chondrosarcoma”, and “spine”, filtered with the race of “Human”, which resulted in 160 articles being identified. Next, we screened the abstracts of these articles, excluding articles in which the lesion did not involve the L-spine, those not describing the surgical interventions, and those in which the tumors were extraosseous, such as epidural lesions. After reviewing the full-text articles, we further excluded articles or cases describing non-L-spine disease locations, distinct tumor types other than CS, or with incomplete descriptions of the surgical methods. As a result, eight articles discussing 23 cases were selected.8–10,14–18
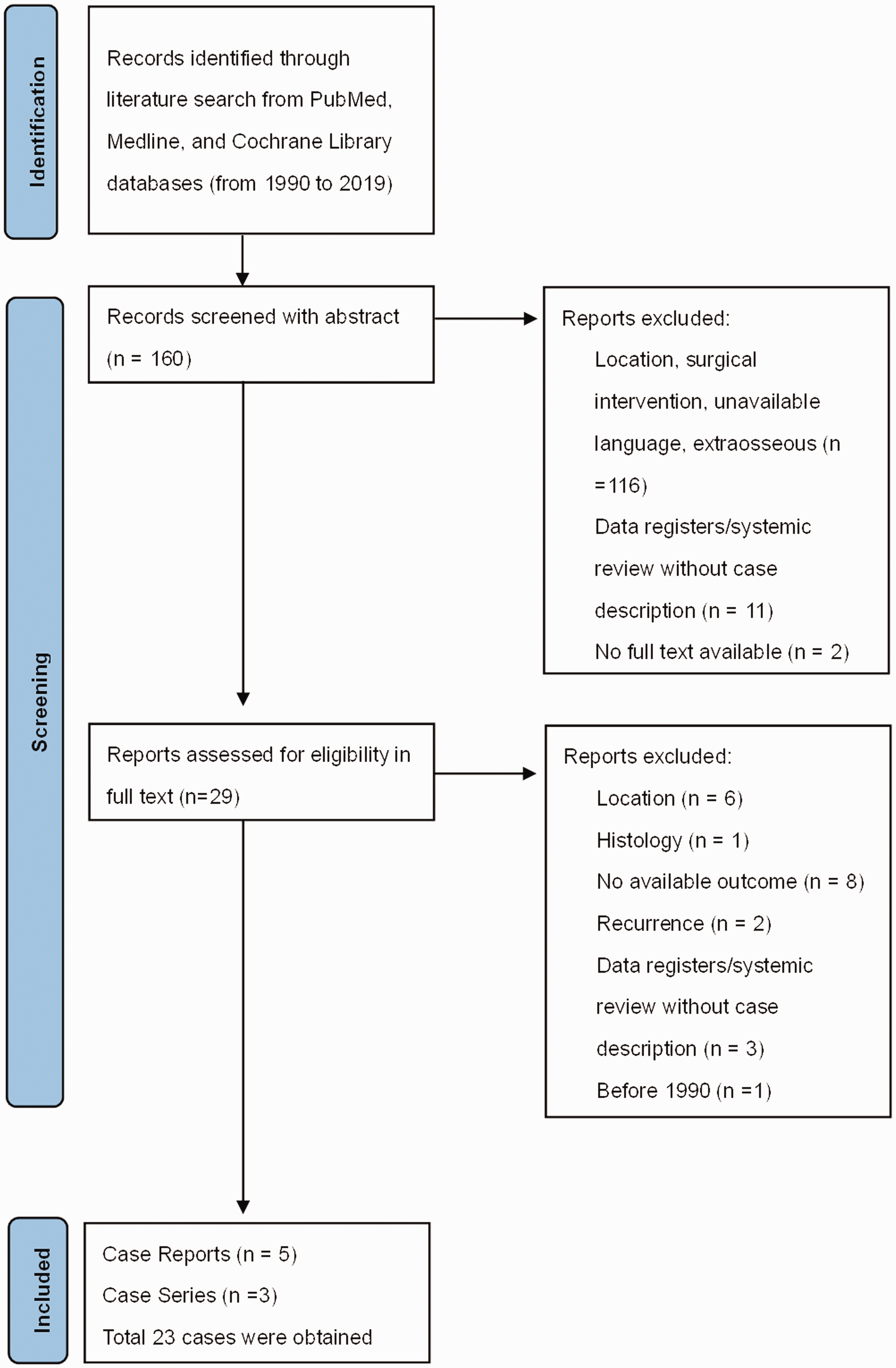
A flowchart showing the literature search and analysis process.
The characteristics of the selected cases, including the present case, are listed in Table 1. The patients’ average age was 39.42 ± 19.8 years (mean ± standard deviation (SD)), and the patients comprised 13 men and 11 women. The distribution of the CS locations for the 23 cases was as follows: L1 (n = 4), L2 (n = 8), L3 (n = 6), L4 (n = 5), and L5 (n = 5).
List of primary intraosseous lumbar CS cases receiving surgical intervention.

F, female; M, male; T, thoracic; L, lumbar; CS, chondrosarcoma; CFP, carbon fiber prosthesis; TPS, traditional pedicle screw; mo, months; PBth, proton beam therapy; RT, radiotherapy; CT, chemotherapy; NED, no evidence of disease; DOD, death of disease; DUD, death unrelated to disease.
ISOLA®, bioMérieux, Marcy l’Etoile, France; VSP®, AcroMed, Cleveland, OH, USA.
Further analysis was performed, and the results are shown in Table 2. Among the 16 patients who underwent en bloc surgery, 7 underwent two-stage surgery, while 9 underwent one-stage surgery. The piecemeal/subtotal group had a significantly lower survival rate (p < 0.001 (Chi-square test)), and the recurrence rate in this group was also higher (87.5%) than that of the en bloc group (18.8%). Two patients in the two-stage en bloc group received adjuvant chemotherapy with an intralesional approach or at a contaminated margin, whereas two patients in the one-stage en bloc group received adjuvant chemotherapy according to the chemotherapy guidelines for pediatric sarcoma. Generally, the results showed a better prognosis following en bloc surgery, similar to findings in previous studies.4,6,7,11
Nearly half of the patients in the en bloc surgery group underwent two-stage surgery (43.7%),8–10,14–16,18 including the patient in our case. Patients with multisegment disease tended to receive two-stage approaches (75%, 3 of 4 patients).10,15,17 In contrast, one-stage approaches were preferred for single-segment lesions (66.7%, 8 of 12 patients).14,17 All of the subtotal/piecemeal (100%) approaches were intralesional14,16,17; however, only 31.2% of the en bloc cases were treated using an intralesional route (2 one-stage and 4 two-stage cases).8,10,14,17,18
The most common pathological type of osseous CS among the collected cases was the conventional type,10,14 which accounted for 50% of all cases. Notably, eight of nine (88.9%) one-stage en bloc cases were the conventional type. 14 However, some of the studies and case reports did not describe the histologic type of the CS.9,16 The mean follow-up time for the two-stage group was 45 months, while that for the one-stage group was 85 months. No recurrence was noted in the two-stage group,8–10,14–16,18 while the recurrence rate in the one-stage group was 33% (three of nine patients, with one death from the disease). 14 However, there was no significant difference in the recurrence rate between the two groups (p = 0.09 (Chi-square test)). All of the en bloc cases (2/2) with the mesenchymal type of CS underwent two-stage surgery, but no subsequent recurrence or death occurred.15,18 The higher recurrence rate observed for the one-stage group may be related to the difficulty of achieving 360° exposure of a tumor that involves the vertebrae and the increased technical difficulties associated with attempting to remove all of the tumors at the same time, especially in CS cases involving multiple segments or all three vertebral columns. In addition, some bias may exist owing to the limited case numbers.
Previous reviews have indicated that en bloc surgery results in a better prognosis compared with piecemeal resection or other surgical methods, with the avoidance of intralesional contamination also being mentioned.1,5,7 However, increased blood loss, prolonged operation duration, and the loss of stability owing to extensive surgical resection cannot be ignored.5,7 In the present case, we performed two-stage surgery to achieve total tumor resection, to preserve neurological function, and to enhance stabilization. No sign of recurrence was noted in the described case at the 2-year follow-up.
Our analysis of studies from the last 30 years showed that in contrast to one-stage surgery, two-stage surgery appears to be beneficial in treating multisegment disease, providing a lower rate of recurrence. Hence, two-stage surgery may be an adequate method for treating low-grade tumors, tumor subtypes with a better prognosis, or tumors with extensive invasion. However, there is still room for further discussion concerning the most appropriate choice of surgical method. The histological type and CS grade were not well recorded in all of the literature that we reviewed. Additionally, evidence based on histological classifications might be helpful in building a decision tree to help CS patients achieve better prognoses and fewer complications.
Using the previous studies, a relationship was identified between CS occurrence and previous cancer history or genetic abnormalities.4,19 The amplification of the c-Myc oncogene has been associated with the malignant degeneration of CS, and the loss of chromosome 6 and the gain of 12q12 have also been correlated with high-grade CS. 3 Childhood malignancies, such as Wilms tumor, Ewing sarcoma, and Hodgkin lymphoma, increase the risk of developing bone sarcoma. 19 Although our patient had no history of cancer or radiation therapy, additional genetic abnormalities should be considered.
Primary spinal CS is rare. 3 En bloc resection and avoiding intralesional curettage can lower the associated recurrence rate and mortality, and enhance overall survival.1,5 However, multiple factors have been identified as adversely affecting survival rates, including older age, higher tumor grade, inadequate surgical margins, and local recurrence.1,12 The case presented herein demonstrates a promising method of two-stage surgery for an extensively invasive tumor that provided good postoperative stability and good recovery, without recurrence.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211058890 - Supplemental material for Primary osseous chondrosarcoma in the lumbar spine: case report and literature review with analysis
Supplemental material, sj-pdf-1-imr-10.1177_03000605211058890 for Primary osseous chondrosarcoma in the lumbar spine: case report and literature review with analysis by Chih-Hisu Tu, You-Pen Chiu, Hui-Ru Ji and Cheng-Di Chiu in Journal of International Medical Research
Footnotes
Availability of data and materials
The datasets used and/or analyzed in the current study are available from the corresponding author upon reasonable request.
Author contributions
CDC designed the study. HRJ acquired the patient’s data. YPC and CDC analyzed and interpreted the data and drafted the manuscript. CHT and CDC revised the manuscript critically for important intellectual content. All authors read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: The present study was supported by a grant from China Medical University Hospital [DMR-108-062]. The China Medical University Hospital also provided financial support for English editing of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.