
Abstract
Study Design:
Systematic review.
Introduction:
Amyotrophic lateral sclerosis (ALS) is a progressive neurodegenerative disease, ultimately resulting in paralysis and death. The condition is considered to be caused by a complex interaction between environmental and genetic factors. Although vast genetic research has deciphered many of the molecular factors in ALS pathogenesis, the environmental factors have remained largely unknown. Recent evidence suggests that participation in certain types of sporting activities are associated with increased risk for ALS.
Objective:
To test the hypothesis that competitive sports at the highest level that involve repetitive concussive head and cervical spinal trauma result in an increased risk of ALS compared with the general population or nonsport controls.
Methods:
Electronic databases from inception to November 22, 2017 and reference lists of key articles were searched to identify studies meeting inclusion criteria.
Results:
Sixteen studies met the inclusion criteria. Sports assessed (professional or nonprofessional) included soccer (n = 5), American football (n = 2), basketball (n = 1), cycling (n = 1), marathon or triathlon (n = 1), skating (n = 1), and general sports not specified (n = 11). Soccer and American football were considered sports involving repetitive concussive head and cervical spinal trauma. Professional sports prone to repetitive concussive head and cervical spinal trauma were associated with substantially greater effects (pooled rate ratio [RR] 8.52, 95% CI 5.18-14.0) compared with (a) nonprofessional sports prone to repetitive concussive head and cervical spinal trauma (pooled RR 0.60, 95% CI 0.12-3.06); (b) professional sports not prone to repetitive head and neck trauma (pooled RR 1.35, 95% CI 0.67-2.71); or (c) nonprofessional sports not prone to repetitive concussive head and cervical spinal trauma (pooled RR 1.17, 95% CI 0.79-1.71).
Conclusions:
Our review suggests that increased susceptibility to ALS is significantly and independently associated with 2 factors: professional sports and sports prone to repetitive concussive head and cervical spinal trauma. Their combination resulted in an additive effect, further increasing this association to ALS.
Keywords
Introduction
Amyotrophic lateral sclerosis (ALS, also known as “Lou Gehrig disease”) is a progressive neurodegenerative disease, considered to be caused by a complex interaction between environmental and genetic factors. 1 The pathological hallmark consists of progressive neurodegeneration of upper and lower motor neurons, ultimately leading to paralysis and death. As a clinical entity, ALS has remained primarily associated with the field of neurology, however spine surgeons may also encounter these patients given that early clinical presentations can mimic a number of spinal disorders, especially such that present as weakness in presence of a compressive cervical spondylosis. The incidence of ALS in Western countries is estimated to be between 1 and 3 per 100 000 per year per person-years. 2 About 90% of cases are sporadic with negative family history whereas in the remaining 10% are familial. 3 Advanced genetic technologies in recent years has led to the identification of around 25 ALS-related genes 4,5 and to the generation of ALS-specific animal models, mimicking the human condition. 6,7 Nonetheless, a unified pathogenic mechanism that would adjoin all known clinical and genetic findings is still lacking. There is also evidence that environmental factors play a role in the pathogenesis of sporadic ALS and may trigger the onset of disease for those with known genetic mutations. Indeed, various exposures that have been linked with ALS include smoking, 8 heavy metals, 9 and pesticides. 10 Of note, a recent growing body of evidence also supports a role for increased physical activity 11,12 and musculoskeletal trauma. 13 Interestingly, various sports such as American football 14 and soccer 15 have also been shown to carry an increased risk of developing ALS, further strengthening a possible mechanical etiology. These contact sports, which in the most advanced competitive implementations combine both vigorous physical activity and carry the risk of potential repetitive head and cervical spine trauma with the resultant risk in the form of traumatic brain injury in varying degrees of severity. Yet analysis of how the level of competitiveness (professional vs nonprofessional) or the type of sport (contact vs noncontact) affect this risk remains unanswered. We hypothesized that not all sports, but only those at the highest competitive levels that involved repetitive head and cervical spine trauma result in an increased risk of ALS compared with the general population or nonsport controls. To test this hypothesis, our systematic review sought to answer the following key questions (KQ).
Clinical Questions
KQ 1: Is there an increased risk of ALS or mortality associated with ALS among those who play organized competitive sports? KQ 2: Does the risk vary by higher levels of competitive play (professional vs nonprofessional)? KQ 3: Does the risk vary by whether the sport is prone to repetitive concussive head and cervical spinal trauma? KQ 4: Within different levels of competitive play, does the risk vary by whether the sport is prone to repetitive concussive head and cervical spinal trauma?
Materials and Methods
Study Design
Systematic review.
Information Sources
PubMed, Cochrane Database of Systematic Reviews, and Cochrane Central Register of Controlled Trials (CENTRAL) from inception to November 22, 2017; Google Scholar and bibliographies of included articles and systematic reviews.
Eligibility Criteria
The inclusion criteria were (a) adults ≥16 years with a history of playing competitive organized sports, (b) comparison of a nonsport control or standardized reference group, and (c) comparative cohort and case-control study designs. The exclusion criteria were (a) youth sports under the age of 16 years; (b) strenuous noncompetitive sport activity, military activity, nonsport trauma; (c) crude (nonstandardized) population reference group; (d) other neurologic disorders as outcomes; and (e) studies not producing an effect measure (odds ratio, rate ratio, standardized ratio, etc), cross-sectional studies, reviews, or case reports.
Outcomes
Incidence of ALS or mortality associated with ALS.
Exposures
Any organized competitive sport either professional or nonprofessional. We defined the following sports a priori as those deemed to expose players to repetitive concussive head and cervical spinal trauma: American football, soccer, hockey, boxing, rugby.
Controls
Controls consisted of the general population or individuals with no history of engaging in organized competitive sports.
Data Collection Items and Process
Data was extracted by a single individual and verified independently by a second investigator. Two individuals independently evaluated the risk of bias and disagreements were resolved through discussion.
Risk of Bias
Risk of bias (RoB) was assessed against preset criteria for prognostic studies. From the RoB, study class of evidence (CoE) was derived. RoB criteria and CoE assessment for each included article can be found in the supplemental material.
Analysis
Several types of measurements enable the assessment of how a certain exposure (in our study contact sports) may be associated with a certain disease (ALS). “Mortality ratio” and “incidence ratio” are the observed number of deaths or patients with a disease in the exposed group, respectively, divided by that in the unexposed group. An assessment of this association over a period of time is termed “Hazard ratio.” Another way of estimating risk is calculating “odds ratio” in which an exposure is associated with a known health outcome (ALS) and is usually performed in case-control studies. Proportional mortality ratio (PMR) calculates the ratio of a specific-cause mortality to the overall mortality. Standardized mortality or incidence ratios, hazard ratios, odds ratios, proportional mortality ratios, and rate ratios were treated as equivalent measures of risk and referred to as the rate ratio (RR). Each of these measures compare the occurrence of ALS in the exposed versus control populations. After undergoing a logarithmic transformation, studies were pooled and weighted according to the reciprocal of their variances (calculated as the square of their standard error, which if not available, was sourced from reported confidence intervals). Results were then transformed back to their original units and presented with 95% confidence intervals along with P values derived from t tests. A random effects model was assumed to address heterogeneity. I2 statistics were calculated with the null hypothesis that there were no differences in the effect sizes across studies and that chi-square distribution was followed. Effect estimates were stratified in order to analyze different patient population characteristics. The same methods used to pool and test at the study level further extend to pool and test at the subgroup level. A sensitivity analysis consisted of removing any study with a high risk of bias, class of evidence IV. All meta-analysis calculations and plots were done using Cochrane’s Revman v.5.3.
Results
Study Selection
Sixteen studies met the inclusion criteria, 12 assessing the incidence of ALS 16 -27 and 4 the mortality associated with ALS 14,28 -30 (Table 1). Three studies were judged to have moderately low risk of bias, CoE II 14,28,29 ; 8 moderately high risk of bias, 16,17,19,21,22,25,26,30 CoE III; and 5 high risk of bias, 18,20,23,24,27 CoE IV. Four studies evaluated professional soccer, 16,17,28,29 1 professional American football, 14 1 professional basketball, 17 1 professional cycling, 17 3 professional general sports (not specified), 21,22,30 1 nonprofessional soccer, 26 2 nonprofessional American football, 20,23 1 nonprofessional marathon or triathlon, 19 1 nonprofessional skating, 19 and 8 nonprofessional general sports (not specified). 16,18,21,22,24 -27 Figure 1 shows the inclusion/exclusion of articles from the search. CoE rating and a list of excluded articles can be found in the supplemental material.
Flow diagram showing results of literature search and study selection.
Characteristics of Included Studies Assessing Risk of Amyotrophic Lateral Sclerosis (ALS) in Athletes.
Abbreviations: ALS, amyotrophic lateral sclerosis; BMI, body mass index; CoE, class of evidence; COI, conflict of interest; EMG, electromyogram; MND, motor neuron disease; NFL, National Football League; NR, not reported.
Is there an increased risk of ALS or mortality associated with ALS among those who play organized competitive sports?
Organized competitive sports was associated with an increased risk of ALS compared with controls (24 comparisons from 16 studies,
14,16
-30
pooled RR 1.80, 95% CI 1.13-2.88, I2 = 83%) (Figure 2). Substantial heterogeneity was present in the analysis. Exclusion of the poorest quality studies (CoE IV) did not change the results or reduce heterogeneity (11 studies,
14,16,17,19,21,22,25,26,28
-30
pooled RR 1.82, 95% CI 1.02-3.25, I2 = 87%).
Forest plot of the association between competitive organized sports and the risk of amyotrophic lateral sclerosis, stratified by levels of competitive play (professional or nonprofessional).
Does the risk vary by higher levels of competitive play (professional vs nonprofessional)?
When stratified by levels of competitive play, professional sports was associated with greater effects (10 comparisons, 8 studies,
14,16,17,21,22,28
-30
pooled RR 4.07, 95% CI 1.99-8.32, I2 = 70%) compared with nonprofessional sports (14 comparisons, 11 studies,
16,18
-27
pooled RR 1.13, 95% CI 0.79-1.62, I2 = 60%), test for subgroup differences, P = .002 (Figure 2).
Does the risk vary by whether the sport is prone to repetitive concussive head and cervical spinal trauma?
Sports prone to repetitive concussive head and cervical spinal trauma was associated with greater effects (8 studies,
14,16,17,20,23,26,28,29
pooled RR 5.98, 95% CI 3.03-11.80, I2 = 56%) than sports not prone to repetitive concussive head and cervical spinal trauma (16 comparisons, 11 studies,
16
-19,21,22,24
-27,30
pooled RR 1.17, 95% CI 0.84-1.63, I2 = 57%), test for subgroup differences, P = .000 (Figure 3).
Forest plot of the association between competitive organized sports and the risk amyotrophic lateral sclerosis, stratified by whether the sport is prone to repetitive concussive head and cervical spinal trauma.
Within different levels of competitive play, does the risk vary by whether the sport is prone to repetitive concussive head and cervical spinal trauma?
Professional sports prone to repetitive concussive head and cervical spinal trauma was associated with substantially greater effects (5 studies,
14,16,17,28,29
pooled RR 8.52, 95% CI 5.18-14.0, I2 = 34%) compared with (a) nonprofessional sports prone to repetitive concussive head and cervical spinal trauma (3 studies,
20,23,26
pooled RR 0.60, 95% CI 0.12-3.06, I2 = 0%); (b) professional sports not prone to repetitive concussive head and cervical spinal trauma(5 comparisons, 4 studies,
17,21,22,30
pooled RR 1.35, 95% CI 0.67-2.71, I2 = 0%); or (c) nonprofessional sports not prone to repetitive concussive head and cervical spinal trauma (11 comparisons, 9 studies,
16,18,19,21,22,24
-27
pooled RR 1.17, 95% CI 0.79-1.71, I2 = 69%), test for subgroup differences, P = .000 (Figure 4). Among professional sports prone to head and neck trauma, 2 studies evaluated the risk by player position. In 1 professional soccer study,
17
midfielders had a greater risk of ALS mortality, standardized morbidity ratio [SMR] 10.5, 95% CI 3.9-22.9) compared with forwards (SMR 6.6, 95% CI 0.2-36.8) and backs (SMR 2.4, 95% CI 0.1-13.4). In 1 study of American professional football,
14
speed positions (fullback, halfback, defensive back, quarterback, wide receiver, running back, linebacker, and tight end) were more likely to die from ALS than nonspeed positions (defensive and offensive linemen), SMR 6.24, 95% CI 2.29-13.6 vs 1.71, 95% CI 0.04-9.50, respectively). A list of professional contact sports athletes publicized as diagnosed with ALS and a case example are presented in Table 2 and Figure 5, respectively.
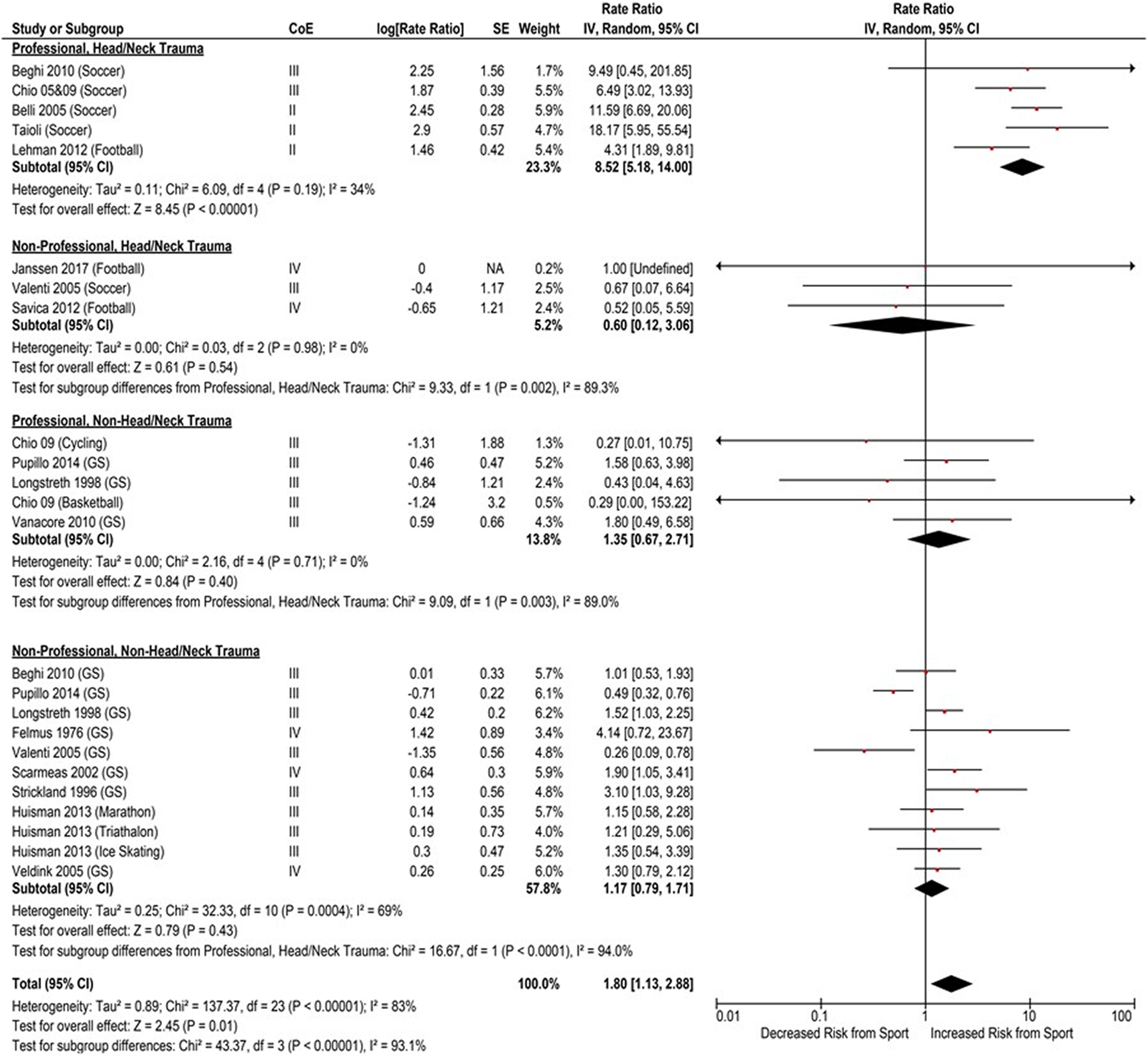
Forest plot of the association between competitive organized sports and the risk of amyotrophic lateral sclerosis, stratified by level of competitive play and whether the sport is prone to repetitive concussive head and cervical spinal trauma.
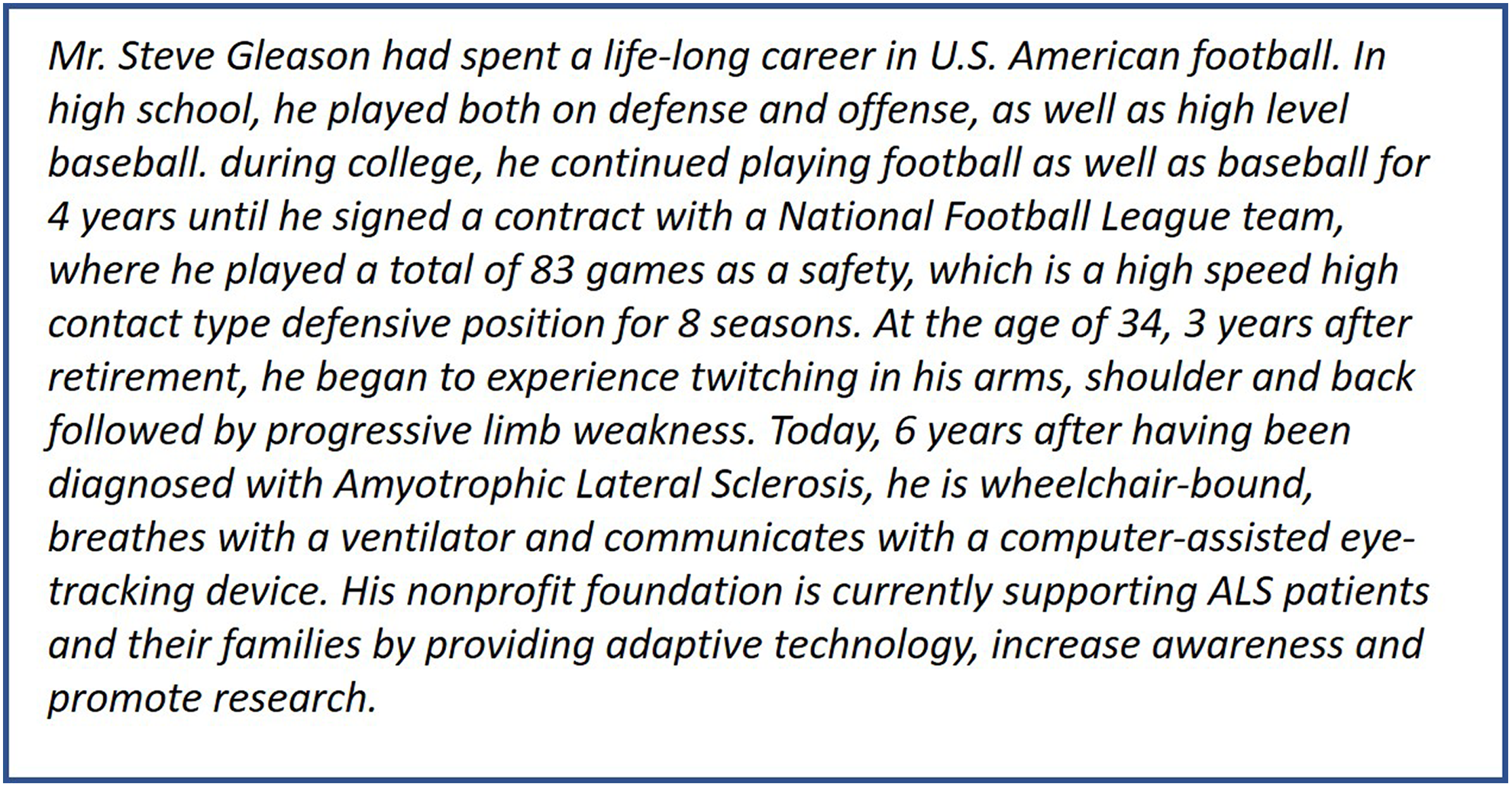
A representative case example.
Professional Contact Sport Athletes Publicized as Diagnosed with ALS.
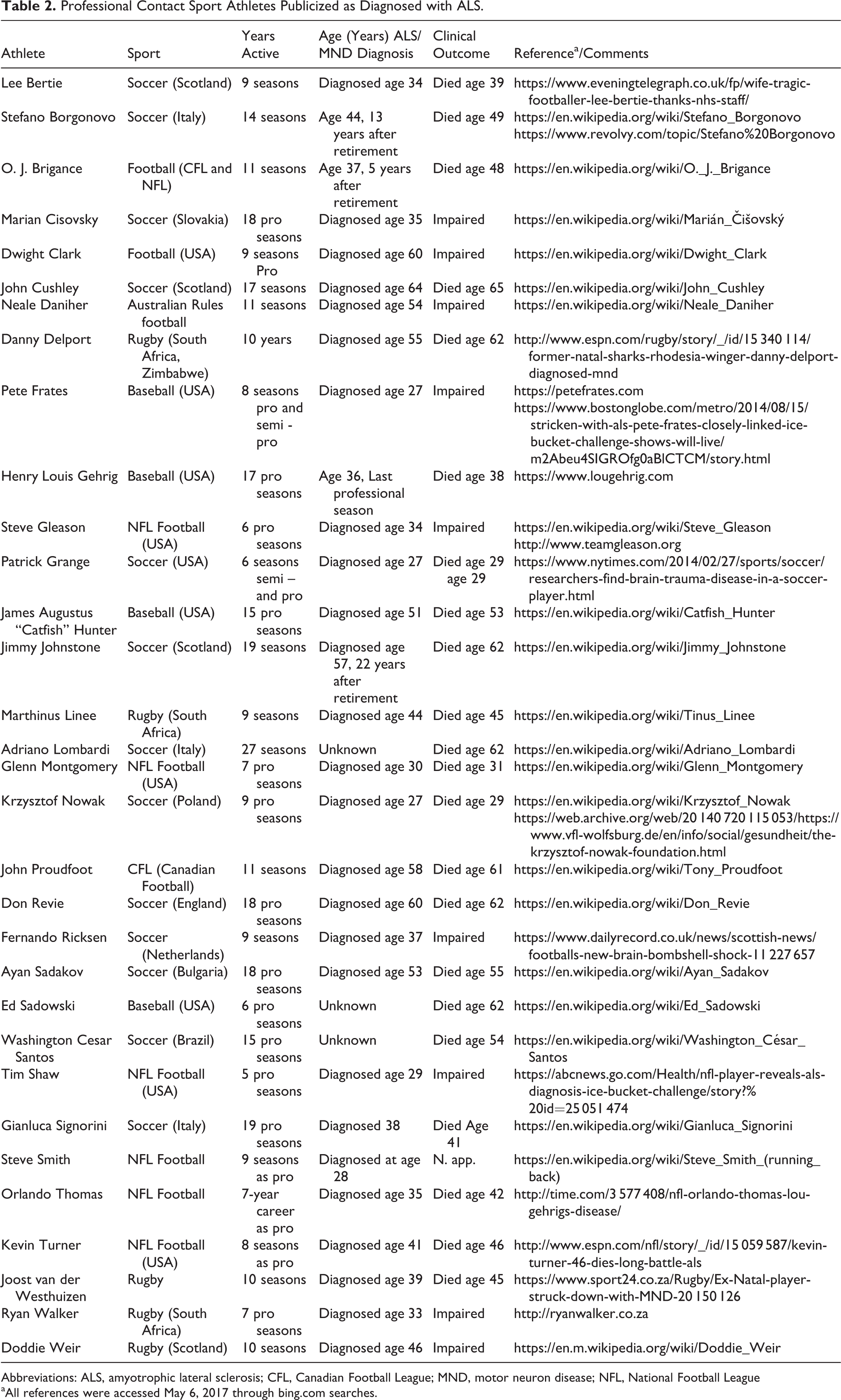
Abbreviations: ALS, amyotrophic lateral sclerosis; CFL, Canadian Football League; MND, motor neuron disease; NFL, National Football League
aAll references were accessed May 6, 2017 through bing.com searches.
Discussion
The recent development of various genetic analysis tools has significantly advanced our understanding of some of the molecular pathways that lead to motor neuron death in ALS patients. 4,5 Furthermore, certain genetic variants have been associated with specific clinical characteristics, providing better estimates of the rate of disease progression and survival. 31 However, possible triggers for the disrupted molecular pathways have remained obscure.
The associations of physical activity 13,19,32 and sports-related trauma 26,33 to ALS have been widely debated. Our review provides evidence that increased susceptibility to ALS may lie in a certain combination of both factors. Competitive organized sports, which usually include high levels of physical activity and sports that include high probability to sustain concussive head and neck trauma were both found to independently increase the risk to develop ALS. When combined together, as is the case with professional American football and soccer, the effect was additive, reaching a rate ratio of 8.52 (Figure 4).
This finding may have several important implications. First, increased awareness among athletes who engage in contact sports as well as by their managing environment, regardless of competitive level, cannot be overemphasized. Precautions aimed at decreasing the likelihood to sustain blunt concussive head or neck trauma, accurate medical documentation and periodic health monitoring may all prove to be life-saving, as is the case with an increased awareness regarding traumatic brain injuries in sports. This is also of potentially increased importance for other professional contact sports lacking similar ALS incidence reports, such as rugby or hockey. In light of these findings additional further formal data-gathering through organizations such as the National Football League and Rugby Union, as is been done with the more recent focus on traumatic brain injury, might also be in order. Second, in light of the accumulated genetic data, future ALS-directed genetic analysis of athletes at-risk may assist in developing appropriate risk-stratification prevention strategies. Third, ALS has been previously associated with chronic traumatic encephalopathy due to some shared clinical and pathological characteristics. 34 Our findings, that sports prone to cervical and head concussive trauma also appear to increase the risk for ALS, highlights an additional region where trauma may play an important role in the pathogenesis of ALS. Cervical cord neuropraxia, also known as transient quadriplegia, is an injury to the spinal cord, usually caused by head collisions with the neck being either hyperflexed or hyperextended. 35,36 This injury, which results in a brief disturbance of limb sensation and/or motor function, commonly lasts less than 24 hours after which the athlete usually displays complete recovery. Whereas usually viewed as a benign condition, our study raises the questions regarding the longer term effects of this type of injury. Our findings warrant further investigation to begin to understand the potential role of brain and spinal trauma in the pathogenesis of ALS.
For spine surgeons and sports physicians who are tasked to assess athletes in contact sports with chronic exposure to head and neck impact trauma with extremity weakness in presence of spinal spondylosis and stenosis the real challenge arises to be aware of the potential of motor neuron disease as an underlying disorder beyond compressive spondylotic myelopathy and radiculopathy.
This systematic review has several limitations. First, there is a significant amount of heterogeneity among the included studies. We attempted to account for this heterogeneity through sensitivity and stratified analyses. Second, a majority of the studies included in this review were judged to have high or moderately high risk of bias due to study design (phase 1 prognostic studies identifying associations between a number of potential prognostic factors and a health outcome 37 ). However, among the subgroup of studies that evaluated professional athletes in sports that are prone to head or neck trauma, 3 of 5 studies were judged to have moderately low risk of bias, 14,28,29 giving us more confidence in the pooled estimate of this subgroup. Third, there is heterogeneity of the diagnostic criteria for ALS among studies. Some used the El Escorial criteria, 16,19,22,26,27 some used study specific criteria, 17,18 and still others used undefined criteria. 20,21,23 -25 Furthermore, some studies enrolled cases based on death certificates. 14,28 -30 While there is some evidence that death certificate diagnosis of ALS is adequate for analytic studies, 38 the variation of the diagnosis on death certificates can be substantial among geographical regions. 39 Fourth, there is substantial variation in sports exposure in our review. Our finding is in keeping with a recent review article by Lacorte et al, 40 where a general sports exposure identified as “physical activity” was identified as an independent risk factor for ALS, but without more specific focus on sports well known to be associated with recurrent head impact trauma. We attempted to control for exposure duration and intensity by stratifying professional versus nonprofessional sports, and by sports prone to head or neck versus no head or neck trauma. However, there were several studies that included any sports activity as a single category that we labeled general sports not defined, which may or may not include sports subject to head or neck trauma. 16,18,21,22,24 -27,30 From a larger systems perspective, this review would seem to invite a more formal evaluation of professional sports exposing its players to repetitive blunt head and neck trauma, such as professional American football, Rugby Union, soccer and ice hockey, possibly also motor racing sports with repetitive impact potential. Despite some case reports of high-profile athletes succumbing to ALS and growing awareness of the deleterious effects of chronic traumatic encephalopathy, so far there have been few if any formal longitudinal or postmortem investigations into a possible association of ALS and high-impact contact sports. Perhaps this systematic review will inspire a more formal investigation on this topic.
Conclusions
Our study raises a number of questions warranting further investigation. In the debate of whether physical activity and sports are related to ALS, we found that professional athletes who engage in sports prone to blunt head or cervical spine concussive injuries such as football and soccer are at an increased risk to develop ALS. This finding has implications in both prevention strategies and in the basic research of ALS pathogenesis.
Supplemental Material
Supplemental_digital_material - Contact Sports as a Risk Factor for Amyotrophic Lateral Sclerosis: A Systematic Review
Supplemental_digital_material for Contact Sports as a Risk Factor for Amyotrophic Lateral Sclerosis: A Systematic Review by Ronen Blecher, Michael A. Elliott, Emre Yilmaz, Joseph R. Dettori, Rod J. Oskouian, Akil Patel, Andrew Clarke, Mike Hutton, Robert McGuire, Robert Dunn, John DeVine, Bruce Twaddle, and Jens R. Chapman in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.