
Abstract
Study Design:
Retrospective cohort study.
Objective:
Malnutrition has been shown to be a risk factor for poor perioperative outcomes in multiple surgical subspecialties, but few studies have specifically investigated the effect of hypoalbuminemia in patients undergoing operative treatment of metastatic spinal tumors. The aim of this study was to assess the role of hypoalbuminemia as an independent risk factor for 30-day perioperative mortality and morbidity after surgical decompression of metastatic spinal tumors using the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database from 2011 to 2014.
Methods:
We identified 1498 adult patients in the ACS-NSQIP database who underwent laminectomy and excision of metastatic extradural spinal tumors. Patients were categorized into normoalbuminemic and hypoalbuminemic (ie, albumin level <3.5 g/dL) groups. Univariate and multivariate regression analyses were performed to examine the association between preoperative hypoalbuminemia and 30-day perioperative mortality and morbidity. Subgroup analysis was performed in the hypoalbuminemic group to assess the dose-dependent effect of albumin depletion.
Results:
Hypoalbuminemia was associated with increased risk of perioperative mortality, any complication, sepsis, intra- or postoperative transfusion, prolonged hospitalization, and non-home discharge. However, albumin depletion was also associated with decreased risk of readmission. There was an albumin level–dependent effect of increasing mortality and complication rates with worsening albumin depletion.
Conclusions:
Hypoalbuminemia is an independent risk factor for perioperative mortality and morbidity following surgical decompression of metastatic spinal tumors with a dose-dependent effect on mortality and complication rates. Therefore, it is important to address malnutrition and optimize nutritional status prior to surgery.
Introduction
In the United States, approximately 1.66 million new cases of cancer are diagnosed each year. Up to 84% of cancer patients develop bony metastasis, with the most common site of metastasis being the spine. 1 -5 Spinal metastases develop in approximately 18 000 patients in North America each year. 5 -7 Surgical treatment of metastatic spinal tumors is often palliative, with the goal of decompressing neural structures, alleviating pain, preventing deformity, and encouraging patient mobilization. 3,8 -12 However, operative treatment of spinal tumors often involves extensive procedures with high rates of perioperative complications that can significantly increase health care costs. 1,2,13 In addition, cancer patients who develop spinal metastasis tend to be a frail cohort with multiple medical comorbidities and poor functional status that are independently associated with high complication rates and health care resource utilization as well. 4,9,14 -16
The role of malnutrition in perioperative complications following orthopedic surgery has received increasing attention in recent literature. 17 -21 Malnutrition is common in cancer patients, especially in patients with late-stage cancer who are suffering from cachexia. 22 The pathophysiology of malnutrition in cancer patients is complex, involving host-tumor interactions, anticancer therapies, inflammatory cytokines, increased energy requirements, and caloric losses despite normal food intake. 23 -25
Serum albumin level is a recognized parameter of assessing nutritional status, as well as disease severity and progression in cancer patients. 26 Hypoalbuminemia has been extensively studied as a prognostic indicator for poor surgical outcomes after spinal surgery, 21,26 -30 but few studies have examined hypoalbuminemia alone as an independent risk factor for perioperative complications following surgical decompression of spinal tumors. 31 In this study, we aim to assess the impact of hypoalbuminemia on 30-day perioperative mortality and morbidity in patients undergoing laminectomy for excision of metastatic spinal tumors using a nationwide surgical outcomes database.
Materials and Methods
ACS-NSQIP Database
This was a retrospective analysis of prospectively collected data from 2011 to 2014 in the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database. 32 The ACS-NSQIP is a national database of 30-day postoperative morbidity and mortality outcomes from more than 500 institutions in the United States. The database includes more than 300 variables on patient demographic, preoperative, intraoperative, and early postoperative variables. 32
Cohort Selection
A total of 1498 adult patients aged 18 years or older undergoing laminectomy and excision of metastatic extradural spinal tumors were identified and included in our cohort. Patients with intradural spinal tumors or primary tumors of the spine were excluded. Primary spinal tumors tend to be intradural and benign in nature, therefore constituting a different patient cohort at baseline than patients with spinal metastases. Cases missing preoperative albumin levels were excluded.
Baseline Patient Characteristics
Baseline patient characteristics included patient demographics, medical comorbidities, preoperative condition, and operative variables. Patient demographics included sex, race, and age. Medical comorbidities included a history of obesity (body mass index ≥30 kg/m2), diabetes, smoking within 1 year of surgery, a history of chronic obstructive pulmonary disease or ventilator dependence within 48 hours prior to surgery, use of hypertensive medication within 30 days prior to surgery or a history of chronic heart failure, dialysis within 2 weeks prior to surgery or acute renal failure within 24 hours prior to surgery, acute or chronic bleeding disorder, and chronic steroid use within 30 days prior to surgery. Preoperative condition was indicated by variables including American Society of Anesthesiologists (ASA) classification ≥3, presence of dyspnea at rest within 30 days prior to surgery, functional status (independent, partial, or total dependence), a history of ≥10% unintentional weight loss during the 6 months prior to surgery, anemia (hematocrit <40% in males and <36% in females), preoperative transfusion of ≥1 unit of packed red blood cells or whole blood within 72 hours prior to surgery, and thrombocytopenia (platelets <150 000). Operative variables included whether the procedure was urgent or emergent, and whether a concurrent fusion was performed with the decompression. The variable of interest was the preoperative serum albumin level. Hypoalbuminemia was defined as a serum albumin level <3.5 g/dL.
Thirty-Day Perioperative Outcomes
Primary outcome measures in this study were mortality and other perioperative complications occurring within 30 days following surgery. Complications included reoperation, operative site complications (deep surgical site infection, organ space infection, or wound dehiscence), cardiac complications (cardiac arrest requiring cardiopulmonary resuscitation or myocardial infarction), pulmonary complications (pneumonia, postoperative reintubation, or failure to wean from a ventilator after 48 hours), renal complications (progressive renal insufficiency or acute renal failure), venous thromboembolism (pulmonary embolism or deep vein thrombosis), sepsis, urinary tract infection (UTI), intra- or postoperative transfusion of packed red blood cells or whole blood, prolonged length of stay (LOS) ≥10 days, non-home discharge, and unplanned readmission.
Statistical Analysis
Univariate analysis was performed on patient demographics and baseline characteristics using Pearson’s χ2 test. Fischer’s exact test was used when appropriate. Multivariate (MVR) regression models were performed while adjusting for patient demographics and baseline characteristics in order to identify the effect of hypoalbuminemia on 30-day perioperative mortality and morbidity. Demographic, medical comorbidity, and operative variables that were statistically different between study groups were included as covariates in the MVR regression analysis. Subgroup analysis was performed in the hypoalbuminemic group by stratifying patients into approximate quartiles based on preoperative albumin levels. Univariate and MVR regression analyses were performed to identify the effect of worsening albumin depletion on 30-day perioperative mortality and morbidity. Odds ratios (ORs) and 95% confidence intervals (CIs) were reported. Statistical significance was set at P = .05. All statistical analysis was performed using SAS Studio Version 3.4 (SAS Institute Inc, Cary, NC).
Results
Patient Baseline Characteristics
In our cohort of 1498 patients, the mean preoperative albumin level was 3.66 g/dL with a standard deviation of 0.66 g/dL (Figure 1). Hypoalbuminemia was present in 34.2% (512/1498) of patients. Baseline patient characteristics were significantly different between the normoalbuminemic and hypoalbuminemic groups (Table 1). There were significant differences in medical comorbidities, including diabetes (P = .010), smoking (P = .002), pulmonary comorbidity (P < .001), renal comorbidity (P = .018), bleeding disorder (P < .001), and chronic steroid use (P < .001). There were significant differences in preoperative patient condition, including ASA classification (P < .001), dyspnea at rest (P < .001), functional status (P < .001), unintentional weight loss (P < .001), anemia (P < .001), preoperative transfusion (P < .001), and thrombocytopenia (P < .001). The proportion of urgent or emergent surgeries was also significantly different between the 2 groups (P < .001).
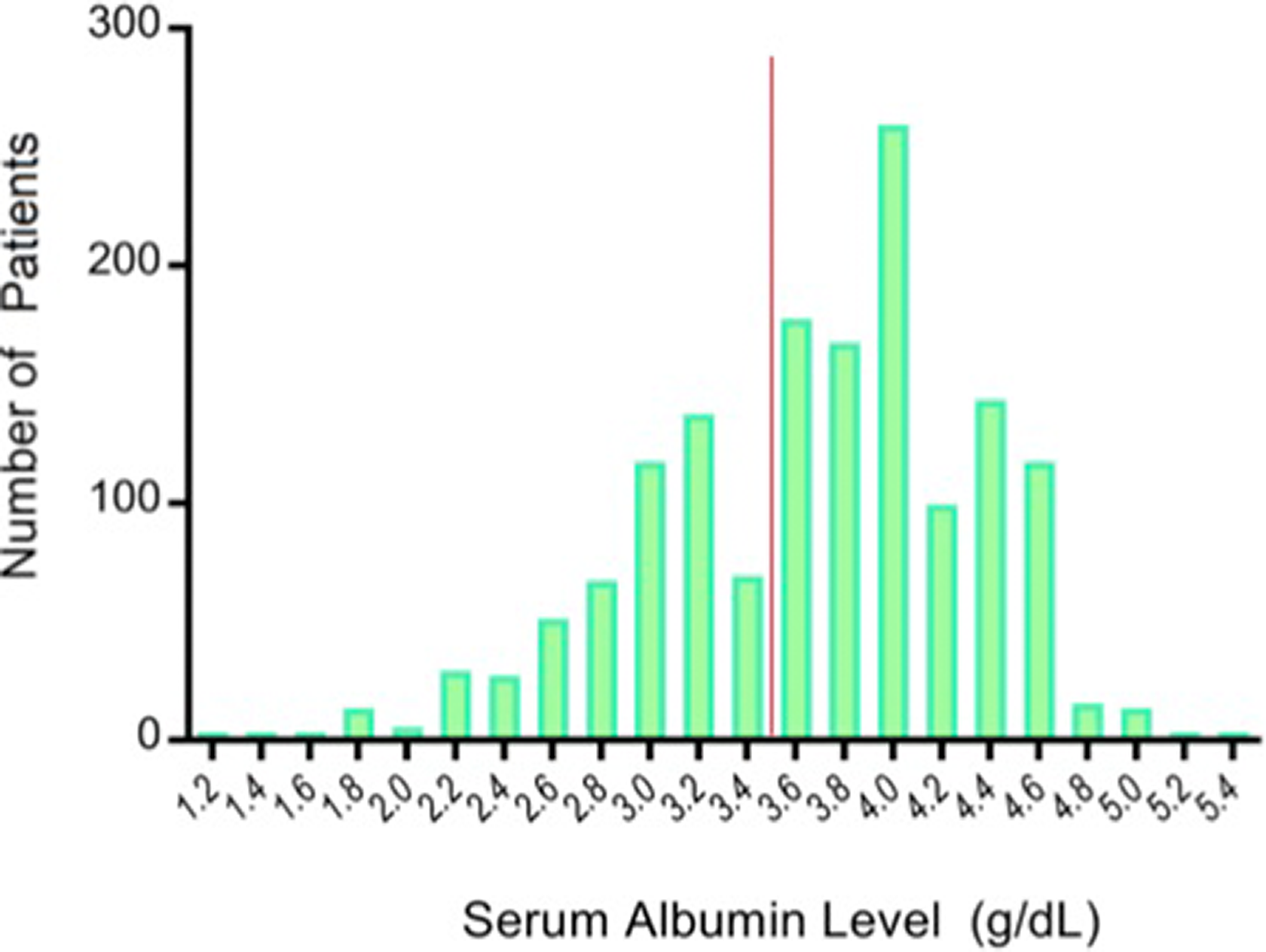
Preoperative serum albumin levels of 1498 patients. The red line represents the cutoff for hypoalbuminemia (ie, albumin ≤3.5 g/dL). The mean albumin level was 3.66 g/dL with a standard deviation of 0.66 g/dL. Hypoalbuminemia was present in 34.2% (512/1498) of patients.
Baseline Patient Characteristics in the Normoalbuminemic and Hypoalbuminemic Groups, Including Medical Comorbidities at the Time of Surgery, Preoperative Condition, and Operative Variables.
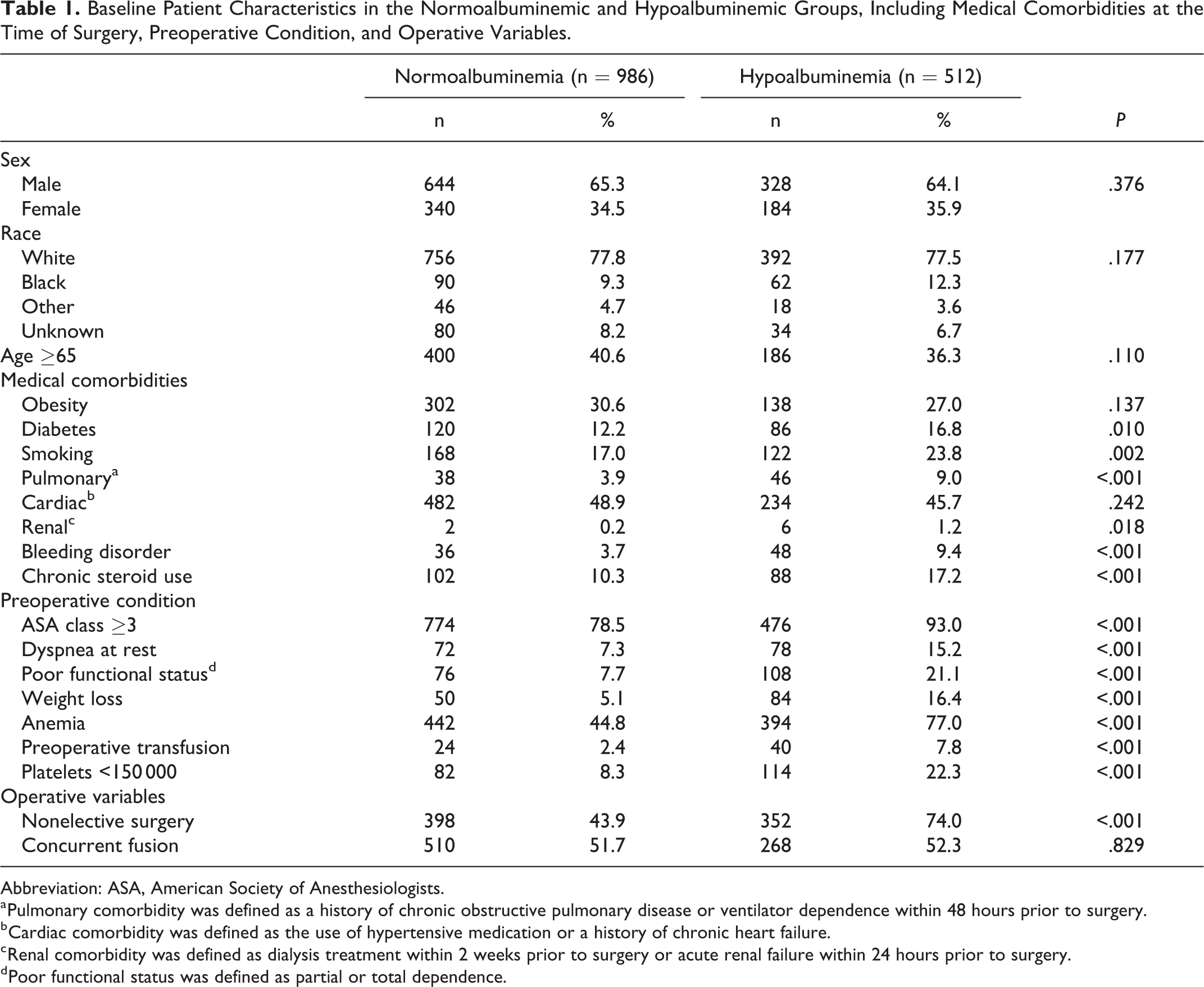
Abbreviation: ASA, American Society of Anesthesiologists.
a Pulmonary comorbidity was defined as a history of chronic obstructive pulmonary disease or ventilator dependence within 48 hours prior to surgery.
b Cardiac comorbidity was defined as the use of hypertensive medication or a history of chronic heart failure.
c Renal comorbidity was defined as dialysis treatment within 2 weeks prior to surgery or acute renal failure within 24 hours prior to surgery.
d Poor functional status was defined as partial or total dependence.
Univariate Analysis
Results of the univariate analysis are summarized in Table 2. There was a statistically significant difference in 30-day mortality between the 2 groups, with a rate of 3.3% in the normoalbuminemic group and 17.2% in the hypoalbuminemic group (P < .001). There were also significant differences in perioperative complications. Hypoalbuminemic patients had a higher rate of any perioperative complication (hypoalbuminemic, 77.3%; normoalbuminemic, 48.1%; P < .001). Specifically, hypoalbuminemic patients had higher rates of pulmonary complications (P = .025), venous thromboembolism (P = .023), sepsis (P < .001), perioperative transfusion (P < .001), prolonged LOS (P < .001), and non-home discharge (P < .001). There were no significant differences in reoperation, surgical site complications, cardiac complications, renal complications, UTI, and unplanned readmission.
Univariate Analysis of 30-Day Perioperative Mortality and Morbidity in Normoalbuminemic and Hypoalbuminemic Patients.
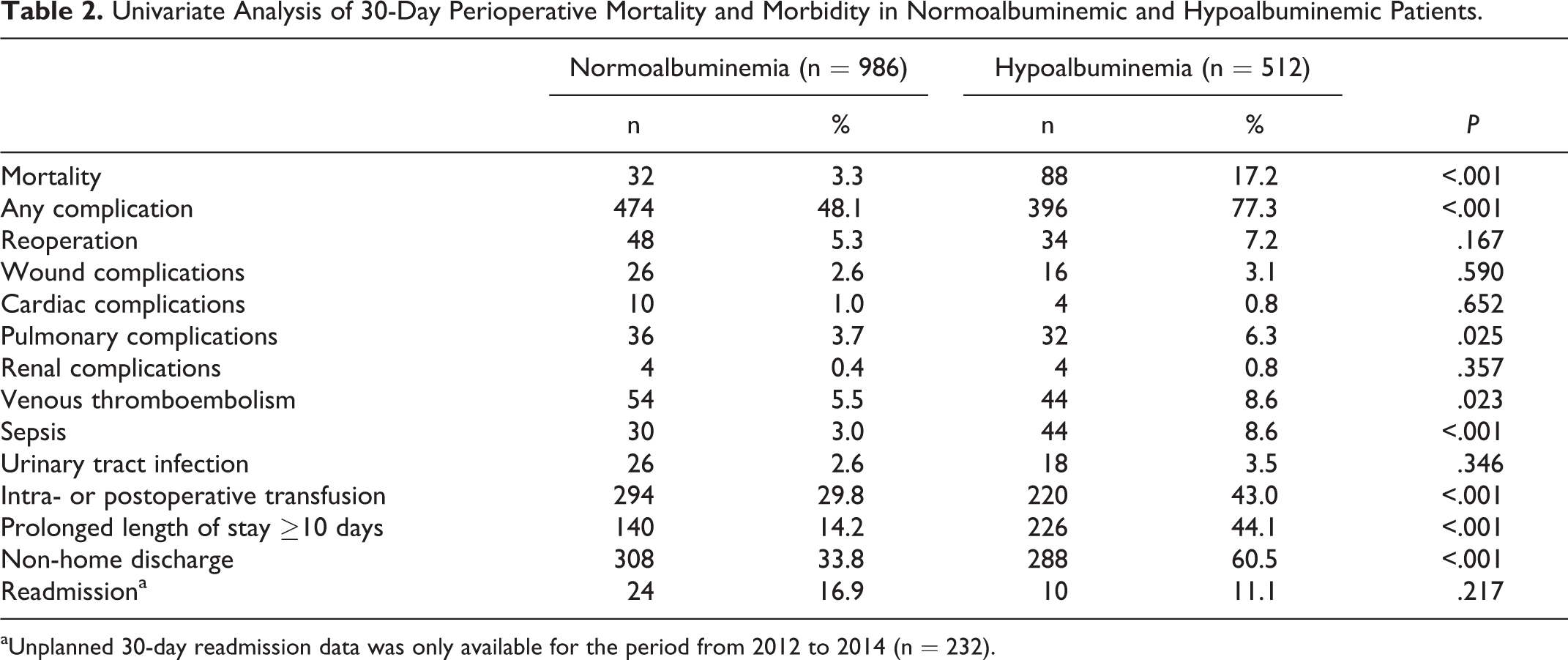
aUnplanned 30-day readmission data was only available for the period from 2012 to 2014 (n = 232).
Multivariate Regression Analysis
Results of the MVR regression analysis are summarized in Figure 2 and Table 3. Hypoalbuminemic patients had a higher risk of perioperative mortality (adjusted OR = 5.20; CI = 3.36-8.04; P < .001), any complication (adjusted OR = 3.16; CI = 2.44-4.10; P < .001), sepsis (adjusted OR = 3.05; CI = 1.88-4.92; P < .001), intra- or postoperative transfusion (adjusted OR = 1.43; CI = 1.11-1.83; P = .005), prolonged LOS (adjusted OR = 4.32; CI = 3.31-5.63; P < .001), and non-home discharge (adjusted OR = 2.92; CI = 2.28-3.73; P < .001). In contrast, the risk of unplanned readmission was lower in patients with hypoalbuminemia (adjusted OR = 0.18; CI = 0.05-0.63; P = .007).
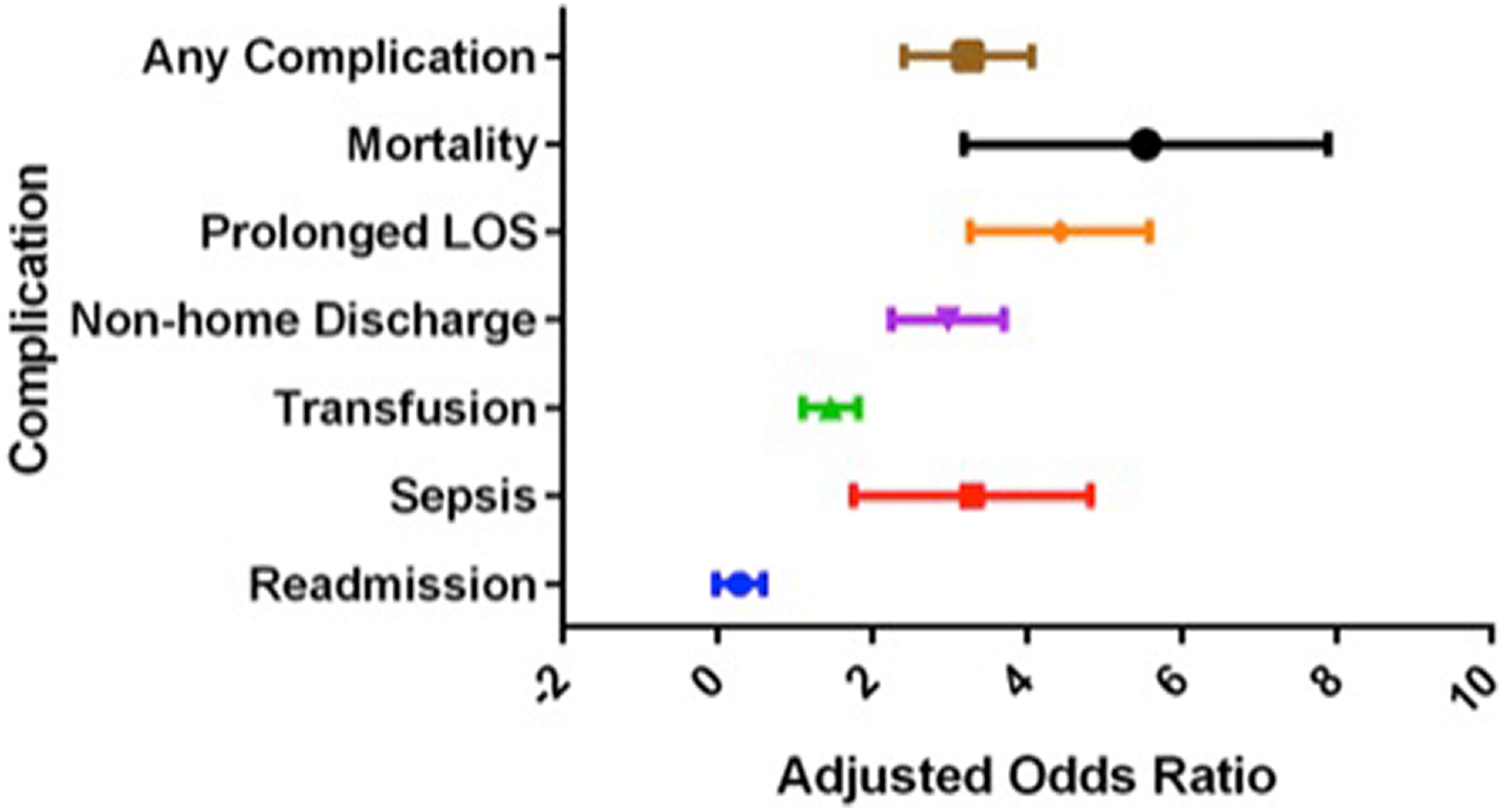
Multivariate regression analysis of perioperative mortality and complications that were significantly associated with hypoalbuminemia. Adjusted odds ratios are illustrated with 95% confidence intervals. LOS, length of stay.
Multivariate Regression Analysis of the Effect of Hypoalbuminemia on Perioperative Mortality and Morbidity Using Normoalbuminemic Patients as the Reference Groupa.
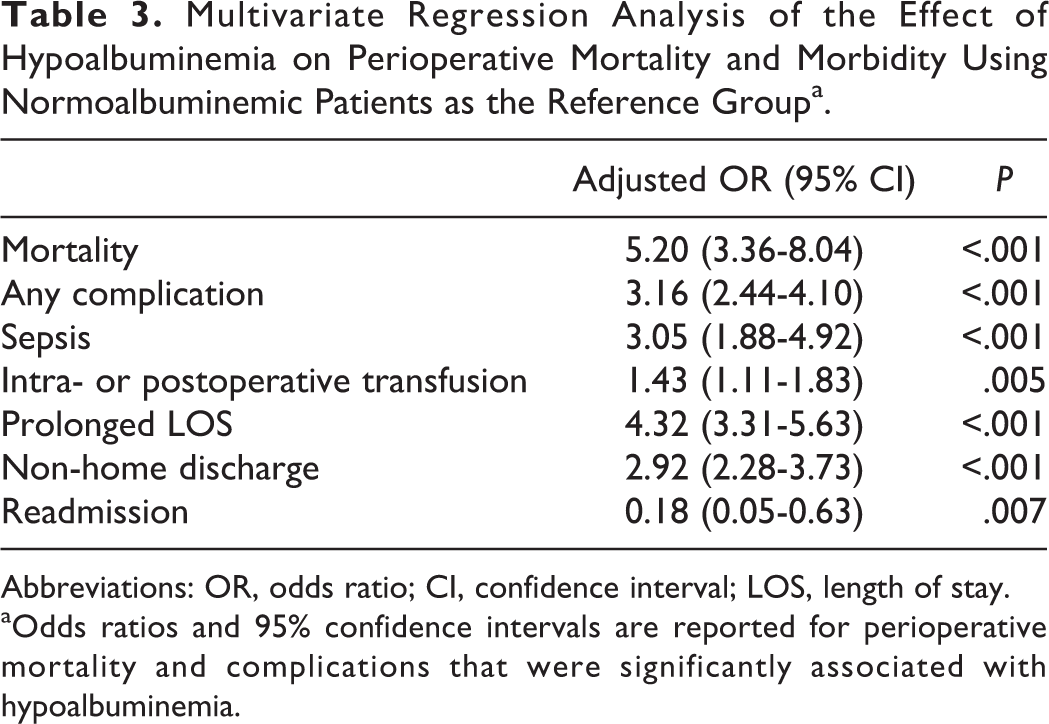
Abbreviations: OR, odds ratio; CI, confidence interval; LOS, length of stay.
aOdds ratios and 95% confidence intervals are reported for perioperative mortality and complications that were significantly associated with hypoalbuminemia.
Subgroup Analysis
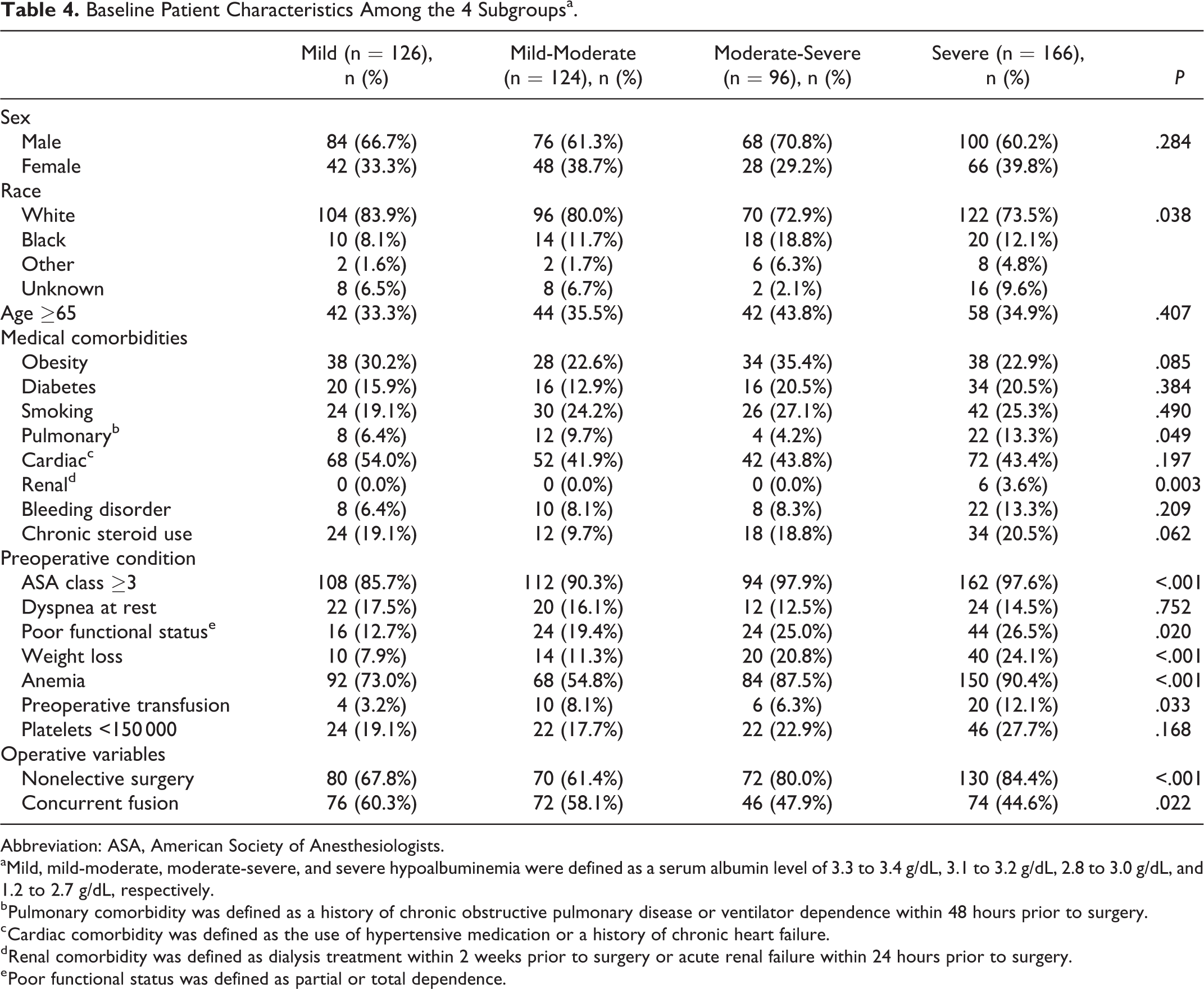
Patients in the hypoalbuminemic group (n = 512) were stratified into approximately quartiles based on preoperative albumin levels. The mild hypoalbuminemia group consisted of 126 patients with serum albumin levels of 3.3 to 3.4 g/dL. The mild-moderate hypoalbuminemia group included 124 patients with serum albumin levels of 3.1 to 3.2 g/dL. The moderate-severe hypoalbuminemia group consisted of 96 patients with serum albumin levels of 2.8 to 3.0 g/dL. The severe hypoalbuminemia group consisted of 166 patients with serum albumin levels of 1.2 to 2.7 g/dL. There were significant differences in race (P = .038), pulmonary comorbidity (P = .049), renal comorbidity (P = .003), ASA classification (P < .001), preoperative functional status (P = .020), unintentional weight loss (P < .001), preoperative anemia (P < .001), and nonelective surgery (P < .001) among the subgroups (Table 4).
Baseline Patient Characteristics Among the 4 Subgroupsa.
Abbreviation: ASA, American Society of Anesthesiologists.
aMild, mild-moderate, moderate-severe, and severe hypoalbuminemia were defined as a serum albumin level of 3.3 to 3.4 g/dL, 3.1 to 3.2 g/dL, 2.8 to 3.0 g/dL, and 1.2 to 2.7 g/dL, respectively.
b Pulmonary comorbidity was defined as a history of chronic obstructive pulmonary disease or ventilator dependence within 48 hours prior to surgery.
c Cardiac comorbidity was defined as the use of hypertensive medication or a history of chronic heart failure.
d Renal comorbidity was defined as dialysis treatment within 2 weeks prior to surgery or acute renal failure within 24 hours prior to surgery.
e Poor functional status was defined as partial or total dependence.
Results of the univariate subgroup analysis are shown in Table 5. There was a consistent relationship between worsening hypoalbuminemia and higher rates of perioperative mortality (mild, 6.4%; mild-moderate, 16.1%; moderate-severe, 18.8%; severe, 25.3%; P < .001) and any complication (mild, 65.9%; mild-moderate, 71.0%; moderate-severe, 79.2%; severe, 89.8%; P < .001). In particular, patients with more severe albumin depletion had higher rates of pulmonary complications (mild, 3.2%; mild-moderate, 3.2; moderate-severe, 8.3%; severe, 9.6%; P = .041) and prolonged LOS (mild, 30.2%; mild-moderate, 41.9%; moderate-severe, 43.8%; severe, 56.5%; P < .001). There were also significant differences in the rates of venous thromboembolism (P = .037), sepsis (P = .036), UTI (P = .025), and non-home discharge (P = .026) among the subgroups, but without a consistent trend in the relationship between the severity of albumin depletion and complication rates. There were no significant differences among the subgroups in terms of reoperation, surgical site complications, cardiac complications, renal complications, perioperative transfusion, and unplanned readmission.
Univariate Analysis of 30-Day Perioperative Mortality and Morbidity in Patients With Varying Severities of Hypoalbuminemiaa.
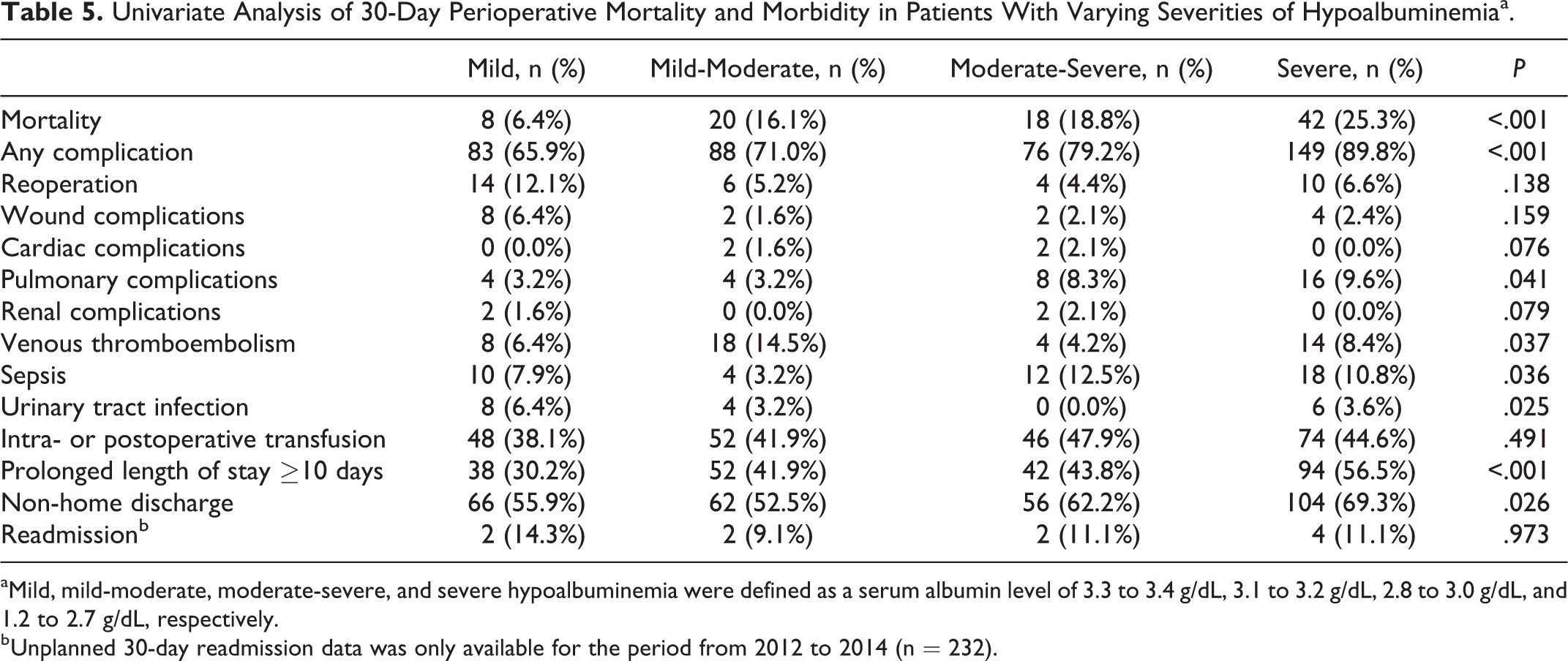
aMild, mild-moderate, moderate-severe, and severe hypoalbuminemia were defined as a serum albumin level of 3.3 to 3.4 g/dL, 3.1 to 3.2 g/dL, 2.8 to 3.0 g/dL, and 1.2 to 2.7 g/dL, respectively.
b Unplanned 30-day readmission data was only available for the period from 2012 to 2014 (n = 232).
On MVR analysis, patients with mild hypoalbuminemia were used as the reference group. Worsening hypoalbuminemia was consistently associated with increased risk of mortality and any complication (Table 6, Figure 3). Patients with severe hypoalbuminemia had significantly higher risk of prolonged LOS than patients with mild hypoalbuminemia (adjusted OR = 2.52; CI = 1.46-4.33; P < .001). Patients with mild-moderate hypoalbuminemia had significantly higher risk of venous thromboembolism than patients with mild hypoalbuminemia (adjusted OR = 3.03; CI = 1.17-7.89; P = .023). However, patients with moderate-severe and severe hypoalbuminemia did not have a significantly different risk of venous thromboembolism than patients with mild hypoalbuminemia.
Multivariate Regression Analysis of the Effect of Varying Severities of Hypoalbuminemia on 30-Day Perioperative Mortality and Morbidity Using Mild Hypoalbuminemia (ie, Serum Albumin Level of 3.3-3.4 g/dL) as Referencea.
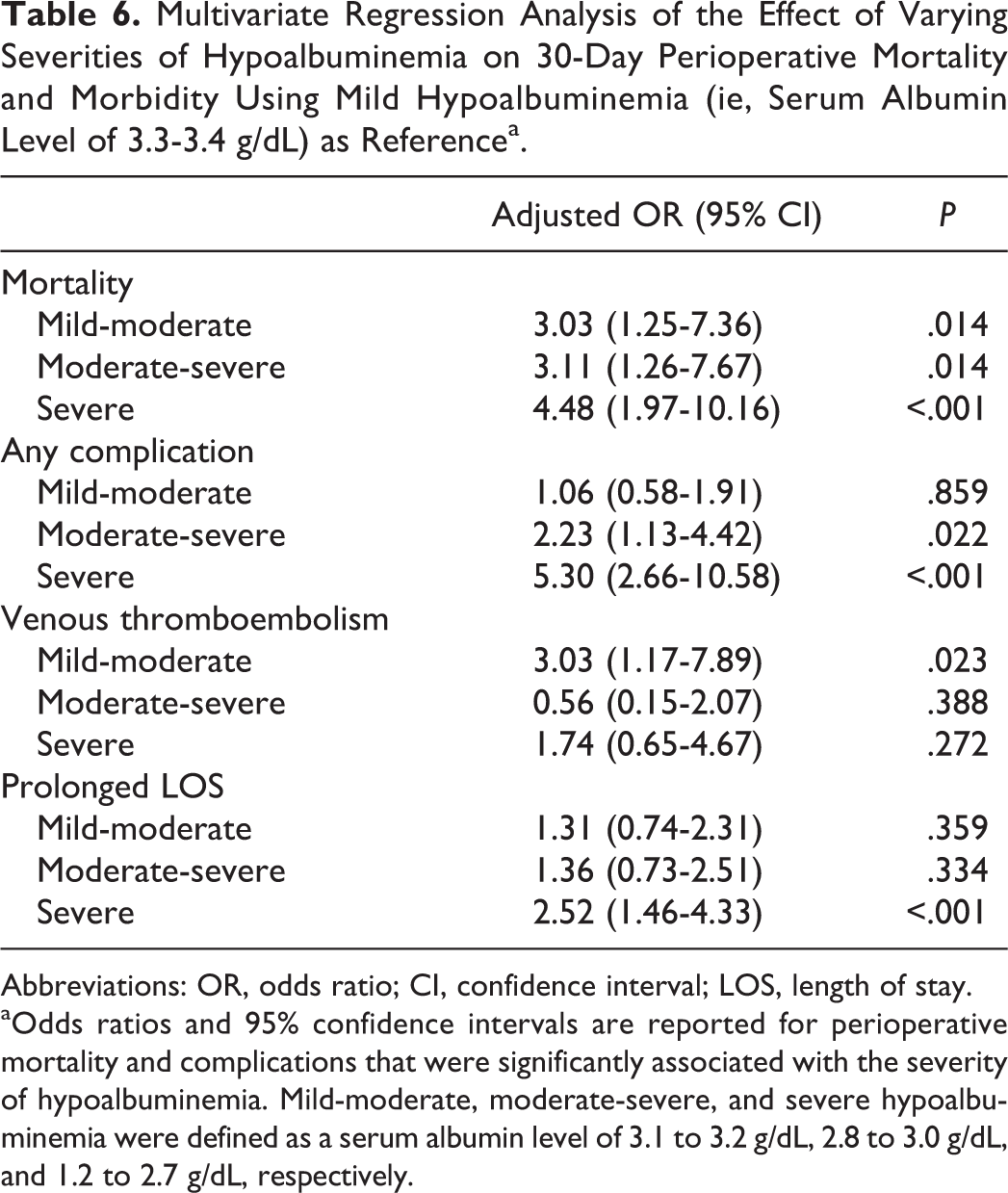
Abbreviations: OR, odds ratio; CI, confidence interval; LOS, length of stay.
aOdds ratios and 95% confidence intervals are reported for perioperative mortality and complications that were significantly associated with the severity of hypoalbuminemia. Mild-moderate, moderate-severe, and severe hypoalbuminemia were defined as a serum albumin level of 3.1 to 3.2 g/dL, 2.8 to 3.0 g/dL, and 1.2 to 2.7 g/dL, respectively.
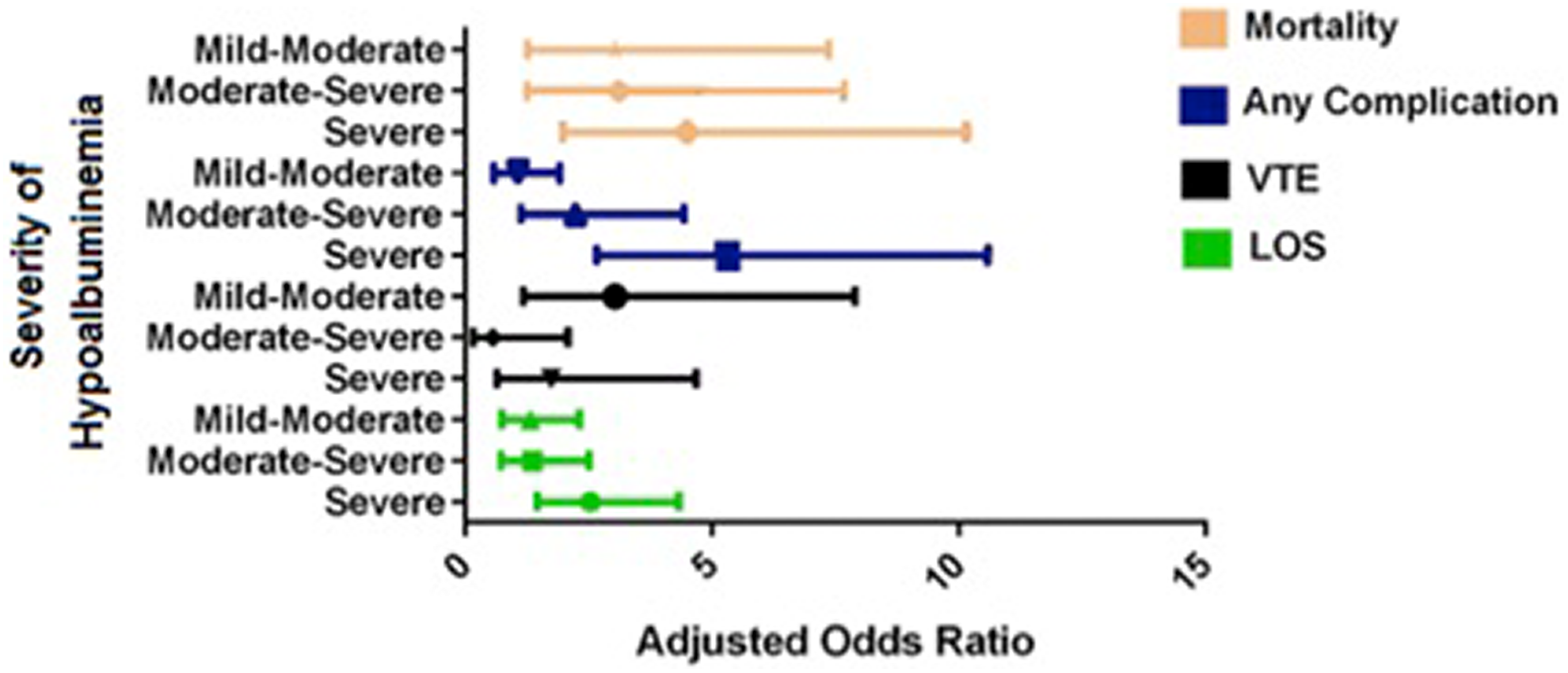
Multivariate regression analysis of perioperative mortality and complications that were significantly associated with varying severities of hypoalbuminemia using mild hypoalbuminemia (ie, serum albumin level of 3.3-3.4 g/dL) as the reference group. Adjusted odds ratios are reported with 95% confidence intervals. Mild-moderate, moderate-severe, and severe hypoalbuminemia were defined as a serum albumin level of 3.1 to 3.2 g/dL, 2.8 to 3.0 g/dL, and 1.2 to 2.7 g/dL, respectively. VTE, venous thromboembolism; LOS, length of stay.
Discussion
Malnutrition is common in the cancer patient population and has been associated with higher rates of complications in patients with metastatic spinal disease. 27,29 -31 In this retrospective study of 1498 patients in the ACS-NSQIP database who underwent surgical decompression for metastatic extradural spinal tumors, we demonstrated that hypoalbuminemia is an independent risk factor for 30-day perioperative mortality and morbidity. Albumin levels below 3.5 g/dL were associated with increased risk of perioperative mortality, any complication, sepsis, intra- or postoperative transfusion, prolonged hospitalization, and non-home discharge. These findings support serum albumin level as a valuable prognostic measure for poor surgical outcomes in patients with metastatic spinal tumors.
Hypoalbuminemia was associated with a 5-fold increase in the risk of 30-day mortality, and our subgroup analysis demonstrated that there was an albumin level–dependent association between the severity of albumin depletion and mortality rate. The perioperative mortality rate in our hypoalbuminemic group was 17.2%, which is higher than previously reported rates of 3% to 13%. 9,13,20,33 -35 Hypoalbuminemic patients also experienced a 3-fold increased risk of any perioperative complication compared with normoalbuminemic patients, with an albumin level–dependent relationship between worsening albumin depletion and complication rate. The rate of any complication in hypoalbuminemic patients was 77.3%, which is slightly higher than previously reported rates of 10% to 76%. 1,15,30,36 -40 These results are consistent with malnutrition being a risk factor for poor early postoperative outcomes.
Patients with hypoalbuminemia had a 1.4 times increased risk of intra- or postoperative transfusion. The incidence of perioperative blood loss requiring transfusion was 43.0% in the hypoalbuminemic group. Mean blood loss after surgical decompression of spinal tumors ranges from 500 to 2300 mL and these procedures are associated with high transfusion rates. 1,20,41 -43 Minimizing blood loss and perioperative transfusions not only reduces health care costs 14,15,44,45 but may also play a role in reducing perioperative mortality. 46 -50 Perioperative transfusion of allogeneic blood has also been associated with higher infection rates following various orthopedic procedures, 48,51 -55 and in this study, 48.6% of patients with perioperative sepsis had received a perioperative blood transfusion. Therefore, our results support optimization of albumin levels preoperatively in order to minimize perioperative transfusions and their associated complications.
Hypoalbuminemia was associated with an increased risk of perioperative sepsis. The incidence of perioperative sepsis in the hypoalbuminemic group was 8.6%. Patients with metastatic spinal tumors are predisposed to infection due to multiple risk factors, including neutropenia, immunosuppression from oncologic therapies or corticosteroids, and compromise of epithelial cell anatomic barriers from radiation therapy. 56 In addition, serum albumin is a negative acute phase reactant and low albumin concentrations may be a marker for subclinical illness. 57 -59 The presence of malnutrition in the setting of these risk factors places patients with metastatic spinal tumors at high risk for perioperative sepsis.
Hypoalbuminemia was also associated with a 4-fold and nearly a 3-fold increased risk of prolonged hospitalization and non-home discharge, respectively. These findings are consistent with prior studies that have identified malnutrition as an independent risk factor for prolonged hospitalization. 19,60 Past studies have reported an increase in LOS by 3 to 7 days for any complication after surgical decompression of spinal tumors. 7,61 Prolonged hospitalization is associated with worse perioperative outcomes, including an increased risk of hospital-acquired conditions and higher overall hospital costs. 2,15,38 It is also a risk factor for non-home discharge, 62 which occurred in approximately 60% of our hypoalbuminemic group. There appeared to be an albumin level–dependent effect, with severe hypoalbuminemia being associated with a 2.5 times increased risk of prolonged hospitalization compared to mild hypoalbuminemia.
Of note, we found that hypoalbuminemia was associated with a lower rate of unplanned 30-day readmissions. This is in contrast to prior studies that have demonstrated an increased risk of readmission in patients with hypoalbuminemia. 19 Patients with metastatic spinal tumors often have multiple medical comorbidities and poor functional status at baseline, putting them at high risk for perioperative mortality. The 30-day mortality rate in our cohort was higher than previously reported, possibly contributing to lower readmission rates. Another contributing factor may have been related to the high proportion of patients discharged to non-home facilities, which likely include palliative care facilities where patients are typically not readmitted to acute care facilities.
The overall association between hypoalbuminemia and perioperative mortality and morbidity following surgical decompression of metastatic spinal tumors supports the implementation of strategies to optimize preoperative albumin levels in this patient population. A proven method of addressing hypoalbuminemia is nutritional supplementation, which has been associated with lower perioperative complication rates in various surgical subspecialties. 63 -65 Unfortunately, nutritional supplementation in the form of total parenteral nutrition (TPN) cannot easily reverse cachexia in cancer patients. 66 Studies have demonstrated that severely malnourished patients may require up to 10 to 14 days of preoperative TPN in order to reduce postoperative complications. 67,68 Furthermore, evidence suggests a possible lack of benefit of TPN in patients who are only mildly or moderately malnourished. 68
There are several limitations to this study. First, the ACS-NSQIP database categorizes patients according to CPT (Current Procedural Terminology) codes, which do not provide information about the location or histology of the primary tumor. The nature of the primary tumor has a significant effect on perioperative mortality and morbidity. 37,42,69 Additionally, the ACS-NSQIP database does not record the presence or number of visceral metastases, which is another important prognostic factor. 70,71 In this study, we did not include other markers that may be better correlated with nutritional status than albumin. For instance, studies have suggested that pre-albumin or transthyretin may be a more accurate marker of nutritional status given its shorter half-life and increased sensitivity to changes in protein level. 72 Last, the ACS-NSQIP database is limited to only 30-day postoperative outcomes and does not include long-term outcomes such as functional or neurological status.
In conclusion, we examined the role of hypoalbuminemia as an independent risk factor for 30-day perioperative mortality and morbidity after surgical decompression of metastatic spinal tumors. Hypoalbuminemia was a risk factor for perioperative mortality, any complication, sepsis, intra- or postoperative transfusion, prolonged hospitalization, and non-home discharge. However, lower readmission rates were seen in patients with hypoalbuminemia. There was also an albumin level–dependent effect with worsening albumin depletion being associated with higher rates of perioperative mortality and any complication. These findings support optimization of nutritional status in patients with metastatic spinal tumors prior to surgical decompression.
Footnotes
Authors’ Note
The article does not contain information about medical device(s)/drug(s). Institutional review board approval was not required for the submitted work at our institution.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.