
Abstract
Study Design:
Cross-sectional observational study (consecutive case series).
Objectives:
The aim of this study was to define a criterion for achieving successful decompression of lumbar spinal stenosis (LSS) using intraoperative ultrasonography (IOUS) and to investigate the pathogenesis of redundant nerve roots (RNRs) based on the ultrasonographic findings.
Methods:
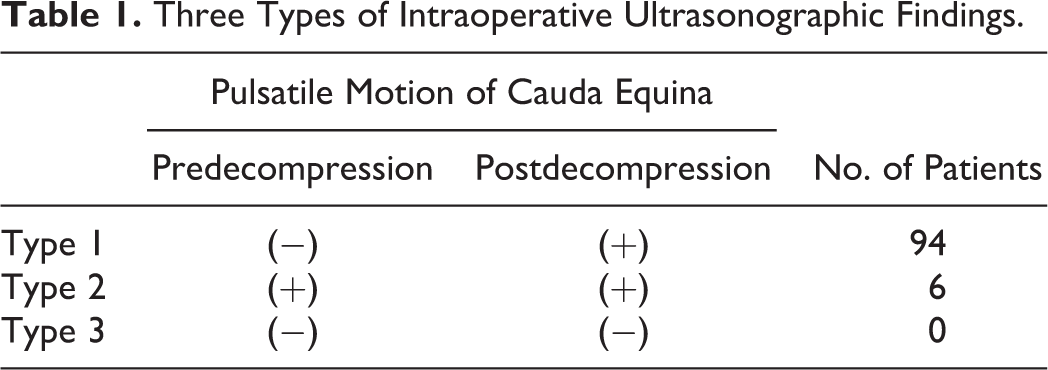
A total of 100 LSS patients (71 males, 29 females, mean age, 71 ± 8 years) with RNRs were enrolled as subjects in this study. IOUS was performed to evaluate pulsatile motion of the cauda equina (PMCE) just before and after decompressive laminectomy. To determine the decompression status of the cauda equina, the ultrasonographic findings were classified into 3 types on the basis of the presence or absence of PMCE: type 1, predecompression PMCE (−) to postdecompression PMCE (+); type 2, pre- and postdecompression PMCE (+); and type 3, pre- and postdecompression PMCE (−). The pathogenesis of RNRs was also investigated based on the ultrasonographic findings.
Results:
Around the stenosis, PMCE was almost always absent before decompression and appeared after decompression (type 1 in 94 patients, type 2 in 6, type 3 in 0). IOUS showed that, before decompression, the cauda equina was held at the stenosis and could not pulsate beyond the stenotic site, and after decompression, PMCE recovered in the craniocaudal direction, leading to the resolution of RNRs.
Conclusions:
The emergence of PMCE can be a sign of successful decompression for LSS. Ultrasonographic findings support the notion that disturbance of PMCE around the stenosis is a basic component of the pathogenesis of RNRs.
Keywords
Introduction
Lumbar spinal stenosis (LSS) is a degenerative spinal disease characterized by neurological intermittent claudication. Decompression of the neural structures by means of decompressive laminectomy has been generally accepted as the treatment for LSS patients with severe symptoms. 1 -4 However, a clear criterion that surgeons can use to be certain that they have achieved successful neural decompression during surgery has not been established.
Redundant nerve roots (RNRs) of the cauda equina are characterized by tortuosity of elongated and enlarged nerve roots in the subarachnoid space of the lumbar spine. Patients with RNRs tend to present with severe clinical symptoms. 5 -8 The incidence rate of RNRs apparent on magnetic resonance imaging (MRI) in patients with symptomatic LSS has been reported to be 33.8% to 42.3%. 7,9,10 Historically, RNRs were first observed by Verbiest 11 in 1954 and named by Cressmann and Paul 12 in 1968. Tsuji et al 13 reported RNRs in patients with LSS and pointed out a causal relationship between RNRs and the severity of LSS. Some assumptions concerning the pathogenesis of RNRs based on examinations by myelography, MRI, and histology have been discussed, 7,13,14 but no study based on the intraoperative findings has been attempted so far.
The recent development of high-resolution intraoperative ultrasonography (IOUS) allows real-time visualization of the spinal cord and cauda equina. 15 In the present study, this technique was used in patients LSS with RNRs, and cauda equina motion was monitored just before and after decompressive laminectomy. The primary goal of this study was to define a criterion for achieving successful decompression of LSS with RNRs and to elucidate the pathogenesis of RNRs based on the intraoperative ultrasonographic findings.
Materials and Methods
Subjects
The participants in this study were 131 patients who underwent decompressive laminectomy for LSS in Mitsui Memorial Hospital from 2014 to April 2017. All surgical procedures were performed by 2 board-certified spine surgeons (YK and AS). The protocol of this study was approved by the institutional review board of Mitsui Memorial Hospital. Inclusion criteria for the study were as follows: (1) history of intermittent claudication, (2) presence of central LSS, (3) preoperative lumbar MRI scans that demonstrated evidence of RNRs of the cauda equina adjacent to the level of spinal stenosis, and (4) absence of any appreciable instability of the lumbar spine to exclude candidates for fusion surgery (slip >3 mm in the neutral position, >2 mm translation, or >10° angulation on flexion and extension views were defined as instability). 16 Finally, 100 patients (71 males, 29 females, mean age, 71 ± 8 years, range 52-89 years) were enrolled in this study.
Radiologic Evaluation
Lumbar MRI scans were obtained preoperatively and 2 weeks after surgery in all patients. MRI was performed with a 1.5-T MR imager (GE Medical systems, Milwaukee, WI, USA) with a phased-array coil. T2-weighted, fast spin-echo sagittal MR images (repetition time = 4025 ms; echo time = 110 ms; slice thickness = 5.0 mm) and axial MR images (repetition time = 4500 ms; echo time = 102 ms; slice thickness = 5.0 mm) were examined. Two board-certified spine surgeons (YK and AS) evaluated the MR imaging studies blindly and independently to assess the reliability of the results. Each of the 2 surgeons has more than 20 years of clinical experience and is familiar with the interpretation of MR images. RNRs were recognized as tortuous, elongated, or coiled nerve roots in the subarachnoid space in patients with spinal stenosis. Qualitative signs of RNRs were observed as previously described by Min et al. 9 To evaluate the severity of spinal stenosis, preoperative MRI was assessed using a grading system (A-D) proposed by Schizas et al. 17
Surgical Procedure
Laminectomy was performed with the lumbar spinous process-splitting approach. 18 Patient were placed prone with the lumbar spine in a neutral position on the operating table. Through a midline skin incision, the tip of the spinous process was exposed. The spinous process was split longitudinally in the middle using a high-speed burr and a chisel. The structure was then divided at its base from the lamina, leaving the bilateral paraspinal muscles attached to the lateral aspect of the split spinous process. The muscles attached to the laminae were gently dissected using an elevator. Ample working space for laminectomy is obtained by retracting the split spinous process laterally together with its attached paraspinal muscles. The laminae were removed with a width of 5 mm on the center line using a high-speed burr. IOUS was performed using a water-path imaging technique to investigate the dynamics of the cauda equina with a digital echo camera (Prosound α10; Hitachi-Aloka Medical Co, Tokyo, Japan) and a 13-MHz linear array transducer. Cauda equina motion was videorecorded in a sagittal view around the narrowest lumbar level identified on preoperative MRI. The ultrasound transducer was directed perpendicular to the dura mater to obtain an accurate sagittal section and was stabilized for several seconds to prevent motion blur in the video. After achievement of complete laminectomy, the motion of the decompressed cauda equina was again video-recorded around the narrowest level using IOUS.
Ultrasonographic Evaluation
Based on the ultrasonographic findings at the caudal side of the stenosis, cauda equina motion was stratified into one of the following 3 types: type 1, predecompression no pulsatile motion in a craniocaudal direction to postdecompression pulsatile motion in a craniocaudal direction (+); type 2, predecompression pulsatile motion (+) to postdecompression no change; and type 3, predecompression no pulsatile motion in a craniocaudal direction to postdecompression no change.
Clinical Evaluation
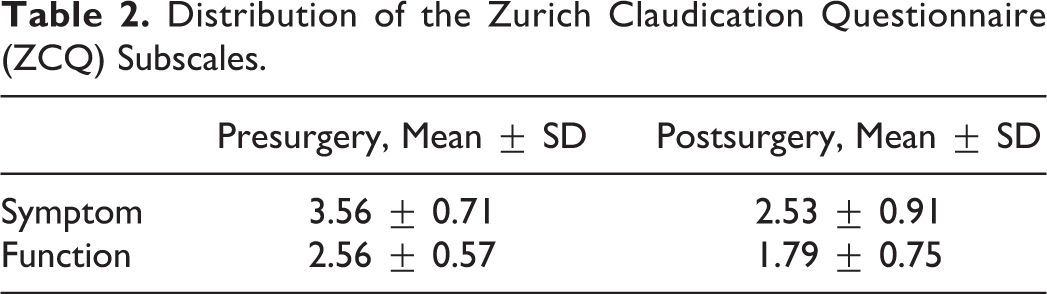
Presence or absence of intermittent claudication was assessed 3 months after surgery in all patients. The symptom domain and the function domain of the Zurich Claudication Questionnaire (ZCQ) were also evaluated preoperatively and 1 year postoperatively. The subjects were 74 patients (53 males, 21 females, mean age, 71 ± 8 years) in this study, excluding those who did not have the ZCQ data.
Statistical Analysis
Statistical analyses were performed using SPSS for Windows version 17.0 (SPSS, Chicago, IL, USA). The symptom domain and the function domain of ZCQ were compared before surgery and 1 year after surgery using the Friedman test. If a significant difference was noted, the data was then compared using the Wilcoxon signed rank test. The level of significance was set at P < .05.
Results
Surgical time was 208 ± 70 minutes (range, 78-467 minutes), and blood loss was 144 ± 133 mL (range, 6-608 mL). The number of decompressed interlaminar levels was 2 ± 1 (range, 1-5). Preoperative MRI stenosis grades proposed by Schizas et al 17 were grade D stenosis in 55 patients, grade C in 45, grade B in 0, and grade A in 0; thus, severe stenosis was common. Figure 1 shows the cauda equina in LSS with RNRs observed by IOUS. Before decompression, ultrasonography showed pulsatile motion of the cauda equina in a craniocaudal direction at the cranial side of the stenosis, with no motion at the caudal side of the stenosis (Figures 1 and 2). After successful decompressive laminectomy, pulsatile motion was observed around the stenosis. IOUS showed type 1 findings in 94 patients, type 2 in 6, and type 3 in 0 (Table 1). Overall, 84 of the 100 patients showed no evidence of RNRs (ie, indicating resolution) on MRI 2 weeks after surgery. Sufficient decompression was obtained in all patients on postoperative MRI. In all patients, intermittent claudication disappeared after decompression surgery. The ZCQ scores before and after surgery are summarized in Table 2. The symptom domain and the function domain of the ZCQ were significantly better 1 year after surgery than before surgery (P = .001).
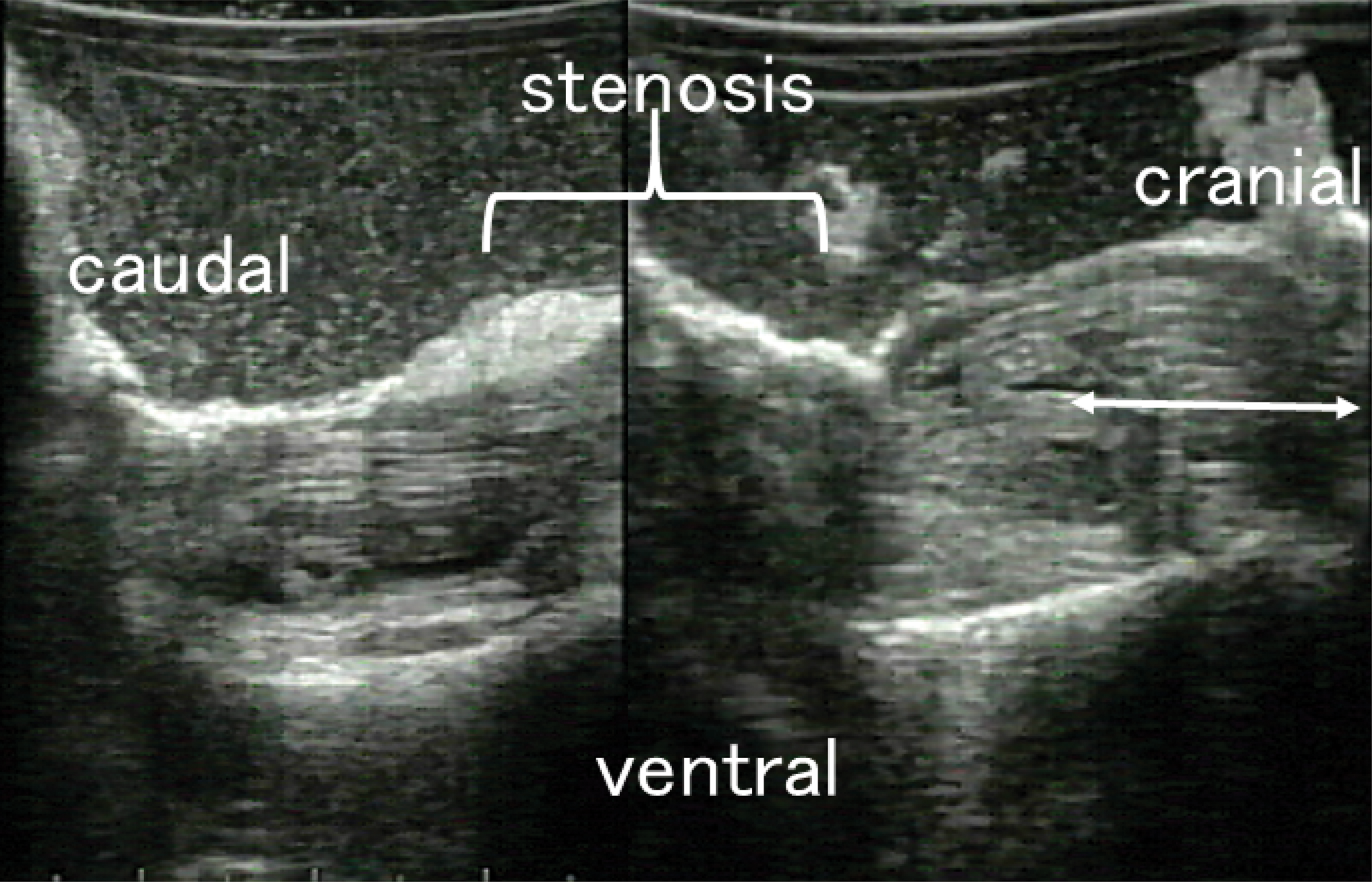
An intraoperative ultrasonographic image in a patient with lumbar spinal stenosis with redundant nerve roots before decompression. Pulsatile motion of the cauda equina in a craniocaudal direction (arrow) is observed at the cranial side of the stenosis, while no motion is observed at the caudal side of the stenosis.
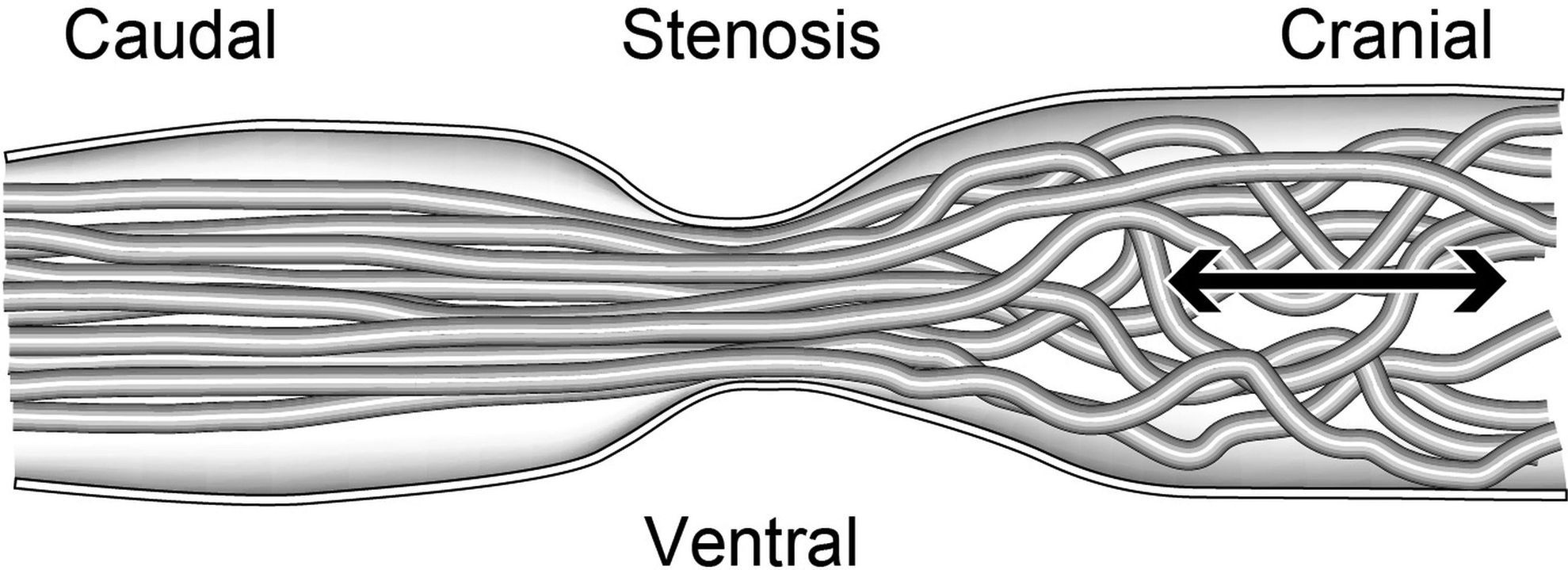
Schematic illustration of intraoperative ultrasonography in lumbar spinal stenosis with redundant nerve roots before decompression. Pulsatile motion of the cauda equina in a craniocaudal direction (the arrow) is observed at the cranial side of the stenosis, while no motion is observed at the caudal side of the stenosis.
Three Types of Intraoperative Ultrasonographic Findings.
Distribution of the Zurich Claudication Questionnaire (ZCQ) Subscales.
Discussion
At the stenosis, IOUS showed that pulsatile motion of the cauda equina was almost always not observed before decompressive laminectomy and appeared after complete decompression. This result strongly supports the use of emergence of pulsatile motion of the cauda equina (cauda equina activation sign) as a sign of successful decompression of the cauda equina with RNRs; no recovery of pulsation can suggest insufficient decompression, including wrong-level surgery. This is the first report to propose a clear criterion on intraoperative ultrasonographic findings to confirm achievement of successful decompression of LSS with RNRs. Cauda equina activation sign can be useful for making the final judgement of successful decompression in patients with multilevel stenosis during surgery. While it is a little difficult to use IOUS before decompression in usual clinical situation because limited laminectomy such as performed in this study is needed, it is very easy to use IOUS after decompression. These properties of IOUS and our IOUS findings suggest the clinical utility of monitoring cauda equina motion by ultrasonography after decompression. We propose “cauda equina activation sign” be used especially after decompression to confirm successful decompression intraoperatively.
Preoperative MRI findings in this study were grade C or grade D, which indicates that RNRs are a sign of severe stenosis in LSS, as previously reported. 19 Pulsatile motion of the cauda equina was clearly seen before complete decompression in the 6 patients with type 2. Minimal laminectomy with a width of 5 mm might result in decompression sufficient enough to allow pulsation of the cauda equina in these patients.
The pathogenesis of RNRs has been attributed to a squeezing force from the constricted spinal canal acting on the nerve roots. 7 The constriction of the dural tube at the stenotic site in LSS patients causes mechanical entrapment of nerve roots, restricting their normal mobility in the craniocaudal direction. A cranially placed cauda equina cannot return to the caudal side of the stenosis if the stenosis is severe. Subsequently, this produces elongation and eventual coiling of the nerve roots proximal to the blockage. The squeezing force has been thought to be generated by repeated lumbar movements. 7 IOUS showed additional findings: before decompression, the nerve fibers were held at the stenosis and could not pulsate through the stenotic site; and after decompression, the nerve fibers pulsated and moved in the craniocaudal direction smoothly. These findings give rise to the view that not only the repeated lumbar movements but also pulsatile motion of the cauda equina is a basic component of the pathogenesis of RNRs. In addition, although there have been a few reports of RNRs at the caudal side of the stenosis, 20 most RNRs occur at the cranial side of the stenosis. In fact, all patients in this study showed RNRs at the cranial side of the stenosis. This may be because the pulling force produced by pulsatile motion of the cauda equina brings nerve fibers to the cranial side of the stenosis.
RNRs still remained in 16 patients on postoperative MRI, which is consistent with the results of another study. 21 The findings about postoperative remaining RNRs on MRI were that not only in the cranial side but also in the stenotic site and the caudal site, the nerve roots were redundant after decompression. These changes may have occurred by the recovery of pulsatile motion of cauda equina through the stenotic site, although the reason why these patients could not obtain complete RNRs resolution is still unknown.
In the present study, intermittent claudication disappeared after surgery. The degree of improvement in the symptom domain and the function domain of the ZCQ after surgery was comparable to that in a previous report. 22
The limitation of the present study is that IOUS cannot show pulsatile motion of the cauda equina without laminectomy, so that pulsatile motion of the cauda equina in the healthy person without stenosis could not be analyzed, although pulsatile motion of the cauda equina was observed and did not change before and after decompressive laminectomy in LSS patients with foraminal stenosis and without central canal stenosis (n = 7, 4 males, 3 females, mean age, 72 ± 5 years, range 65-76 years). Other limitations of this study include the analysis of retrospective data, as well as restrictions imposed by the small sample size from a single hospital.
Conclusions
The emergence of pulsatile motion of cauda equina (cauda equina activation sign) can be a sign of successful decompression during posterior decompression of LSS with RNRs. Pulsatile motion of the cauda equina is a basic component of the pathogenesis of RNRs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.