
Abstract
Study Design
Systematic review.
Objective
The current literature suggests that decompression-only procedures may be an adequate treatment option for low-grade degenerative spondylolisthesis. It is necessary to understand the causes of the failure to adequately select patients to achieve acceptable results. Our aim is to identify factors associated with failure of decompression-only procedures for degenerative lumbar spondylolisthesis.
Methods
An independent systematic review of scientific databases (PubMed, Scopus, clinicaltrials. gov, Web of Science) was performed to identify relevant articles as per the preferred reporting in systematic reviews and meta-analysis (PRISMA) guidelines. Studies analysing the risk factors for failure following decompression-only procedure for degenerative lumbar spondylolisthesis were included. The pooled analysis was performed using the Stata software.
Results
Six studies were included with the baseline characteristics of the successful group and the failed group. Individual study analysis has found factors like motion at index level, and multi-level decompression to be responsible for failure. However, upon pooled analysis patient-related factors (age, sex, BMI), disease-related factors (Pfirrmann grade, slip distance, disc height, facet angulation, translation, movement at index level, sacral slope), and outcome parameters (VAS, ODI and JOA score) between the two groups did not demonstrate any significant difference.
Conclusion
High-quality evidence analysing the risk factors for failure of decompression-only procedure for degenerative spondylolisthesis is limited. Although factors such as motion at index level, and multi-level decompression were found to be potential risk factors in individual studies, pooled analysis did not find any of them to significantly predict failure of decompression-only procedures for degenerative spondylolisthesis.
Introduction
The clinical guidelines of the North American Spine Society suggest decompression-only procedure for low-grade (<20%) symptomatic degenerative spondylolisthesis without foraminal stenosis. 1 The main intention of the procedure is to provide adequate pain relief by decompressing neural structures. The advantages of decompression only procedures compared to decompression followed by fusion procedures are lower blood loss, length of stay, and length of surgical procedure.2,3 It has been argued that in patients with stable degenerative spondylolisthesis, decompression alone may be sufficient to achieve adequate results.1,2,4 This is especially true for elderly patients due to the lower associated morbidity and mortality. 5 A higher incidence of major complications has been observed for fusion procedures in the elderly. 6 Furthermore, selection of patients who would benefit the most from decompression-only procedures avoids potential fusion-related complications such as cage subsidence and additional secondary surgeries such as hardware removal or adjacent lumbar level surgery.5,7,8
The main disadvantage is the concern about the lack of long-term stability that can be achieved with fusion procedures. In some patients, decompression-only procedure can lead to altered spine biomechanics and iatrogenic spondylolisthesis resulting in instability that warrants revision surgery. Taking the progressive degeneration cascade into account, the decompression-only procedure, although providing initial pain relief, may not be able to address the core cause of pain, as evidenced by the higher reported reoperation rates. Other disadvantages include the inability to address certain clinical entities such as foraminal stenosis secondary to loss of disc height. 9 It could also be argued that the decompression-only procedure is unable to restore sagittal balance, which may influence patient-related outcomes. 9
Reported failure rates vary in literature from 0% to 37.5%.2,3,6,8,10 Large differences in reported reoperation rates could be attributed to variations in surgical technique when performing decompression. Inose et al 2 observed different reoperation rates for patients in the decompression-only group, when compared to the Ghogawala et al 3 trial (0% vs 34%). They argued that the disparity could arise from the operative procedure (wide fenestration-removal of only the medial parts of the inferior facets and the adjoining ligamentum vs complete laminectomy with partial removal of the medial facet joint).2,3 A recent meta-analysis of 20 studies comparing decompression to decompression with fusion found higher reoperation rates in the decompression cohort compared to the fusion cohort (8.5% and 4.9% respectively). On the contrary, the fusion cohort had a complication rate of 8.3% compared to the 5.8% rate in the decompression-only cohort. 11
There are several previously reported factors associated with failure. These include the extent of facetectomy, the number of decompressed levels and compromise of posterior ligamentous structures.12,13 These risk factors appear to be related to the decrease in the ability to withstand forces acting on the spinal column. The intervertebral disc and facet joints provide resistance to shear stress. The posterior ligamentous complex balances the flexion and extension forces by keeping the posterior elements of the adjacent vertebrae in stable relation to each other. Any alterations in their biomechanics could also result in instability and subsequent failure of the decompression-only procedure for spondylolisthesis. 14
The current literature suggests that decompression-only procedures may be an adequate treatment option for low-grade degenerative spondylolisthesis. It is necessary to understand the causes of the failure to adequately select patients to achieve acceptable results.
The aim of this study is to identify the key factors associated with potential failure of decompression-only procedures for degenerative lumbar spondylolisthesis.
Methods
The present systematic review was conducted according to the preferred reporting in systematic reviews and meta-analysis (PRISMA) guidelines. 15 The protocol of the study was registered in the prospective registry for systematic reviews (PROSPERO) before the start of the study (CRD42022353300).
Literature Search
Two individual researchers (S.M., S.C.) independently reviewed four scientific databases (PubMed, Scopus, clinicaltrials.gov, Web of Science) to identify relevant articles. The algorithms used for the literature search included the following keywords: “decompression”, “spondylolisthesis”, “laminectomy”, “laminotomy”, “degenerative”, and “surgical management”. Appropriate adjustments to the algorithms were made for each of the databases using Boolean operators such as “AND”, “OR” and “NOT”. The algorithms used in the included databases are presented in Online Appendix 1. The bibliographies of the identified studies were also reviewed for the identification of additional relevant studies. Any conflicts were resolved by consulting a third researcher (ZB).
Eligibility Criteria
Following the removal of duplicates, the titles and abstracts of the identified studies were reviewed for relevance using the online platform www.rayyan.ai/. The full texts of the potential relevant studies were then examined against our inclusion criteria. Studies that fulfilled the following inclusion criteria were included in the systematic review:
Patient
Adult patients (18 years old or older) with a lumbar degenerative spondylolisthesis.
Intervention
Patients with failed decompression only procedure necessitating revision surgery.
Comparison
Patients with successful decompression only procedure.
Outcome
Baseline characteristics of the two groups.
Study Types
Prospective and retrospective studies with at least 10 patients per study group.
Any study that analysed the failed and successful cases undergoing decompression-only procedure for degenerative spondylolisthesis for recurrence of symptoms that required reoperation is considered for inclusion.
Exclusion Criteria
We excluded observational studies with less than 10 patients, study types such as case reports, letters to the editor, brief reports, conference abstracts, and studies including patients with tumours, infections, spinal cord injuries, trauma/fractures, degenerative scoliosis, skeletal immaturity, patients younger than 18 years old, studies involving decompression only procedure without clear distinction between failed and successful group and having their baseline parameters individually listed.
Data Extraction
Using an Excel form, the authors independently extracted the following data from the studies, if available:
Study Characteristics
Name of the first author, year of publication, type of study, number of participants in each group
Patient Characteristics
Age, gender, body mass index (BMI), spondylolisthesis grade, American Society of Anesthesiology (ASA) grading
Procedure Characteristics
Approach and levels of surgery
Baseline Parameters
Degree of slip, Pfirrmann score of disc degeneration, Oswestry disability index (ODI), Visual Analog Score (VAS), Japanese Orthopaedic Association (JOA) score, disc height, facet angle, translation, angulation, movement at the index level, sagittal rotation and spino-pelvic parameters like sacral slope.
Any discrepancies between the reviewers were resolved by a third investigator (ZB).
Quality Assessment
Quality assessment was performed using the ROB2 tool of Cochrane Collaboration for RCTs with five domains of assessment and the ROBINS tool for non-randomized studies that have seven domains of assessment. The quality assessment was performed independently by two investigators (S.M., S.C.). Any discrepancy was resolved upon discussion with the third investigator (Z.B.).
Statistical Analysis
All statistical calculations were performed using Stata (Version 17, Stata Corp LLC) for Windows. The weighted mean difference (WMD) for continuous variables and odds ratio (OR) for event-related discrete variables with a 95% Confidence Interval (CI) was calculated. The random effects meta-analysis model was used for data synthesis when the heterogeneity of the studies was high (I2>50% and P < 0.10), otherwise the fixed-effects model was implemented. Sensitivity and subgroup analysis was performed if heterogeneity was noted among the reported results. Egger’s regression test was performed to analyse publication bias.
Results
Study Characteristics
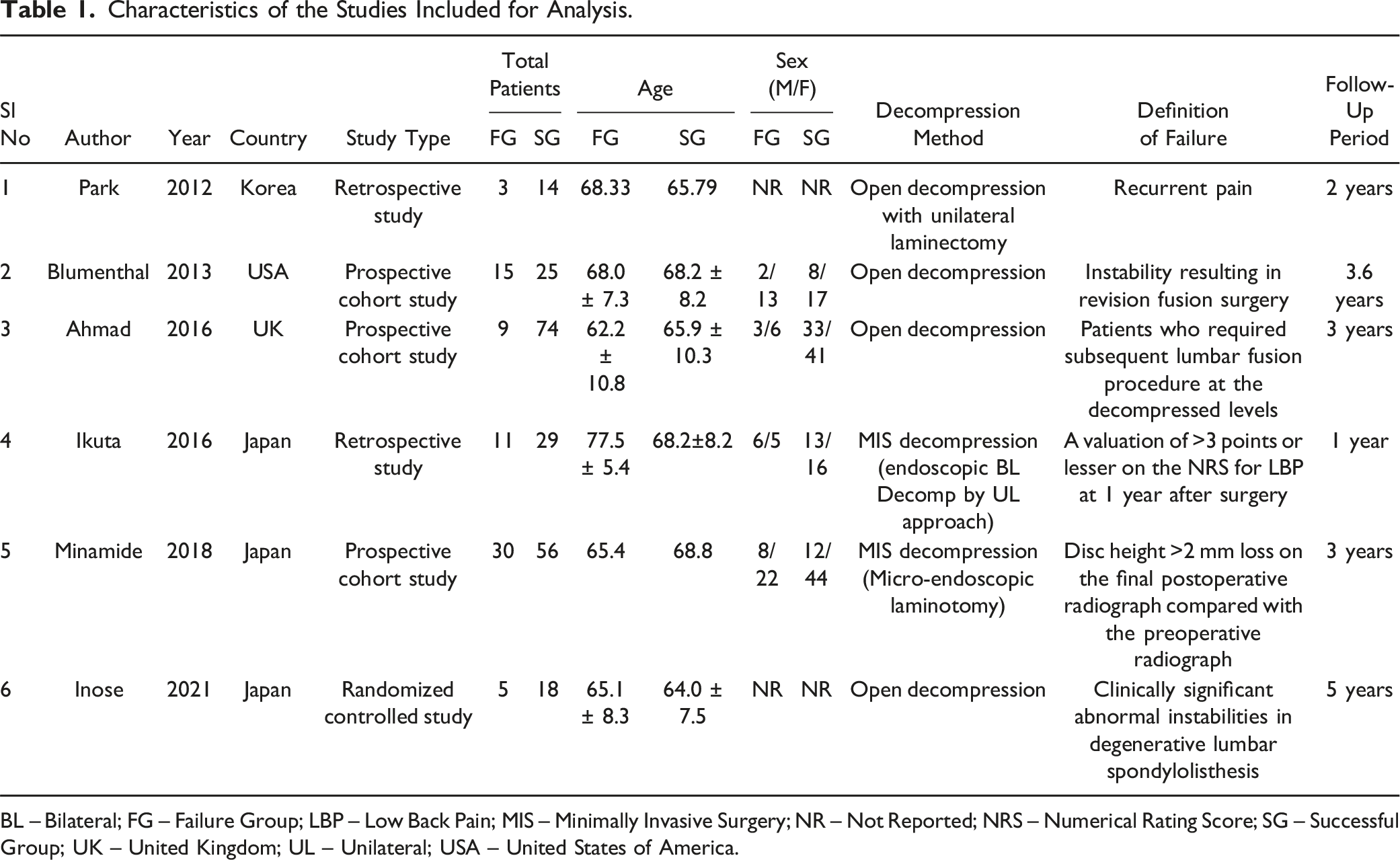
Following duplicate removal, 1560 studies were identified from the included databases and screened for inclusion. After an initial screening of titles and abstracts, 1432 studies were excluded. The full texts of the 128 remaining studies were then examined against our inclusion criteria, leading to the inclusion of six studies9,14,16-19 incorporating 289 patients with clear distinction between the failed and successful patients with baseline characteristics made available for analysis. The reason for the exclusion of studies from the full-text screening is presented in the PRISMA flow diagram in Figure 1. The characteristics of the included studies are presented in Table 1 and that include: one is a randomized controlled trial,
19
three prospective cohort studies,14,16,18 and two retrospective cohort studies.9,17 While four studies9,14,16,19 employed open decompression method, only two studies17,18 utilized minimally invasive decompression method. The definition of failure assigned to the failure group include recurrent pain in two studies,9,17 instability resulting in revision surgery in three studies,14,16,19 and loss of disc height in one study.
18
PRISMA flow diagram of inclusion of studies into the analysis. Characteristics of the Studies Included for Analysis. BL – Bilateral; FG – Failure Group; LBP – Low Back Pain; MIS – Minimally Invasive Surgery; NR – Not Reported; NRS – Numerical Rating Score; SG – Successful Group; UK – United Kingdom; UL – Unilateral; USA – United States of America.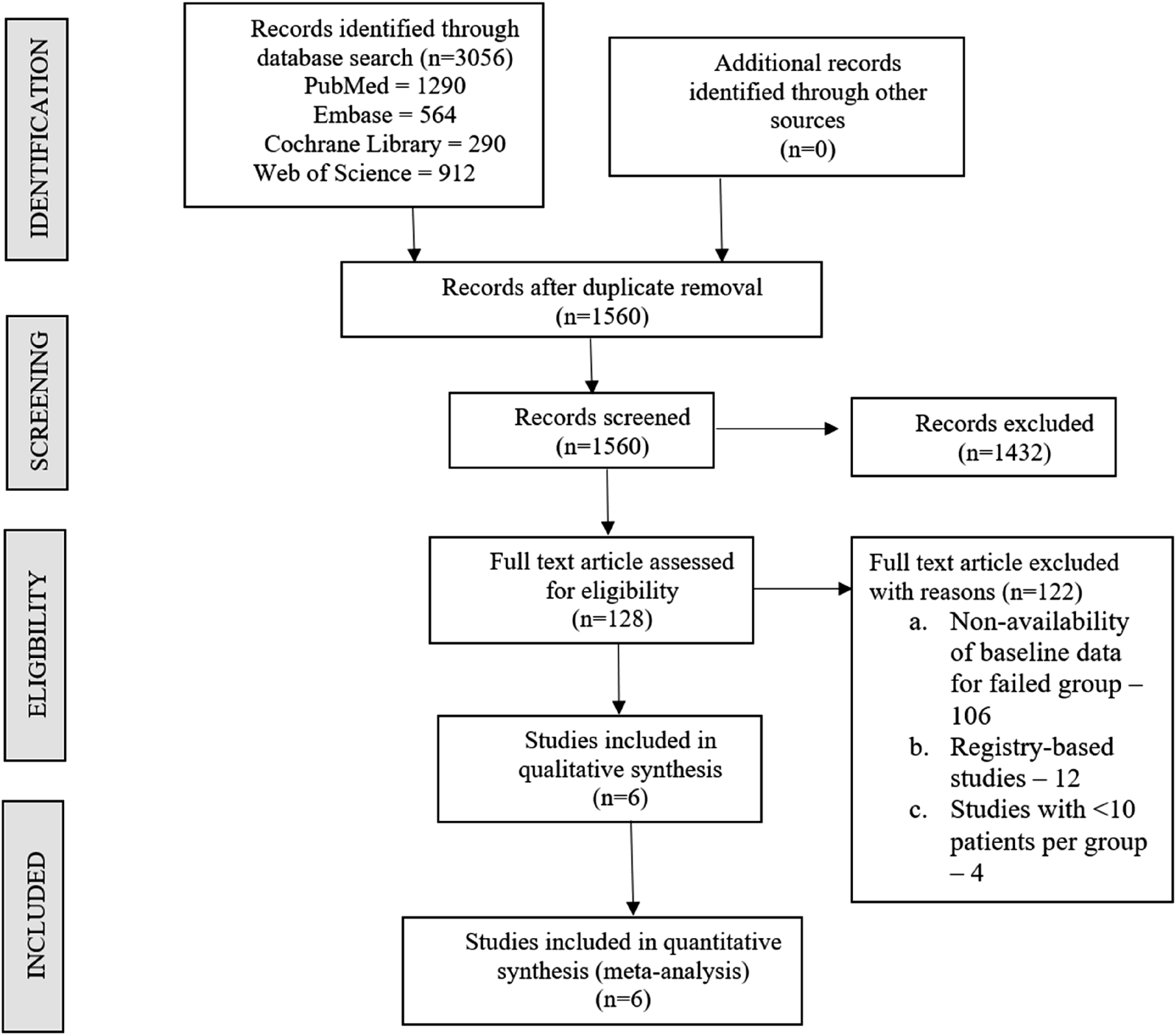
Risk of Bias Assessment
None of the studies had high risk of bias to warrant exclusion from the analysis as shown in Figure 2. Of all the included studies, only two studies scored some concerns in their overall ROBINS assessment for its risk of bias while rest of all studies scored low concerns. Lack of complete data on baseline characteristics were the domains at fault in those two studies. Risk of bias assessment in the included studies using Cochrane Collaboration’s ROB2 for randomized and ROBINS tool for non-randomized studies respectively.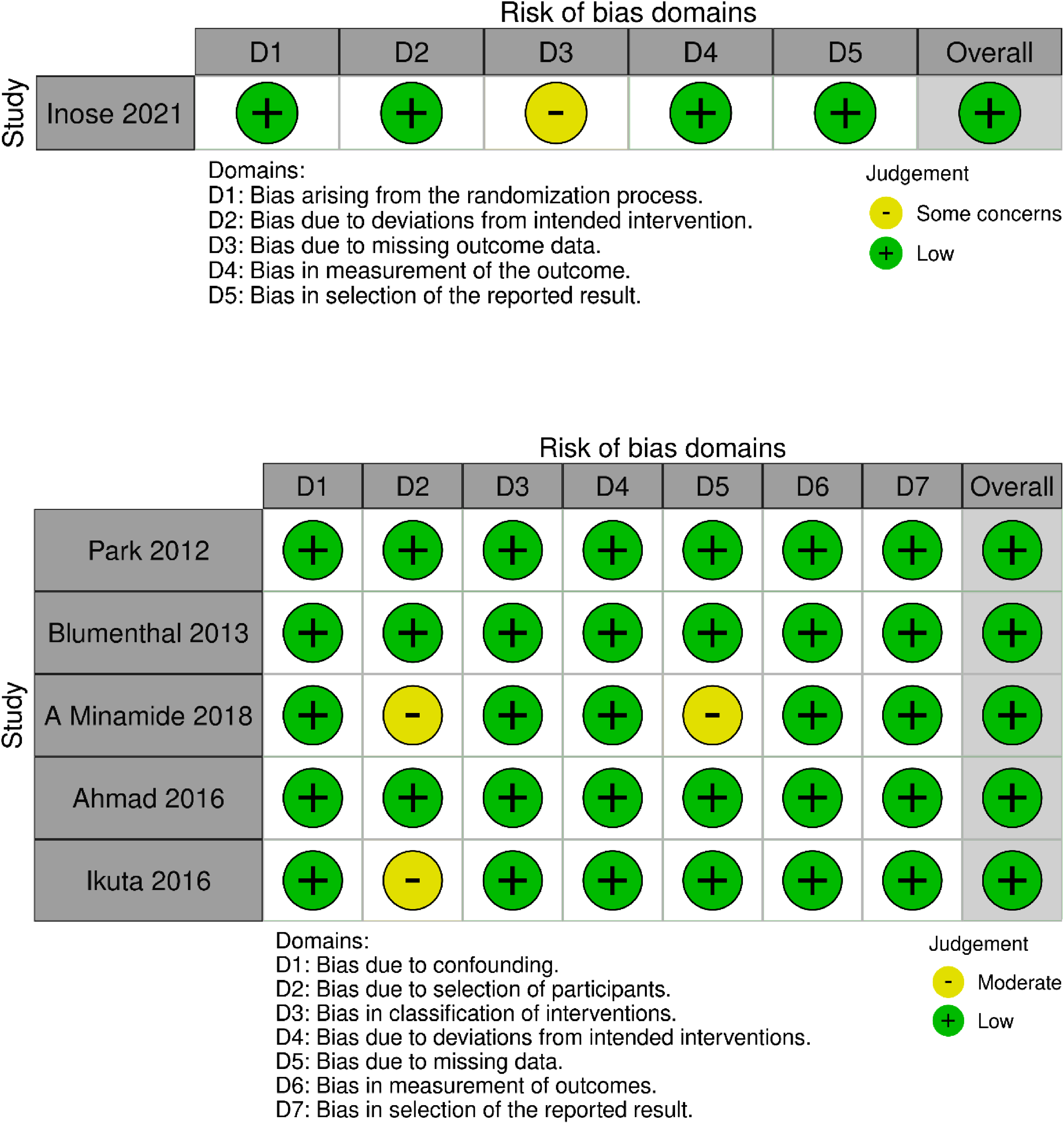
Patient-Related Factors
Age
We analyzed six studies9,14,16-19 with 289 patients with individual age group data for the failed and successful group undergoing decompression-only procedure. Significant heterogeneity was noted among the included studies (I2 = 73.58%, P < 0.01). Hence, a random-effects model was used for analysis. No significant difference was noted between the two groups with regards to age with WMD = 0.08 (95% CI [−0.49, 0.65], P = 0.80) as shown in Figure 3. Forest plot comparing the patient-related factors such as age, sex, and body-mass index between the failed group and the successful group undergoing decompression-only procedure for degenerative spondylolisthesis.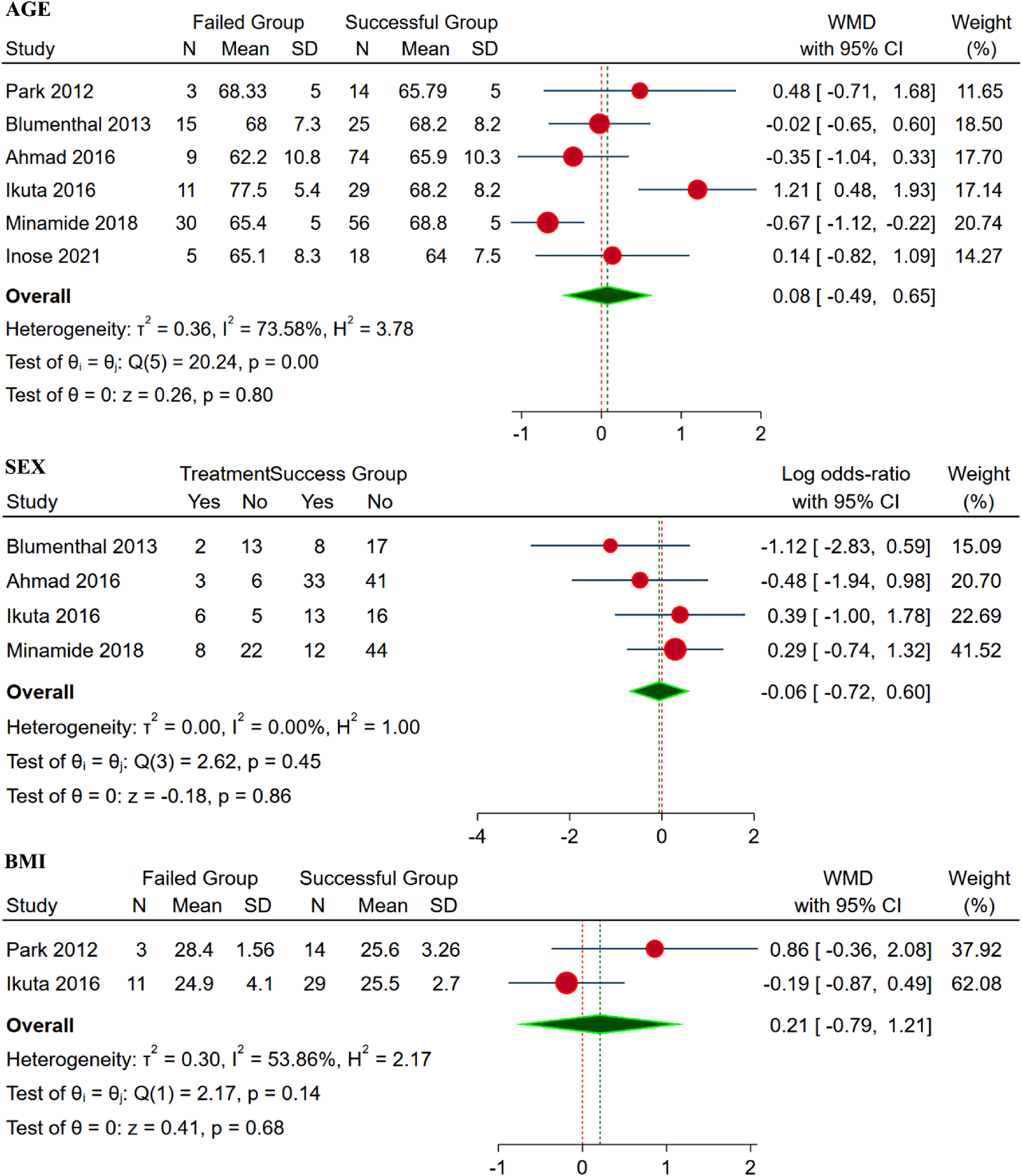
Sex
We analyzed four studies14,16-18 with 249 patients with individual gender data for the failed and successful group undergoing decompression-only procedure. No significant heterogeneity was noted among the included studies (I2 = 0%, P = 0.45). Hence, a fixed-effects model was used for analysis. No significant difference was noted between the two groups with regards to sex with WMD = −0.06 (95% CI [−0.72, 0.65], P = 0.80) as shown in Figure 3.
BMI
We analyzed two studies9,17 with 57 patients with individual BMI for the failed and successful group undergoing decompression-only procedure. No significant heterogeneity was noted among the included studies (I2 = 53.86%, P = 0.14). Hence, a fixed-effects model was used for analysis. No significant difference was noted between the two groups with regards to BMI with WMD = 0.21 (95% CI [-0.79, 1.21], P = 0.68) as shown in Figure 3.
Disease-Related Factors
Slip Distance
We analyzed five studies9,14,16,18,19 with 249 patients with individual slip distance for the failed and successful group undergoing decompression-only procedure. No significant heterogeneity was noted among the included studies (I2 = 0%, P = 0.74). Hence, a fixed-effects model was used for analysis. No significant difference was noted between the two groups with regards to slip distance with WMD = 0.17 (95% CI [−0.12, 0.46], P = 0.26) as shown in Figure 4. Forest plot comparing the disease-related factors such as slip distance, Pfirrmann grade of disc, and disc height between the failed group and the successful group undergoing decompression-only procedure for degenerative spondylolisthesis.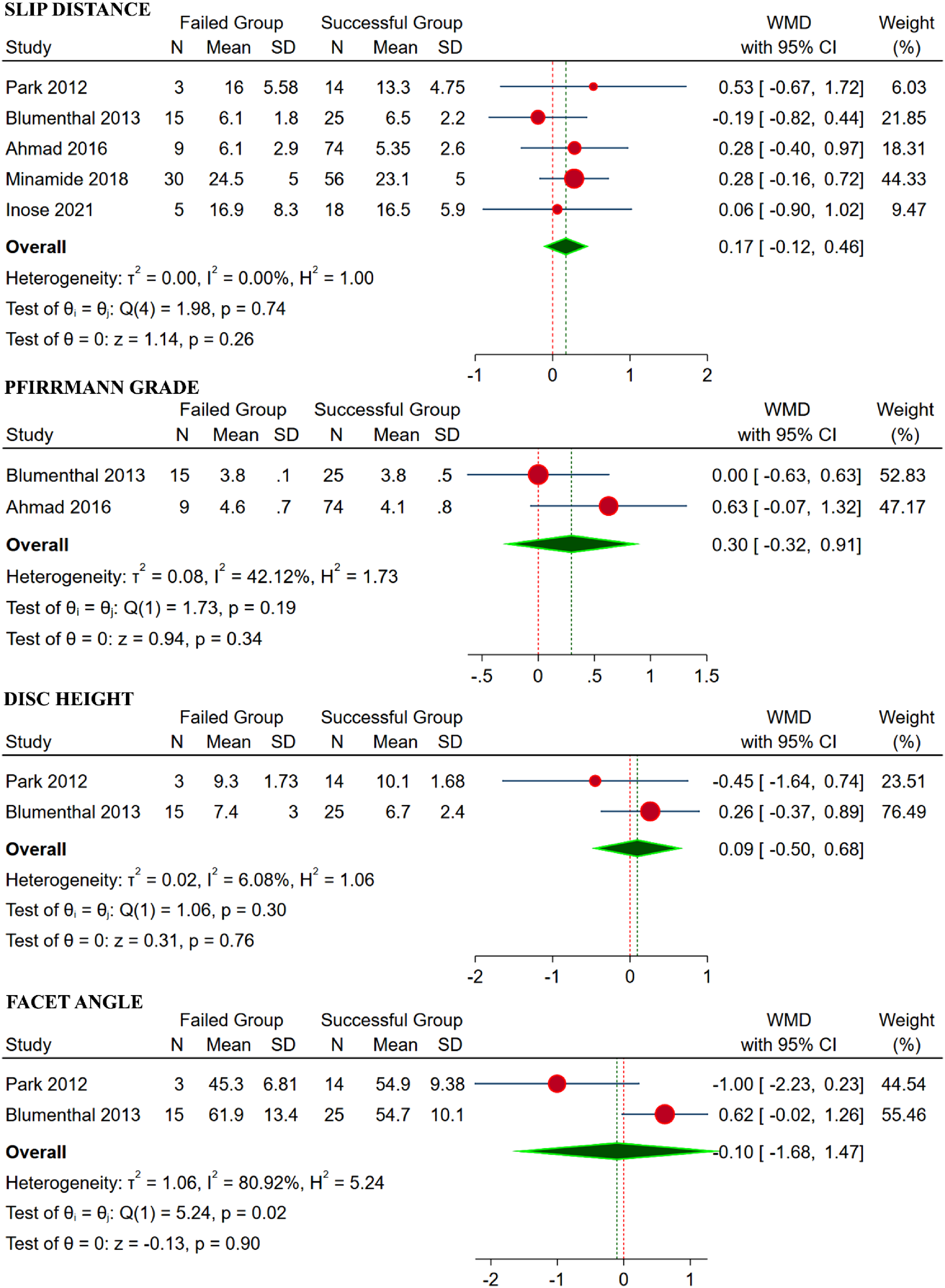
Pfirrmann Grade
We analyzed 2 studies14,16 with 123 patients with individual Pfirrmann grades for the failed and successful group undergoing decompression-only procedure. No significant heterogeneity was noted among the included studies (I2 = 42.12%, P = 0.19). Hence, fixed-effects model was used for analysis. No significant difference was noted between the two groups with regards to Pfirrmann grade with WMD = 0.30 (95% CI [−0.32, 0.91], P = 0.34) as shown in Figure 4.
Disc Height
We analyzed two studies9,14 with 57 patients with individual disc height for the failed and successful group undergoing decompression-only procedure. No significant heterogeneity was noted among the included studies (I2 = 6.08%, P = 0.30). Hence, a fixed-effects model was used for analysis. No significant difference was noted between the two groups with regards to disc height with WMD = 0.09 (95% CI [−0.50, 0.68], P = 0.76) as shown in Figure 4.
Facet Angle
We analyzed two studies9,14 with 57 patients with individual facet angle for the failed and successful group undergoing decompression-only procedure. No significant heterogeneity was noted among the included studies (I2 = 6.08%, P = 0.30). Hence, a fixed-effects model was used for analysis. No significant difference was noted between the two groups with regards to facet angle with WMD = 0.10 (95% CI [−1.68, 1.47], P = 0.90) as shown in Figure 4.
Translation
We analyzed two studies9,17 with 57 patients with individual data regarding sagittal translation for the failed and successful group undergoing decompression-only procedure. No significant heterogeneity was noted among the included studies (I2 = 0%, P = 0.92). Hence, a fixed-effects model was used for analysis. No significant difference was noted between the two groups with regards to translation with WMD = −0.35 (95% CI [−0.95, 0.24], P = 0.24) as shown in Figure 5. Forest plot comparing the disease-related factors such as translation, movement at index level, and sacral slope between the failed group and the successful group undergoing decompression-only procedure for degenerative spondylolisthesis.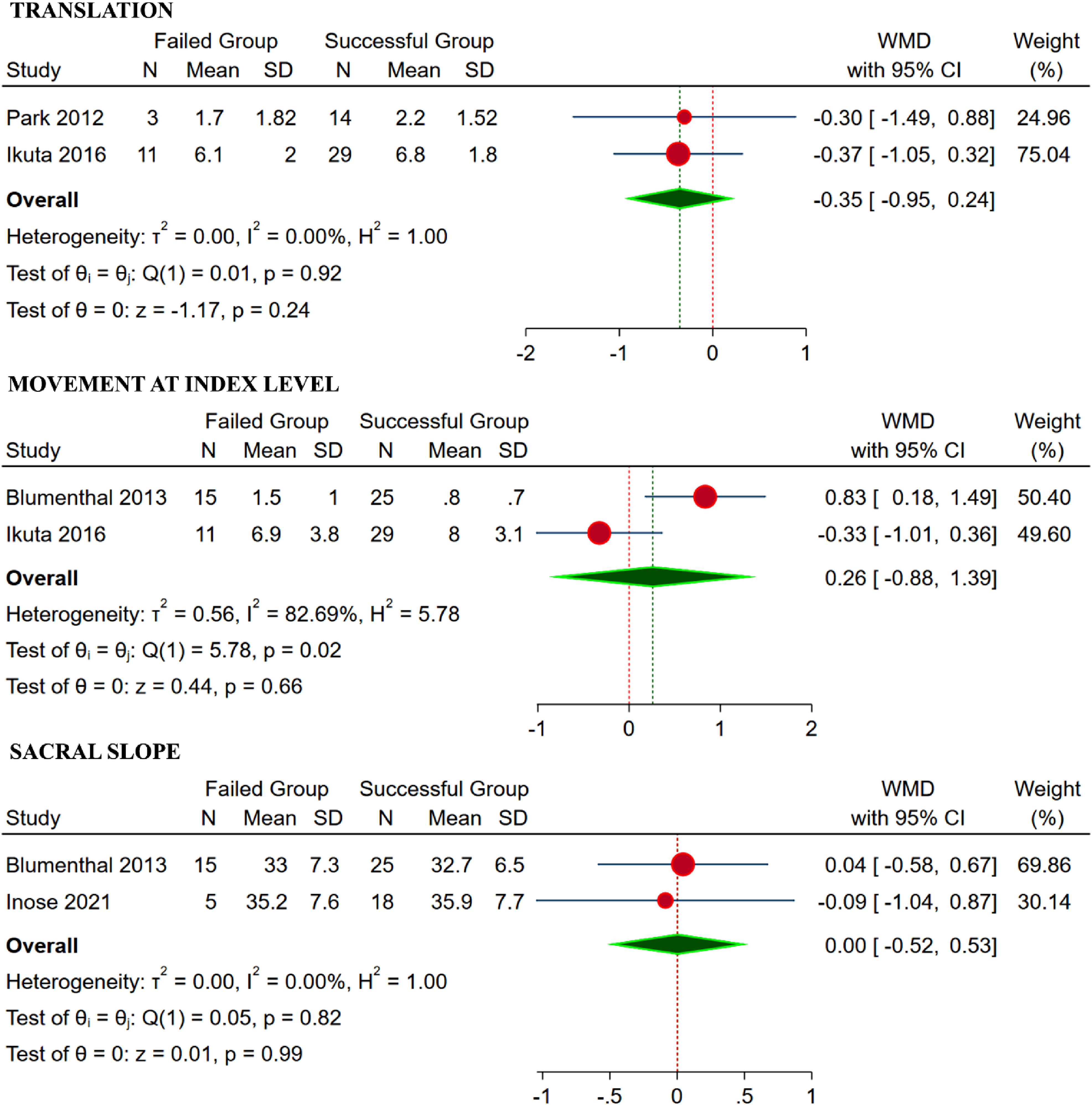
Movement at Index Level
We analyzed two studies14,17 with 80 patients with individual movement data for the failed and successful group undergoing decompression-only procedure. Significant heterogeneity was noted among the included studies (I2 = 82.69%, P < 0.01). Hence, a random-effects model was used for analysis. No significant difference was noted between the two groups with regards to movement with WMD = 0.26 (95% CI [−0.88, 1.39], P = 0.66) as shown in Figure 5.
Sacral Slope
We analyzed two studies14,19 with 63 patients with individual sacral slope for the failed and successful group undergoing decompression-only procedure. Significant heterogeneity was noted among the included studies (I2 = 0%, P = 0.82). Hence, fixed-effects model was used for analysis. No significant difference was noted between the two groups with regards to sacral slope with WMD = 0.00 (95% CI [−0.52, 0.53], P = 0.99) as shown in Figure 5.
Outcome Parameters
VAS Score
We analyzed four studies16-19 with 232 patients with individual VAS score data for the failed and successful group undergoing decompression-only procedure. Significant heterogeneity was noted among the included studies (I2 = 94.13%, P < 0.01). Hence, a random-effects model was used for analysis. No significant difference was noted between the two groups with regards to VAS with WMD = 0.95 (95% CI [−0.54, 2.44], P = 0.21) as shown in Figure 6. Forest plot analysing the VAS, ODI and JOA score between the failed and successful group undergoing decompression-only procedure for degenerative lumbar spondylolisthesis.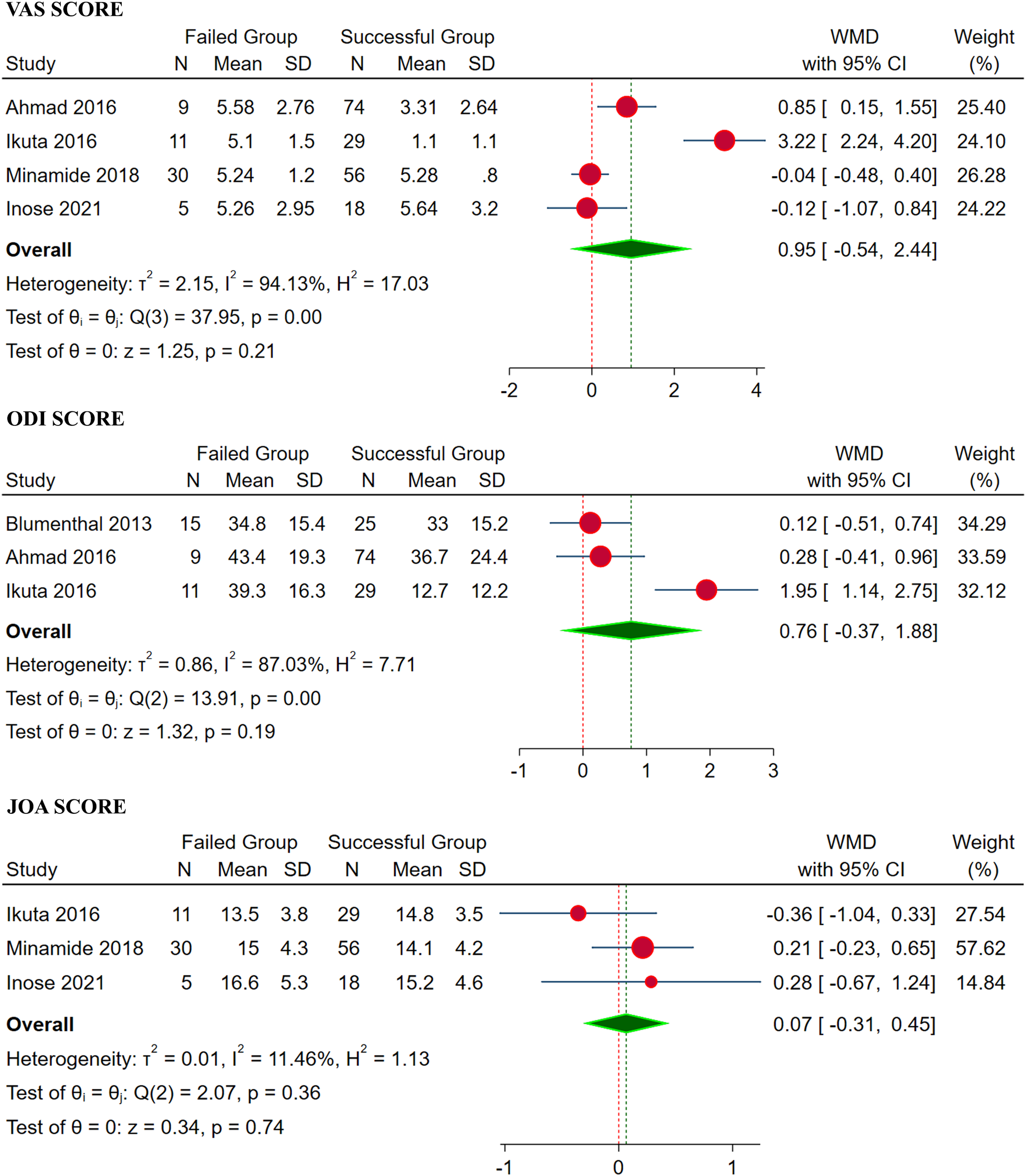
ODI Score
We analyzed three studies14,16,17 with 163 patients with individual ODI score data for the failed and successful group undergoing decompression-only procedure. Significant heterogeneity was noted among the included studies (I2 = 87.03%, P < 0.01). Hence, a random-effects model was used for analysis. No significant difference was noted between the two groups with regards to ODI with WMD = 0.76 (95% CI [−0.37, 1.88], P = 0.19) as shown in Figure 6.
JOA Score
We analyzed three studies17-19 with 149 patients with individual JOA score data for the failed and successful group undergoing decompression-only procedure. No significant heterogeneity was noted among the included studies (I2 = 11.46%, P = 0.36). Hence, a fixed-effects model was used for analysis. No significant difference was noted between the two groups with regards to JOA score with WMD = 0.07 (95% CI [−0.31, 0.45], P = 0.74) as shown in Figure 6.
Sensitivity Analysis
In order to further explore into the heterogeneity noted in the included studies in some of the outcomes, a sensitivity analysis was performed to understand the impact of individual studies on the overall estimate. We did not find a single study to significantly modify the final estimate through a leave-one-out analysis on the outcomes presented.
Publication Bias
Since the total number of included studies is less than 10, we did not perform a funnel plot or Galbraith plot analysis of the publication bias. However, Egger’s regression analysis was performed and found that the limited number of studies did not suffer from significant publication bias (P = 0.054).
Discussion
There is compelling evidence to suggest decompression only may be a viable definite surgical treatment strategy in a select group of patients.16,20,21 Identifying patients who would benefit the most from decompression only would avoid the unnecessary fusion as well as complications to fusion procedure. Although there is no consensus, it is widely accepted that decompression only may be appropriate in patients with radicular symptoms and neurogenic claudication without mechanical back pain.3,16,20,21
The presence of low back pain as a dominant symptom is often considered a sign of instability. 22 It has been argued that decompression is unable to address the underlying instability if present in degenerative lumbar spondylolisthesis. This is one of the strongest arguments in favour of fusion based on the rationale that the pain and symptoms of degenerative lumbar spondylolisthesis are due to instability, and during the natural course of degenerative lumbar spondylolisthesis human body tries to restabilise through decreasing in intervertebral disc space, osteophytic formation, or ossification of spinal ligament. 23 Minamide et al 20 also pointed out that microendoscopic laminotomy may allow degenerative spondylolisthesis to continue its path to restabilization by preservation of structures. In their systematic review Simmonds et al 22 proposed the following variables as probable indicators of stable degenerative spondylolisthesis: facet effusion, restabilization signs including disc height loss, disc angle change on dynamic radiographs, and leg-dominant symptoms with the absence of low-back pain. It is reasonable to conclude that preoperative and operative factors leading to instability can result in unsatisfactory outcomes and failure.
Pearson et al 24 found that radiologically hypermobile patients had better non-operative results than stable patients. Furthermore, some authors have argued that the natural history of degenerative spondylolisthesis is benign and self-limiting.23,25 Inose et al 2 report that there were no significant differences between decompression and stabilization group in terms of occurrence of the postoperative slip progression. Furthermore, postoperative slip progression was not associated with preoperative dynamic instability. It is up for debate if failure due to instability results from improper patient selection or is iatrogenic in nature. Some studies exclude patients with clear mechanical pathology and gross instability, as well as hypermobility.3,26
However, the NORDSTEN trial included patients despite the grade of slippage, with <3 mm in flexion-extension radiographs and observed reoperation in 12.5% of patients, which is comparable to similar studies. 7 Kristoff et al 21 demonstrated satisfactory results in 73.5% of patients treated with decompression alone, which they attribute in part to patient selection ie, exclusion of patients with hypermobile spondylolisthesis. They also found that the duration of back pain, the degree of listhesis, and the height of the disc space correlated with the final outcome.
Blumenthal et al 14 identified three risk factors for postoperative spondylolisthesis after laminectomy-only procedure: motion at spondylolisthesis >1.25 mm on flexion-extension radiographs, disc height >6.5 mm, and facet angle >50. In their study, patients with all three factors had a 75% chance of developing late instability. Considering the relatively high reoperation rate of 37.5% and the preferred surgical technique of wide laminectomy, it could be argued that the identified risk factors mentioned above play a role in the development of postoperative spondylolisthesis in the context of more aggressive decompression methods. A plausible explanation may be that when performing a more radical resection, variables suggesting preoperative instability may have a stronger influence on postoperative results. When analyzing different surgical decompression techniques in the context of failure, issues arise due to the lack of technique standardization and inconsistent definition of failure. When failure is considered to be caused by symptoms attributable to instability associated with the progression of slippage, current evidence suggests that more aggressive decompression may lead to late symptomatic instability. Minamide et al 19 argued that microscopic laminotomy and preservation of structures may relieve symptoms and allow restabilization of spondylolisthesis. However, failure could be attributable to inadequate decompression and residual stenosis, potentially due to insufficient visualization resulting from minimally invasive surgical interventions.
The lack of standardization is evident when comparing the surgical techniques of Blumenthal 11 and Inose. 2 Both are considered open decompression procedures, but in the case of Blumenthal et al, facet-sparing decompressive laminectomy was performed, while Inose et al performed fenestration, which entails removal of the inferior facet and the adjoining ligamentum flavum. Ahmad et al. performed bilateral laminotomy, flavectomy, medial inferior facetectomy, and superior facetectomy, while preserving muscles on one side. 16 Insufficient data exists to strongly and unanimously attribute a specific aspect of the decompression procedure to surgical failure.
Patient Factors (Age, Sex, BMI)
Patient-related factors (age, sex, and BMI) were not significantly different between groups in our analysis. Sato et al 27 found that BMI and higher disc height are associated with higher incidence of SSD (same segment disease). This may be partially attributed to the difficulty in visualisation in obese patients, which can lead to inadequate decompression. Further, higher BMI could lead to higher forces acting on the lumbar spine.
Interestingly, Caelers et al 28 found that higher BMI was associated with a lower probability of postoperative symptomatic spondylolisthesis. They argue that this may be due to lower bone mineral density associated with lower BMI, which may increase the risk of pars interarticularis fracture. The same study found that the female sex is a risk factor for developing symptomatic spondylolisthesis. They argue that the factors leading to the development of postoperative symptomatic spondylolisthesis in women are the same factors that are responsible for the initial development of spondylolisthesis. Due to a more stable lumbosacral joint, higher stress at the intervertebral joints above this level was considered to result in a higher incidence of spondylolisthesis in females.
The clinical guidelines of the North American Spine Society found that there is insufficient evidence on the influence of age or BMI and its impact on treatment results to make any strong recommendations. 1 Our study also did not find age as a risk factor for failure. It should also be noted that although it is not an independent risk factor for failure, a higher age correlates with a higher incidence of complications and should be considered in surgical planning.
Radiological Factors (Disc Height, Facet Angle, Sacral Slope)
The height of the disc, the angle of the facet and the sacral slope were not significantly different between the groups in our analysis. Various studies have reported these factors as risk factors in their analysis. The common perception is that these factors add to the instability by contributing to the inability to resist the shear forces acting on a motion segment. While the facet joints resist one third of shear forces, the intervertebral disc opposes the remaining two thirds. 12 The collapse of disc height is considered a stabilisation mechanism that tries to minimise intervertebral motion. 28 More sagittal-orientated facets allow for more slip to occur by failing to buttress the acting force. The higher sacral slope increases the resulting force acting on the segment. Hence, their role in failure for decompression-only procedure in symptomatic spondylolisthesis needs consideration although their isolated role is proven to be non-predictive to failure in our analysis.
Disease Factors (Movement at Index Level, Pfirrmann Grade, Slip Distance, Translation)
Movement at index level, Pfirrmann grade, slip distance, and translation were not significantly different between groups in our analysis. It was postulated that movement at the index level may be an indicator of instability and may be attributed to postoperative spondylolisthesis. 14 The definition of instability and its effect on the treatment method varies between surgeons. Spina et al 4 found that 57% of surgeons considered translation of 2-4 mm as significant and further 32% considered translation of >4 as significant. They also added that surgeons who prefer fusion were more inclined to employ lower cut-off values for dynamic and static translation when defining instability and the subsequent fusion procedure. Grannum et al 29 argued that decompression only in degenerative spondylolisthesis that is mobile or likely to become mobile may result in unfavourable outcomes. They reported that more mobile spondylolisthesis is associated with higher Pfirrmann grade and more sagittally orientated facets. The Pfirrmann classification is used to grade disc degeneration on MRI. 30 It has been hypothesised that disc degeneration has an inhibitory effect on the progression of disc slippage and that it is part of the physiological mechanism of spinal restabilization. The disc slippage does not progress indefinitely and stops at some point which is not time dependent, and, moreover, the progression of the slippage is not associated with worsening symptoms. 23 Hence, careful assessment of the movement at the index level and objective definition of instability needs to be prioritized before embarking on their role in failure for decompression-only procedure in symptomatic spondylolisthesis.
Individual study analysis has found factors such as motion at index level, and multi-level decompression to be responsible for failure.14,16,27,31 However, upon pooled analysis patient-related factors such as age, sex, body-mass index; disease-related factors such as Pfirrmann grade, slip distance, disc height, facet angulation, translation, movement at index level, sacral slope; and outcome parameters such as visual analog score, Oswestry disability index and Japanese orthopaedic association score between the two groups, did not demonstrate any statistical significance. Hence, careful consideration of individual constellation of factors is necessary to ensure successful outcome with decompression only procedure for degenerative spondylolisthesis.
The study has some significant limitations worth acknowledgement. The number of available studies, comparing the failed group with the successful group of patients undergoing decompression-only procedure, were limited. The criteria for failure noted in the included studies were heterogenous which impacts the overall strength of the evidence generated from the meta-analysis. This might also be a reason explaining the lack of difference between the two groups upon pooled analysis despite some significant differences noted in the individual studies. Hence, we recommend future high-quality randomized controlled trial to be conducted to arrive at a definite conclusion to aid in the development of recommendations on patient selection profile to achieve a consistent favourable outcome with decompression-only procedure for degenerative spondylolisthesis. Further, the heterogeneity noted among the included studies could be due to the variability among the patients included, surgical levels operated, and the invasiveness of the surgical procedure performed in the included studies.
Conclusion
High-quality evidence analysing the risk factors for failure of decompression-only procedure for degenerative spondylolisthesis is limited. Although factors such as motion at index level, and multi-level decompression were found to be a potential risk factors in individual studies, pooled analysis did not find any of them to significantly predict failure of decompression-only procedure for degenerative spondylolisthesis.
Supplemental Material
Supplemental Material - Decompression-Only for Lumbar Degenerative Spondylolisthesis - What are the Risk for Failure? - A Systematic Review
Supplemental Material for Decompression-Only for Lumbar Degenerative Spondylolisthesis - What are the Risk for Failure? - A Systematic Review by Stipe Corluka, Sathish Muthu, Tim Yoon, Carla Cunha, Matthew Gary, Gianluca Vadala, Giovanni Barbanto Brodano, Annalisa Monetta, Andreas Demetriades, Stjepan Ivandić, Yabin Wu, Jeffrey Wang, Hans-Jorg Meisel, Zorica Buser in Global Spine Journal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was organized and supported by AO Spine through the AO Spine Knowledge Forum Degenerative, a focused group of international experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through the AO Spine Research Department.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.