
Abstract
Study Design:
Prospective, observational cohort study.
Objective:
Selective nerve root block (SNRB) is an effective, standard interventional procedure for failed medical management in lumbar disc herniation (LDH). However, the factors that would predict successful outcomes in patients undergoing SNRB have not been clearly studied.
Methods:
Patients with failed conservative treatment for acute LDH, treated with SNRB were periodically followed till 1 year. Patients who failed to have pain relief or had recurrent pain after SNRB, underwent surgery. The pattern of radiculogram during SNRB was classified into 4 types—“arm,” “arrow,” “linear,” and “splash.” Various clinical factors, radiological factors, and radiculograms were compared between patients who had consistent pain relief (group A) and those patients who did not (group B).
Results:
A total of 91 patients underwent SNRB. Sixty-nine had good pain relief maintained till 1 year (75.8% success). Twenty-two patients underwent surgery after failed NRB at a mean of 6.3 weeks. Patients with sensory symptoms (P = .01), higher mean preinjection Oswestry Disability Index (ODI) score (P = .02), higher mean postinjection ODI score at 3 weeks (P = .004), nonmanual job (P = .01), lumbosacral transitional segment (P = .00 005), and splash pattern of radiculogram (P = .005) were predictive of failed NRB. Logistic regression analysis showed that lumbosacral transitional segment at the level of LDH is the most significant factor predicting poor outcome.
Conclusions:
SNRB is an effective technique to provide consistent symptom relief at least till 1 year in patients with acute LDH. The study identified several factors that predicted poor outcomes of SNRB and such patients can be forewarned about need for later surgery.
Introduction
The lifetime prevalence of radiculopathy due to a herniated lumbar disc is estimated to be around 4% in females and 5% in males. 1 Compressive radiculopathy due to acute lumbar disc herniation (LDH) manifests with radiating pain along the compressed nerve root, sensory dysfunction, motor deficits, and rarely, cauda equina syndrome. In most cases, this radiculopathy has an expectant good outcome with a conservative line of care. However, in some patients with recalcitrant pain, prolonged conservative care can result in poor functional outcomes. 2 While early surgery in carefully selected patients with discogenic radiculopathy can achieve rapid relief, potential disadvantages of surgery include risks of infection, discitis, recurrence, nerve root injury, and anesthetic complications. 3,4
The acute radicular pain in patients with LDH is related partly to the mechanical compression by the herniated disc and to a larger extent, due to the perineural inflammatory response around the nerve root. 5 Hence, local instillation of corticosteroids around the inflamed nerve root has an important role in alleviating the pain. Among the different techniques of intraspinal steroid injection such as transforaminal, interlaminar, and caudal epidural steroid injections, selective nerve root block (SNRB) is a highly target-oriented procedure with good efficacy in patients with LDH. 6,7 In SNRB, the corticosteroid is injected directly near the dorsal root ganglion and the inflamed nerve root. Randomized clinical trials indicate that the nerve block is a cost-effective procedure in the majority of cases compared with other operative interventions. 8 Furthermore, potential complications associated with surgery such as recurrence, cerebrospinal fluid leakage, hematoma, and infection can be avoided by SNRB.
The efficacy of SNRB in acute LDH has been quoted variedly in previous studies ranging from 30% to 80%. 8 However, there is a dearth of studies that identify the various clinical and radiological factors that can predict successful outcomes in patients undergoing SNRB. We performed a prospective, observational cohort study of patients with acute LDH treated with SNRB and studied them over a period of one year to evaluate the predictive factors of successful outcomes.
Material and Methods
The study was conducted in a tertiary referral spine care center, between January 2016 and December 2016 and was approved by the institutional review board of the institute. During the study period, all patients with documented LDH in magnetic resonance imaging (MRI), presenting with unilateral radiculopathy, with symptom duration less than 3 months and failed adequate conservative care (3 weeks) were treated with SNRB. Patients with cauda equina syndrome, gross motor neurological deficit, chronic radiculopathy >3 months, multilevel disc prolapse (>2 levels), contralateral radiculopathy, bilateral radiculopathy, recurrent disc prolapse, predominant axial pain, high lumbar disc prolapse (above L3-4), spondylolisthesis and radiculopathy due to trauma, infections, or tumors, were excluded. The remaining patients who opted for SNRB formed the study group (Figure 1). They underwent SNRB by a single fellowship trained spine surgeon, with >5 years of experience in spine surgery. All patients had a standard technique for SNRB as explained below.
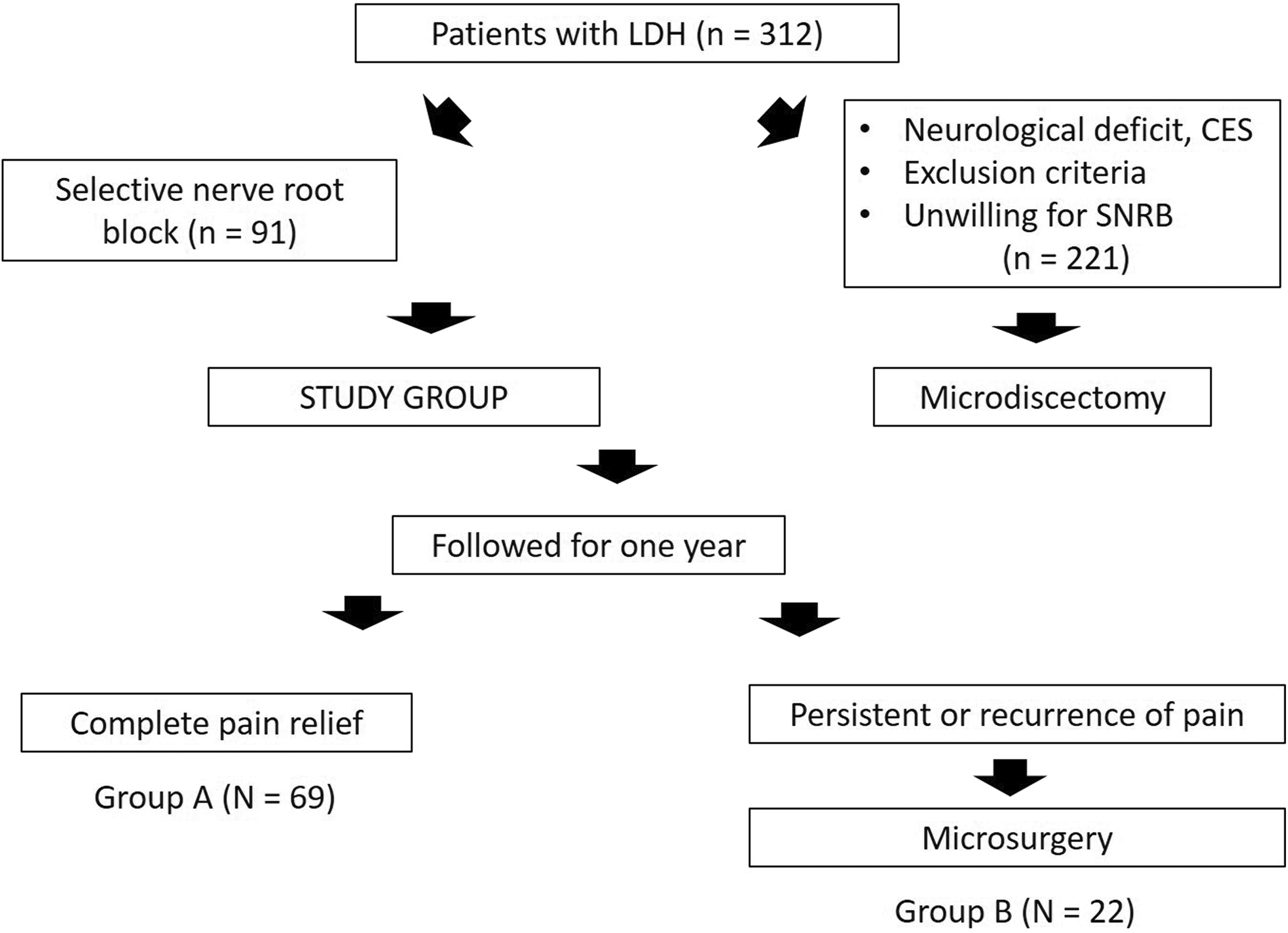
The number of patients available for treatment and their selection into the study.
Nerve Block Technique
Under prone position without any sedation, the patient was made to lie on a radiolucent table. For L3-4 and L4-5 levels, the image intensifier was tilted toward the side of radicular pain to acquire an oblique view of the spine to visualize the “Scotty Dog.” The skin overlying the neck of the dog was anesthetized with 5 mL of 2% lignocaine. A 23-gauge spinal needle was introduced end-on toward the “safe triangle,” that is, above the nerve root and below the pedicle. At L5-S1, the image intensifier was positioned to visualize the sacral foramen through which the spinal needle was inserted. After verifying the correct needle positioning under anteroposterior and lateral fluoroscopic control, 1 mL of contrast solution (Ioxehol) was injected to confirm that the needle was in the desired position close to the selected nerve root and the dye ensured that the drug was not administered intravascularly. Pain reproduction was elicited in all patients before the corticosteroid was infiltrated. Once the radiculogram was visualized, 2 mL of 0.5% bupivacaine mixed with 80 mg of triamcinalone was injected around the nerve root. Following the procedure, the needle entry site was sealed with a sterile dressing, and the patients were kept under observation for 45 minutes. The patients were discharged on the same day with a standard postinjection protocol—rest for a day, limited activities as per comfort limits and tablet pregabalin 75 mg at bedtime for 3 weeks.
Patients were serially followed up at 3 weeks, 6 weeks, 6 months, and 1 year. During the clinical assessment, the clinical data and outcome scores were independently documented by a physician assistant. During the follow-up, the patients, whom failed to have adequate pain relief or had recurrence of pain opted for microsurgery. All the patients received the nerve block only once.
The following clinical, radiological, and radiculogram patterns were collected and compared between patients who had consistent pain relief up to 1 year with those patients who did not have adequate pain relief with SNRB and required surgery.
Clinical Parameters
The following clinical parameters were documented in all patients, including age, sex, duration of symptoms, side of pain, level of lesion (L3-4, L4-5 and L5 -S1), presence of inciting event, presence of back pain, type of job (manual laborer, white collared, home maker), Body mass index, presence of sensory symptoms along the affected nerve root (subjective paresthesia and objective anesthetic zones), visual analogue scale (VAS) score for leg pain (preoperative, 3 weeks, 6 weeks, and 1 year), presence of previous similar episodes, smoking, comorbidities, straight leg raise test positivity, and Oswestry Disability Index (ODI) score at preoperative, 3 weeks, 6 weeks, and 1 year.
Magnetic Resonance Imaging Parameters
In the MRI images, the parameters studied were the level of disc prolapse (L3-4, L4-5, L5-S1), position of disc in the axial T2 image (posterocentral, posterolateral, and far lateral), the type of disc herniation (bulge, protrusion, extrusion, sequestration), Pfirrmann’s grade of the affected disc (grades I to V) and the presence of lumbosacral transitional vertebra at the level of the disc herniation was studied.
Classification of Radiculogram
During nerve block, iohexol was injected extraepineurally to trace the nerve root and this radiculogram was broadly classified into 4 types as “arm,” “arrow,” “linear,” and “splash” (Figure 2). The “arm” pattern was defined as a thick band of dye around the entire thickness of the nerve root, “arrow” pattern was defined by the flow of the dye around the medial aspect of the nerve root and tracks down around the thecal sac, “linear” pattern denoted as a single streak of dye along the lateral aspect of the nerve root, and the “splash” pattern was defined as an irregular distribution of the dye around the nerve root. In patients with combinations of patterns, the predominant pattern of dye distribution was selected as the main type.
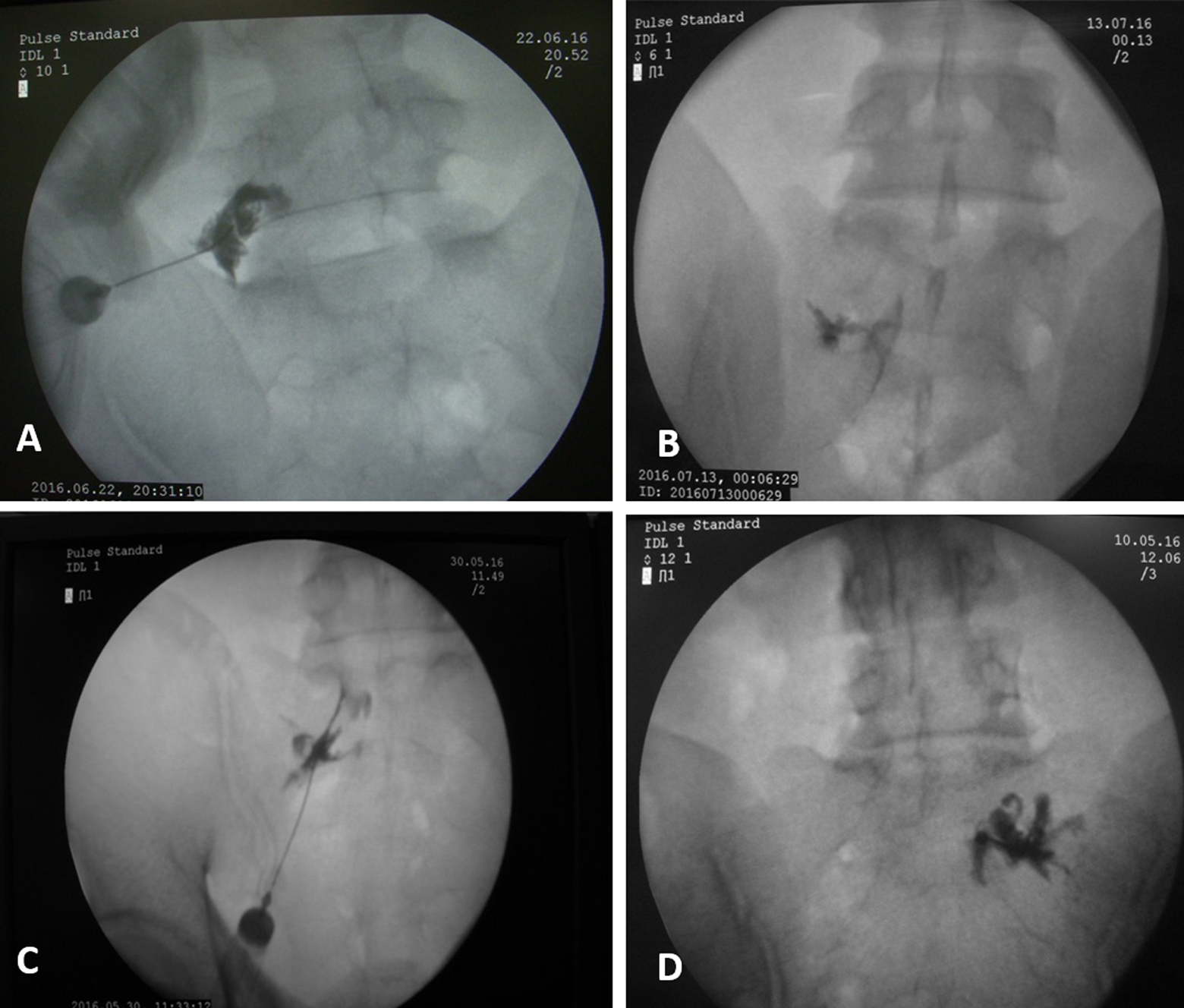
The radiculogram, observed after injecting the dye, was broadly classified into 4 types as “arm,” “arrow,” “linear,” and “splash.” The “arm” pattern was defined as a thick band of dye around the entire thickness of the nerve root, “arrow” pattern was defined by the flow of the dye around the medial aspect of the nerve root and tracks down around the thecal sac, “linear” pattern denoted as a single streak of dye along the lateral aspect of the nerve root, and the “splash” pattern was defined as an irregular distribution of the dye around the nerve root.
Statistical Analysis
We used chi-square test, 2 × 2, and multifactor contingency table for categorical variables, and a proportion of mean analysis for mean values between the 2 comparison groups. A P value <.05 was considered to be statistically significant. For analyzing the effect of multiple variables together, a logistic regression analysis was performed.
Results
During the study period, 312 patients had a failed medical conservative care. Out of which, 221 patients, either did not meet the inclusion criteria for SNRB or opted for surgical care directly, and hence were excluded from the study. The remaining 91 patients underwent SNRB and formed the study cohort. All of them underwent SNRB by a single surgeon as described previously. All patients were available for periodic follow-up till 1 year.
During the follow-up, 69 patients had good pain relief maintained till 1 year (69/91,75.8% efficacy). Twenty-two patients either did not have adequate pain relief (n = 8) or had a temporary period of relief followed by severe pain (n = 14). These 22 patients underwent surgery at a mean of 6.3 weeks after the failed NRB. Four patients had a surgery even before the scheduled first follow-up at 3 weeks after SNRB while the rest had it after 3 weeks.
Univariate analysis showed that patients with sensory symptoms (P = .01), higher mean preinjection ODI score (P = .02), higher mean postinjection ODI score at 3 weeks (P = .004), having a white-collared office job (P = .01), and lumbosacral transitional segment (P = .00 005) and “splash” pattern of radiculogram (P = .005) were predictive of failed NRB. Other factors including age, sex, duration of symptoms, side of pain, level of lesion (L3-4, L4-5 and L5 -S1), presence of inciting event, presence of back pain, smoking, co-morbidities, body mass index, VAS score for leg pain (preoperative, 3 weeks, 6 weeks, and 1 year), previous attacks of sciatica, straight leg raise positivity, and other MRI findings (disc type and position, level of degeneration) were not predictive (Table 1).
Distribution of various Clinical, Radiological, and MRI Findings Between the 2 Groups of Patients.
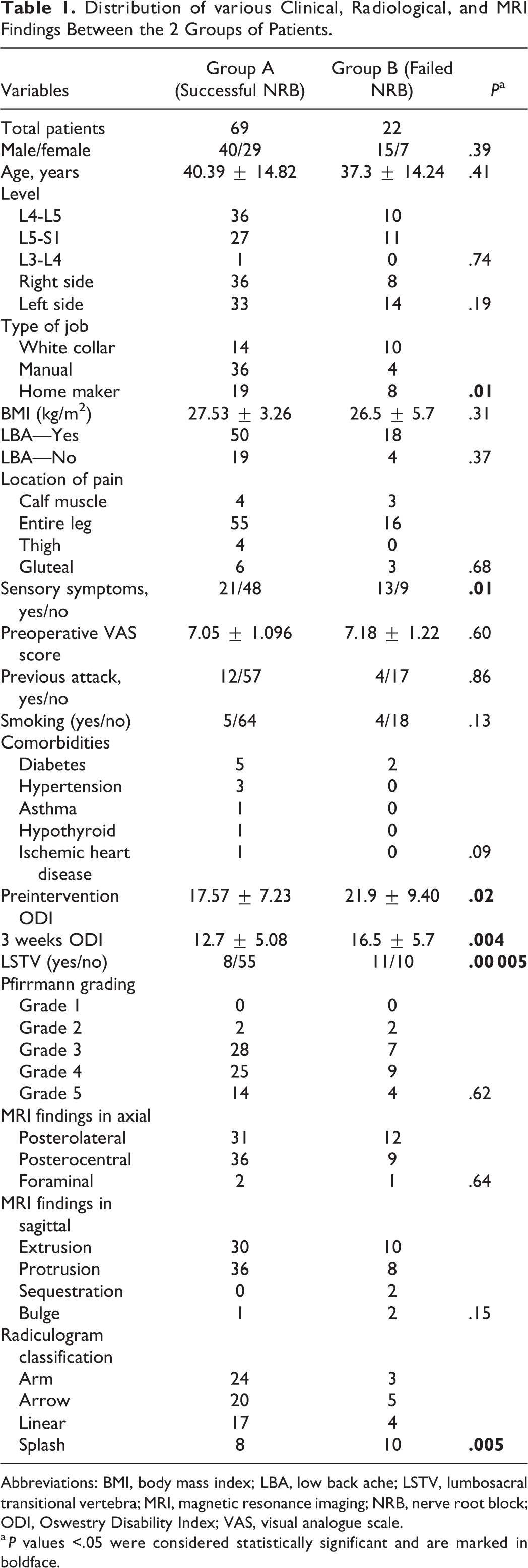
Abbreviations: BMI, body mass index; LBA, low back ache; LSTV, lumbosacral transitional vertebra; MRI, magnetic resonance imaging; NRB, nerve root block; ODI, Oswestry Disability Index; VAS, visual analogue scale.
a P values <.05 were considered statistically significant and are marked in boldface.
Multivariate logistic regression analysis was performed, which showed that presence of lumbosacral transitional segment (P = .0005) was the most significant factor for predicting a failed SNRB with an odds ratio of 20.1.
Discussion
Selective steroidal nerve root block is a standard initial care of intervention in patients with recalcitrant radicular pain following LDH. The therapeutic effect of local steroid infiltration is well recognized in the literature through several clinical studies and the success of pain relief is quoted up to 88%. 9,10 However, these studies have had varied inclusion criteria for patients such as those with radiculopathy, stenosis, disc herniation, degenerative listhesis, and scoliosis. 11 -15 Being a pain-relieving interventional procedure, it also falls in the purview of different medical care specialists, including spine surgeons, radiologists, anesthesiologists, and pain physicians, and thus the inclusion criteria and evaluation of patients varies widely in different studies. 16,17 There is also a dearth of studies that have evaluated together, the multiple clinical and radiological factors that could predict a good functional outcome following SNRB, specifically in patients with LDH.
In the present study, several clinical factors that predicted a failure of SNRB, including significant sensory symptoms, high mean preinjection and mean postinjection ODI score at 3 weeks, and having a white-collared job were identified. Patients with significant sensory symptoms often are worried about the paresthesias and thus have a tendency to consider that surgical intervention would be superior and hence possibly opted for an earlier surgical intervention. McCormick et al 18 evaluated 188 adults who underwent a fluoroscopically guided transforaminal steroid injection for lumbosacral radiculopathy. Pain reduction from preinjection to 2-weeks follow-up was measured by a VAS. The authors noted that patients who experienced ≥50% pain relief at follow-up had reported higher preinjection pain, reported no worsening of their pain with walking and had a positive femoral stretch test. 18 No significant differences were found for other demographic and clinical factors, including the presence of disc herniation, stenosis, or other neural tension signs on physical examination. Interestingly, in our study, we noted that patients with high mean preinjection ODI score and high postinjection ODI scores at the end of 3 weeks reported less improvement with SNRB and opted for surgical intervention.
Patients in nonmanual job (“white collared”) had a poor outcome with SNRB. While studies have shown a higher incidence of LDH in patients pursuing heavy manual labor, its relationship with regard to outcomes of LDH management has not been clear. Interestingly, in 2 separate studies, it has been shown that the incidence of LDH was significantly higher in patients who were in high-stress jobs, specifically patients whose jobs resulted in repeated time-based deadlines, and patients with lower job satisfaction. 19,20
Apart from clinical predictors, the possible radiological predictors which could predict the outcomes of SNRB have also been evaluated. Lee et al 21 studied the MRI-based outcome predictors of lumbar transforaminal steroid injections in patients with LDH (n = 149) and showed that LDH in the foraminal-extraforaminal zone had significantly better outcomes with nerve blocks while other factors such as T2-high signal, relation to nerve root, corner change, Modic change, disc height loss, grade of disc degeneration, and osteophyte were not statistically significant. Kim et al, 22 in a retrospective, small study group of 64 patients, noted that a small disc herniation length with a cutoff value of 6.23 mm and high baseline VAS leg pain were identified as predictors of successful outcomes of leg pain relief in the 30 patients who had a successful NRB. 22
In our study, among several radiological factors studied, we noted that those with sacralized L5 had a poor outcome with SNRB. This was very significant since in the multivariate logistic regression analysis, this was the only highly significant factor with an odds ratio of 20.1. The relationship between disc herniation, low back pain, and lumbosacral transitional vertebra has been described in several studies. This correlation has been attributed to the increased biomechanical stress produced by the transitional segment. 23,24 Interestingly, in our study, the level of disc herniation, the side of herniation, the type of LDH, Pfirrmann’s grade of the herniated disc, and the position of the disc in the axial plane did not correlate with the outcomes.
The radiculogram produced by injecting the dye around the nerve root could be an indicator to evaluate the efficacy of NRB since it demonstrates the pattern of flow of the drug around the inflamed nerve root. Pfirrmann et al 25 studied the flow of contrast material in 36 patients and classified as type 1 (tubular appearance—intraepineural), type 2 (nerve root visible as filling defect—extraepineural), or type 3 (nerve root not visible—paraneural) based on a comparative evaluation in cadavers. The authors noted that SNRB is effective in sciatica, but type 1 injections (intraepineural) were more painful than type 2 injections. In a similar study by Lee et al 21 in 56 patients, 76.8% success was achieved at the end of 2 weeks with SNRB and multiple regression analysis showed that the only factor significantly associated with better outcome was the extraepineural type of injection.
In our study, all the SNRBs were administered extraepineurally since intraepineural injections are painful and can cause chemical radiculitis. None of the previously published studies have clearly studied the pattern of intraepineural radiculogram and its outcomes with SNRB results. We observed 4 patterns of radiculograms—“arm,” “arrow,” “linear,” and “splash.” Probably the “arm” pattern indicates spread of dye completely around the nerve root while the arrow and linear patterns indicate the flow of dye along the medial and lateral parts of the nerve root respectively. Our analysis showed that all these 3 types had a good outcome while the fourth pattern “splash” type had a poor outcome with SNRB. The other patterns typically demonstrated the spread of the dye along the nerve root and the thecal sac, while the “splash” pattern indicated a nonspreading pattern of dye. This could possibly because of venous engorgement and perineural adhesions around the nerve root, impeding the spread of the drug around the nociceptive regions of the inflamed nerve root. There was no MRI evidence of nerve root anomalies in patients who had this splash pattern. In the 10 of 18 patients with splash pattern who required surgery, there was no intraoperative evidence of nerve anomaly.
To the best to our knowledge, this is the first report to evaluate the combined role of different clinical, radiological and radiculogram factors in patients with LDH by selective nerve block. Furthermore, the specific inclusion of only those patients with acute LDH, periodic follow-up of 1-year, single surgeon series (standardized performance), independent analysis of outcomes by a physician assistant (reduced bias), and prospective nature of the study are some of the other strong points of the study. While the study is promising, its major limitation would be the smaller number of patients involved in this study, for the multiple variables studied.
Conclusion
SNRB is an efficient technique (76% efficacy) to provide consistent symptom relief at least till 1 year in patients with acute LDH avoiding surgical intervention. The study identified several clinical and radiological factors that predicted outcomes of SNRB. These include patients with nonmanual job, presence of significant sensory symptoms, high mean preinjection and mean postinjection ODI score at 3 weeks, and lumbosacral transitional segment and “splash” pattern of radiculogram, and such patients can be counseled about the need for later surgical intervention.
Footnotes
Acknowledgments
The authors would like to acknowledge the assistance provided by Dr K. M. Sakthivel, Assistant Professor, Department of Statistics, Bharathiar University, Coimbatore, in statistical works of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Ganga Orthopaedic Research and Education Foundation (GOREF).