
Abstract
Study Design:
Case-control study.
Objectives:
To determine the possible pathogenesis of ossification of the posterior longitudinal ligament (OPLL) in regard to the serum concentration of fibroblast growth factor 23 (FGF-23).
Methods:
The study included 95 patients with OPLL and a control group of 73 age- and sex-matched volunteers. The serum concentrations of FGF-23, creatinine (Cre), alkaline phosphatase, calcium (Ca), inorganic phosphate (Pi), and hypersensitive C-reactive protein (hs-CRP) were analyzed from blood samples, and Cre, Ca, Pi, and tubular reabsorption of phosphate were measured using urine samples. We evaluated the severity of ossified spinal lesions in patients with OPLL according to the ossification index (the OP index and the OS index). Data was compared between the OPLL and control group and between the OPLL progression and no progression group.
Results:
Serum FGF-23 and hs-CRP were higher, and serum Pi was lower in patients with OPLL than in the controls. There was a positive correlation between FGF-23 and hs-CRP and a negative correlation between serum Pi and the OS index; however, the correlations were very weak. Overall, 31.7% of patients had progression of OPLL during follow-up. FGF-23 and hs-CRP were higher in the progression group than in the no progression group.
Conclusions:
These results might indicate that FGF-23 and hs-CRP are positive markers for OPLL. Phosphate metabolism via FGF-23 might be a target for future study on the pathogenesis of OPLL.
Keywords
Introduction
Ossification of the posterior longitudinal ligament (OPLL) is a hyperostotic condition of the spinal ligament associated with a neurological deficit such as myelopathy and/or radiculopathy. 1,2 Patients with OPLL have a systemic increase of new bone formation in the spinal ligament. OPLL is very similar to diffuse idiopathic skeletal hyperostosis (DISH) as reported by Resnick et al. 3 Six genes have been identified as candidate gene locuses 4 ; however, the pathogenesis remains unclear.
Several biomarkers have been identified as possibly related to the pathogenesis of OPLL. Matsui et al. reported increased serum procollagen type I carboxyl-terminal peptide and intact osteocalcin in OPLL. 5 Sugimori et al 6 observed a positive correlation between intact osteocalcin, osteocalcin, and carboxy-terminal propeptide of human type 1 procollagen in patients with combinations of cervical, thoracic, or lumbar OPLL. Furthermore, Kashii et al 7 found that the serum sclerostin level in men with OPLL was higher than in controls, and they identified a negative correlation between the serum sclerostin level and Dickkopf-1 level in males with OPLL. Our recent data demonstrated that hypersensitive C-reactive protein (hs-CRP) in the OPLL group was higher than in controls, 8 and serum inorganic phosphate (Pi) in the OPLL group was lower than in controls. A negative correlation was found between serum Pi and severity of ossification.
Studies have shown that fibroblast growth factor 23 (FGF-23) is an interesting protein related to bone metabolism. FGF-23 is secreted by osteophytes/osteoblasts in bone and helps regulate phosphate concentration in plasma. 9 -11 It is known to act on the kidneys, decreasing reabsorption and increasing phosphate excretion, 12 hence the hypothesis that serum FGF-23 is altered in patients with OPLL. A recent study found higher serum FGF-23 in male patients with OPLL compared with healthy male controls; however, there was no difference in female subjects. 13
In the present study, we focused on the serum level of FGF-23 in patients with OPLL. The purpose of this study was to compare serum FGF-23 levels between patients with OPLL and controls and determine which factors were related to the change in FGF-23.
Materials and Methods
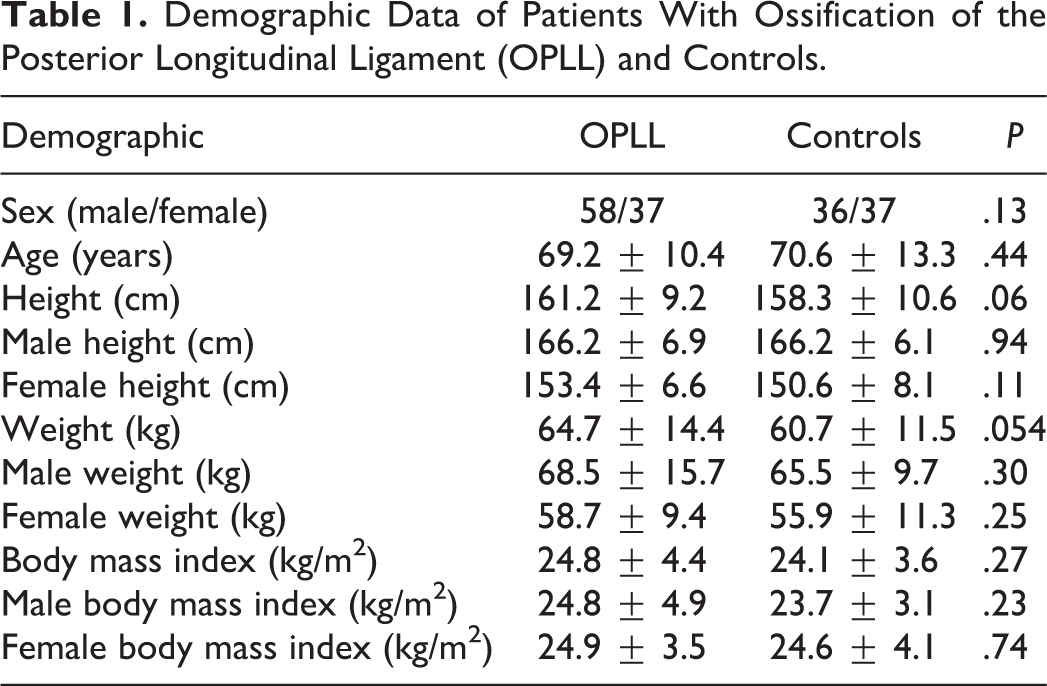
The study comprised 95 patients (58 men and 37 women, average age 69.2 ± 10.4 years; age range, 44-90 years) with cervical or thoracic OPLL. Overall, 73 (36 men and 37 women, average age 70.6 ± 13.3 years; age range, 30-88 years) age- and sex-matched volunteers with degenerative spinal diseases served as the control group. All participants were admitted to the Department of Orthopaedic Surgery at Toyama University Hospital, Japan, between 2014 and 2016. We obtained informed consent from all subjects with a written explanation stating their willingness to participate in the study. The Ethics Committee of the University of Toyama approved the study protocol. The diagnosis of OPLL was based on radiological findings, including radiographs and computed tomography (CT) scans of the whole spine. Metabolic diseases associated with OPLL, such as hypophosphatemic rickets/osteomalacia and hyperparathyroidism, were excluded on the basis of radiographic and biochemical examinations. In all patients with OPLL, CT images were used to evaluate the ossified lesions of OPLL at all spinal levels (cervical, thoracic, and lumbar spine) as well as the presence of DISH. DISH was defined by Resnick et al 3 as a condition with confluent ossification of at least four contiguous vertebral bodies. The control group of age-matched patients had diagnoses of cervical spondylosis, lumbar degenerative disease, and/or spinal disc disease as confirmed on imaging. None of the controls had spinal ossifications. No patient in either the OPLL or the control group had inflammatory disease (such as collagen diseases or rheumatoid arthritis), infection, trauma, myocardial infarction, cerebral infarction, malignant tumor, or kidney disease. Nonsteroidal anti-inflammatory drugs and/or steroids were not used in any patient. Table 1 shows demographic data for the OPLL and the control group.
Demographic Data of Patients With Ossification of the Posterior Longitudinal Ligament (OPLL) and Controls.
The method for sample collection was similar to that in a previous study. 8 Blood and urine samples were obtained on the morning of the hospital visit and immediately stored at −80°C until analysis. The serum intact FGF-23 was analyzed using ELISA Kit (Kainos Laboratories International, Tokyo, Japan) according to the manufacturer’s protocol. The manufacture-reported detection limits are 2 pg/mL, and the intra- and interassay coefficients of variation are reported as 2.1% to 3.8%. 14 Additional routine clinical serum laboratory tests, including creatinine (Cre), Pi, calcium (Ca), and alkaline phosphatase were also assessed. Ca, Cre, Pi in urine, and tubular reabsorption of phosphate (%TRP) were also analyzed. hs-CRP was measured by an ultrasensitive latex-enhanced immunoassay (L-Latex CRP II) using the BN ProSpec Nephelometer (Dade Behring, Newark, NJ, USA). 15
Ossified lesions in the whole spine were evaluated with the same methods used previously. 8 The OP (OPLL) index was used. 16,17 This index is determined by the sum of the levels of vertebral bodies and intervertebral discs in which OPLL is present. We also applied the same index for ossification of the ligamentum flavum (the OF index) and for ossification of the anterior longitudinal ligament (the OA index), both of which were described in previous studiess. 16,17 The total sum of the OP index, OA index, and OF index, known as the total ossification index (the OS index), was used as an indicator for the severity of spinal ligament ossification.
In total, 63 patients (39 men and 24 women with an average age of 70.6 ± 10.2 years; age range, 45-90 years) with OPLL were followed for >2 years using plain X-ray or CT images. Radiographs of the 63 patients were used to evaluate the progression of ossification in the long axis direction and of the width. Progression of ossification was defined as a ≥2 mm increase in the long axis and/or 1-mm increase in the width within and/or adjacent to the cervical lesions. Data was compared between patients with OPLL progression (progression group) and those without progression (no progression group).
Statistical Analysis
The chi-square test was used to determine the difference in sex between the groups. Age, height, weight, and body mass index as well as serum concentrations are shown as mean ± standard deviation. Differences between groups were analyzed for statistical significance using Student’s t test (unpaired). Simple linear regression and Pearson correlation were used to evaluate the correlation between FGF-23 and hs-CRP and between the OP and OS indexes and several biomarkers, including FGF-23. Analysis was performed using StateMate V software (ATMS, Tokyo, Japan), and P < .05 was considered statistically significant.
Results
Table 2 shows the comparison of serum and urine biomarkers between the groups. Mean serum FGF-23 concentration was 52.0 ± 25.6 and 38.0 ± 17.9 pg/dL in the OPLL and control groups, respectively, yielding a statistical difference between the groups (P < .0001); the same difference was found in both the males and females. Serum concentrations of Ca did not differ between the 2 groups, and the concentration of Pi in the OPLL group was lower than in the control group (P = .023) although the difference was very small. The urine concentration of Cre, Ca, Pi, and %TRP was not different between groups. hs-CRP was measured in 85 patients with OPLL and 34 controls, and hs-CRP was higher in the OPLL group than in the control group (P = .027). Furthermore, a positive correlation was found between serum FGF-23 concentration and hs-CRP although it was very weak (P < .0001, r = 0.38) (Figure 1).
Comparison of Serum and Urinary Biomarkers Between Patients With Ossification of the Posterior Longitudinal Ligament (OPLL) and Controls.
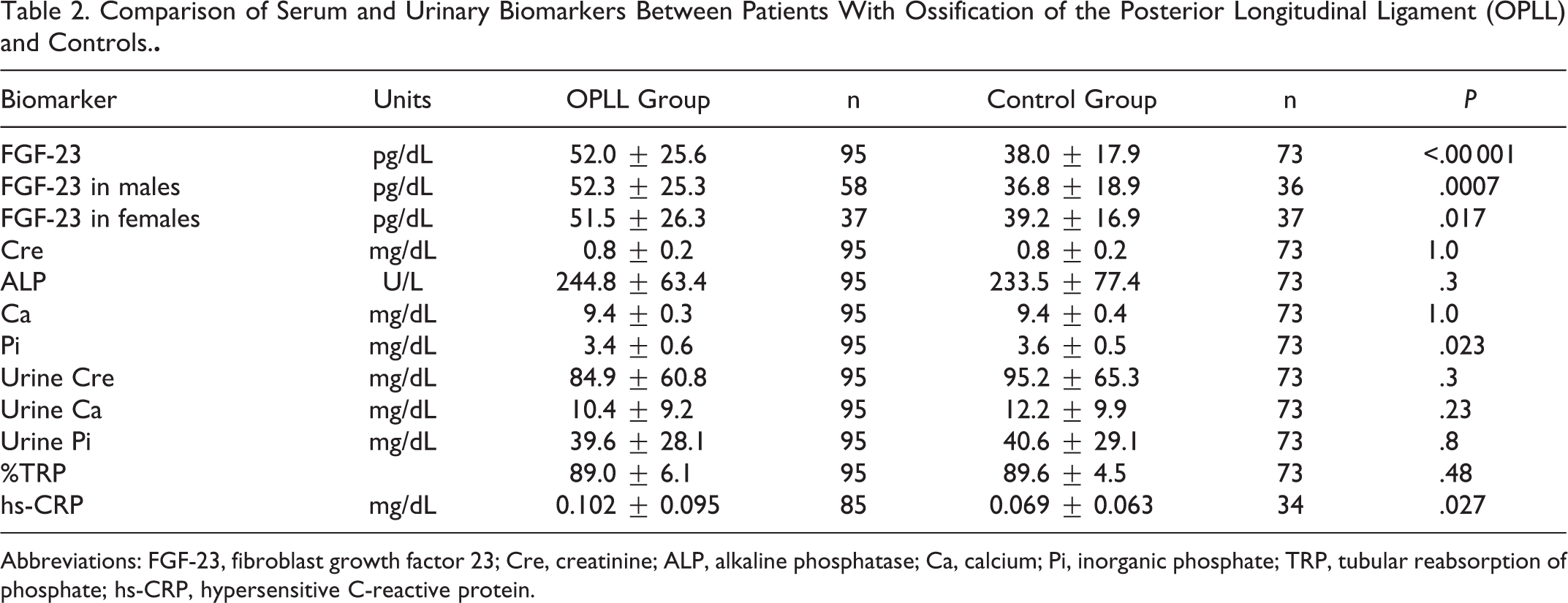
Abbreviations: FGF-23, fibroblast growth factor 23; Cre, creatinine; ALP, alkaline phosphatase; Ca, calcium; Pi, inorganic phosphate; TRP, tubular reabsorption of phosphate; hs-CRP, hypersensitive C-reactive protein.
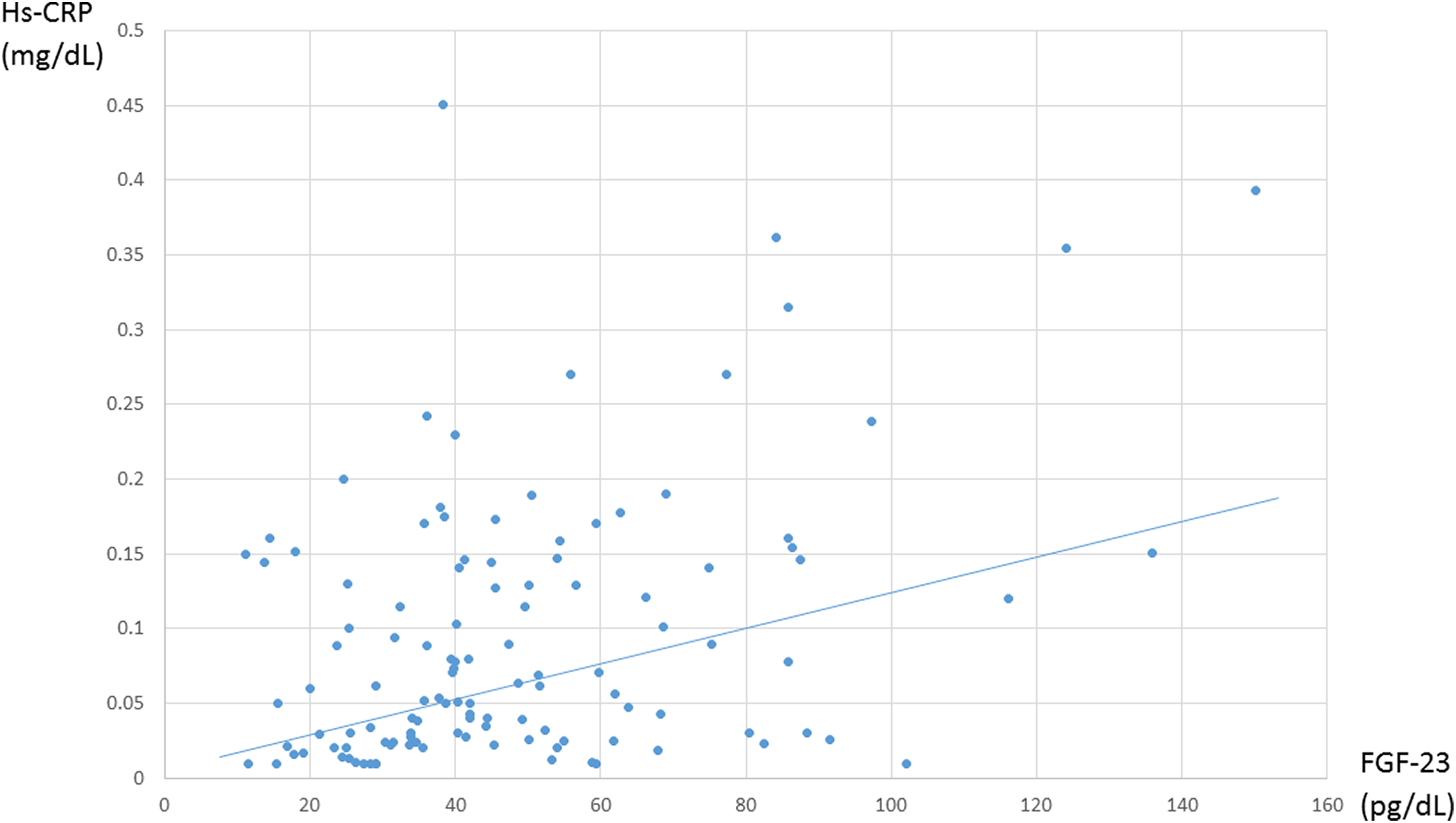
A positive correlation was found in the relationship between the serum concentration of fibroblast growth factor 23 (FGF-23) and hypersensitive C-reactive protein (hs-CRP) (P < .0001, r = 0.38).
The average OP index of the total spine was 10.7 ± 6.5 (range, 2-37), and the average OF index and OA index was 1.0 ± 1.4 (range, 0-6) and 12.3 ± 12.3 (range, 0-48), respectively. Moreover, there also a negative correlation between serum Pi and the OS index although it was very weak (P = .0007, r = −0.34) (Figure 2). No correlation was seen between the serum FGF-23 concentration and the OS index. Of patients with OPLL, 33 were classified as DISH. There was no difference in serum FGF-23 and Pi between patients with and without DISH.
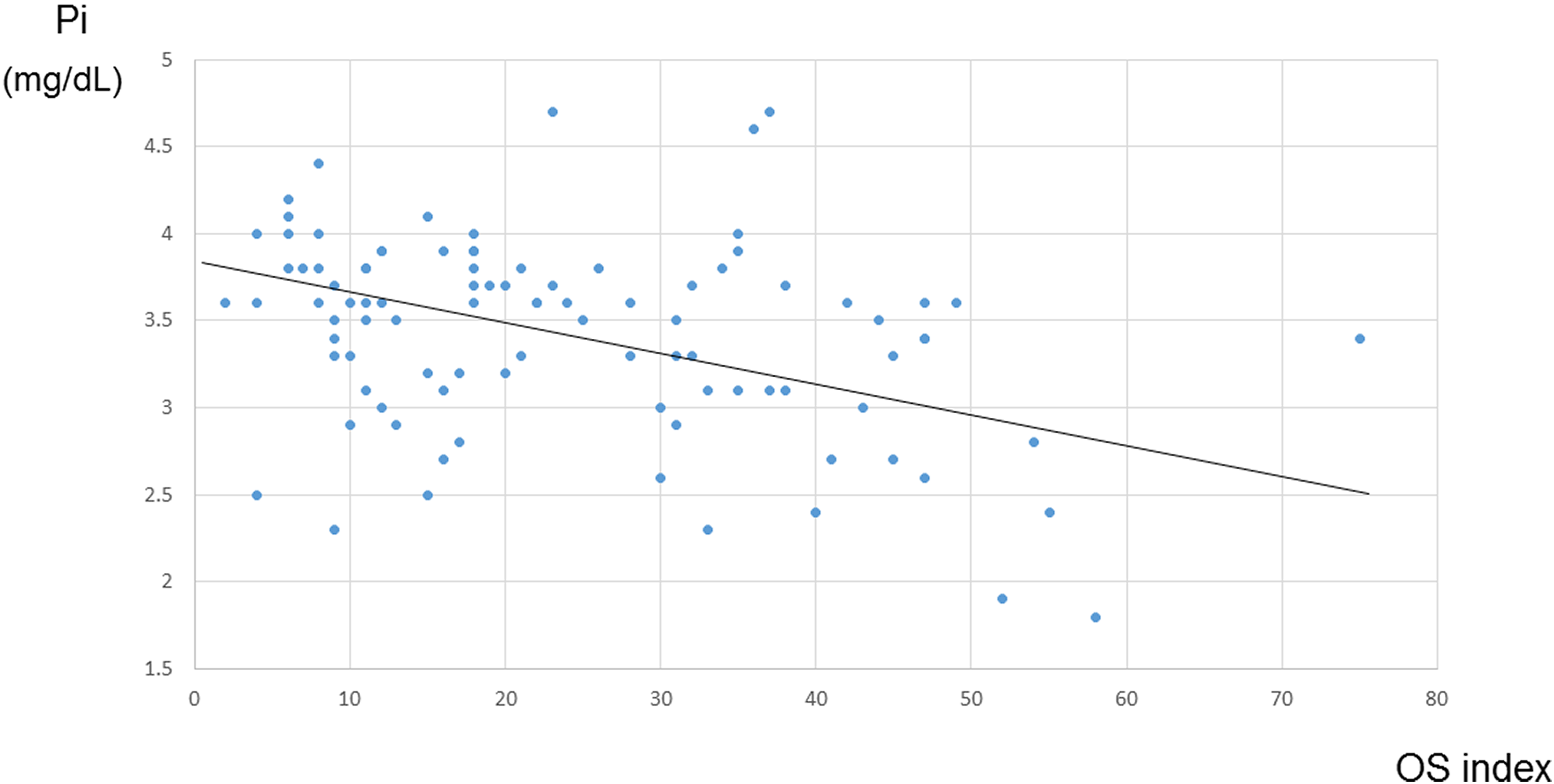
A negative correlation was found in the relationship between the serum concentration of inorganic phosphate (Pi) and the total ossification index (OS index) (P = .0007, r = −0.24).
Twenty (31.7%) of 63 patients had progression of OPLL during follow-up, and FGF-23 and hs-CRP were higher in the progression group than in the no progression group (Table 3).
Comparison of FGF-23 and hs-CRP Between the OPLL Progression Group and the No Progression Group.
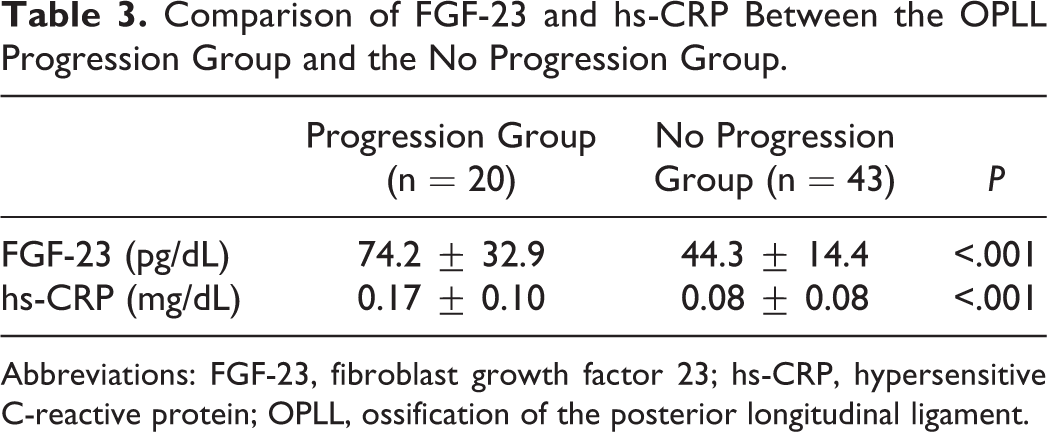
Abbreviations: FGF-23, fibroblast growth factor 23; hs-CRP, hypersensitive C-reactive protein; OPLL, ossification of the posterior longitudinal ligament.
Representative Case
An 80-year-old man with a mixed type of OPLL had C3-6 laminoplasty in 2007 and C3-4 anterior interbody fusion in 2009 (Figure 3). OPLL progression was remarkable during follow-up. At a hospital visit in 2015, his FGF-23 concentration was 124.0 pg/dL and hs-CRP was 0.355 mg/dL, both of which were much higher than normal levels.

Computed tomographic (CT) images of an 80-year-old man with ossification of the posterior longitudinal ligament (OPLL). (A) Sagittal CT image taken 6 months after cervical laminoplasty in 2009. (B) Sagittal CT image taken in 2015. Over 6 years, OPLL progression was found at the C3-4 and C4-5 levels.
Discussion
FGF-23 was isolated as a mouse cDNA encoding a novel FGF using homology of FGF-15. 18 FGF-23 is a phosphaturic hormone produced by osteocytes that bind to Klotho-FGF receptor complex. 19,20 It has been reported that excessive and deficient actions of FGF-23 cause hypophosphatemic and hyperphosphatemic diseases, respectively. FGF-23 was originally identified as one of the genes responsible for autosomal dominant hypophosphatemic rickets. 21 FGF-23 acts as a humoral factor causing tumor-induced osteomalacia. 22 These diseases cause hypophosphate in serum. In contrast, hyperphosphatemic familial tumoral calcinosis is caused by impaired actions of FGF-23. In addition, FGF-23 is related to mineral and bone disorders and is involved in the pathogenesis of chronic kidney disease. 23 On the basis of these results, FGF-23 and FGF-23 receptor/Klotho pathway are considered new drug candidates for targeting disorders of mineral and bone metabolism. 19 The primary function of FGF-23 is to regulate the phosphate concentration in serum. 24,25 In both our previous study 8 and the current study, we demonstrated that the serum concentration of Pi was significantly lower in the OPLL group than in the control group. Different patients and controls were used in the 2 studies indicating reproducibility of the data. Thus, low serum concentration of Pi might be a characteristic of OPLL, although the decrease in Pi was not remarkable even in OPLL. The data in the current study demonstrating higher FGF-23 in the OPLL group than in the control group agrees with the lower serum concentration of Pi in OPLL. Our data also demonstrated a positive correlation between FGF-23 and hs-CRP. Data on FGF-23 in OPLL is new and might be a novel fact related to the pathogenesis of OPLL. Rickets often is reported to be concomitant with OPLL. 26,27 A case report of vitamin D–resistant rickets found extensive ossification of the paraspinal ligaments. 28 The serum Pi concentration in most cases of rickets is lower than in normal controls. A recent study revealed that serum FGF-23 was higher in 41 male patients with OPLL than in 76 healthy male controls although the sample size was very small. 13 Thus, phosphate metabolism, which is regulated by FGF-23, might be an important candidate drug for future research in understanding the pathogenesis of OPLL.
In the current study, %TRP did not differ between groups. Although we expected that %TRP might be reduced in the OPLL group, the result did not match our expectations. Thus, the low serum concentration of Pi in the OPLL group might be affected by other factors including genetic factors. Nucleotide pyrophosphatase (NPPS) gene mutation was identified in an OPLL mouse model, 29 NPPS gene polymorphism was reported to be one of the responsible genes in human OPLL, 30,31 the other possibility being Pi intake from the small intestine. Pi intake from the small intestine is dependent on vitamin D metabolite, which is controlled by FGF-23. For further understanding, the next step in analyzing the NPPS gene and 1,25-dihydroxyvitamin D3 (1,25(OH)2 D3) should be undertaken.
The OS index was established as an indicator for the severity of spinal ligament ossification. The previous studies used a similar index for evaluating the factors related to severe spinal ossification and where spinal ossification exists. 16,17,32,33 The results revealed that severe ossification was found more frequently in females than in males, and >50% of patients with cervical OPLL have spinal ossification in other regions such as the thoracic and lumbar spine. The current study demonstrated a negative correlation between serum Pi and the OS index, indicating the total ossification index (the OP + OF + OA indexes); however, the correlations were very weak. DISH also can indicate the severity of spinal ligament ossification. In the current study, there was also no difference in serum FGF-23 and Pi between the patients with and without DISH. Thus, we did not find any obvious indicators for the severity of spinal ligament ossification.
The results showing that hs-CRP in the OPLL group was higher than in the control group and hs-CRP was higher in the OPLL progression group than in the no progression group are in agreement with our previous data. 8 It is interesting that FGF-23 was positively correlated to hs-CRP, and FGF-23 in the OPLL progression group was higher than in the no progression group. FGF-23 as well as hs-CRP might contribute to the progression of OPLL. Both FGF-23 and hs-CRP might be positive markers for OPLL progression.
The following points are limitations of the study and future perspectives. (1) The number of the patients and controls in this study is limited. More participants are needed for future studies. The correlations shown in the present study were very weak especially based on the limited number of patients. (2) An analysis should be performed on the parathyroid hormone to determine the precise mechanism of lower serum Pi in OPLL. (3) FGF-23 is regulated by 1,25(OH)2 D3; 9 thus, the level of 1,25(OH)2 D3 might be an interesting topic for further study. (4) FGF-23 works by binding to the Klotho-FGF receptor complex. 10,11 A previous study demonstrated an association for Klotho gene polymorphism with bone density and spondylosis of the lumbar spine. 34 Klotho should be examined to determine how the Klotho–FGF receptor complex works in OPLL.
In conclusion, serum FGF-23 was higher and Pi was lower in patients with OPLL than in the controls, and hs-CRP in OPLL was higher than in the controls. FGF-23 and hs-CRP were higher in the OPLL progression group when compared with the no progression group, and FGF-23 and hs-CRP were positively correlated. Phosphate metabolism via FGF-23 might be a future target for understanding the pathogenesis of OPLL.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work reported in this article was supported by grants from the Ministry of Health, Labour and Welfare of Japan: Committee for Study of Ossification of Spinal Ligament and Committee for Research and Development of Therapies for Ossification of the Posterior Longitudinal Ligament.