
Abstract
Study Design
Retrospective cohort study
Objectives
To describe the common types of complications and their risk factors during spine surgery in patients with achondroplasia.
Methods
A retrospective review was performed of medical records of adult achondroplasia patients who underwent spine surgery at our institution between 2007 and 2021. Inclusion criteria were achondroplasia and age >16 years. Surgical encounters were evaluated for durotomy, postoperative neurologic deficit, wound compromise, medical complications, and return to the operating room. Statistical analysis included evaluation of relationships across complications and fisher exact test applied to bivariate/categorical variables and t-test/ANOVA for continuous variables. Multivariable analysis using logistic regression was performed to account for patient characteristics
Results
Fifty-five patients with achondroplasia underwent 95 surgeries. Forty-nine percent of the surgeries involved a complication. These included durotomy (33.7%), neurologic deficit (11.6%), wound compromise (6.3%), and other medical complications (6.3%). Thirteen percent of surgeries required return to the operating room. The greatest number of complications occurred in thoracolumbar region (60.0%) compared to cervicothoracic (18.2%) and craniocervical junction (33.3%). Chronologically later surgical encounters had decreased complications and durotomies only occurred in thoracolumbar surgeries (45.7%).
Conclusions
Adult patients with achondroplasia undergoing surgery chronologically later in this set of consecutive patients were at a decreased risk for complications. Thoracolumbar surgeries were at the greatest risk for durotomies. Male sex was a risk factor for durotomy, while age was a risk factor for neurologic deficit. The potential for adverse surgical events should be considered when evaluating patients with achondroplasia for spine surgery.
Introduction
Skeletal dysplasias, or osteochondroplasias, encompass hundreds of disorders which affect the growth, development, and maturity of bone and cartilaginous structures. The most common of these is achondroplasia which occurs in around 1/25,000 births. 1 Achondroplasia is inherited in an autosomal dominant pattern, with the majority of mutations in the FGFR3 gene occurring spontaneously. 2 While there are no defined criteria which describe the clinical presentation of achondroplasia, there are common occurring features. Typical phenotype of patients with achondroplasia includes short stature, proximal shortening of the limbs, macrocephaly with frontal and/or parietal bossing, midfacial retrusion, and hypermobility of the hips and knees. 2 In addition, these patients also exhibit thoracolumbar kyphosis, lumbar hyperlordosis, and short pedicles.3-5
Due to the altered osteogenic development of the spine, these patients may develop spinal stenosis leading to spinal cord and/or cauda equina compression which manifests as neurogenic claudication, pain, radiculopathy, myelopathy and bowel/bladder dysfunction. 2 Of those with achondroplasia, 20-50% of adults have symptomatic spinal stenosis, and up to 78% of those have neurologic sequelae.6,7 This rate of symptomatic spinal stenosis is much higher than the 11% reported in the general population. 8 Given the unique anatomy that leads to neurologic deficit and injury, patients with achondroplasia are at increased risk for complications during surgical intervention. Specifically, achondroplastic individuals may be at increased risk for dural tears due to altered connective tissue development, decreased epidural fat, and smaller spinal canal.9,10 While there have been prior analyses of patients with skeletal dysplasia following spinal surgery, here we report the largest modern series evaluating the perioperative complications and potential risk factors in this unique patient population.
Material and Methods
Institutional Review Board approval (STUDY00001429) was obtained to retrospectively evaluate the medical records of patients with achondroplasia who underwent spine surgery at a single institution between 2007 and 2021. A Waiver of Consent/HIPAA Authorization was approved for this retrospective analysis. Potential subjects were identified utilizing Deep 6 AI™ (Pasadena, CA) and the keywords “achondroplasia” and “spine surgery or laminectomy or interbody”. These keywords identified 122 patients. Sixty-seven patients were excluded due to age <16 years at time of surgery, history of skeletal dysplasia other than achondroplasia, or insufficient clinical data. Our final cohort consisted of 55 patients who underwent 95 surgical encounters including either open laminectomy, instrumented arthrodesis alone, or laminectomy and instrumented arthrodesis.
For each of the 95 surgical encounters, patient demographics including sex, age, and BMI at time of surgery were recorded. Surgical encounter details included surgical location (craniocervical junction, cervicothoracic, or thoracolumbar), surgical type (open laminectomy, instrumented arthrodesis alone, laminectomy and instrumented arthrodesis, and/or interbody use), number of levels operated on, and history of prior surgery at that level. Length of inpatient stay was recorded, and perioperative complications were defined as complications occurring prior to day of discharge. Total length of follow-up was also noted, including any delayed complications that occurred in this time frame. Surgical records and perioperative notes were reviewed to identify the most common complications previously reported by other authors including dural tear, persistent neurologic deficit present at discharge from hospital, wound infection, and wound dehiscence. Medically-related complications including deep vein thrombosis (DVT), pulmonary embolism (PE), myocardial infarction, and prolonged intubation (remained intubated post-operatively) during the postoperative hospital stay were also noted. Once complications were identified, they were categorized as either durotomy, wound compromise, neurologic deficit, or other. Return to operating room (OR) during the study length period was also recorded, as well as the reason for reoperation and length of time elapsed following the prior surgical encounter.
Statistical Analysis
Demographics and General Characteristics of Surgical Encounters.
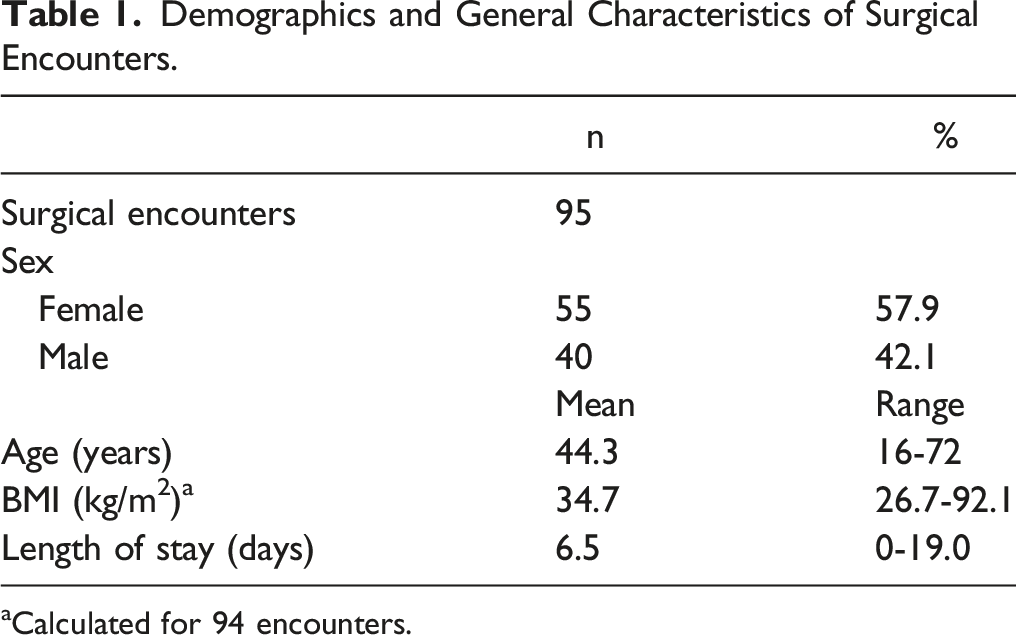
aCalculated for 94 encounters.
Surgical Procedure Characteristics.
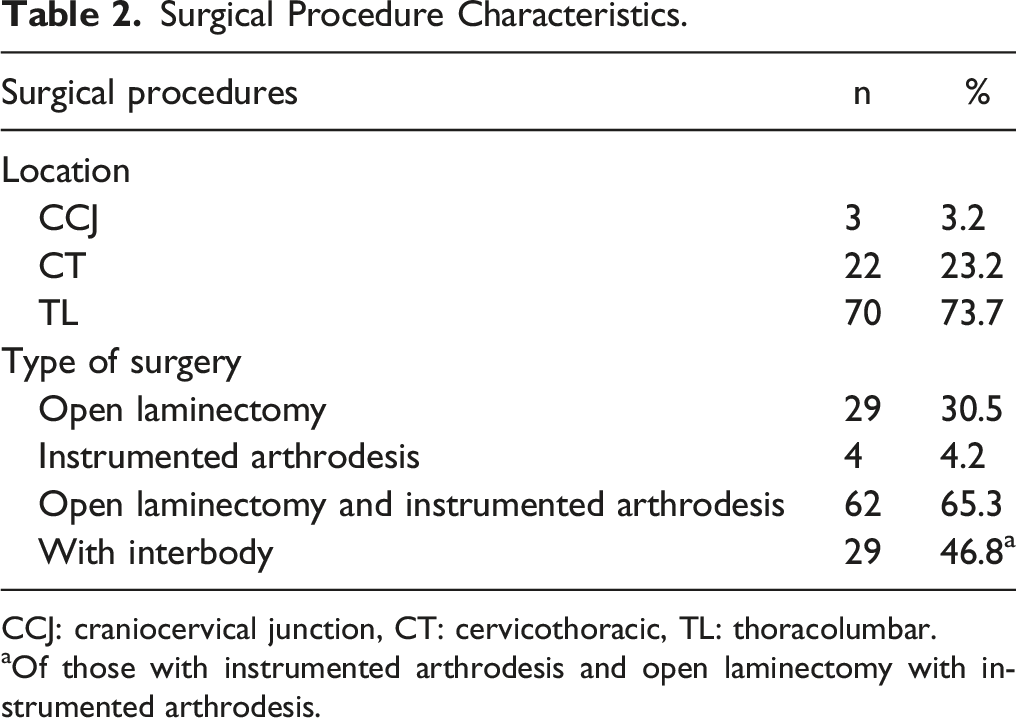
CCJ: craniocervical junction, CT: cervicothoracic, TL: thoracolumbar.
aOf those with instrumented arthrodesis and open laminectomy with instrumented arthrodesis.
Spine Surgery Encounter Complications.
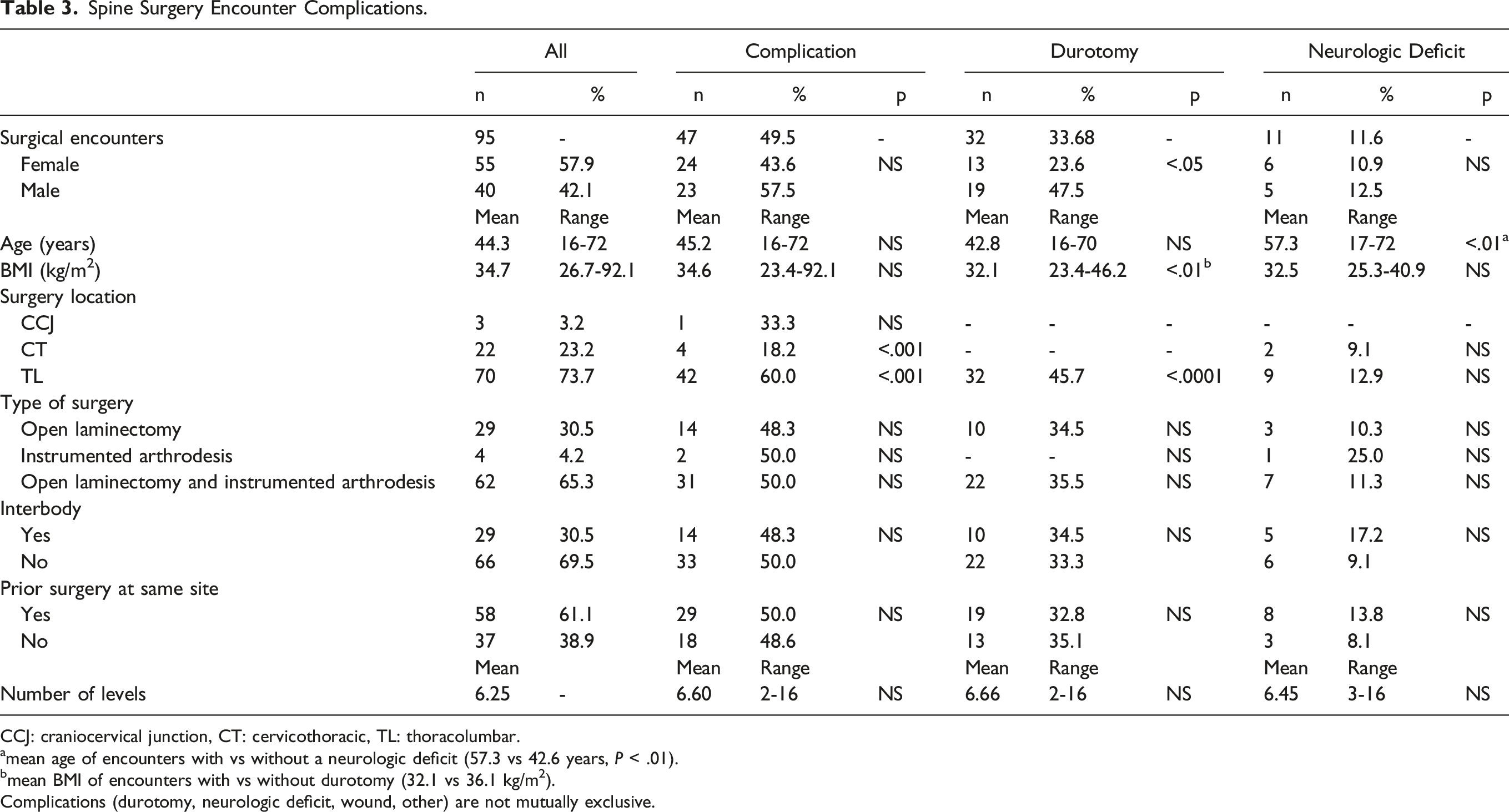
CCJ: craniocervical junction, CT: cervicothoracic, TL: thoracolumbar.
amean age of encounters with vs without a neurologic deficit (57.3 vs 42.6 years, P < .01).
bmean BMI of encounters with vs without durotomy (32.1 vs 36.1 kg/m2).
Complications (durotomy, neurologic deficit, wound, other) are not mutually exclusive.
Results
A total of 55 patients with achondroplasia who underwent 95 surgeries were included in the final patient cohort. All patients underwent elective procedures and there were no emergent procedures included. The mean age was 44.3 years and range 16-72 years. Fifty-five of the encounters were female (57.9%), and the average preoperative BMI was 34.7 kg/m2. The average length of stay for each encounter was 6.5 days (range 0 -19 days), and the average length of patient follow-up was 245 days (n = 52 patients). (Table 1) three surgeries occurred in the craniocervical junction, 22 in the cervicothoracic spine, and 70 in the thoracolumbar spine. Twenty-nine encounters involved decompression only, 4 instrumented arthrodesis alone, and 62 included both laminectomy and instrumented arthrodesis. (Table 2) Twenty-nine encounters with instrumented arthrodesis included interbody placement, 58 involved prior surgery at the same spinal level, and the average number of operative levels per encounter was 6.25. (Table 3)
Forty-seven of the surgeries (47/95, 49.5%) involved a complication. These included durotomy in 33.7% (32/95), neurologic deficit in 11.6% (11/95), and wound compromise in 6.3% (6/95). Other complications were noted in 6.3% (6/95) of the surgical encounters. These complications included 1 epidural hematoma, 3 hardware failures, 1 pulmonary embolism, and 1 prolonged intubation. No patients suffered myocardial infarction or deep vein thrombosis. (Table 3) Of the perioperative complications, 13.7% (13/95) of encounters required return to the operating room. Indications for return to the OR included wound infection (3), wound dehiscence (3), pseudomeningocele (3), instrumentation failure (2), seroma (1), and epidural hematoma (1). The average number of days between index surgical encounter and return to OR was 36.2 days (SD 38.6, range 3-133 days).
Overall, the greatest number of complications were in patients who underwent thoracolumbar surgery 60.0% (42/70) compared to cervicothoracic 18.2% (4/22) and craniocervical junction surgery 33.3% (1/3) (P < .001). Further analysis of encounters with complications demonstrated durotomies only in thoracolumbar surgeries 45.7% (32/70) compared to none in the cervicothoracic or craniocervical junction (P < .0001). Male sex, lower BMI, and thoracolumbar surgery had increased incidence of durotomy (P < .05, P < .01). Neurologic deficits were associated with increased age (mean 57.3 vs 42.6 years, P < .01), and further subgroup analysis of laminectomy and instrumented arthrodesis surgeries also demonstrated increased age (>49 years, P < .001). (Table 3) Chronologically later surgical encounters in this cohort had decreased complications (P < .05), and this relationship was stable when controlling for age and surgical levels. Increased age and history of prior spine surgery were not related to an increased risk of complication (NS) where age and number of surgical levels were positively related to year chronologically. Representative preoperative and postoperative images of 2 patients included in the cohort with low and high complexity thoracolumbar surgeries are demonstrated in Figure 1. Representative preoperative and postoperative images of low and high complexity thoracolumbar surgeries included in the study. Patient 1 had thoracic 7-8 cord compression on MRI thoracic spine T2 sagittal and axial images (A, B) and presented with signs of myelopathy including bilateral lower extremity leg weakness, numbness below the umbilicus, and worsening gait difficulty. This patient underwent thoracic laminectomy (C, D) without perioperative complications and was clinically improved postoperatively. Patient 2 had a history of prior anterior thoracolumbar spine surgery followed by 3 lumbar laminectomies and 1 thoracic laminectomy (prior to presentation to our center) with subsequent kinking of the spinal cord on MRI lumbar spine T2 sagittal image (E) and kyphotic deformity on preoperative scoliosis XR (F, H). She presented with progressive bilateral lower extremity weakness, gait instability, and bladder incontinence. This case was complicated by durotomy and left foot drop. Postoperative scoliosis XR at 9 months (G, I) demonstrate significant improvement in kyphotic deformity with clinical improvement in gait and leg strength with the exception of the left foot drop.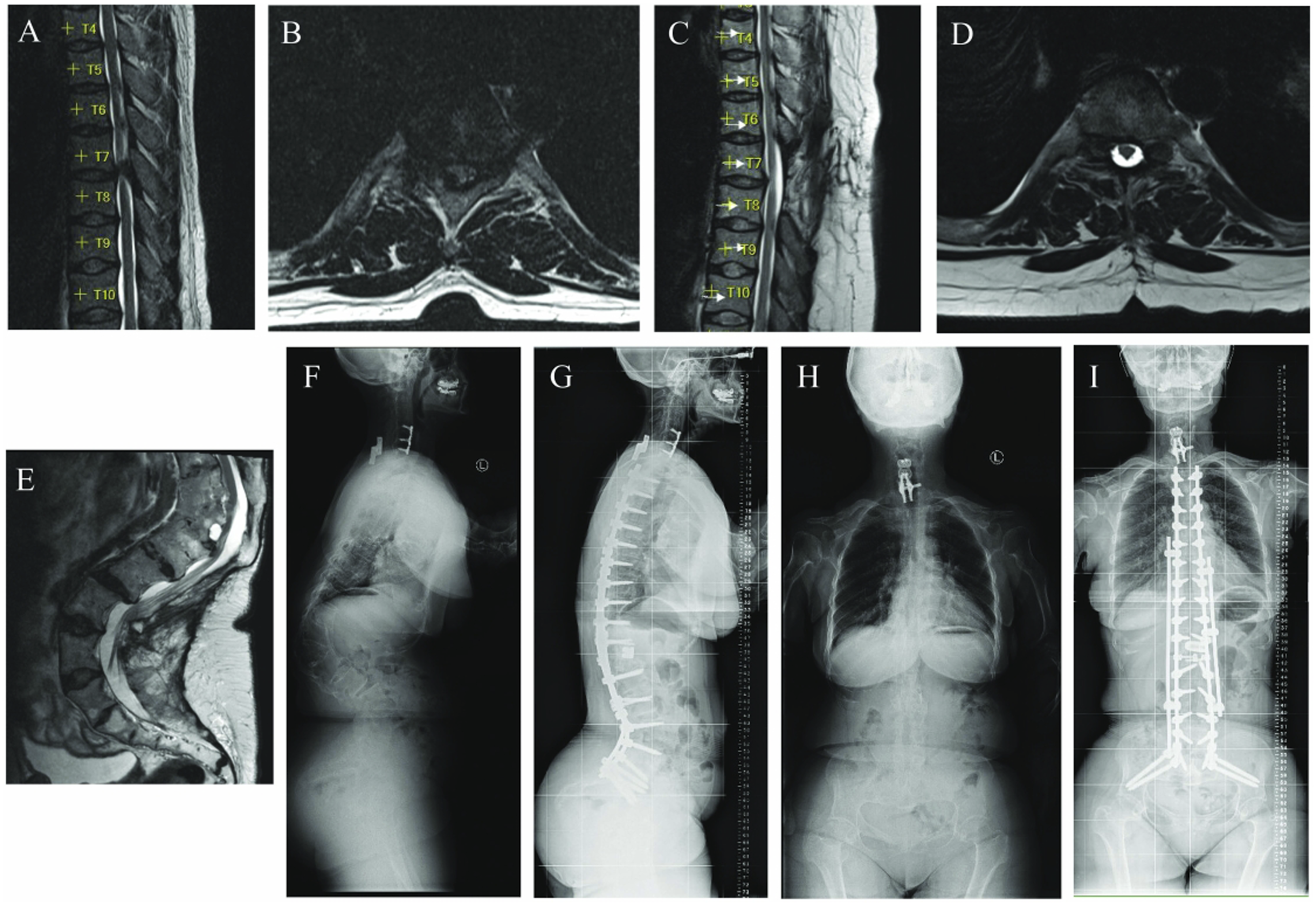
Discussion
This review of 95 consecutive spine cases in patients with achondroplasia demonstrated a 49.5% complication rate. Complications due to surgical intervention were associated with thoracolumbar surgery. Spine surgery performed chronologically later in this set of consecutive patients had decreased complications. These findings comprise the largest modern series to demonstrate a higher risk for perioperative complications following spine surgery in patients with achondroplasia.5,6,11
In a recent review by Nasser et al, 105 articles on spine surgery complications were evaluated, demonstrating complications rates ranging from less than 1% to as high as 70% in different surgical populations. 12 This high variability is likely due to differences in surgical indications, invasiveness of surgical approach, definition of complication, study design, and patient-related factors (such as achondroplasia) that affect outcome. While several studies have evaluated perioperative complications in various spine patient populations, there are only 2 known studies which have specifically evaluated spine surgery complications in patients with achondroplasia.
Complication Rates and Comparison to Prior Studies.
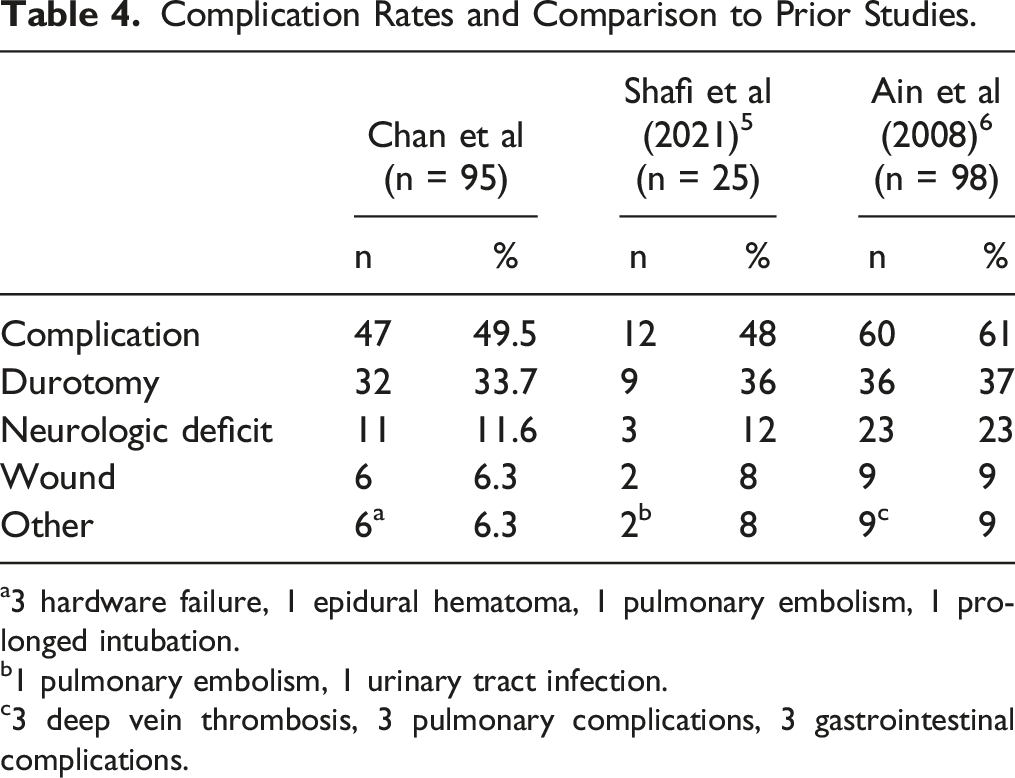
a3 hardware failure, 1 epidural hematoma, 1 pulmonary embolism, 1 prolonged intubation.
b1 pulmonary embolism, 1 urinary tract infection.
c3 deep vein thrombosis, 3 pulmonary complications, 3 gastrointestinal complications.
Studies specifically evaluating dural tears following spine surgery report 1.6-15.8% surgeries experience unintentional durotomy.13-17 Analysis of the Spine Patient Outcomes Research Trial (SPORT) demonstrated incidental durotomy in 3.1% of patients who underwent discectomy for disc herniation and found no differences in demographics including age, sex, race, and BMI. 15 In the current study we found that encounters with durotomy had increased association with male sex and decreased BMI. There has been no previously reported association between sex and complications and this may represent a limitation of our small cohort where 3 males patients each had 2 or 3 encounters with durotomy. Regarding BMI association with spine surgery complications, this finding was also not demonstrated in either of the studies by Ain et al or Shafi et al despite similar BMI means and ranges among the studies. A specific retrospective study evaluating BMI in achondroplasia patients following laminectomy also did not find BMI to be related to clinical outcomes. 18 This finding in our study may be explained by the unreliability of BMI in evaluating achondroplasia patients given their short stature, and thus tends to overestimate obesity and subsequent medical sequelae. 19
The thoracic spine was the most common spinal location for complication, specifically durotomy. While this was not specifically assessed in the studies by Ain et al and Shafi et al, it is reasonable that most complications are located in this region as a majority of all surgeries in this cohort involved the thoracic spine, similar to the other groups’ studies. Regarding the range of reported rates of dural tear in the literature, these findings may be related to the surgical cohort itself as Tafazal et al demonstrated an increase in dural tears in concordance with complexity of surgery. 16 Specifically, it was noted that dural tears occurred at a rate of 3.5% for discectomy alone, 8.5% for spinal stenosis decompression, and 13.2% for revision surgery. Despite stratification of the encounters by surgical complexity over time, these published rates of durotomy by Tafazal et al in the general population remain significantly lower than the 30% documented in our achondroplasia study and those by Ain et al and Shafi et al. This high rate of durotomy in achondroplasia patients likely suggests that spine surgeries in this patient population are of the highest complexity. It is likely that genetic alterations in this condition result in increased dural fragility and/or greater adhesiveness of the dura to the surrounding bony and ligamentous structures.
Much like that of complications related to dural tear incidence, neurologic deficit and wound infection following spine surgery in achondroplasia patients appears higher than that of the general population. A retrospective review of 917 spine surgery patients by Barbanti-Brodano documented neurologic complications occurring in 5.5% of the encounters and wound infections in 3.2%. These reported rates of complications are about half or less than those reported in this study and those by Ain et al and Shafi et al (Table 4) In addition, neurologic complications were closely related to increased age. This is consistent with literature in the general population which supports increased perioperative complications in older adults including durotomy, wound infection, and neurologic injuries. 20 The increased neurologic and wound complication rates in achondroplastic patients may be related to dural injury, and/or may be due to the unique anatomy of achondroplasia patients leading to kyphotic alignment and spinal stenosis.
Interestingly, unlike that of the general population, perioperative complications in patients with achondroplasia were not associated with prior surgical intervention at that same site in our study or that published by Ain et al. Prior studies encompassing general spine patient populations have demonstrated that repeat surgery is a risk factor for dural tears.14,21 Our series demonstrated that, over time, complications were decreased despite the patients being older and undergoing larger surgical interventions. In our small cohort at a single institution, some of the patients included underwent more than 1 surgical intervention in this study and also required longer constructs in the chronologically later interventions. The lack of significance in later surgeries leading to complications may be related to improved surgical technique as well as experience. Despite the limitations of our small cohort, this trend regarding decreased complications over time and experience is similar to findings by Barbanti-Brodano et al which demonstrated that the proportion of complications related to surgeries for elective degenerative spine conditions (as opposed to trauma or oncologic) also decreased over time from 23.1% to 6.4%. 22
Perioperative complications should be identified, particularly those which necessitate return to the operating room. In our study, 13 surgical encounters return to OR, the majority of which were related to unintended durotomy. Specifically, of the 13 encounters which required reoperation (27.7% of encounters with complications, 13/47), 1 each was due to seroma and epidural hematoma, 3 each to pseudomeningocele, wound dehiscence, and wound infection, and finally 2 due to hardware revision. Similar to that described by Ain et al, 6 our group found that primary repair with a combination of suture, fibrin glue, and synthetic dural applications are helpful in reducing persistent CSF leak. In addition to primary repair techniques and careful preoperative evaluation, the surgeon may consider use of tools such as ultrasonic instruments which may reduce risk of dural tear with ultrasonic technology, particularly in the setting of abnormal connective tissue. The potential advantages of these tools is supported by a recent study by Bydon et al which suggests that ultrasonic instruments may reduce the risk of durotomy, specifically in patients with achondroplasia. 23
While the current study validates prior literature suggesting achondroplasia patients are at greater risk for perioperative spine surgery complications, this current study has several limitations. The most notable of these is this is a retrospective review performed at a single institution. This study also has a small sample size and included multiple surgeons introducing high variation in operative techniques as well as heterogeneous procedural indications. Further studies should be performed to evaluate other risk factors for achondroplasia patients during spine surgery as well as investigate new technologies to decrease surgical complications in this unique patient population.
Conclusions
Adult patients with achondroplasia undergoing spinal surgery are at a higher risk for perioperative complications, particularly dural tears in the thoracolumbar spine. The potential for adverse events due to unique anatomy and connective tissue development should be considered when evaluating patients with achondroplasia for spine surgery. Given that patients chronologically later in the series had decreased adverse events, surgeon experience may be key to improving postoperative complications in patients with achondroplasia. As such, it is the authors’ opinion that achondroplasia patients being considered for spinal surgery should undergo significant preoperative evaluation and consideration to mitigate potential operative complications.
Footnotes
Acknowledgments
Margaret Hackett Family Center, Smidt Family Foundation and the Vera and Paul Guerin Family Chair in Pediatric Neurosurgery.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.