
Abstract
Study Design
Retrospective cohort study.
Objective
Endoscopic cervical decompression (ECD) has emerged as a minimally invasive alternative to open cervical decompression, but large-scale comparative data evaluating short-term safety and long-term reoperation remain limited.
Methods
A retrospective cohort study was performed using the TriNetX Global Collaborative Network for adults undergoing endoscopic or open cervical decompression. Thirty-day medical, surgical, and healthcare utilization outcomes were evaluated. Time-to-fusion was analyzed with Kaplan–Meier curves and Cox proportional hazards ratios.
Results
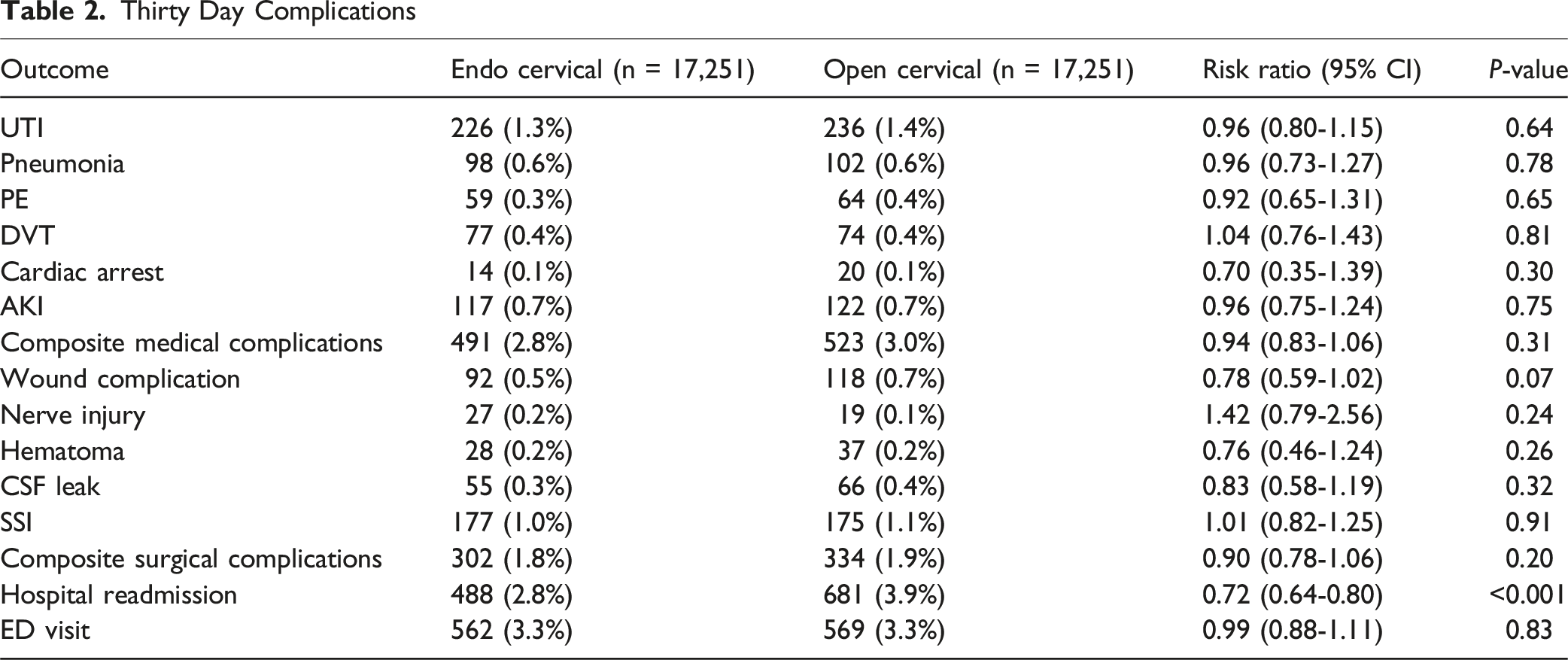
After matching, 17 251 ECD patients were included in each cohort. Thirty-day medical (2.8% vs 3.0%; P = 0.31) and surgical complications (1.8% vs 1.9%; P = 0.20) were similar. Hospital readmission occurred less frequently after ECD (2.8% vs 3.9%; RR 0.72, 95% CI 0.64-0.80; P < 0.001), while ED visits were comparable (3.3% vs 3.3%; RR 0.99, 95% CI 0.88-1.11; P = 0.83). Long-term outcomes showed a significant elevation in subsequent cervical fusion after ECD from 1 to 5 years (log-rank P < 0.001). At 1 year, fusion occurred in 4.2% of ECD patients vs 2.7% of open patients (HR 1.55, 95% CI 1.37-1.75; P < 0.001). At 5 years, cumulative fusion incidence reached 5.9% vs 3.9% (HR 1.48, 95% CI 1.34-1.64; P < 0.001). In a contemporary-era sensitivity analysis (2021-2024), findings remained directionally consistent at 1 and 2 years, although statistical significance was not reached.
Conclusion
ECD offers comparable perioperative safety and lower readmission but carries a higher long-term risk of subsequent cervical fusion, highlighting the importance of counseling patients regarding potential reoperation risk.
Keywords
Introduction
Endoscopic cervical decompression (ECD) has emerged as a minimally invasive alternative to traditional open posterior cervical decompression for the management of cervical radiculopathy, stenosis, and degenerative disc disease.1-3 Cervical radiculopathy has an estimated annual incidence of 80-110 per 100 000 individuals, most commonly arising from age-related spondylosis or disc herniation, with radiographic degenerative changes present in the majority of adults over 50 years of age.4-6 Given the high prevalence and associated functional burden of degenerative cervical disease, surgical intervention remains common for patients who fail conservative management.
Current standards of operative management include anterior cervical discectomy and fusion (ACDF), cervical disc arthroplasty, and posterior cervical foraminotomy, with approach selection determined by pathology location, sagittal alignment, and the presence of instability.7-9 Open posterior decompression techniques are well established and supported by decades of longitudinal data demonstrating durable symptom relief, but are associated with greater paraspinal muscle disruption, postoperative axial neck pain, and prolonged recovery.10,11 By minimizing muscle dissection and soft-tissue trauma, ECD aims to reduce perioperative morbidity while preserving the efficacy for neural decompression. 12 Early institutional studies have reported favorable short-term outcomes, including reduced post-operative pain, short hospitalization, and rapid functional recovery.12-16 Despite these advantages, widespread adoption of ECD has been limited by the absence of large-scale comparative data evaluating both short-term and long-term reoperation risk.
In particular, the long-term durability of ECD relative to open decompression remains an area of active investigation. While open decompression benefits from extensive evidence supporting its biomechanical stability and sustained clinical efficacy, the selective and targeted nature of ECD may introduce distinct biomechanical considerations.17-19 Finite element analyses and kinematic studies suggest that limited bony resection and facet preservation, while advantageous for motion conservation, may predispose certain patients to recurrent foraminal stenosis, incomplete decompression, or progressive segmental instability requiring revision surgery or conversion to fusion.17-19 Existing comparative studies are further limited by small sample sizes, heterogeneous endoscopic techniques, variable surgeon experience, and relatively short follow-up durations, constraining definitive conclusions regarding long-term reoperation risk.20-22
The present study aims to address these gaps by utilizing a large international real-world database to compare 30-day medical and surgical complications and 1-5 year conversion to cervical fusion between patients undergoing ECD and those undergoing open decompression for degenerative cervical disease. By assessing both short-term and long-term structural durability, this study provides clinically meaningful evidence to inform patient selection, risk counseling, and expectations regarding long-term outcomes following endoscopic cervical spine surgery.
Methods
Study Design and Data Source
We conducted a retrospective cohort study from using the TriNetX Global Collaborative Network, which aggregates real-world electronic health record data from healthcare organizations across multiple countries. The network includes patient demographics, diagnoses, procedures, medications, laboratory values, and longitudinal follow-up. All data within TriNetX are de-identified in compliance with Health Insurance Portability and Accountability Act (HIPAA) and therefore, institutional review board (IRB) approval was not required. Informed consent was not required due to the use of fully de-identified data.
Patient Population
Adult patients aged 18-80 years who underwent primary cervical decompression for degenerative pathology between were eligible for inclusion. Endoscopic cervical decompression cases were defined using International Classification of Diseases, 10th Revision Procedure Coding System (ICD-10-PCS) codes for percutaneous endoscopic excision or release of cervical vertebral elements. Open decompression cases were identified using corresponding open-approach excision and release codes. These ICD-10-PCS codes are approach-based and capture percutaneous endoscopic decompression procedures but do not distinguish between full-endoscopic, biportal, or microendoscopic-assisted techniques, and therefore likely represent a spectrum of minimally invasive posterior decompression approaches rather than a single uniform procedure. Patients were required to have a degenerative cervical diagnosis (cervical disc disorder, cervical stenosis, radiculopathy, or cervical spondylosis with myelopathy or radiculopathy) prior to the index procedure. Exclusions included traumatic, infectious, neoplastic, or inflammatory cervical pathology, or prior cervical fusion identified through ICD-10-PCS fusion families (0RG0-0RG4). The index event was defined as the first qualifying decompression, and postoperative outcomes were assessed beginning 1 day after the index date (Supplemental Table 1).
Matching Protocol
Propensity score matching was used to minimize confounding between treatment groups. A 1:1 nearest-neighbor matching algorithm without replacement was applied with a caliper of 0.1 on the logit of the propensity score. Covariates included age, sex, race, ethnicity, hypertension, diabetes mellitus, obesity, chronic kidney disease, chronic obstructive pulmonary disease, ischemic heart disease, heart failure, nicotine dependence or tobacco use, osteoporosis and other bone density disorders, nutritional anemias, and coagulation disorders (Supplemental Table 2). After application of the matching, covariates were assessed for excellent balance if they had a standardized mean difference (SMDs) less than 0.1.
Outcomes
The primary outcome was subsequent cervical fusion within 1 to 5 years following the index decompression. Fusion events were identified using standard cervical arthrodesis procedure definitions and time-to-event was measured beginning 1 day after the index procedure. Cumulative fusion incidence was evaluated at 1, 2, 3, 4, and 5 years. Secondary outcomes included 30-days postoperative complications. Medical complications comprised urinary tract infection (UTI), pneumonia, pulmonary embolism (PE), deep vein thrombosis (DVT), acute kidney injury (AKI), cardiac arrest. Surgical complications included postoperative wound disruption, postoperative nerve injury, hematoma, cerebrospinal fluid (CSF) leak, and surgical-site infection (SSI). Composite medical and surgical complication outcomes were also constructed using the corresponding individual complication codes. Additional secondary outcomes included 30-days hospital readmission and emergency department (ED) visitation.
Statistical Analysis
Descriptive statistics were calculated for both unmatched and matched cohorts. Categorical variables were summarized as counts and percentages and compared using the chi-square test, while continuous variables were presented as means with standard deviations and compared using independent samples t-tests. Between-group differences in postoperative complications were evaluated using risk ratios (RRs) with 95% confidence intervals (CIs). Statistical significance was defined as P < 0.05 for all two-tailed tests. Time to subsequent cervical fusion was assessed using the Kaplan–Meier survival analysis, and differences between survival curves were evaluated using the log-rank test. Hazard ratios (HRs) with 95% CIs were derived from Cox proportional hazards models. All statistical analyses were performed within the TriNetX Analytics platform.
Temporal Sensitivity Analysis
To account for temporal changes in surgeon experience and maturation of endoscopic cervical techniques, a sensitivity analysis was performed restricting the cohort to procedures performed between January 1, 2021 and December 31, 2024. Outcomes were re-evaluated using the same matching and analytic framework for 1-year and 2-year subsequent cervical fusion.
Results
Cohort Characteristics
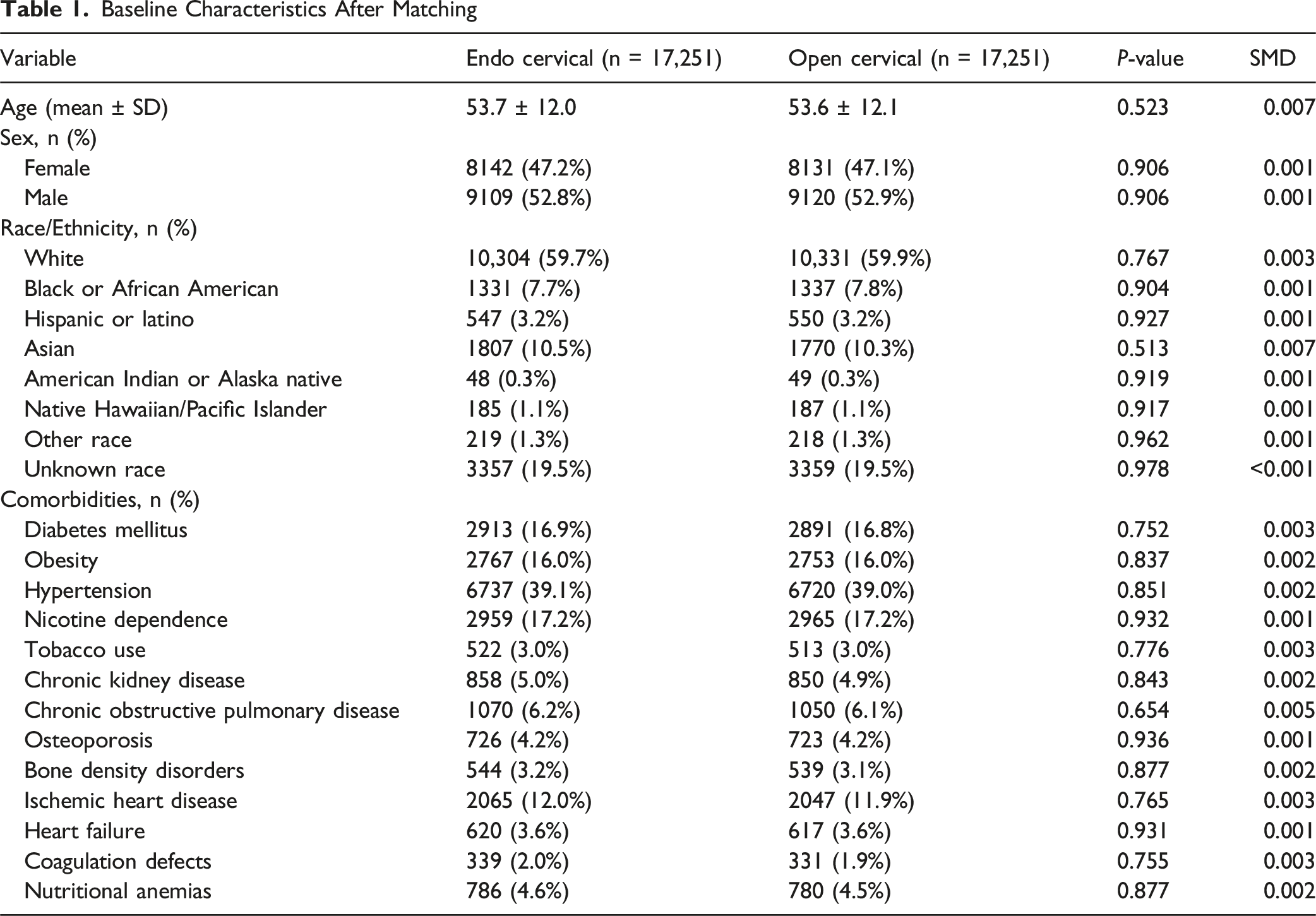
A total of 34 502 patients met eligibility criteria after propensity score matching, with 17 251 undergoing ECD and 17 251 undergoing open cervical decompression (Figure 1). Demographics and comorbidities were well balanced between groups (Table 1). The mean age was comparable across cohorts, and sex distribution was similar, with women representing a nearly identical proportion of each group. Race and ethnicity were also evenly distributed, with no meaningful differences between cohorts. The prevalence of major comorbidities was uniformly balanced after matching, confirming excellent covariate alignment (all SMD <0.1). Patient selection Diagram Baseline Characteristics After Matching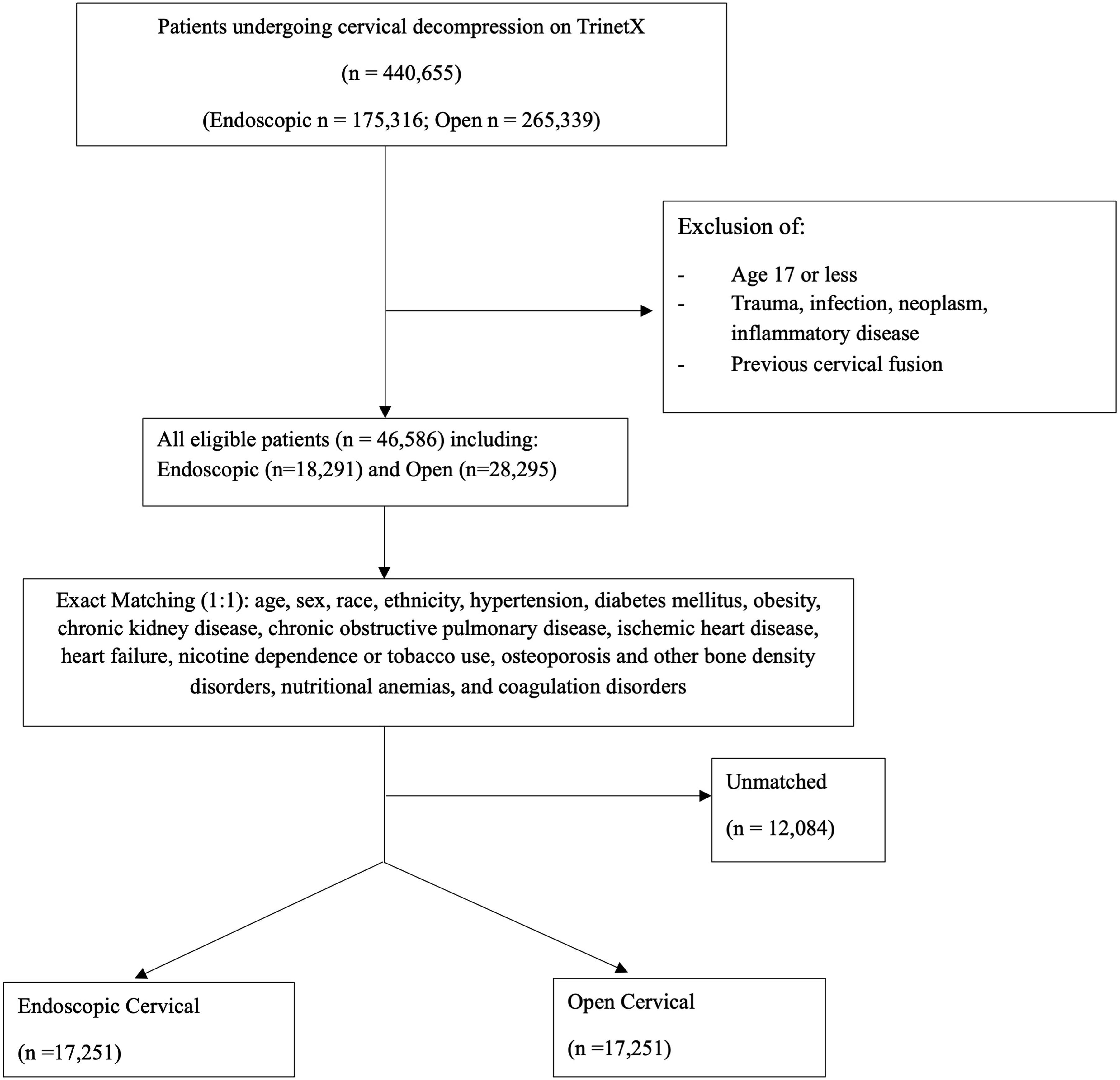
Postoperative Outcomes and Complications
Thirty Day Complications
Rate of Subsequent Cervical Fusion
Rates of Postoperative Cervical Fusion

Survival Analysis of Time to Subsequent Cervical Fusion
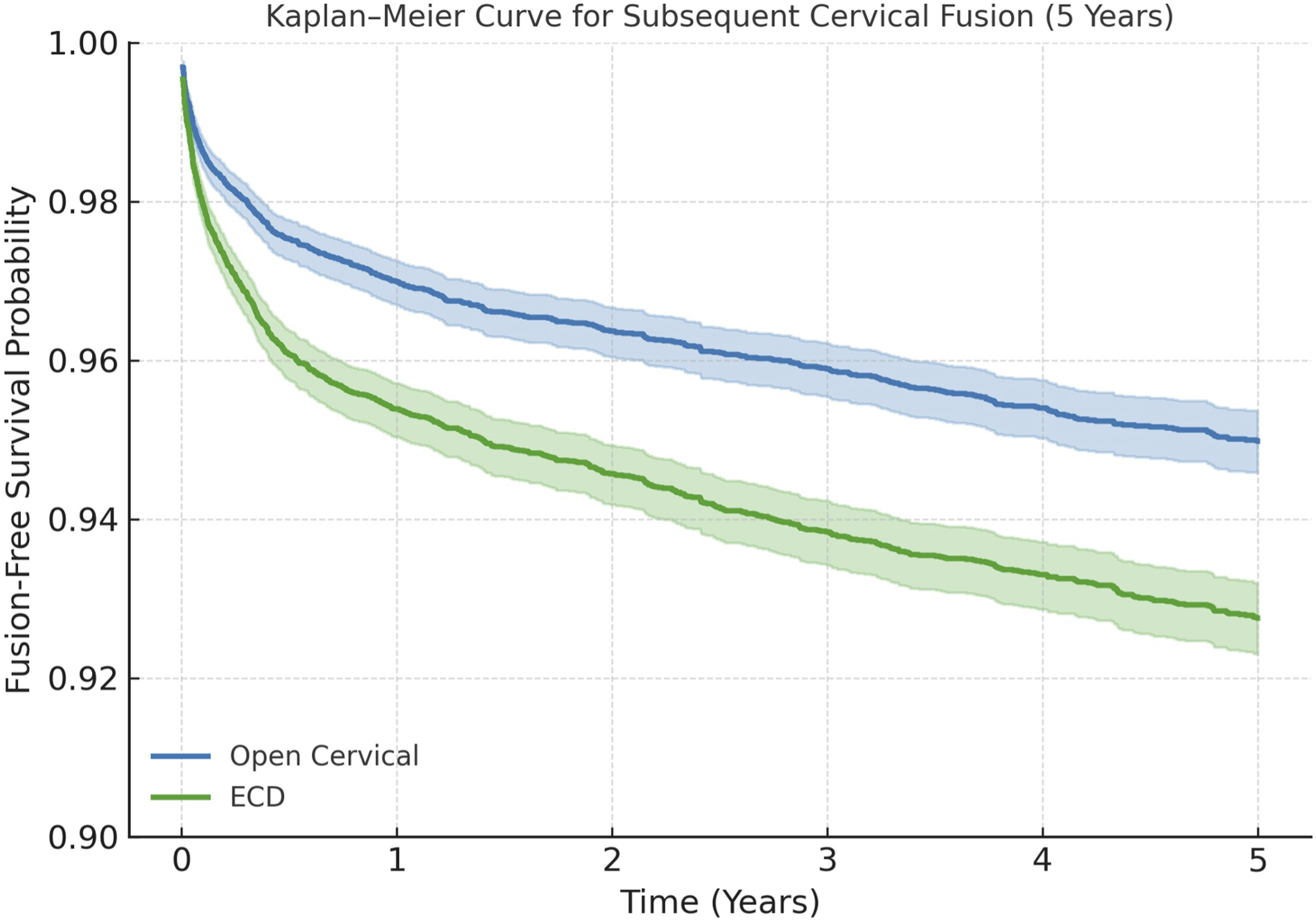
Kaplan–Meier survival analysis was performed to assess time to subsequent cervical fusion after ECD or open decompression. The 2-years Kaplan–Meier curve demonstrated a significantly higher hazard of conversion to fusion in the ECD cohort (HR 1.52, 95% CI 1.36-1.70; P < 0.001) (Figure 2). The 5-years Kaplan–Meier curve showed continued separation of the survival functions, with ECD maintaining a higher cumulative fusion incidence (HR 1.48, 95% CI 1.34-1.64; P < 0.001) (Figure 3). Across both timepoints, the open decompression cohort demonstrated more durable long-term stability, with higher survival probabilities at 2 years and 5 years. Most fusion events in both groups occurred within the first 24 postoperative months, consistent with the steepest decline in the survival curves occurring early in follow-up. Two year Kaplan-Meier curve Five year Kaplan-Meier curve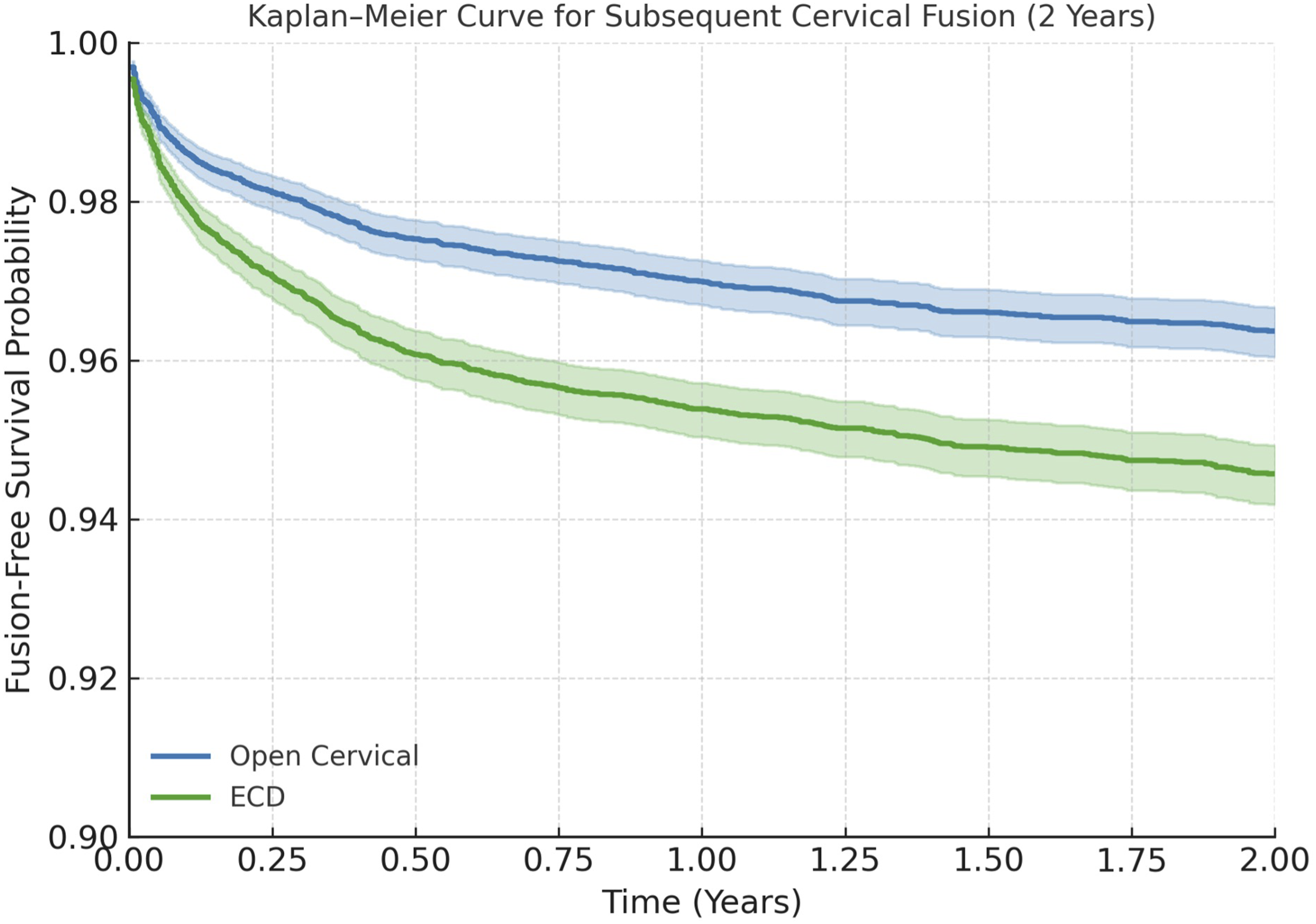
In a temporal sensitivity analysis restricted to the contemporary cohort (2021-2024), the association between ECD and subsequent cervical fusion remained directionally consistent at both 1 and 2 years. At 1 year, the hazard ratio was 1.41 (95% CI 0.76-2.60; P = 0.27), and at 2 years, the hazard ratio was 1.67 (95% CI 0.89-3.12; P = 0.127), although statistical significance was not reached.
Discussion
In this large comparative analysis, we found that ECD demonstrated short-term safety outcomes comparable to open posterior cervical decompression, while exhibiting a significantly lower rate of 30-days hospital readmission. Over extended follow-up, however, ECD was associated with a higher likelihood of conversion to cervical fusion between 1-5 years postoperatively. Taken together, these findings suggest a clinically meaningful trade-off in which the perioperative advantages of a minimally invasive endoscopic approach may be counterbalanced by diminished long-term structural durability in select patients.
The comparable 30-days medical and surgical complication profile observed between ECD and open posterior decompression are consistent with prior institutional series, prospective cohorts, and systematic reviews of endoscopic cervical procedures.2,3,12-16 From a biological and surgical perspective, these findings reflect the fundamental tissue-preserving principle of endoscopic surgery. ECD relies on percutaneous access, tubular dilation, and targeting bony decompression, allowing preservation of the posterior cervical musculature – including the semispinalis cervicis, multifidus, and interspinous stabilizers – as well as the posterior ligamentous complex and facet joint capsules.23-25 In contrast, open posterior approaches necessitate broader muscle detachment and prolonged retraction, which have been linked to muscle ischemia, denervation, postoperative axial neck pain, and delayed functional recovery.26,27 These biomechanical and anatomical differences likely underlie the significantly lower 30-days readmission rate observed in the ECD cohort. Reduced muscle trauma and inflammatory burden translate into less postoperative pain, lower opioid requirements, earlier mobilization, and faster return to baseline activity.12,15,28 Compared with ACDF, ECD also avoids anterior soft tissue manipulation, including esophageal retraction, sympathetic chain irritation, anterior approaches.1,24 Despite these advantages, ED utilization remained similar between groups, suggesting that while ECD reduces clinically significant postoperative issues necessitating inpatient readmission, minor postoperative concerns and reassurance-seeking behaviors may be comparable across surgical techniques. This pattern mirrors prior cervical and lumbar endoscopic literature and underscores that early healthcare utilization is influenced not only by surgical corridor but also by pain management protocols, outpatient access, and social support structures.20,25,28
In contrast, the higher long-term rate of conversion to cervical fusion following ECD represents a central finding of this study and highlights important biomechanical and anatomical considerations. This comparison should be interpreted with caution, as the open cohort likely includes a mix of posterior techniques such as laminoforaminotomy and laminectomy-type decompression. These procedures carry different biomechanical profiles, and the observed difference therefore reflects a composite reference rather than a single uniform approach. Although the relative increase in subsequent fusion was statistically significant, the absolute risk difference at 5 years was approximately 2%, and its clinical significance remains uncertain in the absence of patient-reported or functional outcomes. Understanding of this outcome requires nuance, as subsequent fusion is captured through administrative data. Rather than reflecting a uniform definition of treatment failure, conversion to fusion likely encompasses a spectrum of clinical scenarios, including progression of underlying degenerative pathology, staged surgical management, or cases in which patients may have been borderline fusion candidates at baseline but initially underwent decompression. Posterior decompression – whether open or endoscopic – alters load transmission across the cervical motion segment. 29 Biomechanical studies have demonstrated that posterior foraminotomy, particularly when facet resection exceeds critical thresholds, increases segmental motion, redistributes forces to the intervertebral disc, and accelerates degenerative progression.17,29-31 Although ECD is designed to be more focal, its constrained working corridor may lead to asymmetric facet violation or underrecognized destabilization in cases of severe foraminal stenosis or osteophytic encroachment.
Importantly, ECD does not address anterior column pathology. Progressive disc height loss, uncovertebral hypertrophy, and annular collapse – key contributors to foraminal narrowing and cervical radiculopathy – remain untreated.19,32 Loss of disc height reduces foraminal cross-sectional area and increases facet loading, predisposing patients to recurrent nerve compression and segmental instability that ultimately necessitates fusion.26,27 The temporal clustering of fusion events within the first two postoperative years observed in this study aligns with established timelines for biomechanical failure and degenerative progression following posterior cervical decompression.26,32 In this context, the cumulative fusion rates observed in the open decompression cohort are broadly consistent with prior posterior cervical foraminotomy series, supporting the external validity of the present findings.
Surgeon experience likely further modulates these long-term outcomes. Endoscopic cervical surgery has a well-documented learning curve, with outcomes strongly influenced by procedural volume, endoscopic orientation, and familiarity with specialized instruments.14,21,33,34 Extrapolating from the endoscopic lumbar spine – where similar visualization constraints and tool-specific challenges exist – limited experience has been associated with residual disc fragments, incomplete decompression, inadequate osteophyte removal, dural tears, and thermal injury from radiofrequency probes or high-speed burrs.33–37 In the cervical spine, these risks are magnified by narrower anatomical tolerances, proximity to the spinal cord and vertebral artery, and limited capacity to compensate for technical imprecision. Incomplete decompression or retained pathology may initially yield symptomatic improvement but predispose patients to early recurrence and eventual conversion to fusion. 38
In light of these considerations, a contemporary-era sensitivity analysis was performed to further evaluate the potential influence of temporal adoption and increasing surgeon experience. Restricting the cohort to procedures performed between 2021 and 2024, the magnitude of association between ECD and subsequent cervical fusion remained directionally consistent with the primary analysis at both 1 and 2 years, although statistical significance was not retained. This pattern suggests that the observed increase in reoperation risk is unlikely to be solely attributable to early learning curve effects and may instead reflect underlying differences in patient selection, biomechanics, or the inherent limitations of decompression without fusion. However, these estimates were imprecise, with confidence intervals crossing unity at both timepoints. This pattern may reflect limited statistical power within the contemporary cohort, but it may also indicate a reduction in the magnitude of effect as endoscopic techniques and surgeon experience have evolved. In this context, the contemporary analysis is best viewed as exploratory rather than definitive and does not exclude the possibility of a more attenuated association in current practice.
Selection bias and unmeasured anatomical complexity likely also contribute to the observed differences in long-term durability. Patients undergoing ECD may represent a distinct subset with more advanced foraminal stenosis, facet arthropathy, multilevel disease, or early disc collapse – features not fully captured within administrative coding frameworks.18,19,32 Although propensity matching achieved balance across demographic and comorbidity variables, key radiographic parameters such as sagittal alignment, disc height, foraminal morphology, and dynamic instability were unavailable and could not be controlled for. Additionally, patient-reported outcomes were not captured, limiting assessment of whether subsequent fusion reflects symptomatic failure, progressive structural instability, or elective stabilization. As such, these findings should be interpreted as hypothesis-generating and underscore the need for prospective, imaging-based studies to better define optimal patient selection and long-term outcomes following ECD.
Collectively, these findings indicate that while ECD offers meaningful perioperative benefits – including reduced early healthcare utilization – it may confer a higher long-term likelihood of conversion to fusion compared with open posterior decompression. From a clinical standpoint, this underscores the importance of meticulous patient selection, careful assessment of disc height and facet integrity, and transparent preoperative counseling regarding long-term durability. For surgeons, the results emphasize the need for technical precision, recognition of endoscopic limitations, and cautious adoption during early learning phases. In practice, ECD should be viewed not as a replacement for traditional techniques but as a complementary option whose advantages are maximized when matched appropriately to patient anatomy, pathology, and surgeon experience. Importantly, these findings should be interpreted within the context of an evolving adoption period for endoscopic cervical techniques and may change as surgeon experience increases and training becomes more standardized. As endoscopic technology and training continue to evolve, future prospective studies incorporating imaging-based selection criteria and surgeon level data will be essential to determine whether these long-term differences persist as techniques mature.12,24,39
Limitations
This study has several limitations inherent to its retrospective design and reliance on electronic health record data. Despite rigorous propensity score matching, residual confounding from unmeasured variables – including surgeon experience, extent of decompression, facet resection, disc height loss, and cervical alignment - cannot be excluded. Additionally, the ICD-10-PCS codes used to define endoscopic decompression are approach-based and identify percutaneous endoscopic procedures involving cervical vertebral elements but do not distinguish between specific endoscopic techniques or procedural nuances. As such, these codes may capture a broader spectrum of minimally invasive approaches beyond strictly full-endoscopic or biportal decompression. Although cohort definition was restricted to degenerative cervical pathology to improve specificity, some degree of procedural misclassification remains possible. Importantly, any misclassification would likely bias results toward the null rather than inflate differences between cohorts.
Similarly, the open decompression cohort likely represents a heterogeneous group of posterior decompressive techniques, including laminoforaminotomy, laminectomy-type decompression, and nerve root release procedures, which differ in biomechanical impact and potential for subsequent instability. The ICD-10-PCS codes used do not allow reliable differentiation between these techniques, limiting the ability to perform technique-specific analyses. Although all included procedures represent non-fusion posterior decompression, this heterogeneity may influence long-term fusion risk. Procedural coding also does not capture operative nuances such as incomplete decompression, residual fragments, or intraoperative cerebrospinal fluid leaks, all of which may influence long-term outcomes.17,19
Furthermore, surgeon – and institution-level factors – including case volume, endoscopic equipment, and postoperative care pathways – were unavailable and may meaningfully impact outcomes, particularly given the steep learning curve associated with endoscopic cervical procedures.14,21 Although a contemporary-era sensitivity analysis was performed to account for temporal adoption and increasing experience, this approach remains an indirect proxy for surgeon proficiency. Variability in surgeon training, case volume, and institutional experience likely persists even within the contemporary cohort and may continue to influence both technical execution and long-term outcomes. Furthermore, the database does not allow stratification by surgeon experience or procedural volume, precluding direct assessment of learning curve effects over time.
Differences in underlying pathology, including the relative contribution of disc herniation vs foraminal stenosis, may influence both surgical approach selection and long-term outcomes and could not be reliably distinguished within the database. As such, residual confounding by indication may persist despite matching. Selection bias related to unmeasured anatomical complexity may also influence outcomes, as detailed radiographic parameters, including sagittal alignment, disc height, and foraminal morphology, were not available and could not be controlled for. Follow-up duration varied across institutions, and fusion procedures performed outside participating systems may not have been captured, potentially underestimating long-term preoperative rates. Finally, patient-reported outcomes, functional recovery metrics, and radiographic parameters were not available, limiting assessment of symptom resolution and structural progression. Despite these limitations, this study leverages one of the largest comparative international cohorts of ECD and open decompression to date and provides meaningful insight into both the short-term safety and long-term structural durability of contemporary cervical decompression techniques.
Conclusion
Endoscopic cervical decompression offers comparable 30-days medical and surgical safety to traditional open posterior cervical decompression and is associated with reduced early hospital readmission, reinforcing its utility as a minimally invasive treatment option for degenerative cervical pathology. However, ECD demonstrates a higher long-term risk of conversion to cervical fusion, suggesting that while effective in the short term, its long-term structural durability may be limited in certain patient populations. These findings highlight the importance of individualized surgical planning and comprehensive patient counseling regarding both the benefits and long-term expectations of endoscopic cervical spine surgery.
Supplemental Material
Supplemental material - Long-Term Risk of Subsequent Cervical Fusion after Endoscopic versus Open Cervical Decompression
Supplemental material for Long-Term Risk of Subsequent Cervical Fusion after Endoscopic versus Open Cervical Decompression by Ryan Wang, Mohammed Rasheed, William Zeng, Alexander T. Hong, Hannah Cho, Syed I. Khalid, Ankit I. Mehta in Global Spine Journal
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.