
Abstract
We report a rare case of extraneural metastasis of spinal ependymoma that developed over a very long period. A 28-year-old man underwent surgery for ependymoma in the cauda equina. After he experienced three local recurrences and had undergone five operations, a lung metastasis occurred 46 years after the first operation. Although the tumor did not show the typical morphological malignancy, the maximum standard uptake value obtained by positron-emission tomography and the antigen Ki-67 labeling index demonstrated the tumor's active proliferative ability. One year after the last operation, the patient died of respiratory failure due to progressing lung metastases. The malignant behavior of spinal ependymomas is demonstrated in a case with long-term follow-up.
Ependymal tumors are neoplasms that arise from the ependymal lining of the cerebral ventricles and the central canal of the spinal cord or from ependymal cell clusters in the terminal filum. Most spinal ependymomas are myxopapillary ependymomas or ependymomas that are regarded as histopathologically benign tumors. However, the malignant behaviors of spinal ependymomas become apparent with increased survival time. We present here the case of a man with an ependymoma of the cauda equina who went on to have metastases to the lungs after a very long survival period.
Case Report
History and Examination
A 28-year-old Asian man who reported low back pain underwent resection of a tumor of the cauda equina at the L4–5 level in 1963 (his first surgery). The pathological diagnosis was ependymoma. He remained free of symptoms for 20 years. At age 48 years in 1984, he underwent resection for recurrence of the tumor in the retroperitoneal space (his second surgery). He had no signs of recurrence for 13 years. Then at age 61 years, he had low back pain due to tumor recurrence. He underwent tumor resection, done using an anteroposterior approach (his third surgery); however, the resection was incomplete. At the age of 62 in 1998, he underwent total resection, attempted from a posterior approach (his fourth surgery) with arterial embolization. After the surgery, the patient underwent radiation therapy (45 Gy). His right leg was paralyzed as a complication of arterial embolization. The patient then remained free of symptoms for 10 years.
At the age of 73 in 2009, he was referred to our hospital for the first time, with moderate low back pain and intolerable left leg pain that had continued for 1 year. He was nonambulatory because of loss of muscle and leg pain and had normal function of bladder and bowel. His neurological symptom suggested he suffered from left L5 radiculopathy. Plain radiographs and computed tomography showed scalloping of the lumbar spine with marginal sclerosis (Fig. 1A). Magnetic resonance imaging revealed severe canal stenosis at the L4–5 level due to tumor expansion (Figs. 1B, C). Preoperative plain chest radiographs depicted a coin-size lesion on his right lung, showing metastases of the tumors (Fig. 2). Findings for various tumor makers were negative. A whole-body computed tomography scan detected no primary tumor other than one in the lumbar spine. We identified these lesions as metastases of ependymoma. Because the patient's leg pain could not be controlled even with narcotic analgesics, we performed palliative decompression surgery.
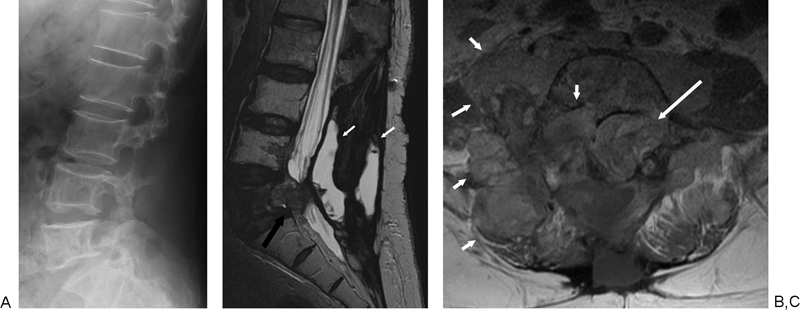
(A) Lateral radiographs of the lumbar spine showing scalloped vertebrae. (B) Sagittal T2-weighted magnetic resonance image showing the high signal intensity of cystic fluid in paravertebral muscle (small white arrow) and the low intensity of the tumor mass (large black arrow). The L5 vertebra was invaded by the tumor. (C) Axial T1-weighted contrast-enhanced image showing the isometric to high intensity of multiple tumors (arrows).
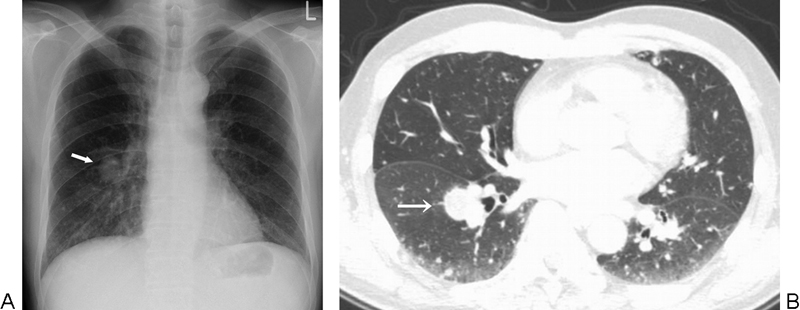
Preoperative anteroposterior chest radiograph showing a coin-size lesion in the right lung field (arrow).
Surgical Procedure
The posterior approach was used. During surgery, the cysts in the paravertebral muscle were found to be suffused with serous liquid and were resected in a piecemeal fashion. After exposing the left facet at L4–5, the residual left inferior articular process of L4 was resected. We curetted the tumors behind the dura mater with the use of a Cavitron Ultrasonic Surgical Aspirator (Cooper Medical, Santa Clara, CA) and identified the L5 nerve root. A soft brown tumor in the extradural space had compressed the L5 nerve root from the ventral side. An intralesional excision of the tumor was performed without adhesion.
Pathological Findings
Tissue sections obtained before 1984 were not acquired for review. The tumor resected in 1998 had proliferation of round cells, forming a perivascular pseudorosette (Fig. 3A). Most of the tumor resected in 2009 had a morphologically identical pattern to that of the 1998 specimen. However, the pseudorosette pattern was more irregular in the 2009 tumor (Fig. 3B). Immunohistochemistry produced positive findings for glial fibrillary acid protein (Fig. 3C) and negative findings for epithelial membrane antigen. The histological and immunohistochemical findings led to the diagnosis of recurrent ependymoma. The Ki-67 labeling index for the 2009 tumor and the 1998 tumor was ∼3% (Fig. 3D). However, there was a limited area in the 2009 tumor with higher cell density than other areas. Some cellular pleomorphism, necrosis, and mitosis was present (Fig. 3E), and the Ki-67 labeling index of the area was >15% (Fig. 3F).
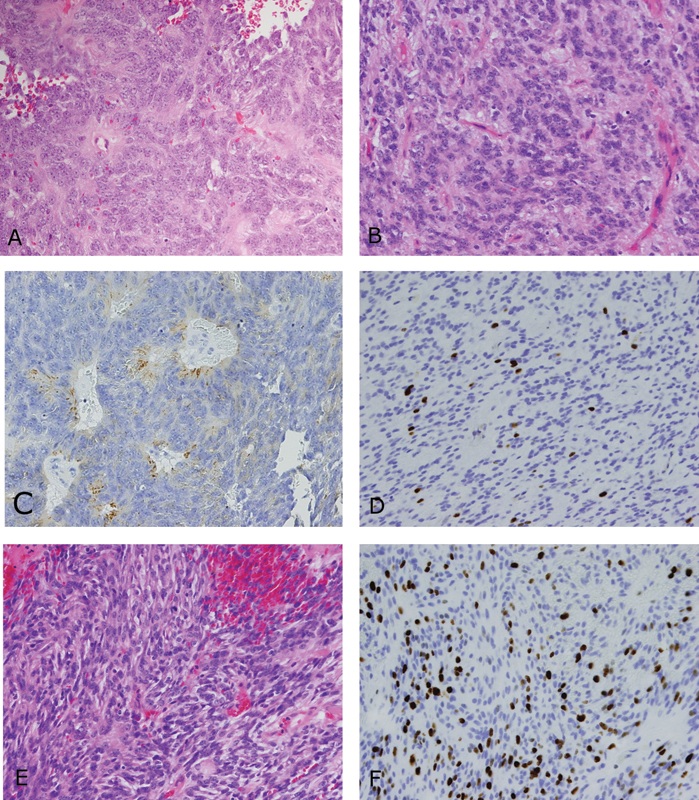
Photomicrographs of specimens. (A) Hematoxylin and eosin (HE) staining of a 1998 specimen showing perivascular pseudorosette patterns (original magnification ×200). (B) HE staining of a 2009 specimen showing irregular perivascular pseudorosette patterns (original magnification ×200). (C) Immunohistochemical image of a 2009 specimen showing tumor cells with positive findings for glial fibrillary acid protein (original magnification ×100). (D) Immunohistochemical image of a 2009 specimen showing a 3% Ki-67 labeling index. (E) HE staining of part of a 2009 specimen showing higher cell density and no perivascular pseudorosette pattern (original magnification ×200). (F) Immunohistochemical image of the high-cell-density area showing a 15% Ki-67 labeling index.
Postoperative Course
After surgery, muscle weakness and pain due to L5 radiculopathy was improved. Although low back pain remained, he became ambulatory with a cane. There were no complications from the surgery. One month after surgery, fluorodeoxyglucose positron-emission tomography was performed for general examination. Pathological uptake was recognizable in the lumbar spine, a lung nodule, the ilium, and abdominal lymph nodes. The maximum standard uptake value (SUVmax) was 7.4 in the lumbar spine, 5.2 in a lung nodule, 4.0 in the ilium, and 3.8 in abdominal lymph nodes (Fig. 4). Six months after surgery, there was extensive pulmonary metastasis (Fig. 5) and bilateral leg swelling. Abdominal computed tomography revealed that the bilateral common iliac vein was occluded by deep vein thrombosis or tumor embolism. Although an inferior vena cava filter was placed to prevent pulmonary embolism, the patient was bedridden with deep vein thrombosis. One year after surgery, the patient died of respiratory failure at the age of 74, 46 years after the first surgery. Permission to perform an autopsy was denied by the patient's family for religious reasons.

Coronal positron-emission tomography image showing increased accumulation of fluorodeoxyglucose in the lung nodule and the lumbar spine (arrow).

Chest radiograph obtained 6 months after surgery showing multiple grown tumor nodules in both lungs.
Discussion
Metastases of intradural ependymomas to other organs are rare events. To the best of our knowledge, only 10 cases of intradural ependymomas metastasizing outside the central nervous system (CNS) have been reported since 1955 (Table 1). 1 , 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9 , 10
Studies Reporting Metastases of Ependymomas Outside the Central Nervous System
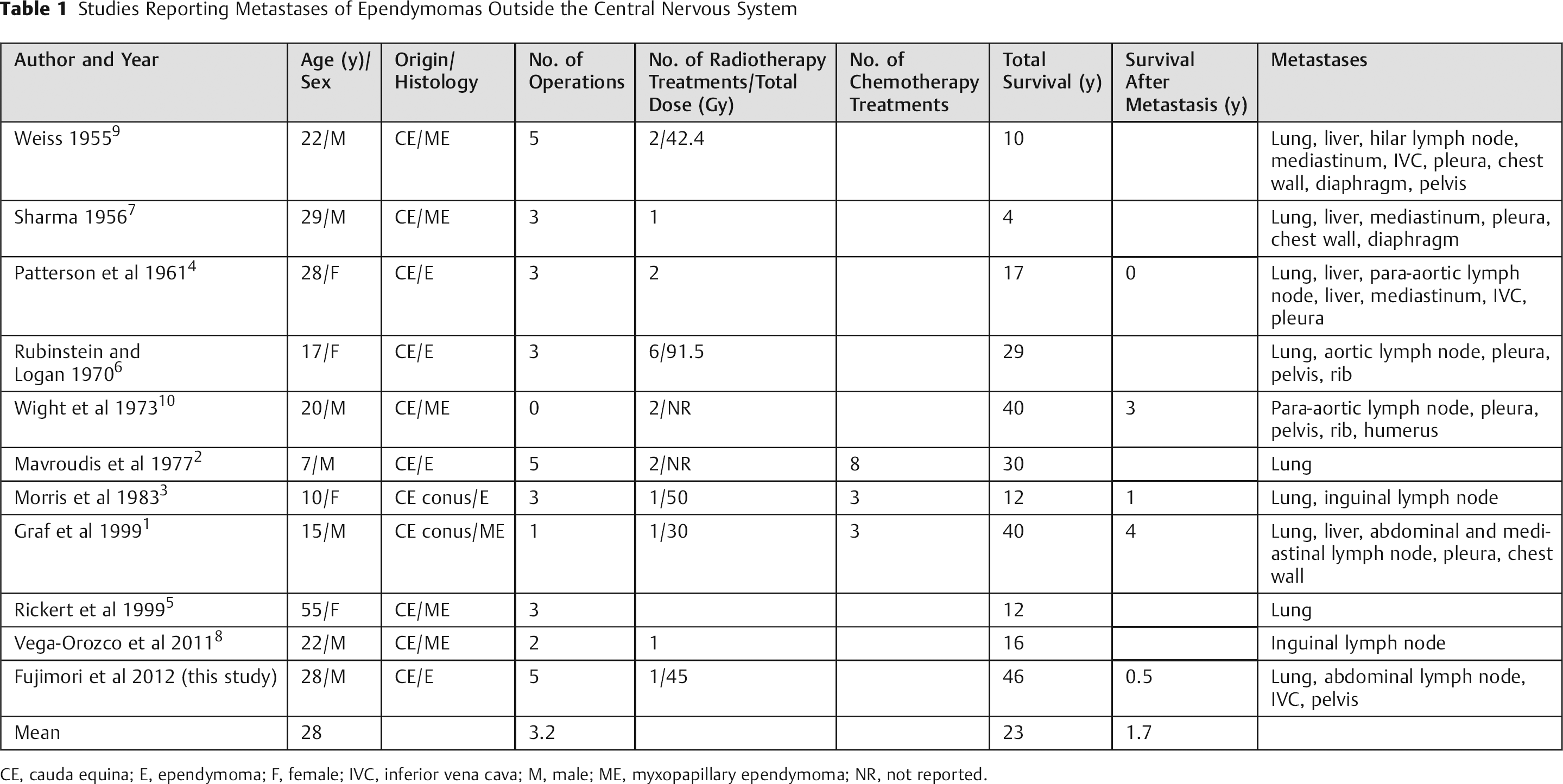
CE, cauda equina; E, ependymoma; F, female; IVC, inferior vena cava; M, male; ME, myxopapillary ependymoma; NR, not reported.
The common characteristics in cases of metastases are young age at onset, a long survival period, and multiple operations. 1 , 2 , 3 , 6 Interestingly, in all 11 cases, the tumors originated in the cauda equina; there were no cases of intramedullary ependymoma with metastasis to other organs. It was speculated that the reason for this was either that patients with intramedullary ependymomas have a short survival period or that multiple reoperations are difficult at this level. Mork and Loken reported that the 10-year survival rate for patients with ependymoma of the cauda equina was 94%, whereas the rate for patients with intramedullary ependymoma was only 55%. 11 However, once the metastasis appeared, the prognosis for ependymoma of the cauda equina was very poor and therapeutic options were limited. The mean survival for five patients after metastasis was only 1.7 years (Table 1). Additionally, aggressive local invasion occurred at the time that the metastasis was noted. 1 , 2 , 3 However, pathologically, few studies found cellular pleomorphism or mitosis, even after metastasis occurred. The relationship between histological type and metastatic potential has not been determined. 1 , 9 , 10 In the same way, the most recent tumor in our patient also did not have a typical malignant morphology, such as mitosis or necrosis. However, some of our findings suggested a strong cell proliferative ability. A portion of our patient's tumor had a high Ki-67 labeling index of 15%. Suri et al reported that the Ki-67 labeling index of CNS tumors was 0 to 2.4% for grade 1, 1.5 to 3.6% for grade 2, and 9.5 to 34% for grade 3. 12 , 13 , 14 , 15 , 16 In a case of metastatic myxopapillary ependymoma, Rickert et al reported that the Ki-67 labeling index was 3.1% for the initial tumor and 14.2% for the recurrent tumor. 5 These findings suggest the possibility of anaplastic-like change in recurrent ependymal tumors. Findings on positron-emission tomography also suggested a high activity level in our patient's tumor. Even considering surgical invasion, the SUVmax of 7.4 for the lumbar spine and 5.2 for lung metastases in our patient was comparatively high. 17 Kosaka et al reported that the mean SUVmax of malignant gliomas (grade 3 or 4) is 11.6 ± 3.7 and of metastatic brain tumors is 7.8 ± 2.7. 18 Wilmshurst et al reported that the SUVmax of low-grade spinal cord tumors (grade 1 or 2) ranges from 1.0 to 5.2. 19
The most likely pathway of extraneural metastasis of ependymal tumors is thought to be the bloodstream and/or the lymphatic system. 1 , 2 , 3 , 6 , 10 It has been proven that some kinds of glioma can spread outside the CNS through the venous system, invading the intact intracerebral blood-vessel lumina. 20 However, in all reported cases of metastatic ependymomas there was a history of previous operations; the surgical manipulation itself had the possibility to produce distant metastases. In this sense, the characteristics of recurrent ependymomas in the extradural space rather resemble those of primary extradural ependymomas. It has been reported that patients with extradural ependymomas have a poor prognosis because they are at high risk for tumor metastasis to other organs instead of dissemination within the CNS. 21 , 22 , 23 , 24 , 25 , 26
Because of the rarity of ependymomas, there have been no randomized, controlled studies of the effectiveness of adjuvant therapies in recurrence or metastasis of ependymomas. 27 Most reports have supported some efficacy of radiation in preventing recurrence. 28 , 29 , 30 , 31 Except in myxopapillary ependymomas in which total resection is confirmed by magnetic resonance imaging, the benefit of postoperative radiation outweighs the risk of adverse effects. 1 However, the effectiveness of chemotherapy is less clear. Although several protocols have been attempted, few reports have shown that they are effective. 1 , 2 , 3 , 25 , 32 , 33 Thus, there are few therapeutic options for metastasis.
Although most spinal ependymomas correspond to grade 1 or grade 2 tumors, the clinical course is not always good. Armstrong et al reported that nearly 40% of patients were unable to work from the time of diagnosis and had significant symptoms, such as pain, weakness, cognitive changes, and sexual dysfunction. 34 Nakamura et al advocated treating spinal ependymomas as clinically malignant tumors. 30 Local recurrence, CNS dissemination, and even metastasis can occur in the long term. Careful operation and long-term follow-up is recommended for patients with spinal ependymomas.
Disclosures
Takahito Fujimori, Research Support: AO spine research grant; a grant-in-aid for Scientific Research C (KAKENHI: 22591632) from the Ministry of Education, Culture, Sports and Technology, Japan
Motoki Iwasaki, Research Support: AO spine research grant; a grant-in-aid for Scientific Research C (KAKENHI: 22591632) from the Ministry of Education, Culture, Sports and Technology, Japan
Yukitaka Nagamoto, Research Support: AO spine research grant; a grant-in-aid for Scientific Research C (KAKENHI: 22591632) from the Ministry of Education, Culture, Sports and Technology, Japan
Masafumi Kashii, Research Support: AO spine research grant; a grant-in-aid for Scientific Research C (KAKENHI: 22591632) from the Ministry of Education, Culture, Sports and Technology, Japan
Hironobu Sakaura, Research Support: AO spine research grant; a grant-in-aid for Scientific Research C (KAKENHI: 22591632) from the Ministry of Education, Culture, Sports and Technology, Japan
Hideki Yoshikawa, Research Support: AO spine research grant; a grant-in-aid for Scientific Research C (KAKENHI: 22591632) from the Ministry of Education, Culture, Sports and Technology, Japan
Footnotes
Acknowledgments
The authors thank Tadashi Watabe, radiologist, for measuring SUVmax and Hideyuki Arita, neurosurgeon, and Hirostugu Oshima, pathologist, for advice on pathology findings. Katharine O'Moore-Klopf, ELS (East Setauket, NY), provided professional English-language editing of this article.