
Abstract
Study Design:
Sickle cell disease (SCD) is a relatively common blood disorder that has profound implications on the musculoskeletal system and particularly the spine; however, there is a paucity of data in the literature discussing this important topic.
Objectives:
(1) To elucidate common spinal pathologies affecting patients with SCD, as well as the medical and surgical treatments available for these patients. (2) To discuss indications for surgical management of spinal complications of SCD and important for orthopedic surgeons when taking patients with SCD to the operating room.
Methods:
A narrative review of the literature was performed.
Results:
Patients with SCD have a significantly higher risk of developing spinal pathologies including vertebral osteomyelitis, compression fracture, vertebral vaso-occlusive crises, and osteoporosis, among others. In addition, patients with sickle cell disease are particularly susceptible to developing perioperative and post-operative complications including surgical site infection, implant malfunction, and vertebral body compression fracture. Postoperatively patients with SCD are prone to developing complications and adequate hydration is necessary in order to reduce complications of SCD.
Conclusions:
Several spinal pathologies may arise secondary to SCD and distinguishing these pathologies from one another may be challenging due to similarities in symptoms and inflammatory markers. Although most patients with SCD can benefit from conservative treatment involving rest, symptomatic therapy, antibiotic therapy, and/or orthosis, surgical intervention may be indicated in certain cases. It is preferable to avoid surgery in patients with SCD due to an increased risk of complications such as wound infection and vaso-occlusive crisis.
Introduction
Sickle cell disease (SCD) is a type of blood disorder that follows an autosomal recessive pattern of inheritance. SCD is caused by a point mutation in the β-globin chain of hemoglobin, causing the hydrophilic amino acid glutamic acid to be replaced with the hydrophobic amino acid, valine, at the sixth position. The β-globin gene is found on the short arm of chromosome 11. 1 The abnormal morphology of hemoglobin in this condition starkly reduces the flexibility of red blood cells so that they become a rigid, sickle shape in the setting of low oxygen tension. Once “sickled,” these cells are not able to conform back into their normal biconcave disc shape even after normal oxygen tension has returned. Normally, red blood cells are flexible and are able to contort their shape to pass through low caliber vessels such as capillaries; however, the sickle-shaped red blood cells have markedly decreased flexibility and are unable to change their shapes to cross the capillary bed. 2 The cells therefore accumulate in the capillaries leading to vessel occlusion and subsequent ischemia. Physiology stress, high altitude, temperature changes, and dehydration are common conditions that can precipitate the sickling of red blood cells in patients with SCD.
Repetitive vessel occlusion in SCD leads to the progressive deterioration of organs, including the spleen, lungs, liver, kidneys, skeleton, and central nervous system. It follows that one of the most commonly encountered clinical manifestations of SCD are due to the osteoarticular involvement. In an acute context, patients can present with severely painful vaso-occlusive crises in bone. In the chronic setting, repetitive sickling can present with avascular necrosis. Spine pathology is prevalent in SCD as well. Although the spine involvement is widespread in SCD population, there is a paucity of information regarding the relationship between SCD and spine pathologies.
Methods
A narrative review of the literature was performed between January through March of 2017 of the NCBI PubMed database. Articles published between 1950 and 2018 containing the keywords sickle cell disease, spinal disease, chronic pain, spinal surgery, SCD, sickle cell anemia, and microinfarction were reviewed by 2 of the coauthors. All articles discussing the pertinent topic, including case reports, biochemical studies, meta-analysis, prospective and retrospective trials, and other publication forms were included. The articles that were selected for inclusion in the present study were selected on the basis of the quality of the publication.
Results
SCD and Spine Pathology
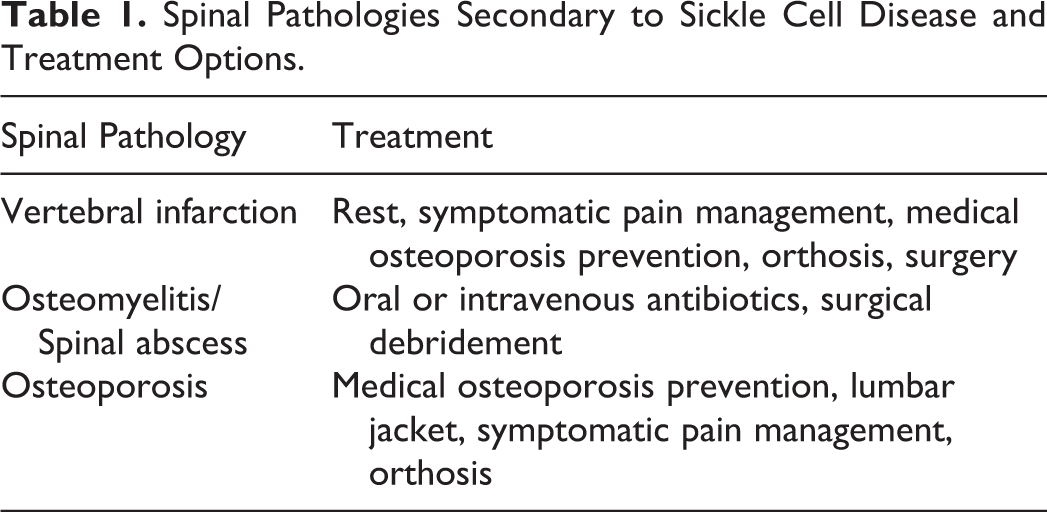
The sickling of red blood cells can result in abnormalities in many organ systems, especially in the musculoskeletal system. While these musculoskeletal complications typically do not contribute to mortality, they do cause a significant amount of morbidity. Bone involvement both of the spine and elsewhere is the most common clinical manifestation of SCD and comprises both acute and chronic pathology (Table 1). Acute bone problems in SCD include painful vaso-occlusive crises, osteomyelitis, stress fractures, orbital compression syndrome, dental problems, vertebral collapse, and bone marrow necrosis. Chronic bone problems in SCD include avascular necrosis, chronic arthritis, osteopenia, and osteoporosis. 3,4 Each of these problems can be localized to the spine in patients with SCD.
Spinal Pathologies Secondary to Sickle Cell Disease and Treatment Options.
Vaso-occlusive Crisis
Vaso-occlusive crisis is the most common of the bone pathologies affecting patients with SCD. 4 -6 Vaso-occlusive crises are the most common acute clinical presentation of SCD in children. These crises affect almost all SCD patients and this problem recurs throughout life. Vaso-occlusive crises are caused by microvasculature occlusion by sickled red blood cells resulting in chronic tissue ischemia and infarction, which ultimately leads to pain and swelling in the ischemic tissues. 4,5
Acute painful vaso-occlusive crisis can occur in any bone with active marrow, but most commonly occurs in the spine and knee. The femur and sternum are commonly affected areas as well. Roughly two-thirds of patients have involvement of the lumbosacral level of the spine, while an additional 20% of patients have involvement of the thoracic level of the spine. Clinical manifestations of vaso-occlusive crisis in the spine include severe back pain and pain to palpation of the vertebrae. Flat bones, such as the cranium, ilium, and ribs, are less likely to be the site of vaso-occlusive crisis and infarction relative to nonflat bones because of have relatively more vascular channels and are therefore better perfused. 7
In terms of imaging related to vaso-occlusive crises, radioisotope bone scans using combined Tc-99m-labeled sulfur colloid (for bone marrow uptake measurement) and Tc-99m-diphosphonate (for bone uptake measurement) can reliably recognize acute phase areas of infarction. 8 While a bone scan is usually sufficient, a bone marrow scan or magnetic resonance imaging might be more sensitive in detecting infarcts. 9 Radiographs usually are not helpful in confirming a bone marrow infarction since acute phase vaso-occlusive crises typically show up as normal bone. 9 However, there have been reported radiographic signs of bone infarction, including the “fish vertebra” sign and “vanishing” of the vertebra in a patient with SCD. The fish vertebra sign appears as a biconcave deformity of lumbar vertebrae with “bone softening in lateral and posterior-anterior radiographs of the spine” (Figure 1a and b). 5 This amplification in the normal concave curvature of the top and bottom surface of one or multiple vertebral bodies is due to ischemia of the middle part of the vertebral growth plate. 5 There is damage in the central area of the vertebra while the outer areas of the vertebral end-plates are retained. 2 Different arteries supplying different areas of the vertebra is the cause of these findings. Blood is supplied to the central vertebra by the long branches of the vertebral nutrient artery, while short perforating branches of the periosteal vessels supply blood to the peripheral areas. 2 Vaso-occlusion and destructive events are more likely with the longer end vessels than with the shorter vessels. 10

Posterior-anterior and lateral view of fish vertebrae sign highlighting bilateral concavity of the vertebral bodies.
The case of the vanishing vertebra on radiograph may be explained by the combination of vaso-occlusive infarction, secondary infection, compressive forces along the spine, and reactive bone response. 11 Other radiological findings include a coarse trabecular pattern, persistent anterior vertebral notching, biconcavity of the bodies, step ladder effect, massive collapse of the “central,” and compression deformities. 12,13 There can be a presentation of multiple osteolytic lesions involving the bodies of lumbar vertebrae with a decrease in the height of affected vertebral bodies.
Osteomyelitis
Osteomyelitis is the second most common bone pathology in patients with SCD. The incidence of acute osteomyelitis or infection of the bone is dramatically increased in SCD patients compared with the general public because of the combined effects of tissue infarction, immunodeficiency secondary to splenic dysfunction, and excess iron, an important bacterial nutrient secondary to increase red cell turnover. 4
While studies have shown the most common pathogens of osteomyelitis in SCD patients are Salmonella spp and Staphylococcus spp, there are reports of anaerobic osteomyelitis. 4,14,15 Several case reports have described Bacteroides fragilis as the pathogen in vertebral osteomyelitis, and the collection of these reports reveal that B fragilis osteomyelitis may not be as rare as previously thought. The clinical presentation of these cases included fever, chills, nausea, vomiting, and localized, nonradiating low back pain without neurological symptoms. These patients were also jaundiced and found to have elevated bilirubin, erythrocyte sedimentation rate, and the diagnosis was confirmed with computed axial tomography scan, technetium-99m bone scan, and magnetic resonance imaging. Osteomyelitis in these cases was treated successfully with intravenous antibiotics. It may be inferred from these cases that acute hematogenous anaerobic osteomyelitis may respond to antibiotics without surgical debridement. 14
In the chronic setting, the bone changes due to repetitive infarction and subsequent marrow hyperplasia contribute to avascular necrosis and osteoporosis, respectively. Thrombosis together with infarction most often affects the head of the femur or of the humerus. 4,16 Erythropoietic marrow hyperplasia due to chronic anemia affects the bone trabeculae, causing absorption, softening, shape change and osteoporosis. 17 A pediatric study by Buison et al 18 adjusted for the poor growth observed in SCD patients and supported an association between children with SCD and significant deficits in bone mineral density and total bone area. This factor may place children with SCD at higher risk for fragility fractures relative to the general public. 18
Osteoporosis
Individuals with SCD are predisposed to osteoporosis secondary to both low levels of vitamin D level and reduced bone mineral density. Reduced bone mineral density may lead to medullary hyperplasia. 9 The pathophysiologic mechanism related to why patients with SCD have low bone mineral density and reduced vitamin D levels is not well described, though it is likely to be related to the chronic inflammation present in the bone of individuals with SCD. A Boston-based study observed bone health of adults with SCD by measuring vitamin D levels, bone mineral density, markers of bone resorption, and the formation of vitamin D and calcium before and following 12 months of treatment. The C-terminal component of pro-collagen type 1 level, which is a marker of bone resorption, was elevated in the subjects before and after the treatment. Other studies have claimed that the pathophysiology of low bone mineral density in patients with SCD is related in part to increased bone resorption resulting from the action of inflammatory cytokines such as tumor necrosis factor–α and interleukin-6 that are released in bone during ischemic conditions. 19,20
Patients with osteoporosis and nutritional deficiencies of vitamin D are at increased risk of fragility fractures. Therefore, both low vitamin D levels and low bone mineral density of the lumbar spine are indications for treatment in patients with SCD to prevent osteoporosis and osteopenia. 7,21,22 Some studies have shown that 65% of children with SCD had low serum 25(OH)D levels and 64% of adults with SCD had a low bone mineral density compared with age-, race-, and sex-matched controls. 22
In children, vaso-occlusive crisis and resulting bone pain is the one of the most common presenting symptoms in a child with SCD. As in adults, the most commonly affected portions of the skeletal system are the spine and knee. In one study conducted at the Children’s Hospital of Eastern Ontario, the authors treated 30 patients between 1990 and 1996 for active SCD and found that the spine represented 26% of all bone involvement secondary to vaso-occlusive crisis. This was surpassed only by the knee in this cohort, which represented 35% of cases. 23
Beyond acute vaso-occlusive crisis other commonly encountered issues that are unique to young SCD patients include abnormal body structure, nutritional deficits, and late sexual and skeletal development, which cannot be wholly explained by bony deficits alone. 24 Taking this into account, some studies have shown that children with sickle cell disease have lower bone mineral density compared with healthy controls which increases the risk of stress fractures and vertebral collapse and which is a marker for nutritional deficiency. A study of Brazilian children and young adults with SCD concluded that the lumbar spine was the best site for assessment of bone mineral density, while radiographs were unreliable. 24 A study of bone mineral density in young adults with SCD found that 72% had low bone mineral density and that the proportion of cases of osteopenia and osteoporosis in a young adult population with sickle cell disease is very high. 25
Conservative Treatment of Spinal Pathology in SCD
According to the SCD literature, the treatment of spine pathologies in SCD patients is mainly conservative. Surgical management is usually avoided due to the frequent complications that result from spine surgery in this patient population. Most notably, collapse of osteoporotic vertebrae in this patient population is a very common complication of surgery. It is important to point out that clinically, it can be difficult to distinguish between bone infarction and bone infection in patients with SCD. Both these conditions present with elevated inflammatory markers, fever, and tenderness. Certain factors such as high fever, fluctuance, and erythema may make a diagnosis of infection more likely than infarction.
The treatment for vertebral infarcts and destruction in patients with SCD is chiefly conservative because of a high incidence of intra and perioperative complications, including acute respiratory syndrome, vaso-occlusive crisis, and increased rate of implant failure, following surgery. Conservative management includes rest, symptomatic therapy of acute painful episodes, osteoporosis medical therapy, and orthosis. 14 Pain medications and muscle relaxants can be useful but their chronic use can bring side effects, including sedation and anticholinergic effects such as dry mouth and constipation. 14 The need for such medications can be reduced by use of proper thoracic or lumbar orthosis. 14 A Nigerian case report in 2001 describes conservative management of a 9-year-old female child with SCD who presented with lower extremity hypertonia with hyperreflexia. 26 Her imaging showed multiple osteolytic lesions involving the bodies of L3-5 with a loss of height of affected vertebral bones. She wore a lumbar jacket for 3 months, she was treated with analgesics and was on bed rest for the initial 6 weeks. After 3 months of therapy, repeat imaging showed marked healing of the affected vertebral region with significant regeneration of the bone tissue.
In patients with SCD who have spondylodiscitis with or without formation of spinal abscesses, the treatment is often conservative with antibiotic therapy in the absence of a neurologic deficit. 27 Since Salmonella and Staphylococcus aureus are the most common causative agents of osteomyelitis in patients with SCD, ceftriaxone and oxacillin are the mainstay antibiotic therapy to cover both pathogens, as these antibiotics target these organisms. 28 There is a recognized risk of the development of a postoperative kyphotic deformity secondary to laminectomy in patients with associated spondylodiscitis. 29 A Brazilian case report presented a case of a 6-year-old girl with SCD who presented with fever, hip pain, and refusal to walk. 27 She was found to have spondylodiscitis with paravertebral collections and epidural abscess. She did not have any neurologic deficits at the initial evaluation. After 6 weeks of antibiotics therapy with ceftriaxone and oxacillin, she recovered fully.
The indications for conservative treatments are osteoporosis due to bone marrow hyperplasia, osteomyelitis, bone necrosis, and vertebral fracture. Conservative management includes symptomatic treatment with pain medications, antibiotic therapy for frequent infections, osteoporosis prevention, and lumbar jacket. The application of lumbar jackets may sometimes be recommended to stabilize the affected patients’ spines and prevent further deterioration and loss of bone. The indications for lumbar jackets include impaired mobility at the waist, stiff gait, and lumbar lordosis. 26 Lumbar jackets also improve the patient’s ability to ambulate, which improves their ability to participate in outpatient management. 26
Surgical Treatment of Spinal Pathology in SCD
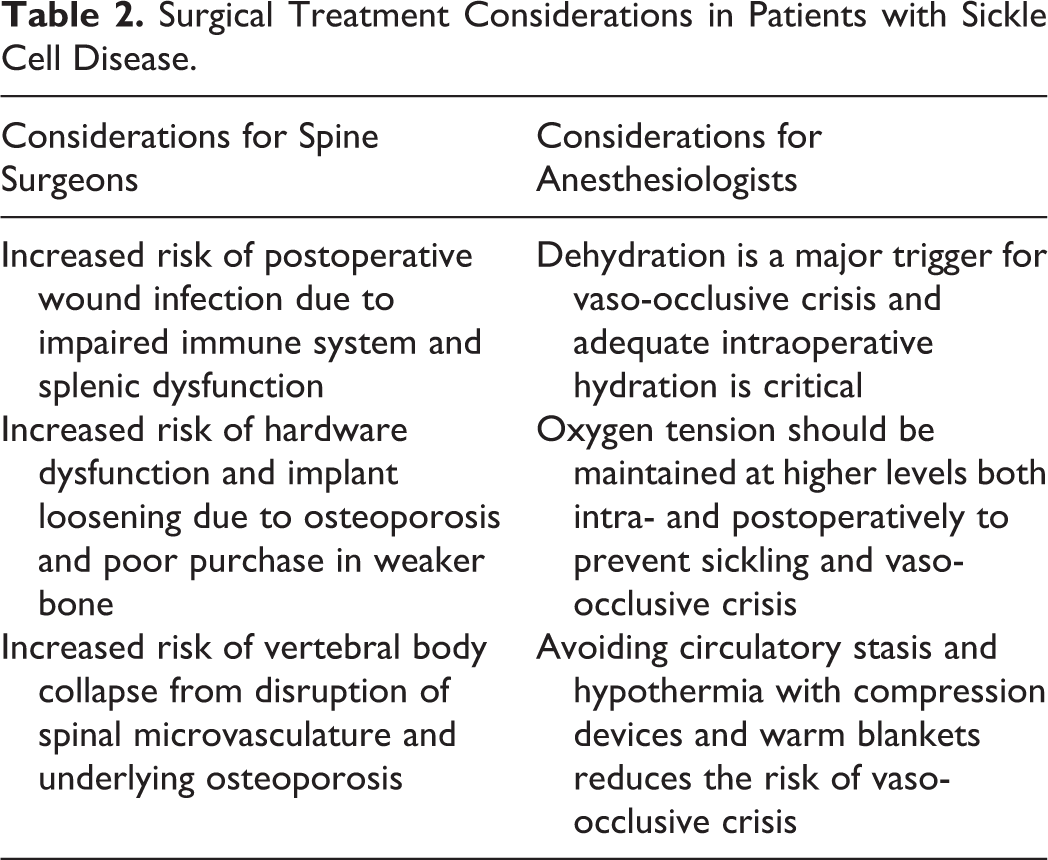
Surgical treatment (Table 2) can be considered when the clinical impact of spinal pathology secondary to SCD occurs in a young patient with otherwise well-controlled SCD. 21 Surgical debridement of the spine should also be considered when antibiotic therapy alone is inadequate to treat the extended abscesses. 28 As noted above, relative to non-SCD patients, patients with SCD are often immunocompromised secondary to splenic infarct and therefore are less likely to respond to antibiotic therapy alone for spinal abscess and osteomyelitis. This is because even when antibiotics are prescribed, the baseline immunologic function of patients with splenic infarctions are reduced compared with the general population. Therefore, prolonged antibiotic therapy may fail to resolve infections in many patients with SCD. 22 In such cases that antibiotic therapy fails to treat patients with overwhelming signs of spinal abscess or osteomyelitis, surgical debridement is the next step in treatment. Examples of failure of antibiotic treatment include failure of resolution of fever, elevated white blood cell count, and fluctuance and tenderness over the suspected infectious site after a full course of antibiotics lasting 6 to 8 weeks. 22
Surgical Treatment Considerations in Patients with Sickle Cell Disease.
An Italian case report describes a patient with SCD who received laminectomy at T12 level and T10-L1 arthrodesis with fenestrated cemented screws for worsening and potentially invalidating kyphosis deformity. The patient suffered subsequent collapse of the osteoporotic vertebra below the instrumentation, which ultimately required a surgical revision. Four months after the revision, the patient was pain-free and computed tomography scan showed a good evolution of arthrodesis, preserved alignment, and no new fracture. 28 Other case reports that surgical treatment may be required in some patients with SCD who develop a kyphotic deformity. 30,31 In 1994, a Saudi Arabian article reported a case of an acute kyphosis with incomplete paraplegia in a patient secondary to ischemic necrosis of 2 vertebral bodies. The patient’s neurologic deficit was fixed with decompression and stabilization. 30 There are several other studies describing surgical interventions in SCD patients to treat skeletal extravertebral manifestations such as ischemic epiphyseal necrosis. 2,28,29
To prevent vaso-occlusive crises in SCD patients during spine surgery, several anesthetic factors should be considered, for example, oxygen delivery, volume status, temperature, and circulatory stasis. Hypoxia in the perioperative period is important to avoid in order to ensure that vaso-occlusive crises do not occur intraoperatively. 30 Anesthesiologists should attempt to maintain a higher oxygen pressure, thereby lowering the concentration of molecules in the T quaternary structure and reduced the propensity of red blood cells to polymerize. 31
Dehydration is also considered to be a trigger of vaso-occlusive, and therefore, adequate hydration is critical during the intraoperative period. 30 Reducing intracellular hemoglobin concentration, which has been shown to reduce the propensity for polymerization and sickling, can be achieved by high fluid intake, sodium restriction, and use of an antidiuretic in the preoperative and perioperative period. 31 Avoiding circulatory stasis and hypothermia is the anesthesiologist’s another important goal during surgery in SCD patients, for the same reason. 6 Rehabilitation is the postoperative period decreases stasis and perfusion, and has also been shown to lessen the occurrence of vaso-occlusive crisis. 30
Since there is a higher rate of osteoporosis of spine in SCD patients, implants such as pedicle screws may lose purchase and eventually pull out, which explains the high rate of instrument failure in this population. 32 Methods to tighten the pedicle screws include correcting for anticipated loosening by using larger diameter screws, expanding screws, screws coated with osteoinductive material, and augmenting of pedicle screws fixation with acrylic cement (polymethylmethacrylate) or with resorbable cement. 32 -35
Conclusion
SCD can markedly affect the musculoskeletal system and is responsible for a large burden of morbidity related to spinal pathology in this population. Though information about the relationship between SCD and spine pathology is lacking, it is well understood that the spine undergoes the same disease processes as the rest of the bones in the body of a patient with SCD. These disease processes include vaso-occlusive crises and microinfarction, osteomyelitis, and osteoporosis, all of which lead to both acute and chronic presentations. One key clinical point to remember is that oftentimes these pathologies are difficult to distinguish from each other given the overlap in inflammatory markers and clinical symptoms. Nonetheless, the majority of SCD spine pathology can be treated conservatively with rest, symptomatic therapy, antibiotics, and orthosis. It is preferable to avoid surgery if possible as these are patients have a higher risk of developing perioperative complications, including surgical site infection, and the stress of surgery and anesthesia can trigger vaso-occlusive crises in the perioperative setting. If indicated, surgery may be necessary for certain SCD spine pathology. This is often the case in patients who fail to respond to 6 to 8 weeks of antibiotics for a spinal abscess. With careful planning and technique of anesthesia and surgery, spine pathology from SCD can be effectively treated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.