
Abstract
Study Design:
Longitudinal comparative cohort.
Objectives:
To determine if the duration of symptoms in patients with degenerative spondylolisthesis affects postoperative outcomes after 1- or 2-level decompression and fusion.
Methods:
Patients undergoing primary surgery for grade 1 degenerative spondylolisthesis at a single Quality Outcomes Database (QOD) participating site were identified. Demographic, surgical and patient-reported outcomes (PROs) data, including baseline and 12-month postoperative Oswestry Disability Index (ODI), back pain (BP, 0-10), leg pain (LP, 0-10), and EuroQOL-5D (EQ-5D) scores were collected. Individual medical records were reviewed for data on duration of symptoms prior to surgery. Patients were stratified into 3 cohorts—those with preoperative symptom duration of less than 1 year, 1 to 2 years, or greater than 2 years.
Results:
Complete data was available in 123 patients. Significant improvement in ODI, BP, and LP scores were observed in all groups. At 12-month follow-up improvement in ODI, BP, or LP was similar among the cohorts; with a trend toward significance with better improvement in LP scores in patients with a symptom duration of less than 1 year to those with symptom duration greater than 2 years (P = .058).
Conclusions:
The duration of symptoms up to 2 years prior to surgery may not be a useful predictor of improvement of back pain or disability scores in patients with spondylolisthesis requiring decompression and fusion. Although there was a positive trend for improvement in leg pain for those with a shorter duration of symptoms, this did not reach statistical significance in our study.
Introduction
Surgical decompression and fusion has been shown in multicenter trials to improve health status in well-selected patients with lumbar degenerative disease who have failed conservative treatment. 1 -3 A recent meta-analysis concluded that patients who received fusion for spondylolisthesis had a greater improvement in Oswestry Disability Index (ODI) as compared with those who received spine surgery for other indications. 4
Prior studies have shown that the duration of leg pain impacts surgical outcomes in patients undergoing decompression for disc herniation or stenosis, 5,6 with longer duration of symptoms correlating with a blunted improvement in postoperative symptoms. However, the effect of symptom duration on surgical outcomes after decompression and fusion for degenerative lumbar spondylolisthesis has been debated, as prior studies have shown conflicting results. 7 -9
While some studies failed to show a difference in outcomes among patients with a shorter duration of symptoms prior to surgery 9,10 more recent studies have reached different conclusions. 7,8 The results of prior studies may have been affected by heterogeneous cohorts containing patients both with and without spondylolisthesis, or concurrently examining outcomes after decompression alone and decompression with fusion. This study intends to reconcile these divergent results by exclusively examining patients with a 1- or 2-level degenerative spondylolisthesis and stenosis who underwent decompression and fusion. The hypothesis is that patients with 1- or 2-level degenerative spondylolisthesis and stenosis who have had symptoms 2 years prior to surgery will have worse outcomes compared to those with shorter duration of symptoms. Our aim is to determine if the duration of symptoms prior to surgery effects postoperative outcomes in this group.
Methods
After receiving institutional review board approval, patients who had primary lumbar spine decompression and fusion for grade 1 spondylolisthesis enrolled from 2013 to 2015 at a single Quality Outcomes Database (QOD) participating site were identified. The QOD lumbar module 11 -13 is a prospective observational registry that collects standard demographic and surgical data, 30- and 90-day morbidity; and baseline, 3- and 12-month patient-reported outcomes (PROs). Six cases per site are enrolled per week on a rolling 6-day cycle; so that the first day of each 6-day week falls on each weekday with equal frequency. This creates a sampling method that prevents a disproportionate volume of enrollment on any 1 day of the week or from any 1 surgeon’s schedule at any 1 site, thus limiting potential enrollment bias. Patients enrolled in QOD are assigned a principal spine diagnosis by the operating surgeon. Principal spine diagnoses at the time QOD was queried included symptomatic lumbar disc herniation; symptomatic recurrent lumbar disc herniation, spondylolisthesis, stenosis, and adjacent segment disease.
Local site QOD data was downloaded from RedCap, the software platform for N2QOD onto SPSS IBM SPSS software version 21.0 (Armonk, NY). Filters were the used to identify patients that met inclusion criteria. Demographic characteristics collected included age, sex, body mass index (BMI), race, educational level, employment status, diagnosis, insurance status, workers’ compensation status, and American Society of Anesthesiologists grade. 14 Numeric rating scales (0 to 10) for back pain (BP) and leg pain (LP), 15,16 surgical, and PRO data, including baseline and 12-month postoperative ODI, 17 and EuroQOL-5D (EQ-5D) 18 scores were collected. Individual medical records were reviewed for data on duration of symptoms prior to surgery. The most recent episode of back pain exacerbation for which the patient sought surgical consult for was considered as the patient’s duration of symptoms. Patients were stratified into 3 cohorts—those with preoperative symptom duration of less than 1 year, 1 to 2 years, or greater than 2 years. These time frames were selected in order for the current study to be comparable to previously published literature. Prior studies used similar time frames, 5 -9 with a majority using the cutoffs used in the SPORT trials. 2,3,9 An additional time frame of 1 to 2 years was added to the current study in order to increase the increase the sensitivity. A longer time frame of greater than 2 years was also added as it has been our experience is that patients with a degenerative condition like spondylolisthesis have a longer duration of symptoms. Of 172 patients meeting inclusion criteria complete data was available in 123 (72%) patients.
Statistical analysis was carried out with IBM SPSS software version 21.0. Statistical significance was set at P < .05. One-way analysis of variance was used to determine differences in continuous variables, and Fisher’s exact test was used to determine differences in categorical variables among the 3 cohorts. Spearman’s correlation (rs) was used to determine associations between the symptom duration and change in patient reported outcomes after surgery in the 3 cohorts.
Results
Demographic data was similar among the 3 cohorts in terms of age, gender, workers compensations status, and American Society of Anesthesiologists grade (Table 1). Preoperative PROs were also similar among the groups. The proportion of patients reporting that they were moderately or extremely anxious in the Anxiety-Depression domain of the EQ-5D was similar among the 3 groups (P = .373). The majority of the subjects (78, 63%) had a single level posterior decompression and fusion. Approximately half (63, 41%) had an interbody fusion. Statistically significant improvements in ODI, BP, and LP scores from baseline to 12 months post-operative were observed in all groups (Table 2). However, at 12-month follow-up, there was no statistically significant difference in improvement in ODI (P = .355), BP (P = .508), or LP (P = .153) among the 3 cohorts (Table 2). Despite a lack of statistical significance, there was a trend toward significance with better improvement in LP scores in patients with a symptom duration of less than 1 year compared to those with symptom duration greater than 2 years (P = .058). Power analysis showed that the current sample size of 123, at an α = .05 and a moderate effect size (0.30) has a power of 0.83 to show a difference between the 3 groups. 19
Summary of Demographic Data.
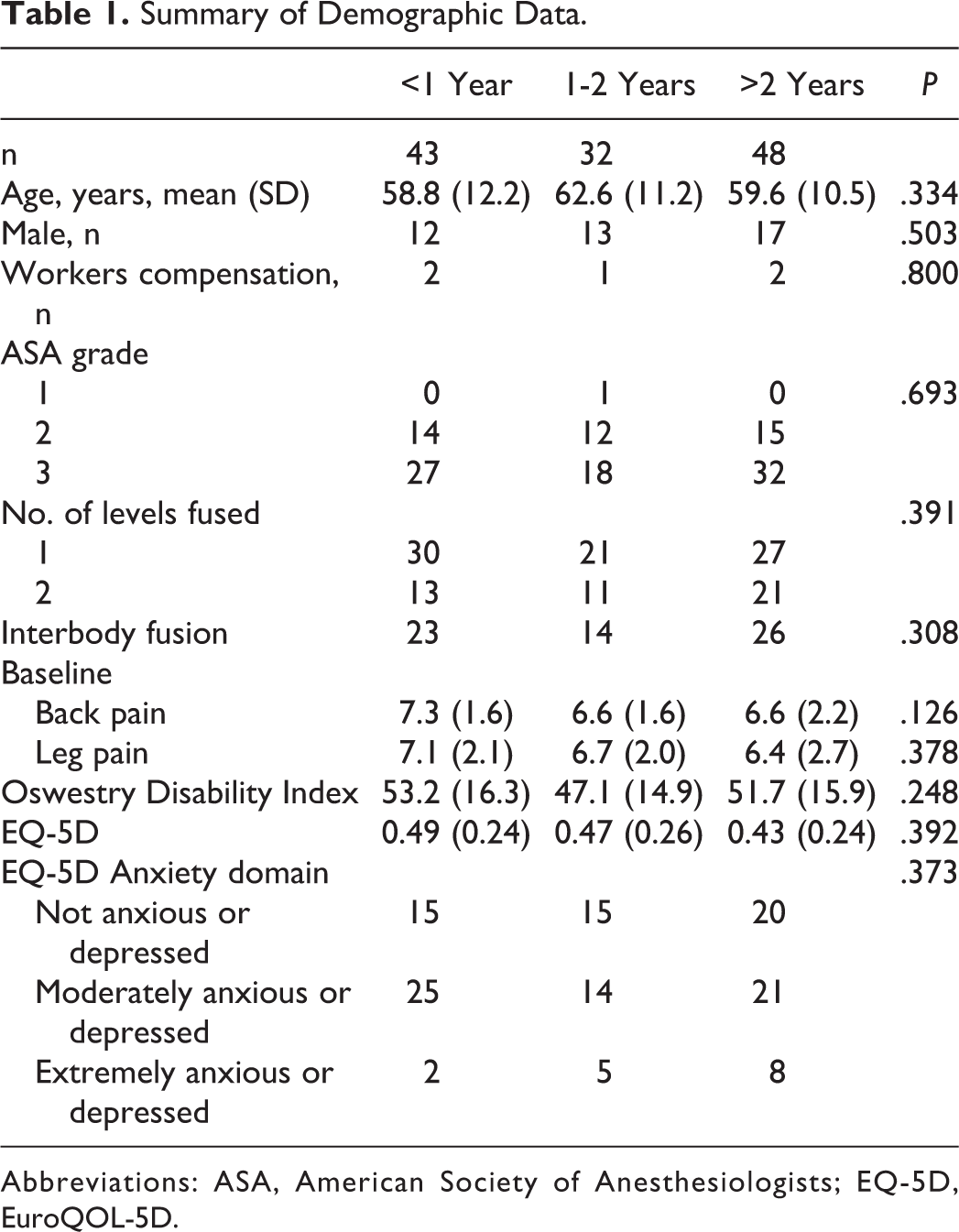
Abbreviations: ASA, American Society of Anesthesiologists; EQ-5D, EuroQOL-5D.
Summary of 12-Month Patient-Reported Outcomes.
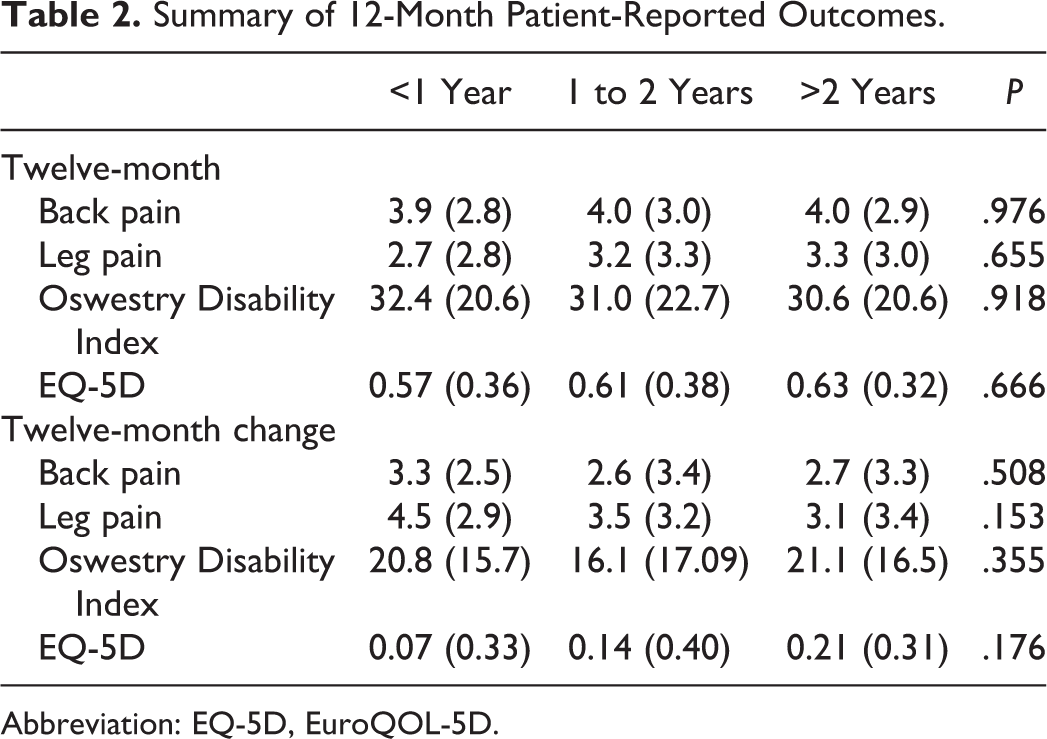
Abbreviation: EQ-5D, EuroQOL-5D.
Discussion
Across multiple studies, the use of spinal fusion for the treatment of symptomatic spondylolisthesis had been shown to improve outcomes as compared with symptomatic treatment alone. 1 -4 The Spine Patient Outcomes Research Trial (SPORT) was designed to address the utility of spine surgery as compared with nonsurgical treatment for a variety of spine conditions. In this trial, an as-treated comparison showed that patients with spinal stenosis and spondylolisthesis fared better—in terms of function and pain relief—at 2 years 3 and 4 years 2 after spinal fusion surgery than those who received nonoperative treatment. However, a significant amount of variability in patient improvement has been observed among different patients, and between different centers. 20 Thus, there has been a push in the surgical community to identify factors that may predict the outcomes of individual patients. Our study aims to specifically address the outcomes with different symptom duration prior to operative treatment, as this is a potentially modifiable risk factor in determining the timing of elective surgery.
Previously collected data had determined that duration of leg pain was a significant factor in improvement after surgical decompression for lumbar disc herniation. 5,6 Duration of leg pain of less than 8 months correlated with better clinical outcomes postoperatively. 5 However, this data addressed a population of patients with a relatively acute condition, lumbar disc herniation. The question remained as to whether this finding extended to other populations, namely those with more chronic conditions such as spondylolisthesis.
In prior studies based on SPORT, a significant difference was found between patients treated for spinal stenosis alone with symptom duration of less than 1 year, as compared to those with symptoms of greater than 1 year. On as as-treated analysis, those who received earlier surgical treatment fared better on SF-36 and ODI outcomes. 9 However, this finding did not carry over to the spondylolisthesis cohort—no difference was found between the symptom duration cohorts. There were inherent limitations present in this study, as the specific surgical treatment, decompression alone versus decompression and fusion, was not controlled among cohorts. Some spondylolisthesis patients were treated with nonfusion decompression. Additionally, the inherent limitations of SPORT were present in this study; the trial was not designed to compare 2 surgical cohorts, and there was a high degree of crossover.
More recent research sought to determine if the wait time to surgery for patients with degenerative spine conditions affected short- and medium-term clinical outcomes. 7,8 Braybrooke et al 8 examined if time spent on a Canadian wait list for surgery effected the outcome for lumbar spinal disease. A component of this study was based on the time between symptom onset and surgery. With a median symptom duration of 409 days, there was found to be a significant correlation between duration and the physical subsections of the Short Form–36 Health Questionnaire (SF-36) component and domain scores. 8 Additionally, those with a wait time greater than the median were found to have less improvement in ODI as compared to those with a shorter wait time.
Similarly, Bailey et al 7 studied the outcomes for patients with a median wait time of less than, or greater than 12 months. There was a positive correlation between longer wait time and high ODI scores (worse outcome) at 6-month (P < .01) and 12-month (P < .05) follow-ups; however, there was no difference at the 24-month follow-up. The authors suggested that a wait of more than 12 months for surgical treatment resulted in delayed improvement. Notably, this study did not look at symptom duration specifically. Rather, it focused solely on the time spent on a wait list for surgery, which may comprise a mix of different symptom duration groups.
One of factors that has been shown to affect outcomes of spine surgery in patients with chronic low back pain is the presence of depression and anxiety. 21 Although in the current study the presence of depression and anxiety status were not directly assessed, the proportion of patients reporting that they were moderately or extremely anxious in the Anxiety-Depression domain of the EQ-5D was similar among the 3 groups. This may mean the presence of anxiety or depression in the current study cohort is not associated with the length of symptoms.
Our research limited the study population to 123 patients who received 1- or 2-level fusion for degenerative spondylolisthesis, and specifically examined patient reported duration of symptoms. This cohort condition comprises a representative sample of patients often treated for degenerative conditions in the United States. Through homogeneity of our treatment group, we hoped to avoid confounding factors present in some prior studies. Although it may be possible that patients with worse symptoms present early, or the intensity of the pain or disability might be driving a more expeditious surgical intervention, our data showed that the three cohorts had similar baseline ODI, BP, or LP numerical scores.
All cohorts with spondylolisthesis who received a fusion surgery showed improvement in symptoms, consistent with previous data. 1 -3,22 However, there was no significant difference found in ODI, BP, or LP numerical scores between patients with a symptom duration of less than 12 months, 12 to 24 months, or greater than 24 months. This lack of significance may be due to the small sample size within the cohorts as well as the relatively large standard deviations of the ODI, BP, or LP scores at 12 months after surgery. This is consistent with data published by SPORT for this specific degenerative group. Nevertheless, when comparing leg pain improvement between patients with symptom duration of less than 12 months and greater than 24 months, there was a trend toward significance (P = .058). Combined with the observation of Radcliff et al 9 that patients who received predominantly decompression surgery for spinal stenosis had a greater improvement with more expedient surgery, this finding may suggest a dichotomy between the effects of symptom duration on improvement after neurologic decompression, as compared with fusion/osseous stabilization.
The LP component of the pain rating likely has a root cause of radicular compression originating in the spinal column. However, BP is multifactorial, and may be composed of musculoskeletal pain generators, as well as pain originating from the facet joints and/or intervertebral discs. 10 Studies involving treatments that focus on reliving neurologic compression and leg pain seem to show a greater dependence on symptom duration for improvement, 5,6,9 perhaps elucidating the decreased propensity for recovery after prolonged neural compression.
There were several limitations present in our study. As a retrospective cohort analysis, blinding and randomization were not possible. Thus, some potential confounding factors may have gone unrecorded. Although differences were not found through a subgroup analysis examining symptom duration as a continuous variable, it is possible that cohorts of different time frames than those studied may have produced dissimilar statistical conclusions.
Differential losses to follow-up may also have limited the observation of treatment effect. As the symptom duration was based on preoperative patient reporting, there remains the possibility of recall bias. In addition, longer follow-up may be necessary to fully evaluate the outcomes of surgical treatment on patients with degenerative spondylolisthesis.
Based on our study, it seems that for patients planning 1- or 2-level fusion for degenerative spondylolisthesis, there is likely little detriment to delaying surgery for up to 2 years after symptom onset to complete full trials of nonoperative, conservative care. Additionally, patients who have had a longer duration of symptoms should not be expected to have less proportionate improvement in back pain or disability postoperatively. Although it did not reach statistical significance in our study, our trend toward less symptomatic improvement in leg pain indicates that spine surgeons may counsel patients with predominantly long-term radicular symptoms on the possibility of a less robust treatment effect after surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SDG is an employee of Norton Healthcare; received consulting and royalties from Medtronic. JRD is an employee of Norton Healthcare; receives royalties, consulting and speaker fees from Medtronic; and is a Member of Board of Directors of the Scoliosis Research Society. LYC is an employee of Norton Healthcare; Member, Editorial Advisory Board, Spine Deformity, Spine and Spine Journal; Institutional Review Board Member, University of Louisville; Research Committee Member, Scoliosis Research Society; receives research funds from the Orthopedic Research and Educational Fund, 2013 to present; received funds for travel for Study Planning Meetings from the Center for Spine Surgery and Research of the University of Southern Denmark; University of Louisville. The authors’ institution received research support from Norton Healthcare, Integra, IntelliRod, and Pfizer.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.