
Abstract
Study Design:
Systematic review.
Objectives:
(1) Study indications for cement-augmented pedicle screws (CAPS) in patients with osteoporosis. Have they changed over the years (2000-2017)? Are there any differences in usage of CAPS based on the geographical region? (2) What were the outcome of the studies? (3) What are the complications associated with this technique?
Methods:
Electronic database and reference list of desired articles were searched from the database (2000-2017). Articles were selected discussing indications, clinical and radiological outcomes, and complications in cases of preexistent osteoporosis treated surgically using CAPS.
Results:
Seventeen studies were identified; 3 were comparative studies and had a control arm (cemented vs noncemented screws). Most studies originated from Europe (10) or Asia (7). Painful vertebral fracture with or without neurological deficit, Kummell’s lesion, deformity and failure to respond to conservative treatment are the common indications for cement augmentation. Visual analogue scale score was the most commonly used to assess pain and average improvement after surgery was 6.1. Average improvement in kyphosis was 13.21° and average loss of correction at the end of the study was 3°. Cement leak was the most common complication observed and pulmonary cement embolism was the most dreaded complication. Nevertheless, majority of cement leaks discussed in studies were asymptomatic.
Conclusion:
CAPS are being increasingly used in osteoporotic spine. Pain scores, functional quality of life, and neurological function indices were studied. CAPS improved anchorage in osteoporotic vertebra and helped improve/maintain clinical and radiological improvement. Common risks of cement leak were observed.
Introduction
Osteoporosis is a systemic disease, primarily affecting the skeleton, leading to decrease in bone mass and micro-architectural derangement, rendering the bone fragile. Affected fragile bones are insufficient to withstand forces beyond physiological load and fractures with minimal trauma. Vertebral fractures are the most common among osteoporotic fractures. Loss of trabecular architecture weakens the bone and decreases the mechanical hold of the pedicle screws, compromising the strength and hastening osteolysis around the screws. Multiple cyclic loading leads to clear-zone formation around the screws preventing osseous integration at screws-bone interface resulting in screw loosening and screw pull-out in osteoporotic spine. 1 Several strategies have been used by investigators to prevent screw pull-out. Cement (polymethylmethacrylate or PMMA) usage to fill trabecular space provides strong anchorage points for fixation. Studies have demonstrated increased pull-out strength and decreased loosening after PMMA augmentation of pedicle screws. 2 Despite the frequent use of PMMA for osteoporotic spine fixation, several questions still remain unanswered. Authors did a systematic review of all the published studies between year 2000 and 2017 to find answers to the most important leading questions pertaining to the use of cement-augmented pedicle screws (CAPS) in osteoporotic spine cases.
Materials and Methods
Key Questions
What were the indications for CAPS in patients with osteoporosis? Have they changed over the years (200-2017)? Are there any differences in usage of CAPS based on the geographical region? What were the outcome of the studies? Has there been change observed in the outcome over the years? What were the complications associated with this technique?
Eligibility Criteria for Selection of Studies
Prospective and retrospective observational studies were included in analysis. Patients included in analysis were adults (age >45 years) diagnosed with osteoporosis and treated surgically with CAPS.
Key Question 1. We searched for the indications of surgery by examining the inclusion and exclusion criteria of the studies available from year 2000 through 2017. Surgical treatment offered in osteoporosis were included in analysis. Key Question 2. All the published data was searched regarding the outcomes of cement augmented screws used in osteoporosis since year 2000 and data was analyzed. Key Question 3. We searched for all the publications reporting cement-related complications with screw augmentation in cases of osteoporosis since year 2000.
Data Extraction
Literature search was done in accordance with PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) check-list and algorithm 3,4 from 2000 to 2017 on PubMed, Cochrane database, MedLine, Google Scholar. Search keywords included “vertebral osteoporosis,” “cement,” “polymethylmethacrylate,” cement augmented pedicle screws,” and “osteoporotic vertebral fractures.” MeSH terms such as vertebral fractures/cement augmented screws, vertebral fractures/PMMA augmented screws and cement augmented screws/complications were also used for data search. Literature available in the English language only were included in the review. All the articles considered suitable for the review were collected and their bibliography was further scanned to search additional data.
Data was extracted independently by 2 independent investigators (TR and VS) and compared. The following data items were recorded: For Key Question 1. Study citation, country of origin, inclusion and exclusion criteria, spine segments treated, intervention and control procedure, year of study. For Key Question 2. Study citation, outcomes assessed, year of the study. For Key Question 3. Study citation, complications noticed, surgery performed (corpectomy, kyphoplasty, or posterior stabilization), amount of cement used, type of cement used, spine segments treated.
Study Selection
Study selection was based on following eligibility criteria: Patients in the study had to have vertebral osteoporosis. Patients were treated surgically with CAPS. Studies had analyzed outcomes of surgery or operative complications.
Studies that included revision surgery, kyphoplasty, and vertebroplasty alone and complications of vertebroplasty or kyphoplasty were excluded. Similarly, biomechanical studies, cadaveric studies, and in vitro studies were excluded.
Authors searched for all the preliminary data finding citations that could be included in the review. Initially, searched articles were screened based on the title and their abstracts. If the screened data was unable to provide sufficient information whether to include or exclude the study, full text of the articles were retrieved for evaluation. Full texts of all the potential articles were included in the assessment (Figure 1).
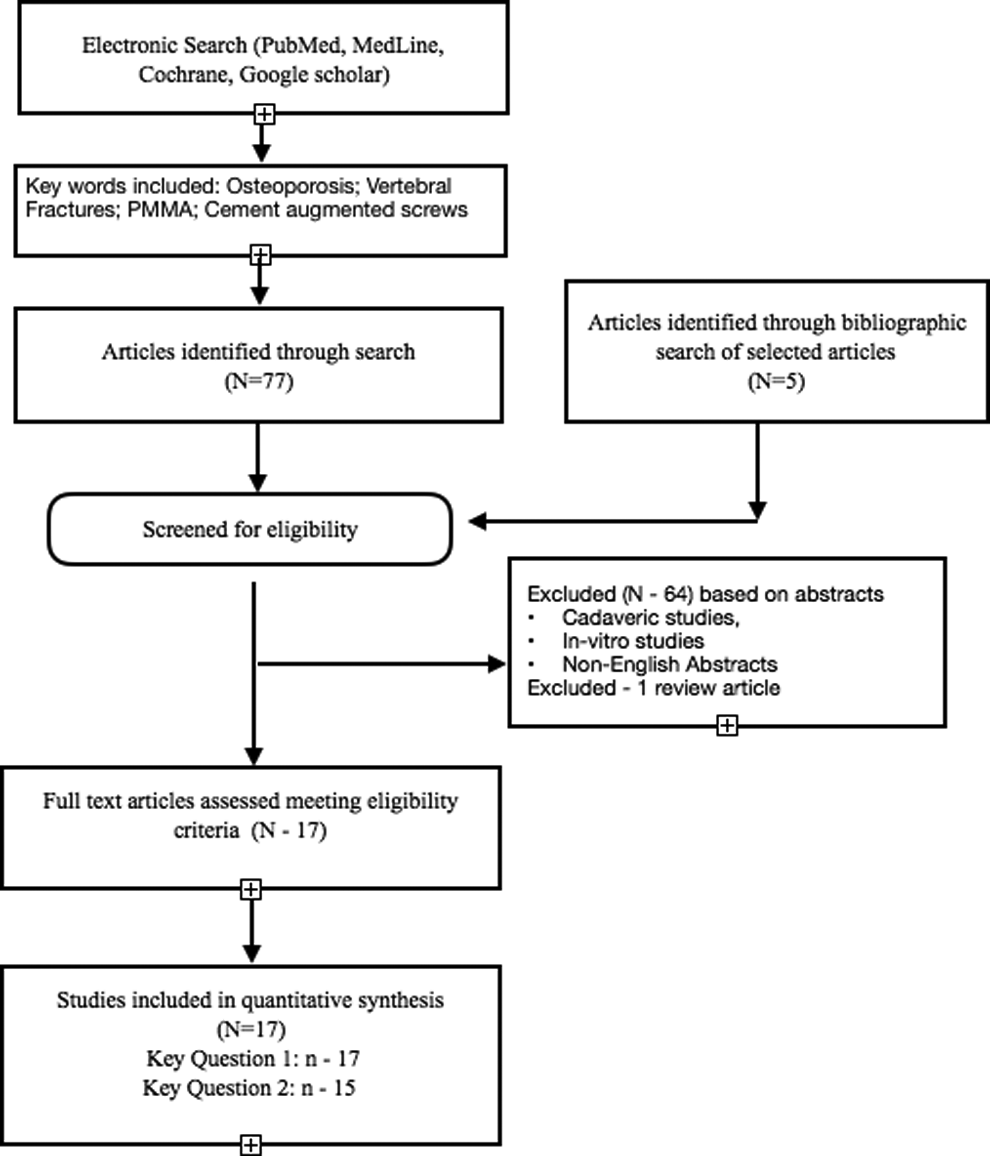
Data search and article selection algorithm.
Data Collection
Data was collected based on a predetermined form which included study title, author details, year of study, age of patients, number of patients, indications of surgery, level of spine treated, follow-up duration, and complications of the surgery. Details of clinical outcomes were recorded from the studies as noted by visual analogue score (VAS), Oswestry disability index (ODI), MacNab’s criteria, Prolo’s score, and Short Form–36 (SF-36) questionnaire. Radiological parameters were recorded from the studies that included segmental kyphosis, kyphosis correction or restoration, canal occlusion, screw loosening, and degree of fusion.
Segmental kyphosis, in included studies was described on lateral spine radiographs by drawing tangent along the end plates using Cobb’s method or by measuring vertebral height (anterior, middle, and posterior). Canal occlusion and fusion were assessed by using computed tomography (CT) scans. Pseudoarthrosis was recognized on lateral radiographs or CT scans by intervertebral cleft or vacuum sign. Screw loosening was identified using different methods in various studies by use of CT scans or specialized software. Neurological assessment was done using Frankel’s grading. Cement-related complications (cement leak) have been assessed using CT scan postoperatively and Yeom’s criteria were used in several studies to classify cement leak based on CT scan images.
Risk of Bias Assessment
The methodological quality of the studies meeting the inclusion criteria was evaluated in accordance with the Newcastle-Ottawa Quality Assessment Scale (NOS), 5 as recommended by the Cochrane Collaboration for assessing the quality of nonrandomized studies. The NOS is a system based on a score (maximum 9 points) set in three different categories: selection of study groups, comparability of cases, controls and their ascertainment of the outcome/exposure on cases and controls. Studies were classified as high risk of bias (1-3 points), medium risk of bias (4-5 points), or low risk of bias (6-9 points) (Table 1).
Details of the Studies Included in the Review With Details.
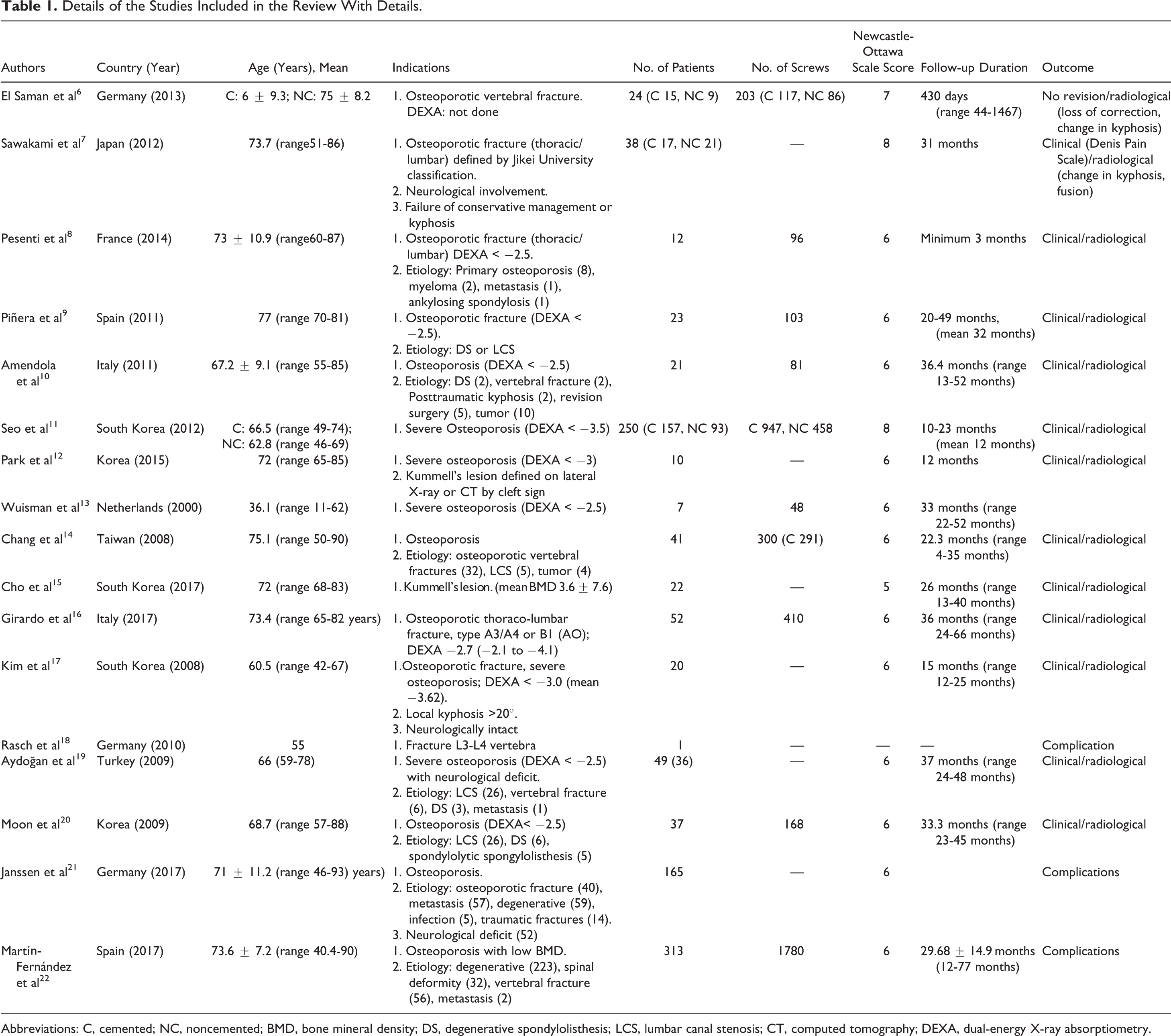
Abbreviations: C, cemented; NC, noncemented; BMD, bone mineral density; DS, degenerative spondylolisthesis; LCS, lumbar canal stenosis; CT, computed tomography; DEXA, dual-energy X-ray absorptiometry.
Results
The initial search identified 77 potential articles, which were screened for eligibility based on the abstract of the study. One review article was excluded as well. Seventeen studies in total met the eligibility criteria and their full texts were retrieved for synthesis of review.
Out of 17 published articles selected for review, 6 were prospective studies, 10 were retrospective observational studies, and 1 was a case report presenting the complication of Palacos cement. Ten studies (Figure 2) were from European region (3 from Germany, 2 each from Spain and Italy, and 1 each from France, Turkey, and the Netherlands) and 7 were from Asia (5 from South Korea and 1 each from Japan and Taiwan). Table 1 describes the characteristics of the studies included in the review.
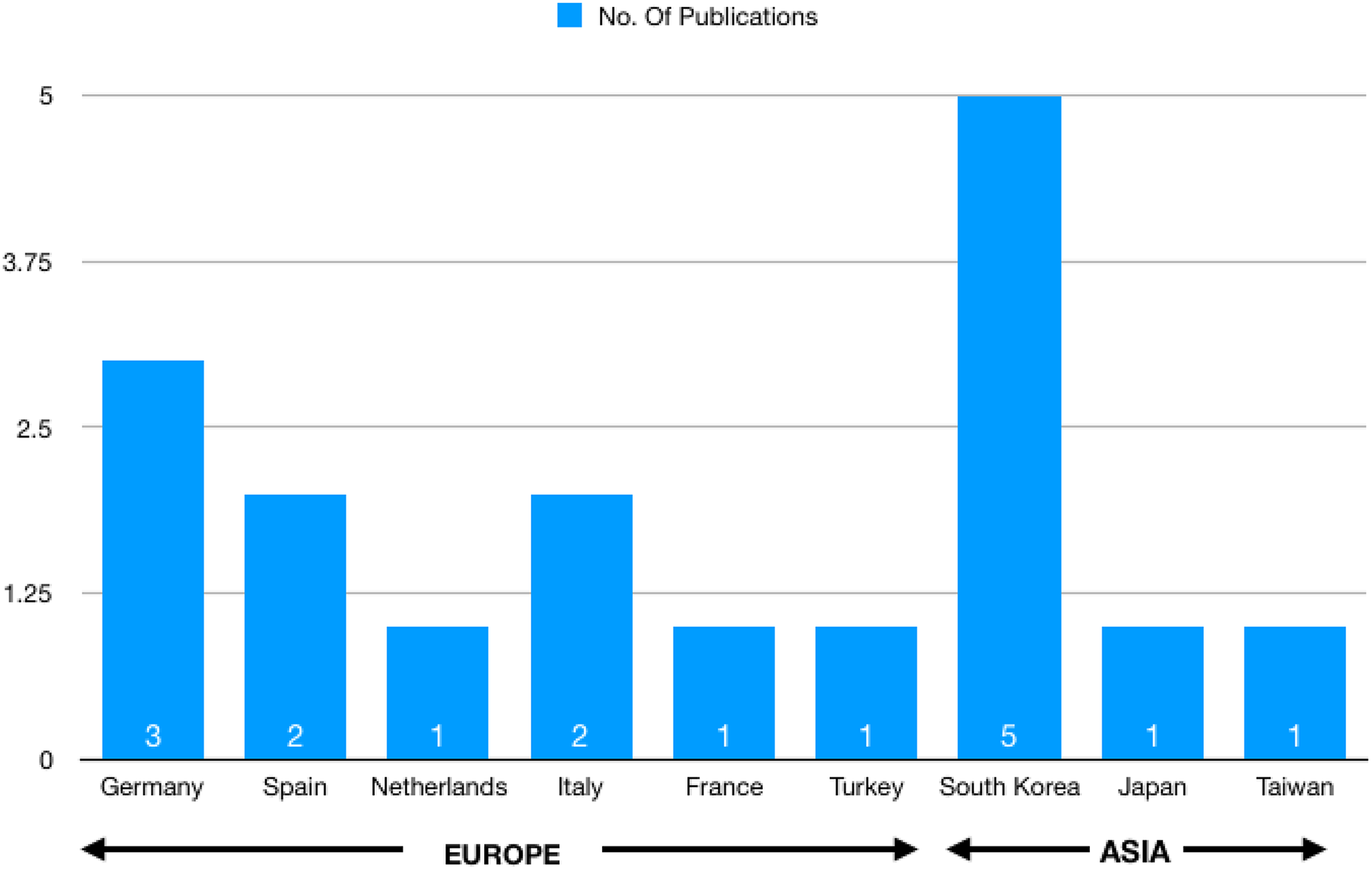
Region-wise distribution of published articles on cement-augmented pedicle screws.
Two retrospective studies and 1 prospective study had control arm wherein outcome of cement-augmented screws was compared with noncemented screws (Table 2). Two studies included used the cement augmented screws in cases of Kummell’s lesion and 1 studied the outcome in pseudoathrosis. 12,15 Cumulatively, study included 1085 patients and sample size ranged from 7 to 313 patients.
Studies With Comparative Group With the Details of the Outcome and Complications.
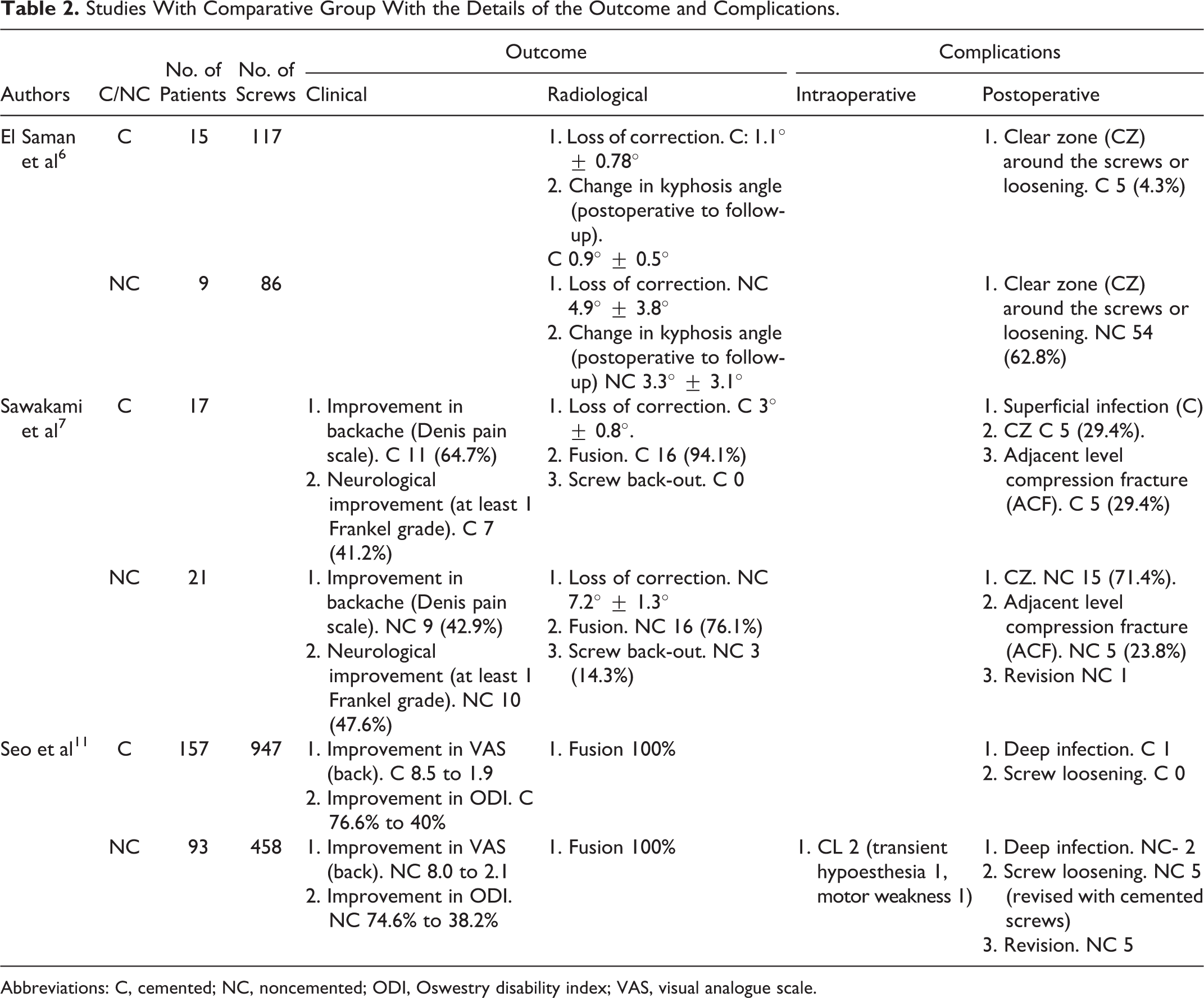
Abbreviations: C, cemented; NC, noncemented; ODI, Oswestry disability index; VAS, visual analogue scale.
Key Question 1: What were the indications for cement augmented screws in patients with osteoporosis? Have they changed over the years? Does the indication vary depending on the geographical region? The details are presented in Table 1. Primary indication for using CAPS in various studies consistently included preexisting vertebral osteoporosis. Most common indications for surgery was painful osteoporotic vertebral fracture. Vertebral osteoporosis was either primary (senile and postmenopausal) or secondary osteoporosis. Etiologies of osteoporosis are mentioned in Table 1. Additional surgical indications were concomitant vertebral fractures, neurological deficit following vertebral fracture, progressive kyphosis, failure of conservative treatment leading to decreased quality of life. Sawakami et al,
7
Park et al,
12
and Cho et al
15
considered pseudarthrosis following vertebral fractures and Kummell’s lesion as indication for using CAPS. Sawakami et al
7
and Cho et al
15
performed corpectomy of the fractured vertebra with anterior reconstruction along with posterior stabilization using cement-augmented screws in their patients. Preexistent spinal pathological conditions in these osteoporotic spines included spinal stenosis and degenerative spondylolisthesis. Osteoporosis was defined by dual-energy X-ray absorptiometry (DEXA) scan with bone mineral density (BMD) assessment. A total of 10 studies used DEXA scan to determine BMD and classified osteoporosis according to World Health Organization guidelines (T score < −2.5 with or without fragility fracture was defined as severe osteoporosis). Sawakami et al
7
used Jikei University classification for determination of osteoporosis. Patients with severe osteoporosis based on BMD were treated with CAPS in most of the studies. There is lack of evidence to determine that the indications of surgery changed over the year since year 2000. The reviewed articles are from Asian and European regions only. There is lack of difference regarding indications for using CAPS in the geographical regions under study. Key Question 2: What were the outcomes of the studies? Has there been change observed in the outcomes over the years? VAS score was the most frequent pain assessment scale used in the studies. Total of 9 studies used VAS score and average improvement in VAS score was 6.1 points. Average postoperative VAS was 2.3 (range 1.42-4.8) compared with 8.4 (8-9.2) reported preoperatively. Sakawami et al
7
used the Denis pain scale for assessment of pain whereas Kim et al
17
and Park et al
12
used modified MacNab’s criteria for pain assessment. All patients reported good to excellent outcome. ODI was most commonly used to assess the functional outcome. Three studies used ODI for assessment of function and average improvement was 42.1. SF-36 questionnaire was used in 1 study. Prolo’s score was used by Moon et al
20
wherein most patients were found to have normal to grade 1 score. Two studies (Pesenti et al
8
and Piñera et al
9
) looked at the length of the hospital stay after using CAPS. Average hospital stay was 7.2 days. Improvement in kyphosis from presurgery to postsurgery was assessed using angular measurement and by assessing vertebral height restoration. Angular improvement of correction was studied in 5 studies and the average immediate correction of kyphosis was found to be 13.21° (7.8°-26.17°). Loss of angular correction (LOC) following CAPS was studied in 6 studies and average LOC was 3.0° (2°-4.6°) at the end of follow-up. Anterior vertebral height was measured in 3 studies where 56.26% height of the vertebral body could be restored in the postoperative period. Pesenti et al
8
used Beck’s index to assess improvement in local kyphosis. Two studies compared the loss of angular kyphosis using noncemented screws and found average loss of 6.05° (4.9°-7.2°) at last follow-up.
6,7
Objective improvement in neurological function was assessed using American Spinal Injury Association (ASIA) and Frankel scale by 4 studies where 79.3% (41.2%-100%) cases improved by at least 1 grade. Aydoğan et al
19
subjectively reported improvement in all patients operated in their series. Simultaneous fusion procedure was done in 9 studies. Seven studies used radiographs for assessment of fusion whereas 2 studies used CT scans to confirm fusion at operated levels. Average fusion rate was 98.4%. El Saman et al,
6
Sawakami et al,
7
and Seo et al
11
performed a comparative study between cement-augmented screws and noncemented screws (Table 3). There was lack of evidence to suggest any change in outcome observed using cement augmentation since year 2000. Key Question 3: What were the complications described in the studies? Complications discussed in the studies were cement (PMMA) related, associated with spinal fixation, or associated with spine surgery. Cement leak (CL) was the most common complication observed in the studies. Most of the CL were asymptomatic or with minimal complications such as transient hypoesthesia or motor weakness. Three studies used Yeom’s classification to define cement leak. Most common pattern of CL occurred through basivertebral veins (type B). It was noticed in 32 (57%) patients. Janssen et al
21
noted 66.7% asymptomatic CL and 5.5% symptomatic leak of which 1.2% required revision surgery for cement removal from epidural space. Martín-Fernández et al
22
in their large series of 313 patients observed 62.3% incidence of CL. Overall, 1.55% of these CL were symptomatic with radicular pain. Overall pulmonary cement embolism (PCE) was reported in 16 cases (1.5%); highest incidence of 7.9% was described by Janssen et al
21
in their study (Table 4). Superficial infection was noted in 16 (1.5%) patients, which responded to antibiotics. Twenty-one (2.1%) patients developed deep surgical site infection and were treated with wound debridement and antibiotics. Dural leak was noticed in 3 patients and Cauda equina syndrome after surgery was noticed in 1 patient. A total of 89 (1.93%) screws were found loosened, out of which 15 (0.32%) were in cemented group and 74 (1.61%) were in noncemented group. Adjacent level compression fracture (ACF) was noticed in 30 (2.76%) patients.
Details of the Outcomes (Neurological, Clinical, and Radiological).
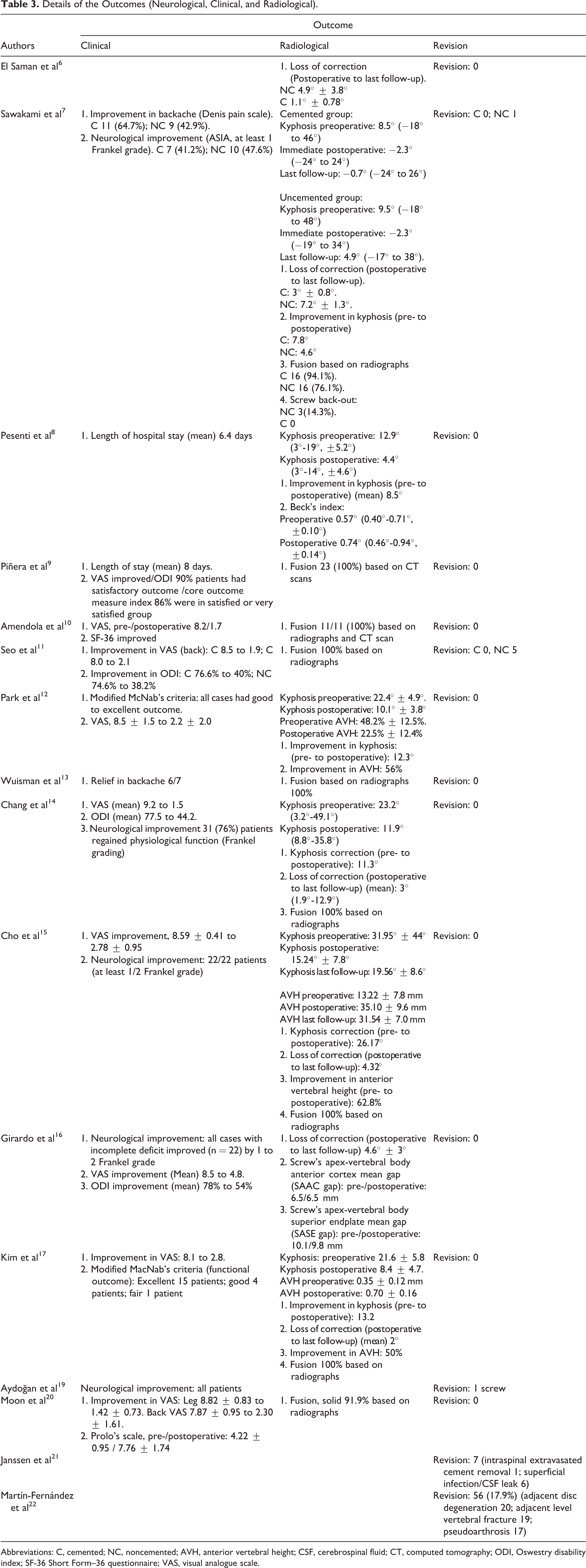
Abbreviations: C, cemented; NC, noncemented; AVH, anterior vertebral height; CSF, cerebrospinal fluid; CT, computed tomography; ODI, Oswestry disability index; SF-36 Short Form–36 questionnaire; VAS, visual analogue scale.
Complications Reported in the Studies With the Details.
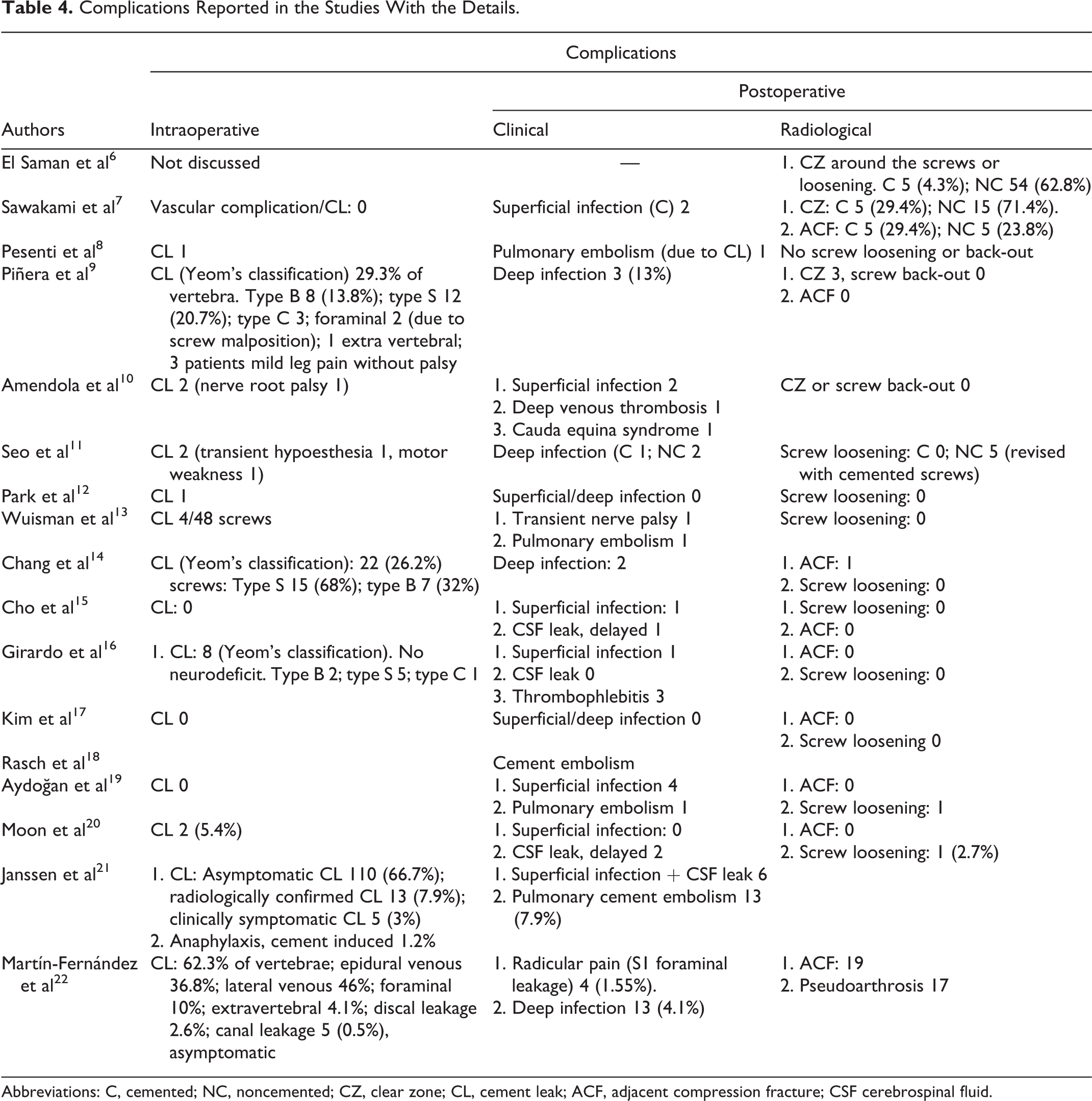
Abbreviations: C, cemented; NC, noncemented; CZ, clear zone; CL, cement leak; ACF, adjacent compression fracture; CSF cerebrospinal fluid.
Discussion
Osteoporosis affects around 200 million people around the globe.
23
Vertebral osteoporosis with decreased bony trabeculae results in poor bone metal integration. Use of cement augmentation in known to increase the pull-out strength by 250% thus imparting immediate construct stability.
2,6
Other salvage methods include alternate methods of fixation like sublaminar wires and hooks, increasing screw dimensions, expandable screws and hydroxyl-apatite–coated screws. However, none of these methods provide immediate construct stability as provided by cement augmented fixation.
24
-26
Most of the studies over CAPS in osteoporotic vertebra have been published lately. Five studies have been published during the period 2000-2008 whereas 12 studies were reported in the later half of study period (2009-2017). PMMA is cement of choice for screw augmentation. Wuisman et al
13
used calcium apatite cement in their study. Authors have suggested that calcium apatite cement hardens with nonexothermic reaction with lesser risk of injury to the neural tissue in case of leakage. However, it may get integrated with surrounding bone and get resorbed with time. Eventually, resorption of the cement matrix around the screws may loosen the purchase in bone and may lead to pull-out. There was improvement in clinical and radiological outcome parameters in all studies. Only few studies have performed a comparative analysis with noncement-augmented screws. Sawakami et al
7
found screw back-out in 3 (14.3%) cases in the noncemented group and 1 such case required revision. Five noncemented screws required revision in study by Seo et al.
11
Martín-Fernández et al
22
reported the highest number of cemented screw revisions. They revised 56 (17.9%) screws; however, their revisions were mostly to address adjacent segment–related issues, including adjacent vertebral fracture, adjacent disc disease, or pseudo-arthrosis formation. CL is the most common complication, which may progress in pulmonary cement embolism. CL was classified according to Yeom’s classification.
27
Type-B leakage occurred through basivertebral epidural veins, type-S occurred through segmental veins, and type-C through cortical defects. Janssen et al
21
and Martín-Fernández et al
22
in their large studies, have reported CL rates of 66.7% and 62.3%, respectively. Although, majority of CL were asymptomatic requiring no further treatment, morbidity and mortality associated with cement usage were significant. Janssen et al
21
noticed 30-day mortality of 1.8% in their study group and suggested against liberal use of cement augmentation. They have concluded that technical improvement in instrumentation or cementing technique has not decreased the rates of CLs and associated complications. Strategies have been suggested to reduce the incidence of CL. Fenestrated screws have been preferred choice for cement augmentation. A total of 8 studies used fenestrated screws and their used has been more frequent in studies reported after year 2010. Pilot hole preparation into the pedicle followed by cement injection and screw placement was done in numerous studies. Sawakami et al
7
performed augmentation by manually covering the screws with PMMA cement before placing it into the pedicles. Chang et al
14
suggested inserting the cement cannula 5 mm short of the selected screw length to avoid anterior cement breach. Wuisman et al
13
showed that 5 of their 7 cases had cement leak when retrograde type of cement injection was used from pressurization effect during screw insertion and advocated for direct method of cement injection. Additional vertebroplasty was done using PMMA cement in few studies. Aydoğan et al
19
performed vertebroplasty in all cases along with cement placement adjacent to the instrumented levels. Chang et al
14
used additional laminal hooks at levels adjacent to CAPS. Amount of cement per screw ranged from 1 to 3 cm3. Frequency of CL were higher in cases where multiple vertebra have been instrumented rather than the amount of the cement used. Hu et al
28
suggested that rate of CL was higher with lower BMD and was not dependent on amount of cement injected per vertebra. Consistency of cement at the time of injection was not widely studied; however, few studies did recommend using toothpaste like consistency to avoid extravasation.
14
Fusion procedure was done in nine studies over the patients with nonmalignant affection of vertebra. Most common of procedure to be performed was posterolateral fusion. Interbody fusion was done in cases with neurological impairment and severe vertebral height loss. Cho et al
15
performed corpectomy with interbody fusion in all cases of Kummell’s disease. Sawakami et al
7
in their comparative study has found better fusion rates in cemented group as compared to the noncemented group. In our review, cement augmentation provided improved anchorage for the pedicle screws in the osteoporotic vertebral body. Improvement in pain parameters were maintained after surgery. Patients in CAPS group, maintained alignment better after correction of deformity with mild loss of correction. Cement augmentation provided desired resilience to the vertebra to withstand corrective forces for deformity correction and allow interbody fusion procedure. Perhaps, categorization of osteoporosis based on the nature of the lesion (osteolytic and nonosteolytic) would have been better, however it was beyond the scope of the present study based on the literature search. Etiologies for osteoporosis have been defined in a few studies, which have been mentioned in Table 1. However, authors have not considered distinction between osteolytic and nonosteolytic osteoporosis in describing their results, outcomes and complications. There is a paucity of literature comparing cemented versus noncemented screws in treatment of osteoporosis. We could not find any clinical trial comparing efficacy or safety of cement augmented screws. There were 3 comparative studies demonstrating improved pain relief with maintenance of spinal alignment. However, cement-related complications cannot be overlooked. Judicious use of cement augmentation and active vigilance toward vascular complications could minimize catastrophic events.
Conclusion
Most common indication for CAPS is osteoporotic affections of vertebra. Osteoporotic fractures were most frequently treated condition. However, CAPS can be extended to primary as well as secondary osteoporosis (metastasis, myeloma, drug-induced). There has been no change in indications for CAPS usage between study duration. The past decade saw a greater number of published articles on cement augmentation. The majority or articles were European or Asian in origin. Fewer comparative studies prevented us from concluding significant advantage of CAPS. Nevertheless, clinical outcome was improved in the CAPS group. Radiological parameters showed maintained correction with minimal loss at the end of follow-up. CL was the most common complication reported. Most of the CL remained asymptomatic but indiscriminate use of cement augmentation was warranted. There was no consensus that technical improvement in instrumentation or cementing techniques have decreased the rates of complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.