
Abstract
Study Design:
Anatomical cadaver study.
Objectives:
Postoperative dysphagia is a significant complication following anterior approaches to the cervical spine and the etiology of this complication is poorly understood. Herein, we studied the esophageal branches of the recurrent laryngeal nerves to improve understanding of their anatomy and potential involvement in dysphagia.
Methods:
Ten fresh frozen cadaveric human specimens were dissected (20 sides). All specimens were adults with no evidence of prior surgery of the anterior neck. The recurrent laryngeal nerves were identified under a surgical microscope and observations and measurements of their esophageal branches made.
Results:
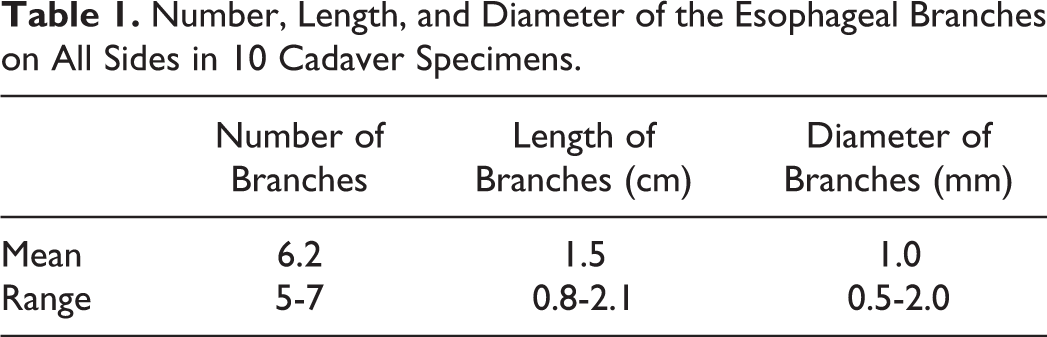
For each recurrent laryngeal nerve, 5-7 (mean 6.2) esophageal branches were identified. These branches ranged from 0.8 to 2.1 cm (mean 1.5 cm) in length and 0.5 to 2 mm (mean 1 mm) in diameter. They arose from the recurrent laryngeal nerves between vertebral levels T1 and C6. They all traveled to the anterior aspect of the esophagus. No statistical differences were seen between left and right sides or between sexes.
Conclusion:
The esophageal branches of the recurrent laryngeal nerve have been poorly described and could contribute to complications such as swallowing dysfunction following anterior cervical discectomy and fusion procedures. Therefore, a better understanding of their anatomy is important for spine surgeons. Our study revealed that these branches are always present on both sides and the anterior surface of the esophagus should be avoided while retracting it in order to minimize the risk of postoperative dysphagia.
Introduction
Anterior approaches to the cervical spine are widely used for treating various conditions, including trauma, cervical spondylosis, spinal tumors, and degenerative changes, especially in symptomatic patients with radiculopathy or myelopathy. 1,2 This approach typically yields good results in halt of disease progression, reduction of pain and entails a low incidence of intraoperative complications. However, postoperative dysphagia is a prevalent risk of this approach. Previous studies have demonstrated a prevalence of postoperative dysphagia following anterior cervical spine surgery (ACSS) of anywhere from 1.7% to 50.3%, a more recent study reporting 26%. 3 -5 Although most patients do not experience long-term dysphagia, up to 10% experience varying degrees of swallowing difficulty for 12 or more months postoperatively. 6 Such difficulties result in reduced quality of life and negative effects on our health care system.
In the case of anterior cervical discectomy and fusion (ACDF), it is speculated that the profile of the implant and its position in the retropharyngeal space, with the possibility of forming adhesions and esophageal abutment, can affect long-term dysphagia. Excessive retraction of the esophageal branches of the recurrent laryngeal nerves could contribute to the development of postoperative dysphagia.
The recurrent laryngeal nerve (RLN) lays on the anterior aspect of the esophagus and the retractor has to be placed carefully lateral to the esophagus and medial the longus colli muscle. To get access to the anterior cervical spine, the retractor has to displace the esophagus, RLN, trachea, sternohyoid muscle, and the thyroid gland contralaterally. 7,8 This could lead to a direct irritation of the RLN and its esophageal branches. We therefore studied the esophageal branches of the RLN to improve understanding of their anatomy and potential involvement in dysphagia.
Materials and Methods
Ten fresh frozen cadaveric human specimens (20 sides) were dissected. All specimens were adults with an average age at death of 78 years (range 49-92 years). Five specimens were male and 5 were female. No specimen had evidence of prior surgery of the anterior neck. The recurrent laryngeal nerves were identified under a surgical microscope (OPMI CS NC31, Carl Zeiss, Oberkochen, Germany) and their esophageal branches were observed and measured. Measurements were made with microcalipers (Mitsutoyo, Kanagawa, Japan). The protocol of this study did not require approval by the ethics committees of our institutions, and the work was performed in accordance with the requirements of the Declaration of Helsinki (64th WMA General Assembly, Fortaleza, Brazil, October 2013). Statistical analysis was performed between sides and sex with significance set at P < .05.
Results
Esophageal branches of the recurrent laryngeal nerves were identified on all sides (Figures 1 and 2). For each RLN, 5 to 7 (mean 6.2) esophageal branches were identified (Figure 3). The length of these branches ranged from 0.8 to 2.1 cm (mean 1.5 cm). Their diameter ranged from 0.5 to 2 mm (mean 1 mm). They arose from the recurrent laryngeal nerves between vertebral levels T1 and C6. Esophageal branches sometimes (20% of sides) arose from a common stem giving rise to both a single tracheal and esophageal branch (Figure 4). When present, these common stems were no more than one per side with the tracheal branches traveling anteriorly to the anterior surface of the trachea and the esophageal branches traveling to the anterior surface of the anterior surface of the esophagus. All single esophageal branches traveled to the anterior aspect of the esophagus. All branches ascended from an inferior direction at an oblique, almost vertical course toward the anterior wall of the esophagus. Retractor blade replacement onto the lateral surface of the esophagus did not compress esophageal branches of the left or right recurrent laryngeal nerves. No nonrecurrent laryngeal nerves were identified or signs of local pathology such as lymphadenopathy. Although in general, the female specimens had fewer esophageal branches, this did not reach statistical significance. Additionally, no statistical differences were seen between left and right sides (P > .05). The results are summarized in Table 1.
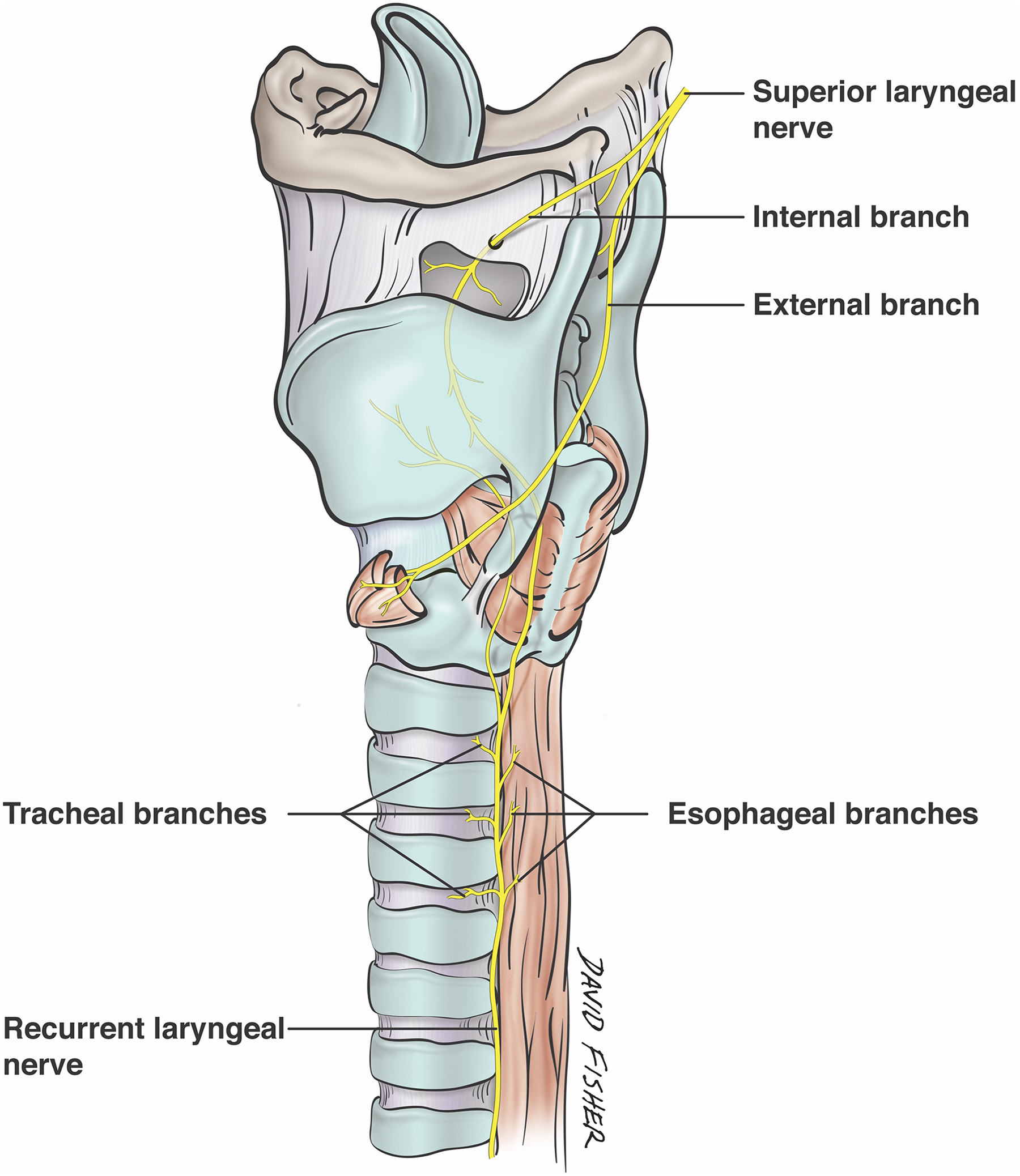
Label drawing illustrating the esophageal branches on the left side.
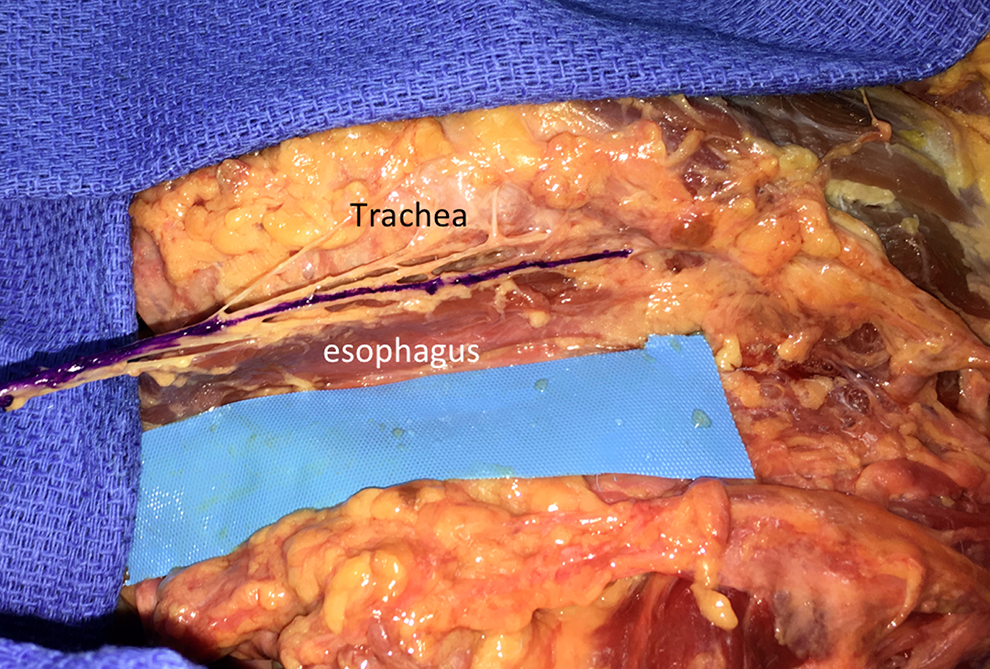
Left cadaveric dissection noting the tracheoesophageal groove. The left recurrent laryngeal nerve is seen in purple. Branches to the esophagus and trachea are difficult to visualize in this position.
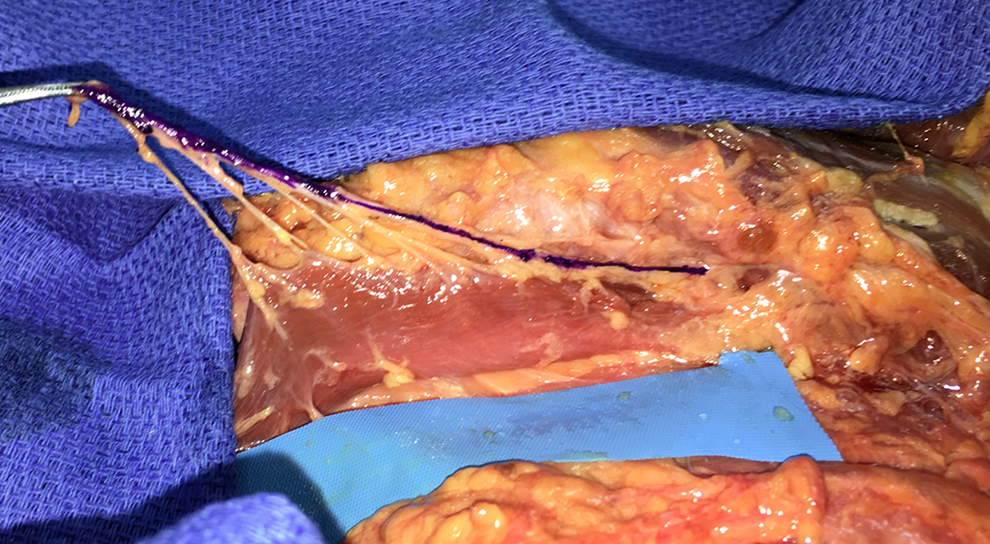
Figure 2 with the inferior aspect of the left recurrent laryngeal nerve lifted to illustrate branches traveling to the anterior aspect of the esophagus.
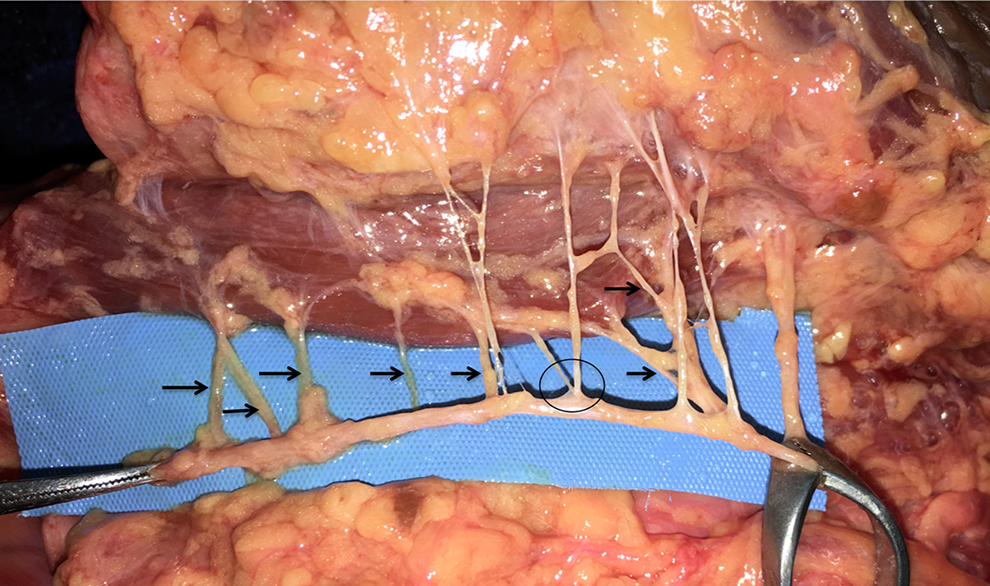
Lateral retraction on the left recurrent laryngeal nerve highlighting esophageal branches (black arrows). A common nerve stem giving rise to an esophageal and tracheal branch is seen at the circle.
Number, Length, and Diameter of the Esophageal Branches on All Sides in 10 Cadaver Specimens.
Discussion
Dysphagia is a common postoperative complication with ACSS. Despite its prevalence, its etiology is still not well understood, and incidences of postoperative dysphagia differ significantly among studies. Prevertebral swelling, hematoma and the prominence of the cervical plate are considered to be possible causes. 9 -11 We have studied the esophageal branches of the RLN to improve our understanding of their anatomy and potential involvement in postoperative dysphagia.
Our dissections showed that all esophageal branches arose from the RLN between vertebral levels T1 and C6. This could suggest that an ACSS is more likely to occur in patients who underwent anterior surgery in the lower cervical spine (C6-T1) compared with the mid (C3-C5) or upper (C1-C3) cervical spine. To our knowledge, there is no study supporting this suggestion. Furthermore, Carucci et al 12 reported in their retrospective study analyzing 1789 patients who underwent anterior cervical fusion that dysphagia was most likely occur following surgery in the mid (9.6%) cervical spine compared with the upper (7.4%) or lower (2.2%) cervical spine. However, a postoperative hematoma and/or swelling is not only limited to the operated level. Furthermore, C4-C6 are reported to be the most common osteophyte levels resulting in dysphagia. 13 Nevertheless, our findings suggest that a dysphagia caused by direct compression or manipulation of the esophageal branches is more likely to occur in the lower cervical spine. However, as already mentioned by Carucci et al, 12 the increased incidence of dysphagia after anterior spine surgery in the mid cervical spine is most likely multifactorial caused by altered swallowing mechanisms with abnormal epiglottis function and displacement of the pharynx.
A potential factor in postoperative dysphagia related to ACSS is injury to the branches of the RLN resulting from retractor placement and profile. 11 In this study, we hypothesize that this is the most significant contributor as the esophageal branches of the RLN are poorly described in the current literature. Liebermann-Meffert et al 14 conducted a similar study mapping the anatomy of the RLNs. They found that the left RLN contained 2 to 7 branches (mean, 5 branches) and the right RLN contained 5 to 11 (mean, 9 branches) to the esophagus. Furthermore, they found the length of each branch ranged from 1.8 to 2.5 cm. This data is similar but not identical to our findings. Compared with this study, we found no statistical differences between the left and right RLNs in our dissections. Both RLNs contained 5 to 7 esophageal branches (mean, 6.2) with branch length ranging from 0.8 to 2.1 cm (mean, 1.5 cm).
Liebermann-Meffert et al 14 went on to identify surgeons’ unfamiliarity with RLN structure and composition as a primary cause of perioperative injury and postoperative dysphagia during ACSS. Another study by Steinberg et al 15 concluded that the RLNs on both sides of the neck have 2 divisions, one going to the larynx and the other to the cricopharyngeus muscle. The laryngeal division branches both anterior and posterior to the esophagus with each branch being responsible for different actions: The anterior branch is more involved in motor control whereas the posterior is more involved sensation. 15 Thus, injury to the anterior laryngeal division of the RLN could relate to various degrees of loss of motor function in the esophagus.
Also, many studies identify potential causes of dysphagia following ACSS. Li et al 16 suggested in their study of rats that the lateral half of the right thoracic vagus nerve is responsible for neurogenic inflammatory responses related to parts of the esophagus, whereas the RLN is primarily responsible for regulating inflammatory responses in the upper and dorsal portions of the trachea. These findings raise the question of whether the right thoracic vagus nerve is involved in dysphagia following ACSS. 16
A rare but possible cause of dysphagia is a diffuse idiopathic skeletal hyperostosis (DISH). This ossification of the anterior longitudinal ligament occurs most commonly in the thoracic spine. Mild asymptomatic forms are often seen in the cervical spine in elderly patients. However, the osteophytes can lead to local compression and cause dysphagia when it occurs in the cervical spine. 17 -19
In terms of risk factors, Siska et al 20 found that smokers are statistically significantly more prone to postoperative dysphagia than nonsmokers. Olsson et al 5 also found that the prevalence of postoperative dysphagia from ACSS among smokers tended toward statistical significance (P < .08). Thus, both studies identified smokers as being at risk for developing postoperative dysphagia following ACSS. Other factors, including age, sex, body mass index, and number of levels fused have yielded little or no correlation with increased risk for postoperative dysphagia. 5,21
The use of steroids in the treatment of postoperative dysphagia remains controversial although many reports suggest that steroids might reduce prevertebral swelling. 22,23 However, other studies failed to confirm this effect and the existing studies used highly variable steroid schemes and doses, which makes a well-founded conclusion extremely difficult. 24
In terms of prevention, Apfelbaum et al 25 found one method with significant results. In their study, endotracheal tube injury was limited by an inflated endotracheal cuff. By releasing and then reinflating the cuff after placement of a cervical retractor, Apfelbaum et al 25 could maintain a central positioning of the endotracheal tube, thereby minimizing injury to the RLNs. They performed their procedure on 650 patients and found a decrease in incidence of postoperative RLN palsy from 6.8% to 2.0%. Furthermore, performing ACSS laterally, which is ultimately what we recommend, Rajabian et al 26 found the inferior thyroid artery and Berry’s ligament to be reliable landmarks for attempts to identify and avoid the RLNs. Such anatomical landmarks could help surgeons to refine techniques for identifying RLNs during surgery in order to minimize unnecessary injury. 26
Overall, reports in the existing literature are very heterogeneous. Many studies are retrospective, there are differences in the measurement of swallowing difficulty, and there could be surgeon bias. Furthermore, patient follow-up times are not the same in different studies. For instance, Bazaz et al, 3 who found postoperative dysphagia rates of 50.3% at 1 month, had follow-up times of 1, 2, 6, and 12 months. However, Yue et al 27 found the incidence to be 35.1% with an average 7.2-year follow-up, and Olsson et al 5 found a 26% incidence with an average 2.75-year follow-up.
However, these etiologies and results require further study. Prospective randomized controlled trials, including a precise study setting, definition of postoperative dysphagia, the time range and a comparison of upper, mid and lower cervical spine surgeries in respect to dysphagia would be optimal to fully understand postoperative dysphagia.
Conclusion
The esophageal branches of the recurrent laryngeal nerve have been poorly described and could contribute to complications such as swallowing dysfunction following anterior cervical discectomy and fusion procedures. Therefore, a better understanding of their anatomy as seen in the present study is important for spine surgeons who often depend on anatomical landmarks for avoiding vulnerable neurovascular structures during surgical approaches. 28 -31 Our study revealed that these branches are always present on both sides and the anterior surface of the esophagus should be avoided while retracting it to minimize the risk of postoperative dysphagia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.