
Abstract
Study Design
Retrospective Cohort Study.
Objective
Scoring systems for metastatic disease of the spine are used to select patients for surgical treatment based on survival estimation, but it is unknown whether they can be used to predict the outcome of surgery. This study aims to investigate the association between two widely used prognostic scores and the neurologic function after surgery.
Methods
Retrospective analysis of 204 patients with thoracolumbar metastases treated with decompressive surgery at Karolinska University Hospital (2001-2020). Modified Bauer and Tokuhashi scores were categorized based on surgical indication, and post-operative neurological function was assessed using the Frankel scale at two different post-surgery intervals.
Results
Modified Bauer scores ≥2 yielded higher late follow-up Frankel scores (3.9 ± 1.1) than scores <2 (3.5 ± 1.1), P = .03. Modified Tokuhashi scores ≥9 correlated with higher Frankel scores (4.5 ± .9) than scores <9 (3.5 ± 1.1), P < .0001. Both scoring systems positively predicted neurological outcomes at late follow-up, with odds ratios of 1.6 (P = .03) for Bauer and 9.2 (P < .0001) for Tokuhashi. However, only Tokuhashi predicted ambulatory function at late follow-up (P < .0001), demonstrating its utility in prognosticating post-surgical mobility.
Conclusion
Higher modified Bauer and Tokuhashi scores were associated with better neurologic function at last follow-up, as well as greater likelihood of being able to walk again. The Tokuhashi score was found to be more accurate than the modified Bauer score in predicting the neurological outcome after surgery.
Introduction
In the current retrospective study, our objective was to determine the feasibility of using two common prognostic scores as predictive indicators for neurologic outcome following decompressive surgery, in patients with spine metastasis leading to neurologic impairment.
Methods
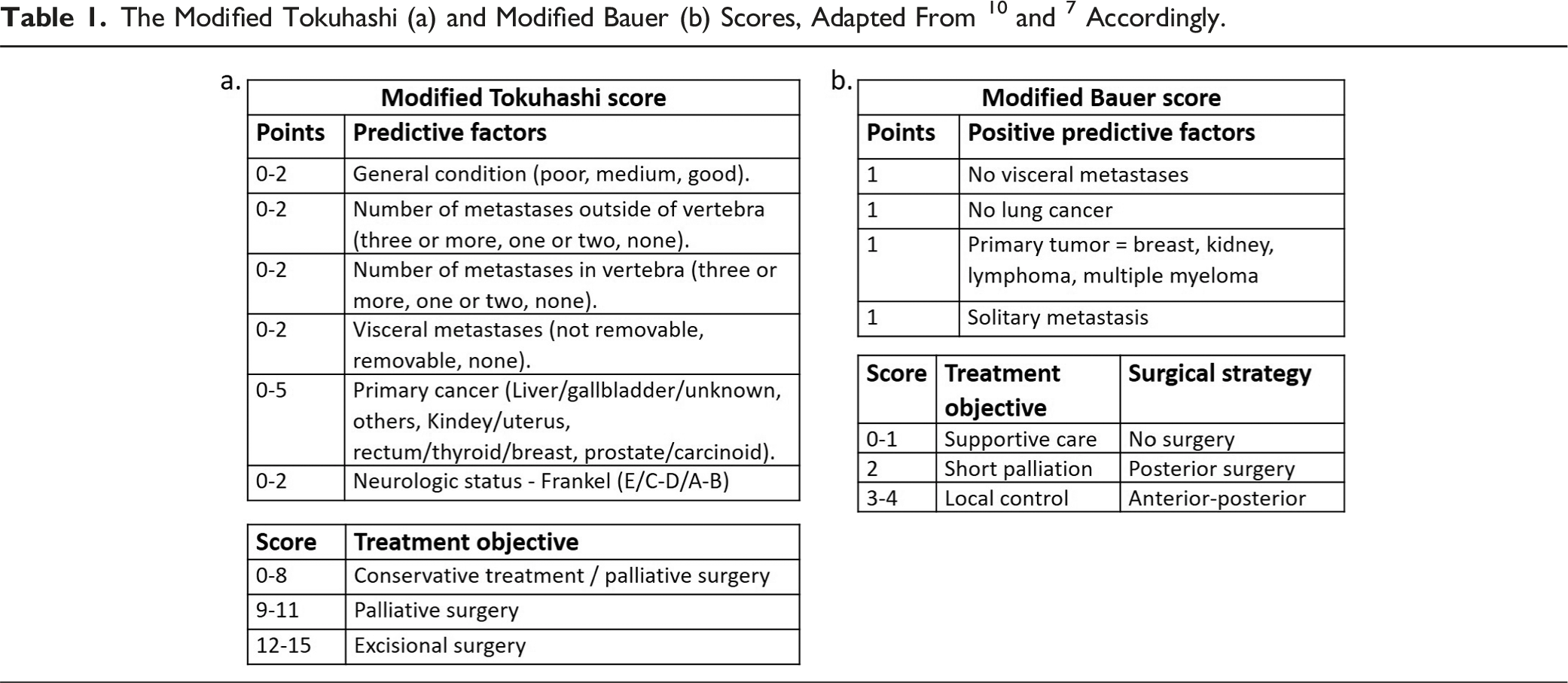
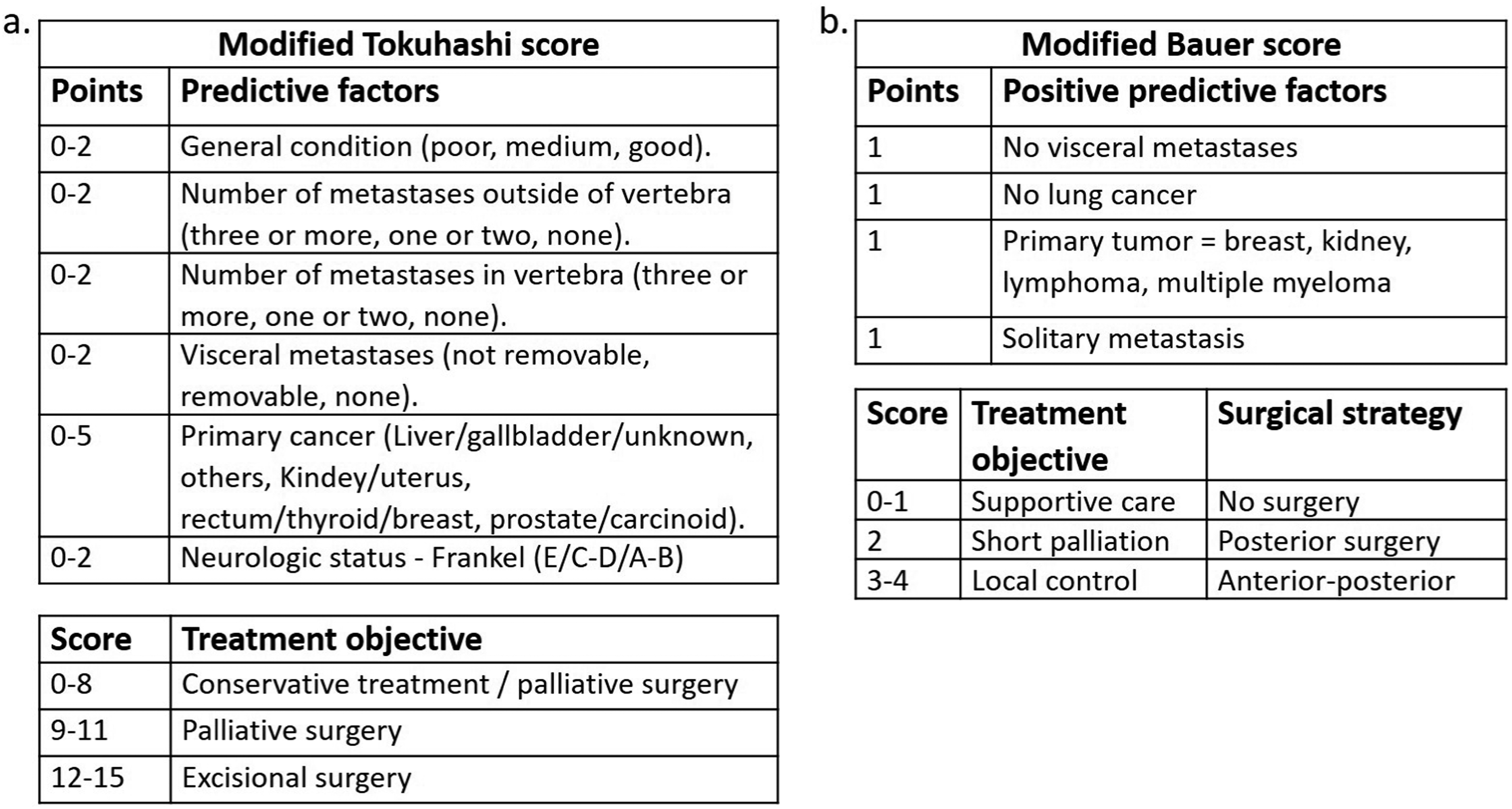
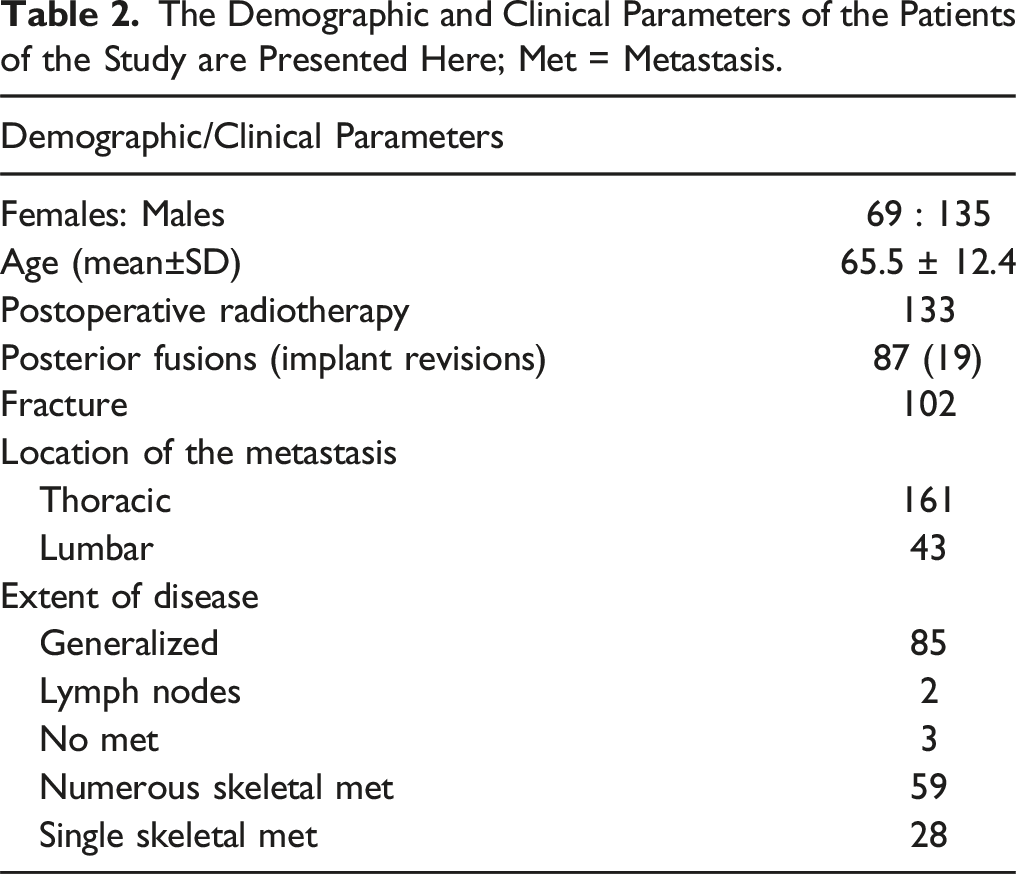
The Demographic and Clinical Parameters of the Patients of the Study are Presented Here; Met = Metastasis.
Data on the survival of these patients were collected. The severity of the disease was assessed using the modified Bauer score (0-4), and the Tokuhashi score (1-15). The Frankel scale, converted to a numeric scale (1-5), was used to evaluate the patients’ neurological status preoperatively, as well as an early (median of 6 weeks) and late (median of 6 months) postoperative follow-up.
We subdivided the modified Bauer/Tokuhashi scores in two groups based on the recommendation for surgery or conservative treatment provided by the scores. For the modified Bauer score, the first group had a score of <2 and the second ≥2; for the modified Tokuhashi score, the groups were <9 and ≥9 respectively. Survival plots and graphs were created using the survival and the ggplot2 packages. The non-parametric unpaired Mann-Whitney-Wilcoxon test (MASS package) was used to compare the mean scores. The Kruskal Wallis test was used to compare the means of multiple groups; if Kruskal Wallis test came out positive, pairwise comparison was performed with Dunn’s test. To determine the predictive value of Bauer and Tokuhashi scores on neurological outcomes, a univariate ordinal (cml) and logistic (logit) regression analysis were performed. Statistical tests (with a level of significance of P < .05) were performed and graphs were generated with R.11
Results
Since both prognostic scores give a recommendation regarding treatment (surgical vs non-surgical), with a cut-off value of 2 for the Bauer and 9 for the Tokuhashi score, we first analyzed whether these scores were associated with the primary outcome of treatment, which is preservation and restoration of the neurological function. We observed that the mean (±SD) numeric Frankel score was higher in the group of patients with a modified Tokuhashi score of ≥9, in comparison to the group that had lower scores at the early [4.1 (±.9) vs 3.7 (±.9)] and at the late follow-up [4.4 (±.9) vs 3.6 (±1.1)], P < .0001 (Figure 1A). For the modified Bauer score of ≥2, the neurologic outcome was slightly higher than if the score was <2 at the early follow-up [3.9 (±1.0) vs 3.7 (±.9), P = .07], a difference that became statistically significant at the late follow-up [3.9 (±1.1) vs 3.6 (±1.1), P = .02] (Figure 1B). Patients that had a preoperative Frankel score of D-E had higher postoperative score at the first follow-up than those that had a preoperative score of A-C [4.3 (±1.0) vs 3.5 (±.7), P < .0001] (Figure 1C). Similar trends were seen at the second follow-up, patients with a score of D-E had a postoperative Frankel score of 4.2 (±1.1) and those with an initial score of A-C had 3.5 (±1.1), P < .0001. The neurologic outcome was not differentially affected by other demographic and clinical parameters such as age (P = .48), sex (P = .89), primary tumor type (P = .49), and location of metastasis (P = .19). Dot plots of postoperative Frankel scores in relationship to the patients’ modified Tokuhashi (A), Bauer (B) and preoperative Frankel (C) scores at first and second follow-up; 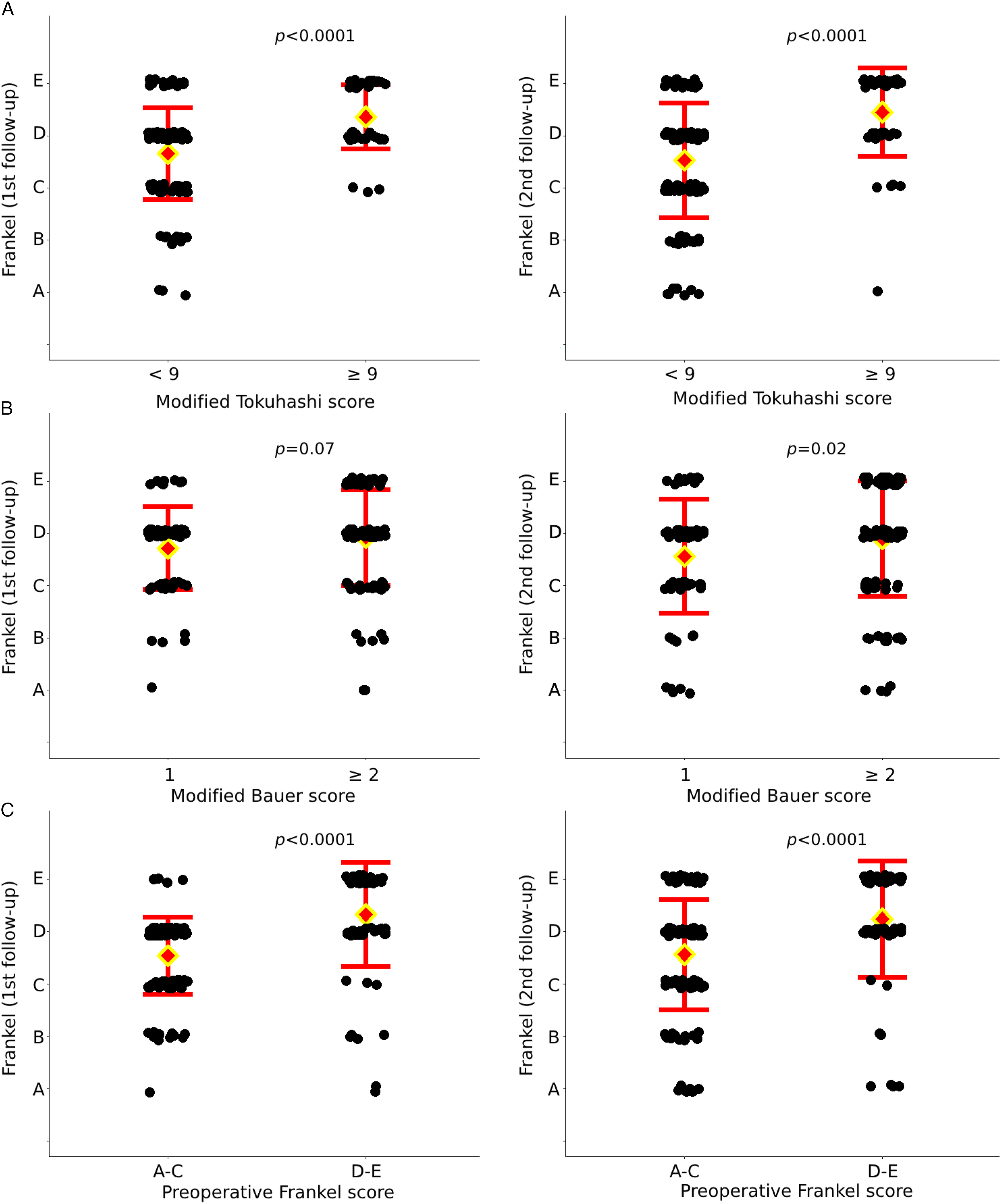
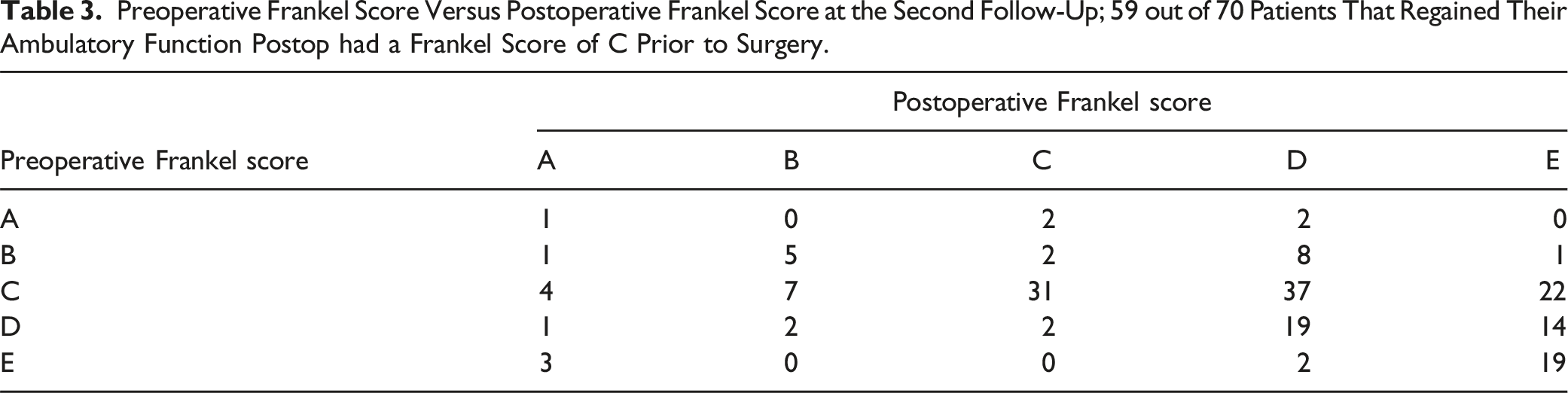
Apart from our review of the neurologic function based on the Frankel scale, we analyzed the results regarding the restoration of the ambulatory capacity, which is often easier to interpret and has a high clinical value. Prior to surgery, 130/201 patients did not have ambulatory capacity, while at the first follow-up that number had decreased to 59/199 (Figure 2A). By the second follow-up, 61/185 patients were non-ambulating, suggesting lasting positive outcomes of treatment. Both the modified Tokuhashi and the modified Bauer scores were shown to be predictors of postoperative neurologic outcome (Figure 2B), with the modified Tokuhashi score exhibiting a stronger predictive capability than the modified Bauer score, as indicated by the OR and CI. At the same time, preoperative ambulatory function (Frankel D or E) was also shown to be a significant predictor of postoperative neurologic outcome (Figure 2B). The OR of modified Tokuhashi was 6.91, higher than that of the preoperative Frankel score, which was 4.62. The univariate logistic regression analysis showed that the modified Tokuhashi score and the preoperative Frankel score of D/E were positive predictors of postoperative ambulatory capacity; the modified Bauer score was however not a predictor (Figure 2C). Table 3 compares the neurological function of the patients prior to surgery with the neurological function that they had at the second follow-up. The majority of the patients that could not ambulate prior to surgery but regained their ambulatory capacity postoperatively, had a preoperative Frankel score of C (84%). Few patients deteriorated in their neurologic function scores after surgery, most of the patients experienced an improvement (supplementary Table). Paired dot plot of ambulatory (Frankel D-E) and non-ambulatory (Frankel A-C) patients, pre- and post-surgery (A), univariate ordinal regression for postoperative Frankel score (B) and univariate logistic regression for ambulatory capacity (C) at the second follow-up; Preoperative Frankel Score Versus Postoperative Frankel Score at the Second Follow-Up; 59 out of 70 Patients That Regained Their Ambulatory Function Postop had a Frankel Score of C Prior to Surgery.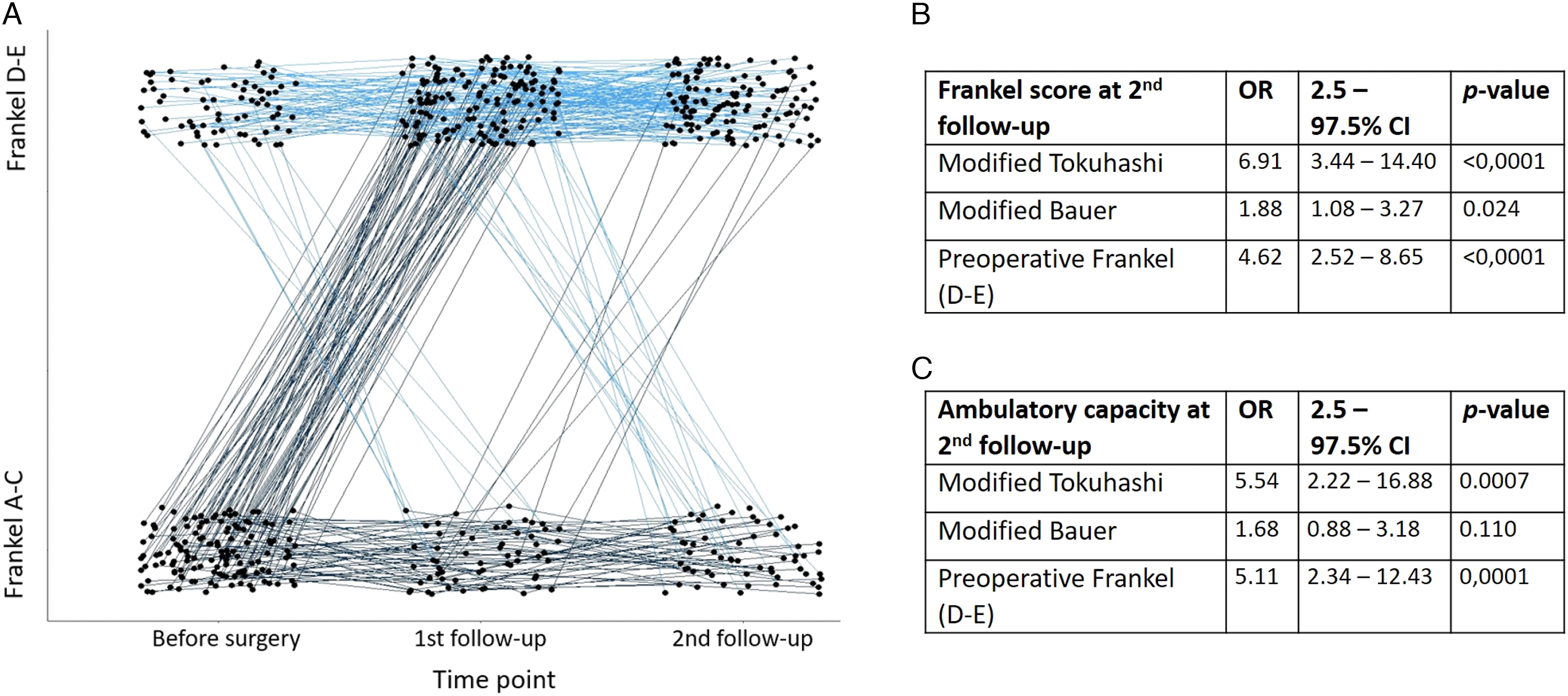
We lastly wanted to confirm that the categorization of patients we used based on recommendation for surgical treatment or not, was valid regarding their survival. The survival analysis of the different groups is depicted in Figure 3. A modified Tokuhashi score of ≥9 conferred a median survival time of 47 (27 - 83) months vs 7 (6 - 10) months in patients with lower score. The same applied to the modified Bauer score, where patients with a score of ≥2 had a median survival of 15 (11- 23) months than the ones with a lower score which survived for a median of 7 (3 - 10) months. Kaplan Meier survival curves of patients with different modified Tokuhashi and modified Bauer scores. Higher scores entailed longer median survival time (months).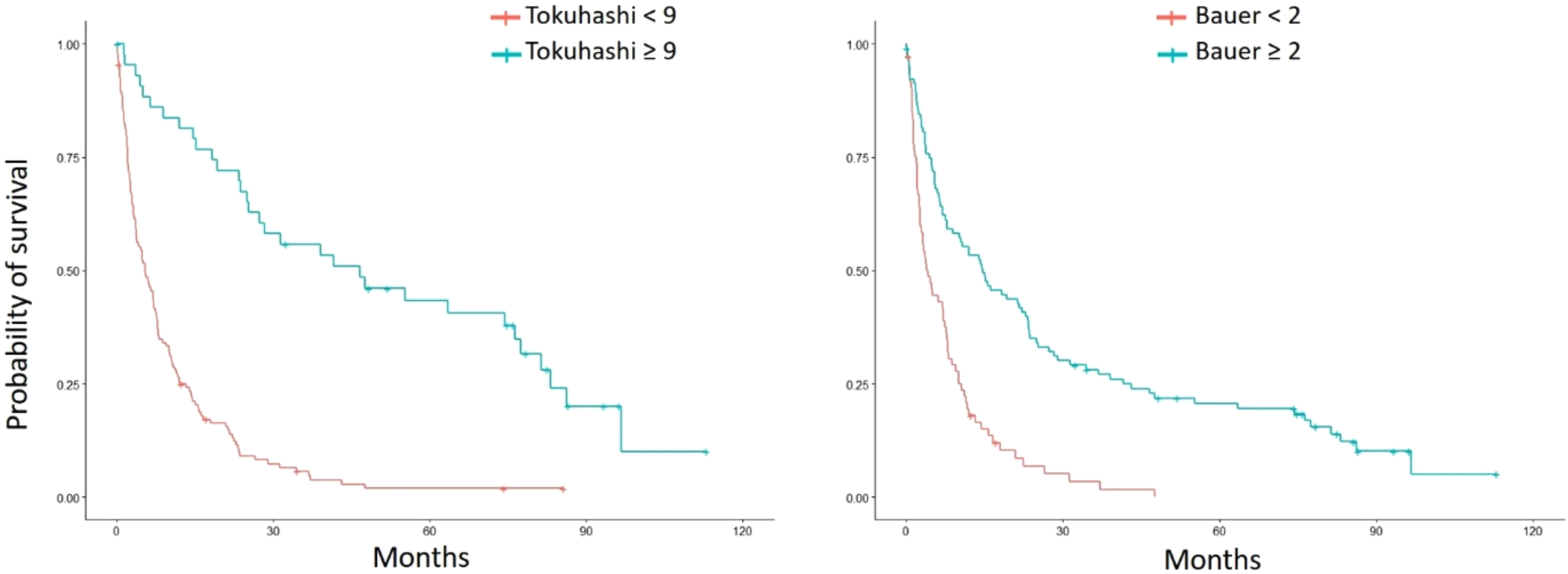
Discussion
The spinal metastasis scores have been widely adopted, enabling clinicians to quantify the impact of spinal metastasis and facilitate decision-making regarding surgical interventions, radiation therapy, or systemic treatments. Despite the acknowledged limitations, including potential underestimation of survival, 12 our findings align with existing literature, indicating that patients with modified Tokuhashi and Bauer scores of ≥9 and ≥2, respectively, exhibited more favorable survival. Preoperative ambulatory capacity.13,14 and regaining ambulatory capacity in the postoperative period, are factors that have important implications for patient survival as well. Patients that regain their ambulatory capacity can have a double as much longer median survival in comparison to the patients that remain nonambulatory. 15
Little is known whether the modified Tokuhashi and Bauer scores can predict the neurological outcome after decompressive surgery. We showed that patients with a modified Tokuhashi score of ≥9 had higher postoperative scores on the Frankel scale at the first and second follow up, while a modified Bauer score of ≥2 entailed higher scores only at the second follow-up. 7 A modified Bauer score of ≥2, a Tokuhashi of ≥9 and preoperative Frankel score of D or E were significant predictors of postoperative Frankel scores. It is reasonable to expect that patients with a higher Tokuhashi score will have a higher postoperative neurologic function scores as the Frankel score is included in the modified Tokuhashi score, however the OR for the modified Tokuhashi score to predict Frankel scores at late follow-up was higher than that of preoperative Frankel (6.91 vs 4.62).
Decompressive surgery is vital in order to alleviate neurologic compromise and to restore motor function, due to medullary cord compression.16,17 In this study, only 34% of the patients were ambulatory prior to the surgery. Most of the patients that were operated on regained the ability to ambulate (70%) and that was maintained at 6 months (68%). We found that preoperative ambulatory capacity and a modified Tokuhashi score of ≥9 are strong predictors of postoperative ambulatory capacity, the modified Bauer score however was not a predictor. There are limited studies in the literature that explore the prognostic value of the common spinal metastasis scores. In a prospective study of 202 patients by Schoenfeld et al, 18 it was shown that the Tokuhashi score was a good predictor of ambulatory function at 3 and 6 months after operative or non-operative treatment for spinal metastases. The SINS score was a good predictor of ambulatory function only at 3 months of follow-up. Cho et al 19 did not find a correlation between a Tomita score of ≤5 and postoperative neurological recovery in cases of patients with cervical spine metastases.
The present analysis indicated that the modified Tokuhashi and Bauer scores can serve as predictors of the postoperative neurologic outcome. The retrospective design and the fact that there is no equal representation of the patients along the scales of the used metastasis scores constitute weaknesses of this study. The Frankel score is included in the scoring system of the modified Tokuhashi score, which could explain why it performed better than the modified Bauer score at predicting the neurologic outcome. Another limitation of the study is that the low number of patients with low Tokuhashi scores (supplementary Table). Lastly, the fact that all of the patients were treated surgically could constitute a bias.
There is a need for further research into that topic, in order to potentiate the results, either with the inclusion of more patients to increase the power, or to test the validity of other known spine metastasis scores. In 2015, Ghori et al created a scoring system combining the patients’ ambulatory status, modified Bauer score and preoperative albumin, the New England Spine Metastasis Score, 20 which was shown to have a similar capacity with the modified Tokuhashi score to predict the postoperative ambulatory status. 18 The advent of machine learning tthas introduced the usage of dynamic scoring systems, with the examples of SORG and PathFx 3.0.21,22 The use of these scores is however more difficult to interpret, since they do not provide for a treatment recommendation regarding surgery or conservative treatment,
Conclusions
Postoperative ambulatory capacity is a crucial factor influencing patient survival and quality of life. The modified Tokuhashi and Bauer scores were shown to be useful adjuncts for the surgeon, and provided with insights not just on survival, but also on the potential to regain ambulatory function after decompressive surgery. Patients with scores that suggest surgical treatment had higher chances of being ambulatory at follow-up and the Tokuhashi score performed better in this setting.
Supplemental Material
Supplemental Material - Can Survival Scoring Systems for Spinal Metastases be Used to Predict Postoperative Neurologic Recovery? A Retrospective Study on 204 Patients With Thoracolumbar Metastases Treated at a Tertiary Center
Supplemental Material for Can Survival Scoring Systems for Spinal Metastases be Used to Predict Postoperative Neurologic Recovery? A Retrospective Study on 204 Patients With Thoracolumbar Metastases Treated at a Tertiary Center by Michael G. Kontakis and Panagiotis Tsagkozis in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.