
Abstract
Study Design:
Systematic literature review.
Objective:
It is estimated that one third of the world population is overweight and 20% of adults have some low back symptoms at some point of their lives. The association of obesity and low back pain and physical deterioration has been well established. We designed this study to evaluate the role of bariatric surgery (BS) for lumbar spine symptoms in obese patients.
Methods:
A systematic literature review was performed using the PubMed database identifying lumbar spine symptoms (pain, functional status, disability index) and/or complications of lumbar spine surgery before and after BS. Study quality was assessed according to the Oxford Centre for Evidence-Based Medicine.
Results:
Ten studies were identified. Nine evaluated the role of BS in low back pain and/or functional status before and after surgery: all reported that bariatric surgery had a positive impact in improving low back pain symptoms and decreasing disability in severely obese patients. One study evaluated the role of posterior lumbar surgery in patients who were obese at the time of surgery and those who had a previous bariatric procedure: bariatric surgery decreased postoperative surgical complications. The level of the evidence was low (III and IV).
Conclusions:
Bariatric surgery in severely obese patients decreases the intensity of low back symptoms and also decreases disability secondary to back problems. Additionally, bariatric surgery may be advantageous for patients who need a posterior lumbar surgery and are severely obese. Prospective studies with longer follow-up are necessary to confirm this conclusion.
Introduction
About one third of the world population is overweight, and it is estimated that by 2030 nearly 40% of the world’s adult population will be overweight and 20% will be considered obese. 1,2 Obesity is a complex, multifactorial, and preventable disease. 2 Obesity today is standardized through the use of the body mass index (BMI), a ratio of an individual’s body weight to height. 2 BMI is calculated using the weight divided by the square of the body height (kg/m2). The resultant number may be grouped into different scales of obesity. When the BMI is ≥30, adults are classified as obese. A high BMI is associated with cardiovascular disease, type 2 diabetes, osteoarthritis, musculoskeletal disorders, depression, various forms of cancer, and many other systemic diseases. 3
Indications for bariatric surgery vary across regions and practices, but a BMI ≥ 40 without comorbidities or BMI ≥ 35 with at least one obesity related comorbidity (eg, hypertension, diabetes, nonalcoholic fatty liver disease, osteoarthritis, or heart disease) classifies a patient as morbidly obese and is generally an accepted indication for bariatric surgery after conservative weight loss measures have failed. 4
The association between obesity, back pain, and physical deterioration has been well established. 5 -7 Lumbar spine disease, such as low back pain (LBP) or lumbar disc herniation, is also extremely common and important from an economical and epidemiological point of view, affecting about 20% of the adult population. 8 The prevalence of obesity and lumbar spine disease, and the association between obesity and spinal symptomatology, has created a large economic and social burden on public health. This study intends to evaluate the impact of bariatric surgery for lumbar spine symptoms in obese patients.
Methods
We performed a systematic literature review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA). 9
The PICOS acronym used for our review is described as follows: Patient: Obese patients with low back pain/musculoskeletal symptoms Intervention: A bariatric surgery was performed to reduce weight Comparison: Functional/pain status without a bariatric surgery Outcomes: Does this treatment benefit? What are the adverse effects? Study types: Retrospective and prospective clinical trials
Search Strategy, Selection of Studies, and Data Collection
We included studies that discussed the differences in lumbar spine symptoms (pain, functional status, disability measurements) and/or complications of lumbar spine surgery before and after bariatric surgery.
The literature search was performed on July 30, 2018. Our search strategy was based on the following keywords and terms, using articles in English, French, Spanish, and Portuguese (PubMed database): First search: “bariatric,” “surgery,” “low back pain.” A total of 21 articles were reviewed and 7 included in our review. Second search: “bariatric,” “surgery,” “lumbar spine.” A total of 65 articles were reviewed and 3 were selected but only 2 included (one article was already included from the first search).
Cross-referenced articles were also screened and one additional article included. See Figure 1 for a flow chart of our search and the 10 articles included in our study. The 10 selected studies were reviewed independently and collaboratively, through virtual web conferences, by 2 authors (AFJ, AAP). Discrepancies were solved by consensus of the 2 authors.
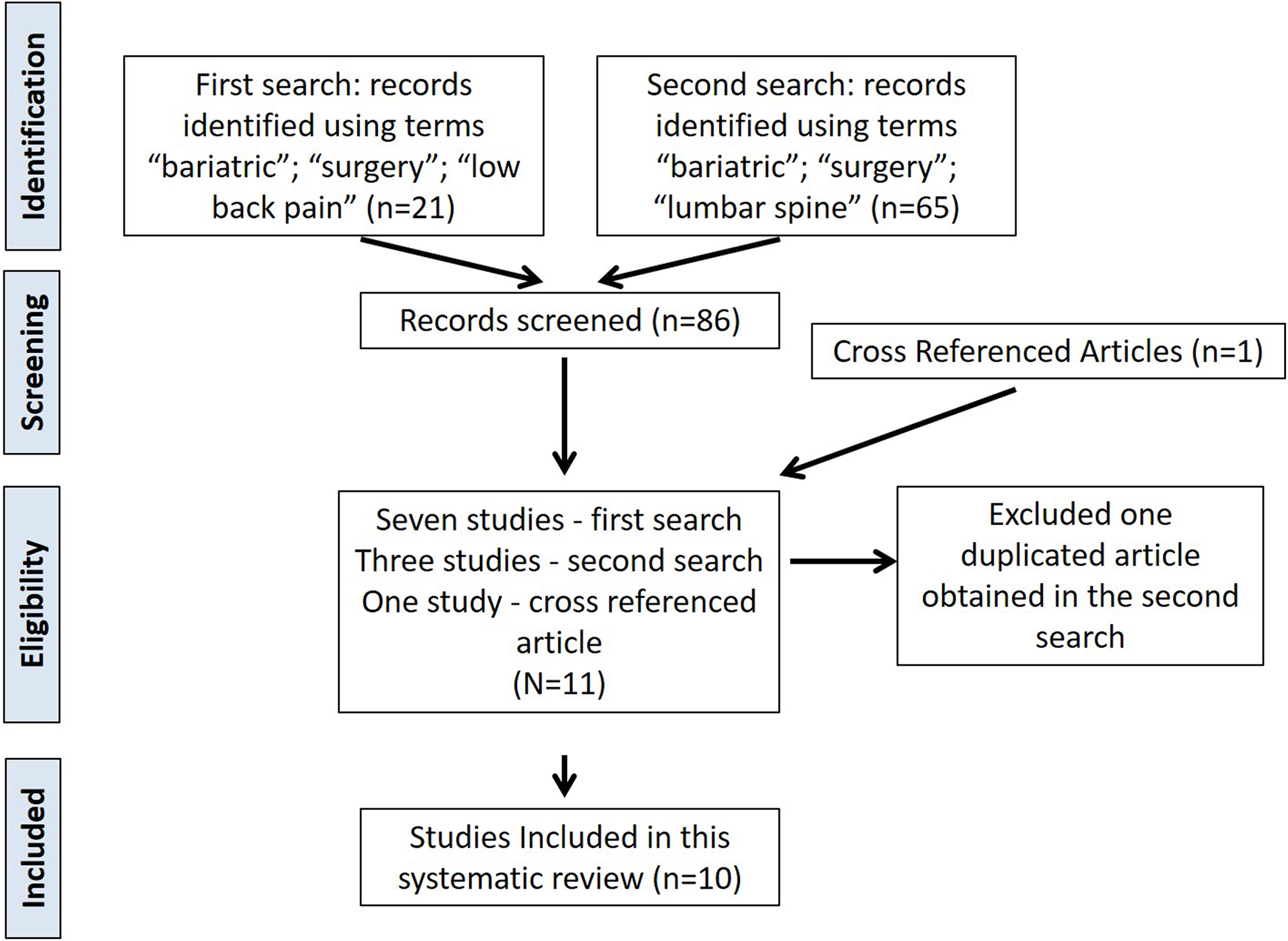
Flow chart of our search mechanism.
Data Extraction
All the data was extracted into a specific spreadsheet according to the number of patients in each group, study methodology, and main results/outcomes.
Methodological Quality Evaluation
We assessed a study’s quality according to the Oxford Centre for Evidence-Based Medicine Levels of Evidence categorization. 10
Data Extraction
Data was extracted in a spreadsheet, including the number of patients evaluated, outcome measurements, study methodology, and primary outcomes (Table 1).
Summary of the Findings of the 9 Included Articles About Low Back Pain/Functional Status Before and After Bariatric Surgery.
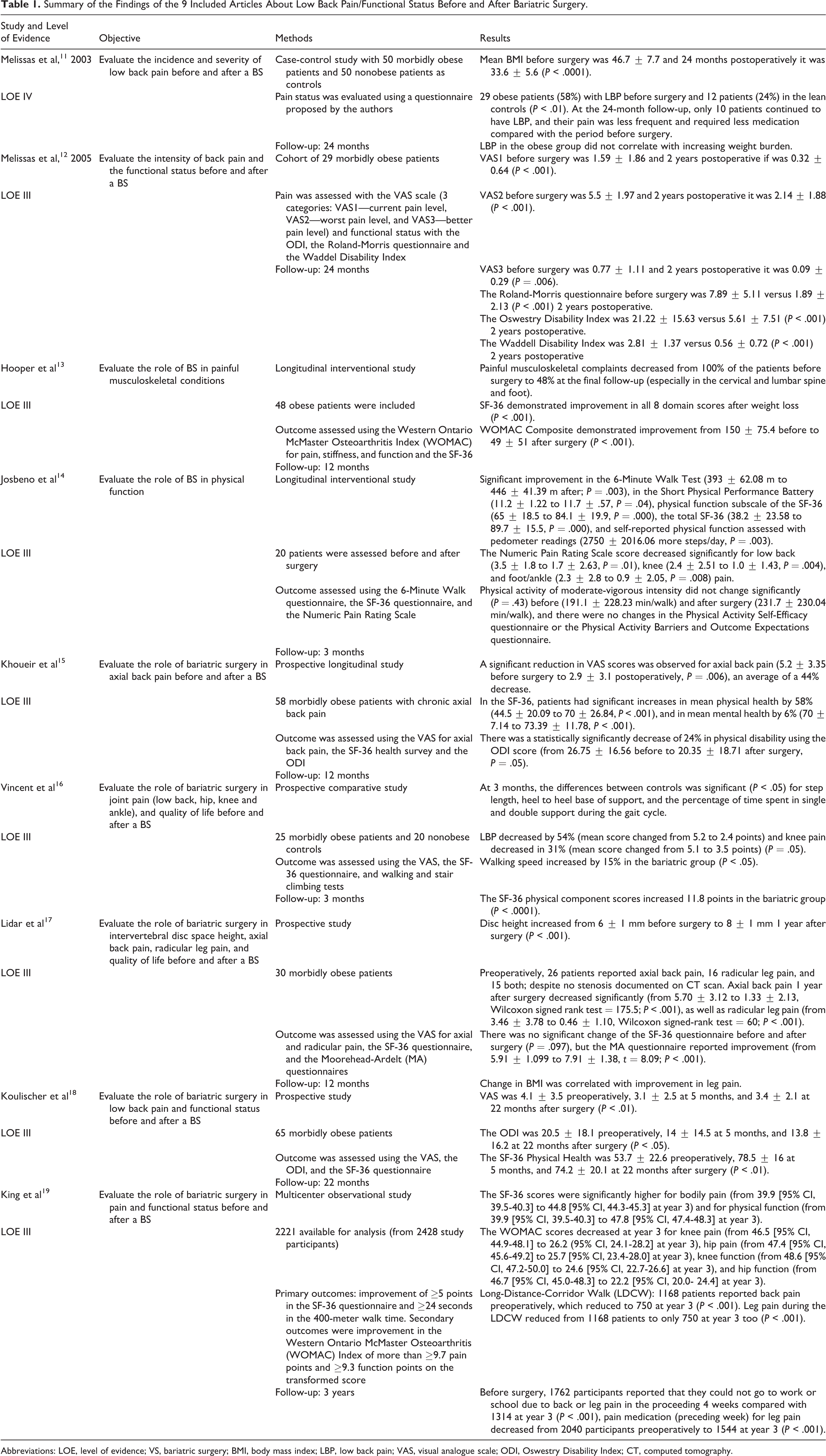
Abbreviations: LOE, level of evidence; VS, bariatric surgery; BMI, body mass index; LBP, low back pain; VAS, visual analogue scale; ODI, Oswestry Disability Index; CT, computed tomography.
Results
Of the 10 included articles, 9 evaluated the role of bariatric surgery in LBP and/or functional status of obese patients before and after surgery. 11 -19 Patient follow-up in the studies ranged from 3 months to 3 years. The total number of patients who underwent bariatric surgery and had follow-up assessment was 2526 (2221 from the multicenter study of King et al 19 ).
One article evaluated the role of posterior lumbar surgery and complications in patients who were obese at the time of surgery, obese patients who had a previous bariatric surgery, and patients with a normal BMI. 20 This article is discussed below separately from the other 9 articles.
Low Back Pain and/or Functional Status Before and After Bariatric Surgery
Melissas et al 11 performed a case-control study with 50 morbidly obese patients who underwent bariatric surgery (vertical band gastroplasty) and 50 nonobese patients as controls. Both groups were surveyed about the incidence and severity of low back pain. After 24 months, the morbidly obese patients were evaluated again. Pain status was evaluated using a questionnaire proposed by the authors describing pain intensity and frequency. The mean BMI before surgery was 46.7 ± 7.7 and 24 months postoperatively it was 33.6 ± 5.6 (P < .0001). There were 29 obese patients (58%) with low back pain before surgery and 12 patients (24%) in the lean controls (P < .01). Interestingly, LBP in the obese group did not correlate with increasing weight burden. At the 24-month follow-up, only 10 patients continued to have low back pain, and their pain was less frequent and required less medication compared with the period before surgery. They concluded that back pain was more frequent in obese patients than in the lean control and that weight reduction results in significantly less low back pain. Level of evidence (LOE) IV.
Melissas et al 12 performed a cohort study of 29 morbidly obese patients with back pain who had bariatric surgery. These patients were evaluated according to weight loss, functional status, and pain before and 2 years after a vertical banded gastroplasty. Pain was assessed using a visual analogue scale (VAS) and graded in 3 categories: pain immediately (current pain level; VAS1), at its worst pattern (VAS2), and at its best pattern (VAS3). The VAS1 before surgery was 1.59 ± 1.86 and 2 years postoperative it was 0.32 ± 0.64 (P < .001), the VAS2 before surgery was 5.5 ± 1.97 and 2 years postoperative it was 2.14 ± 1.88 (P < .001), and the VAS3 before surgery was 0.77 ± 1.11 and 2 years postoperative it was 0.09 ± 0.29 (P = .006). They also found a statistically significant improvement in functional status: the Roland-Morris Questionnaire before surgery was 7.89 ± 5.11 versus 1.89 ± 2.13 (P < .001) 2 years postoperative, the Oswestry Disability Index (ODI) was 21.22 ± 15.63 versus 5.61 ± 7.51 (P < .001) 2 years postoperative, and the Waddell Disability Index was 2.81 ± 1.37 versus 0.56 ± 0.72 (P < .001) 2 years postoperative. LOE III.
Hooper et al 13 performed a longitudinal interventional study to evaluate the role of bariatric surgery (open or laparoscopic Roux-en-Y gastric bypass) in painful musculoskeletal conditions. Of note, patients also received intensive nutritional counseling and were required to start an exercise program and quit smoking before surgery. A total of 48 obese patients were included. The outcomes were assessed using Western Ontario McMaster Osteoarthritis Index (WOMAC) for pain, stiffness, and function; and the SF-36 for quality of life. Follow-up assessment was performed at 6 to 12 months after surgery. The mean BMI before surgery was 51 ± 8 kg/m2 and at final follow-up it was 36 ± 7 kg/m2. Painful musculoskeletal complaints decreased from 100% of the patients before surgery to 48% at the final follow-up, especially in the cervical and lumbar spine, and foot. The only musculoskeletal conditions without improvement after weight loss were the shoulder, the hip, and the trochanteric bursa. Functional status assessed with the SF-36 demonstrated improvement in all 8 domain scores after weight loss, with a P value <.001 in all. The same improvement was observed in the WOMAC questionnaire (in all its subscales)—WOMAC Composite was 150 ± 75.4 before and 49 ± 51 after surgery (P < .001). The authors concluded that most musculoskeletal complaints decrease significantly after weight loss and physical activity. LOE III.
Josbeno et al 14 evaluated the role of bariatric surgery on physical activity and function in 20 patients who underwent gastric bypass surgery. Outcomes were assessed preoperatively and at 3 months postoperatively using the 6-Minute Walk Test, the SF-36 questionnaire, and the Numeric Pain Rating Scale. At 3 months after surgery, the mean weight loss was 24.4 ± 5.6 kg and the mean decrease in BMI was from 46.9 ± 6.3 kg/m2 to 37.4 ± 5.7 kg/m2 (P = .00). There was significant improvement in scores for the 6-Minute Walk Test (393 ± 62.08 m before surgery to 446 ± 41.39 m after; n = 17, P = .003), Short Physical Performance Battery (11.2 ± 1.22 to 11.7 ± .57; n = 18, P = .04), physical function subscale of the SF-36 (65 ± 18.5 to 84.1 ± 19.9, P = .000), the total SF-36 (38.2 ± 23.58 to 89.7 ± 15.5; n = 17, P = .000), and self-reported physical function assessed with pedometer readings (2750 ± 2016.06 more steps/day, P = .003). The Numeric Pain Rating Scale score decreased significantly for low back (3.5 ± 1.8 to 1.7 ± 2.63, P = .01), knee (2.4 ± 2.51 to 1.0 ± 1.43, P = .004), and foot/ankle (2.3 ± 2.8 to 0.9 ± 2.05, P = .008) pain. Physical activity of moderate-vigorous intensity did not change significantly (P = .43) before (191.1 ± 228.23 min/walk) and after surgery (231.7 ± 230.04 min/walk), and there were no changes in the Physical Activity Self-Efficacy questionnaire or the Physical Activity Barriers and Outcome Expectations questionnaire. The authors concluded that bariatric surgery helps in improving health-related quality of life, pain, and also some modest improvement in physical activity. LOE III.
Khoueir et al 15 performed a prospective longitudinal study to evaluate the role of bariatric surgery in axial back pain before and after bariatric surgery. A total of 58 morbidly obese patients with chronic axial back pain were initially enrolled. After 12 months, 38 patients (65%) were available for follow-up: 30 women and 8 men, with an average age of 48.46 years (range of 20-68 years). They were evaluated using a VAS for axial low back pain, SF-36 health survey, and the ODI. The mean weight was 144.52 ± 41.21 kg before and 105.59 ± 29.24 kg after surgery (P < .001). The mean BMI was 52.25 ± 12.61 kg/m2 before and 38.32 ± 9.66 kg/m2 after surgery (P < .001). There was a significant reduction in VAS scores for axial back pain (5.2 ± 3.35 before surgery to 2.9 ± 3.1 postoperative, P = .006), an average of a 44% decrease. In the SF-36, patients had significant increases in mean physical health by 58% (44.5 ± 20.09 to 70 ± 26.84, P < .001), and in mean mental health by 6% (70 ± 7.14 to 73.39 ± 11.78, P < .001). There was also a statistically significantly decrease of 24% in physical disability using the ODI score (from 26.75 ± 16.56 before to 20.35 ± 18.71 after surgery, P = .05). LOE III.
Vincent et al 16 performed a prospective comparative study to evaluate the role of bariatric surgery in joint pain using numeric pain scales (low back, hip, knee, and ankle), walking and stair climbing, and quality of life (using the SF-36 questionnaire). A total of 25 morbidly obese patients had bariatric surgery (laparoscopic Roux-en-Y gastric bypass or laparoscopic adjustable gastric banding), with 20 nonsurgical controls for comparison. The surgical group lost an average 21 ± 7.7 kg. At 3 months, the differences between controls was significant (P < .05) for step length, heel to heel base of support, and the percentage of time spent in single and double support during the gait cycle. Low back pain decreased by 54% (mean score changed from 5.2 to 2.4 points) and knee pain decreased in 31% (mean score changed from 5.1 to 3.5 points), compared with no changes in the control group (P = .05). Walking speed increased by 15% in the bariatric group (P < .05) with no changes in the control group. The SF-36 physical component scores increased 11.8 points in the bariatric group, and there was no change in the control group (P < .0001). The authors concluded that bariatric surgery improved many gait parameters, as well as pain status and quality of life after 3 months in this case-control study. LOE III.
Lidar et al 17 performed a prospective study to evaluate the role of bariatric surgery on the intervertebral disc space height, axial back pain, radicular leg pain, and quality of life in 30 morbidly obese adults. Disc space height at the L4-5 level was evaluated with computed tomography (CT) scans before and 1 year after surgery. Visual analogue scale was used to evaluate axial and radicular pain; the 36-Item Short Form Health Survey and Moorehead-Ardelt (MA) questionnaires were used to evaluate quality of life. Bariatric surgeries performed included the following: laparoscopic gastric band, banding, sleeve gastrectomy, laparoscopic Roux-en-Y gastric bypass, and duodenal switch procedure. There was no physiotherapy or rehabilitation after surgery. The average BMI before surgery was 42.8 ± 4.8 kg/m2 and 29.7 ± 3.4 kg/m2 after surgery (P < .001). The body weight decreased from 119.6 ± 20.7 kg to 82.9 ± 14 kg (P < .001). There was a significant increase in disc height (from 6 ± 1 mm before surgery to 8 ± 1 mm 1 year after surgery, P < .001). Preoperatively, 26 patients reported axial back pain, 16 radicular leg pain, and 15 both, despite no stenosis documented on CT scan. Axial back pain 1 year after surgery decreased significantly (from 5.70 ± 3.12 to 1.33 ± 2.13, Wilcoxon signed rank test = 175.5; P < .001), as well as radicular leg pain (from 3.46 ± 3.78 to 0.46 ± 1.10, Wilcoxon signed-rank test = 60; P < .001). There was no significant change of the SF-36 questionnaire before and after surgery (P = .097), but the MA questionnaire reported improvement (from 5.91 ± 1.099 to 7.91 ± 1.38, t = 8.09; P < .001). Change in BMI was correlated with improvement in leg pain. LOE III.
Koulischer et al 18 evaluated prospectively 65 patients that were candidates for bariatric surgery (gastric bypass, mini-gastric bypass, and sleeve gastrectomy). A total of 54 patients (80%) were available for analysis 5 months postoperative and 47 patient (72%) 22 months postoperative. The mean weight loss at 22 months was 19 ± 9 kg (P < .001), and the mean BMI was 43 ± 5.2 kg/m2 before surgery and 33 ± 5.1 kg/m2 (P < .001) at 5 months postoperative. Functional and low back pain evaluation was performed using the Numeric Rating Scale (NRS; an analogue to the VAS), ODI, and SF-36 scores. The NRS was 4.1 ± 3.5 preoperatively, 3.1 ± 2.5 at 5 months, and 3.4 ± 2.1 at 22 months after surgery (P < .01). The ODI was 20.5 ± 18.1 preoperatively, 14 ± 14.5 at 5 months, and 13.8 ± 16.2 at 22 months after surgery (P < .05). The SF-36 Physical Health was 53.7 ± 22.6 preoperatively, 78.5 ± 16 at 5 months, and 74.2 ± 20.1 at 22 months after surgery (P < .01). They concluded that after bariatric surgery and weight loss there was improvement of lumbar pain and functional status of the patients. LOE III.
King et al 19 performed a multicenter, observational study evaluating the effect of bariatric surgery (Roux-en-Y gastric bypass and laparoscopic adjustable gastric banding) on improvement in pain and physical function in the first 3 years after surgery. Primary outcomes were based on improvement of ≥5 points in the SF-36 questionnaire and ≥24 seconds in the 400-meter walk time. Secondary outcomes were improvement in the WOMAC Index of more than ≥9.7 pain points and ≥9.3 function points on the transformed score. A total of 2221 patients had data available for analysis (from 2428 study participants), with pain and function status assessed at 1 year postoperative in 2042 participants (84%), 1794 (74%) at 2 years, and 1724 (72%) at 3 years. The SF-36 scores were significantly higher for bodily pain (from 39.9 [95% confidence interval (CI) 39.5-40.3] preoperatively to 44.8 [95% CI 44.3-45.3] at year 3) and for physical function (from 39.9 [95% CI 39.5-40.3] preoperatively to 47.8 [95% CI 47.4-48.3] at year 3). There was also a decrease in the WOMAC scores at year 3 for knee pain (from 46.5 [95% CI 44.9-48.1] preoperatively to 26.2 [95% CI 24.1-28.2] at year 3), hip pain (from 47.4 [95% CI 45.6-49.2] preoperatively to 25.7 [95% CI 23.4-28.0] at year 3), knee function (from 48.6 [95% CI 47.2-50.0] preoperatively to 24.6 [95% CI 22.7-26.6] at year 3), and hip function (from 46.7 [95% CI 45.0-48.3] preoperatively to 22.2 [95% CI, 20.0- 24.4] at year 3). These improvements suggested that knee and hip pain decreases and function improves after surgery. During the Long-Distance-Corridor Walk (LDCW), 1168 patients reported back pain preoperatively, which reduced to 750 at year 3 (P < .001). Leg pain during the LDCW reduced from 1168 patients to only 750 at year 3 too (P < .001). Before surgery, 1762 participants reported that they could not go to work or school due to back or leg pain in the proceeding 4 weeks compared with 1314 at year 3 (P < .001). Finally, pain medication (preceding week) for leg pain decreased from 2040 participants at baseline to 1544 at year 3 (P < .001). The authors concluded that among the patients who underwent bariatric surgery, there was improvement in baseline pain and physical function over 3 years. They stated, however, that the improvement decreased between year 1 and year 3 following surgery. LOE III.
The evidence obtained according to Oxford Centre for Evidence-Based Medicine Levels of Evidence categorization the of the 9 evaluated studies was considering as level III in 8 studies 12 -18 and level IV in one of them (a case-control study). 11
Complications of Posterior Lumbar Surgery
Jain et al 20 performed a retrospective cohort study to determine the impact of bariatric surgery on perioperative complications of posterior lumbar fusion. Patients undergoing a posterior lumbar fusion in the State Inpatient Databases of New York, Florida, North Carolina, Nebraska, Utah, and California were included. Outcome evaluation included 30 medical and surgical complications, death, readmission, and hospital length of stay (LOS).
A total of 156 517 patients who underwent posterior lumbar fusion were included and divided into 3 groups: 590 patients who underwent bariatric surgery, 5791 obese patients with a BMI > 40 (severely obese), and 150 136 normal weight patients (BMI < 25).
When comparing patients of group 1 (who underwent a BS) with those of group 2 (severely obese), the first had lower rates of complications such as respiratory failure (odds ratio [OR] 0.59, P = .019), urinary tract infection (OR 0.64, P = .031), acute renal failure (OR 0.39, P = .007), overall medical complications (OR 0.59, P < .001), and infection (OR 0.65, P = .025). Additionally, patients who underwent a BS had a shorter hospital LOS. Interestingly, comparing group 1 with group 3 (normal weight patients), there were higher rates of infection in BS patients (OR 2.70, P < .001), higher reoperation rates (OR 2.05, P = .045), and also more hospital readmissions (OR 1.89, P < .001).
The authors concluded that bariatric surgery before elective posterior lumbar fusion decreases complications compared with severely obese patients, even though the profile of complications are still higher than those who had a normal BMI. Finally, the authors proposed that severely obese patients should be considered for BS before undergoing a lumbar fusion.
Discussion
In our review, a total of 2526 patients underwent bariatric surgery for treatment of obesity and had available follow-up assessment for functional status and/or back pain. Although the follow-up was relatively short, ranging from 3 months to 3 years, all 9 included studies reported that bariatric surgery has a positive impact on improving low back pain symptoms, physical function, and/or decreasing disability in severely obese patients. It is also important to mention that there was a significant amount of body weight loss and, consequently, decreased BMI in all studies evaluated.
Although low back pain evaluation criteria was heterogeneous in our study sample, in all 9 studies there was statistically significant improvement in low back pain after surgery. 11 -19 Radicular leg pain was evaluated in the study of Lidar et al, with significant improvement (VAS from 3.46 ± 3.78 before surgery to 0.46 ± 1.10 in the last follow-up, Wilcoxon signed-rank test = 60; P < .001). Finally, musculoskeletal complaints were evaluated in 3 of the included articles, with improvements documented for cervical, foot, ankle, and knee pain. 13,14,19
The potential explanations for pain improvement may be mechanical in nature and directly related to decreased load on the muscles and joints, subjective improvement of well-being and self-perception, and/or change in lifestyle after surgery with more physical activity. Interestingly, in a paper not included in our review because it was not indexed in the PubMed database, the authors found a worsening of preexisting back pain or new onset of low back pain after bariatric surgery in 30 patients with a BMI ≥ 30. 21 The authors speculated that pain may exacerbate after surgery due to a decrease of intraabdominal pressure that may change spinal biomechanics. According to the authors, a high intraabdominal pressure unloads the spine, by producing an extensor moment on the lumbar spine that lessens the erector spinaes muscle burden. After surgery, decreasing intraabdominal pressure with decreasing body weight results in a forward bending and kyphosis, which may result in low back pain and radiculopathy. 22,23 Although low back pain may be present after bariatric surgery, the methodology of the Skaf et al 21 study diverges from our systematic review—they included obese patients with back pain that worsened post bariatric surgery (a selection bias). It is obvious that, due to its high prevalence and multifactorial etiology, some patients may have episodes of back pain despite a bariatric procedure. However, in all included articles of our review, there was a significant improvement in low back pain.
The included studies also reported improvement in patients’ function after surgery, which was measured using various outcome measurements such as ODI, SF-36, the Waddel Disability Index, 6-Minute Walk Test, and others. 11 -14,16 -19 Improvement in physical fitness and function improves general health and may allow patients to exercise more readily, possibly explaining a decrease in musculoskeletal pain.
Finally, bariatric surgery prior to a posterior lumbar fusion seems to have a protective effect on postoperative complications. 20 For morbidly obese patients in which a lumbar posterior surgery is indicated, if acceptable to be postponed, a bariatric surgery prior to spinal surgery may be a reasonable option to decrease the risk of complications related to the lumbar procedure. However, risk may continue to be higher than among nonobese patients.
Our systematic literature review is limited by the small number of patients, heterogeneity of the study and types of bariatric interventions, different outcome assessment measurements, and low level of evidence in all studies. However, it was evident that bariatric surgery has a favorable impact on low back symptoms and improves function of obese patients, at least for the time period available during the studies. Longer follow-up studies with better methodological designs are necessary to evaluate the role of bariatric surgery as a primary treatment of low back symptoms in this population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Alpesh A. Patel discloses the following: Consulting: Zimmer Biomet, DePuy Synthes, nView, Amedica, Kuros Biosciences; Product Design/Royalties: Nuvasive, Zimmer Biomet, Amedica; Stock options/Ownership (<1%): Amedica, Vital5, Nocimed, Cytonics, Tissue Differentiation Intelligence, Endoluxe, nView; Institutional Fellowship Program Support: NuVasive, AO Spine North America; Board of Directors (non-financial): Cervical Spine Research Society, Lumbar Spine Research Society Editorial Board; and Contemporary Spine Surgery: Journal of American Academy of Orthopaedic Surgery (Deputy Editor).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.