
Abstract
Study Design:
Retrospective cohort study.
Objective:
Factors that predict outcomes for adult cervical spine deformity (ACSD) have not been well defined. To compare ACSD patients with best versus worst outcomes.
Methods:
This study was based on a prospective, multicenter observational ACSD cohort. Best versus worst outcomes were compared based on Neck Disability Index (NDI), Neck Pain Numeric Rating Scale (NP-NRS), and modified Japanese Orthopaedic Association (mJOA) scores.
Results:
Of 111 patients, 80 (72%) had minimum 1-year follow-up. For NDI, compared with best outcome patients (n = 28), worst outcome patients (n = 32) were more likely to have had a major complication (P = .004) and to have undergone a posterior-only procedure (P = .039), had greater Charlson Comorbidity Index (P = .009), and had worse postoperative C7-S1 sagittal vertical axis (SVA; P = .027). For NP-NRS, compared with best outcome patients (n = 26), worst outcome patients (n = 18) were younger (P = .045), had worse baseline NP-NRS (P = .034), and were more likely to have had a minor complication (P = .030). For the mJOA, compared with best outcome patients (n = 16), worst outcome patients (n = 18) were more likely to have had a major complication (P = .007) and to have a better baseline mJOA (P = .030). Multivariate models for NDI included posterior-only surgery (P = .006), major complication (P = .002), and postoperative C7-S1 SVA (P = .012); models for NP-NRS included baseline NP-NRS (P = .009), age (P = .017), and posterior-only surgery (P = .038); and models for mJOA included major complication (P = .008).
Conclusions:
Factors distinguishing best and worst ACSD surgery outcomes included patient, surgical, and radiographic factors. These findings suggest areas that may warrant greater awareness to optimize patient counseling and outcomes.
Introduction
Early attempts to surgically treat adult cervical spine deformity (ACSD) focused on the most severe forms, and the treatments were considered high risk and had high complication rates. 1 -4 As advances have been made in anesthesia and critical care, as well as surgical techniques and instrumentation, there has been an increased interest in surgically treating these deformities. 5 -13 In contrast to the progress that has been made in treating adult thoracolumbar deformities, only recently have similar advances begun for ACSD. 14 Recent advances have included proposal of a cervical deformity classification 15 and development of a standardized nomenclature to describe the osteotomies used to treat these deformities. 16 Other recent studies have highlighted the remarkable lack of consensus for ACSD treatment strategies 17 and have demonstrated that, similar to thoracolumbar deformity surgery, ACSD surgery is associated with high complication rates. 18,19
Although surgery for ACSD has the potential to significantly improve pain, disability, and neurological function, reported outcomes are often presented as averages. 8 While averages may be useful for summarizing data, they do not fully reflect the spectrum of outcomes. As has been shown for thoracolumbar deformity surgeries, 20,21 there is a range of outcomes for ACSD. Not every patient can expect to achieve the average outcome, and at the 2 extreme ends of the spectrum are those who have been left with little or no residual pain and disability (“best outcome”) and those who have improved minimally, not at all, or even worsened (“worst outcome”). Comparing patients with the best and worst outcomes following surgery for ACSD may prove useful for better optimization of patient selection, treatment strategies, and patient counseling.
In the present study, we provide assessment of a prospective, multicenter observational cohort of surgically treated ACSD patients. Our objectives were to assess the range of patient outcomes following surgical treatment for ACSD based on multiple outcomes measures. In addition, we sought to compare the patients with the best and worst outcomes based on each standardized outcome measure in order to identify factors that may distinguish these 2 groups.
Methods
Patient Population
As part of a prospective, multicenter observational cohort study, consecutive adult patients presenting for surgical evaluation of cervical and cervicothoracic deformities were enrolled at 13 centers across the United States. Each participating site obtained institutional review board approval, and each patient provided written consent. Inclusion criteria were the following: age ≥18 years, cervical deformity, and plan for surgical deformity correction. Cervical deformity was defined as the presence of at least one of the following: cervical kyphosis (C2-7 sagittal Cobb angle >10°), cervical scoliosis (C2-7 coronal Cobb angle >10°), C2-7 sagittal vertical axis (C2-7 SVA) >4 cm, or chin-brown vertical angle >25°. Patients with active tumor or infection were excluded. For the present study, only patients with complete baseline data and minimum 1-year follow-up were included.
Data Collection and Radiographic Assessment
Patient demographics, clinical data, surgical procedure details, and complications were collected using standardized forms. Standardized measures of health status included Neck Disability Index (NDI), modified Japanese Orthopaedic Association (mJOA), and the Neck Pain Numerical Rating Scale (NP-NRS). Osteotomies were classified as low-grade or high-grade based on a recently published classification system. 16 Complications were classified as major or minor. A complication was termed major if it involved invasive intervention, had prolonged or permanent morbidity, or resulted in death.
Full-length, free-standing spine radiographs, in combination with focused cervical lateral radiographs, were obtained at baseline and at regular follow-up intervals. Radiographs were analyzed using validated software at a central core facility based on previously reported techniques. 5,22 -25 Measures included C2-C7 lordosis, C2-C7 sagittal vertical axis (C2-C7 SVA), C7-S1 SVA, cervical-thoracic pelvic angle (CTPA), pelvic tilt (PT), and mismatch between pelvic incidence and lumbar lordosis (PI-LL).
Data and Statistical Analysis
Patients with the best and worst clinical outcomes were defined separately based on 3 measures, NDI, mJOA, and NP-NRS. The changes from preoperative baseline to last follow-up were calculated for each measure for each patient and were used to create distribution plots. Thresholds for best and worst outcomes were established based on the tails at the extremes of the distribution plots and previously reported score correlates to health states. 26 -30 The resulting best and worst outcomes groups within each measure were then compared. To minimize floor effects of the NDI, comparisons of best versus worst outcomes were based on patients with a preoperative baseline NDI of at least 20. To minimize the floor effects of the NP-NRS, comparisons between best versus worst outcomes were made with patients having a baseline NP-NRS score of at least 3. Based on assessment of distribution plots and established threshold cutoffs for the best and worst groups, similar cutoffs were not necessary for the mJOA. These baseline threshold cutoffs for NDI and NP-NRS were selected to reflect levels of at least moderate disability and pain based on previous reports. 26 -30
Demographic, clinical, and surgical variables were summarized using means and standard deviations for continuous variables and frequencies and percentages for categorical variables. For continuous variables, normality of distribution was assessed using the Kolmogorov-Smirnov test. T tests were used to assess for differences between normally distributed continuous variables, and the independent-samples Mann-Whitney U test was used for comparisons between continuous variables without normal distribution. Binary logistic regression analysis was used to adjust for the effects of multiple covariates predictive of best versus worst outcomes. Forward stepwise regression analyses were performed using variables with P < .1 on univariate assessment to distinguish between patients with best versus worst outcomes. Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 24 (IBM Corp, Armonk, NY). Statistical tests were 2-tailed, and P < .05 was considered statistically significant.
Results
Patient Population
Of 111 patients who met inclusion criteria, 80 (72%) had minimum 1-year follow-up and were included in the present study. Baseline demographic, clinical, and operative parameters are summarized in Table 1. The mean available postoperative follow-up was 1.4 years and ranged from 1 to 2 years.
Demographic, Clinical, and Operative Parameters for 80 Surgically Treated Adults With Cervical Spinal Deformity.
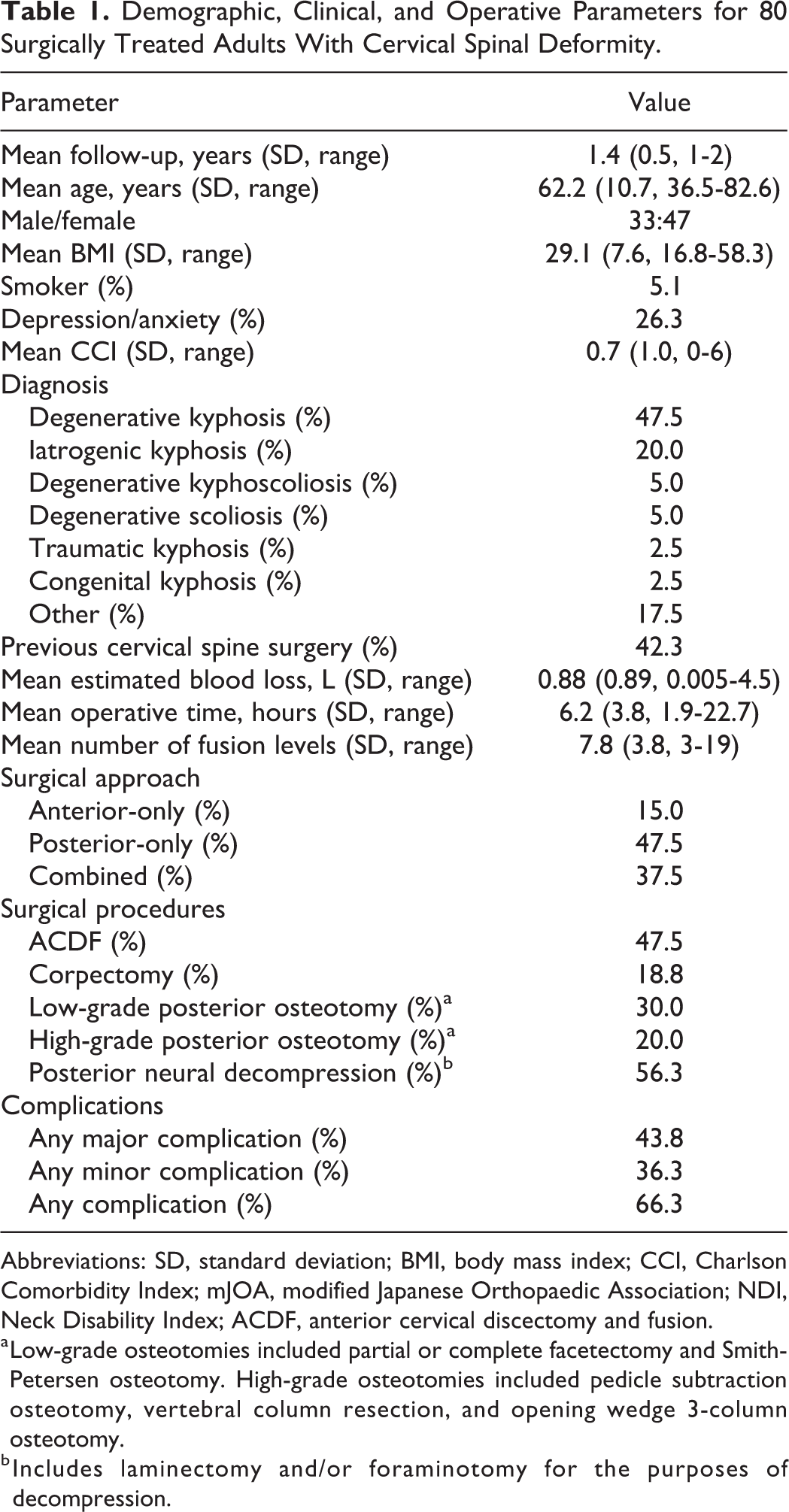
Abbreviations: SD, standard deviation; BMI, body mass index; CCI, Charlson Comorbidity Index; mJOA, modified Japanese Orthopaedic Association; NDI, Neck Disability Index; ACDF, anterior cervical discectomy and fusion.
a Low-grade osteotomies included partial or complete facetectomy and Smith-Petersen osteotomy. High-grade osteotomies included pedicle subtraction osteotomy, vertebral column resection, and opening wedge 3-column osteotomy.
b Includes laminectomy and/or foraminotomy for the purposes of decompression.
Mean preoperative and follow-up clinical outcomes scores and radiographic measures are summarized in Table 2. Compared with baseline, the mean NDI and NP-NRS scores improved significantly at last follow-up. The overall mJOA modestly improved, but this change did not reach statistical significance. The mean C2-C7 lordosis and overall global sagittal alignment (C7-S1 SVA) improved significantly, while significant changes were not appreciated for C2-C7 SVA, CTPA, PT, or PI-LL mismatch.
Radiographic and Clinical Outcomes at Baseline and Minimum 1-Year Follow-up for 80 Surgically Treated Adults With Cervical Spinal Deformity. 1
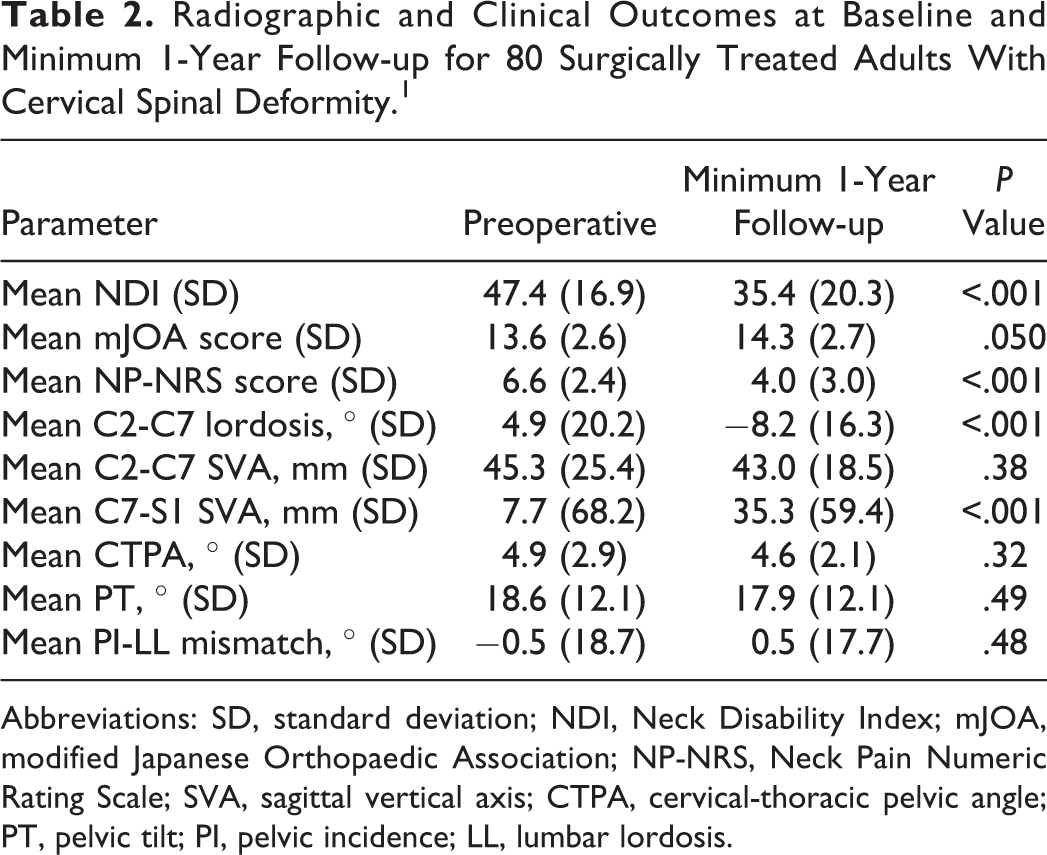
Abbreviations: SD, standard deviation; NDI, Neck Disability Index; mJOA, modified Japanese Orthopaedic Association; NP-NRS, Neck Pain Numeric Rating Scale; SVA, sagittal vertical axis; CTPA, cervical-thoracic pelvic angle; PT, pelvic tilt; PI, pelvic incidence; LL, lumbar lordosis.
Best and Worst Outcomes Based on NDI
Of the 80 patients in the study cohort, 77 (96.3%) had a baseline NDI of ≥20. For these 77 patients, the mean baseline NDI was 48.8 (SD = 15.7, range 22.2 to 92.0) and the mean follow-up NDI was 36.0 (SD = 20.3, range 0.0 to 80.0; Figure 1). Based on the NDI, the best outcome group (NDI improved by ≥20 points) consisted of 28 patients, and the worst outcome group (NDI improved by <10 points or worsened) consisted of 32 patients (Figure 1). The best outcome group had a mean baseline NDI of 49.7 (SD = 14.9) that improved to a mean of 21.4 (SD = 14.1) at follow-up. In contrast, the worst outcome group had a mean baseline NDI of 48.5 (SD = 14.4) that increased to a mean follow-up NDI of 50.3 (SD = 14.7).
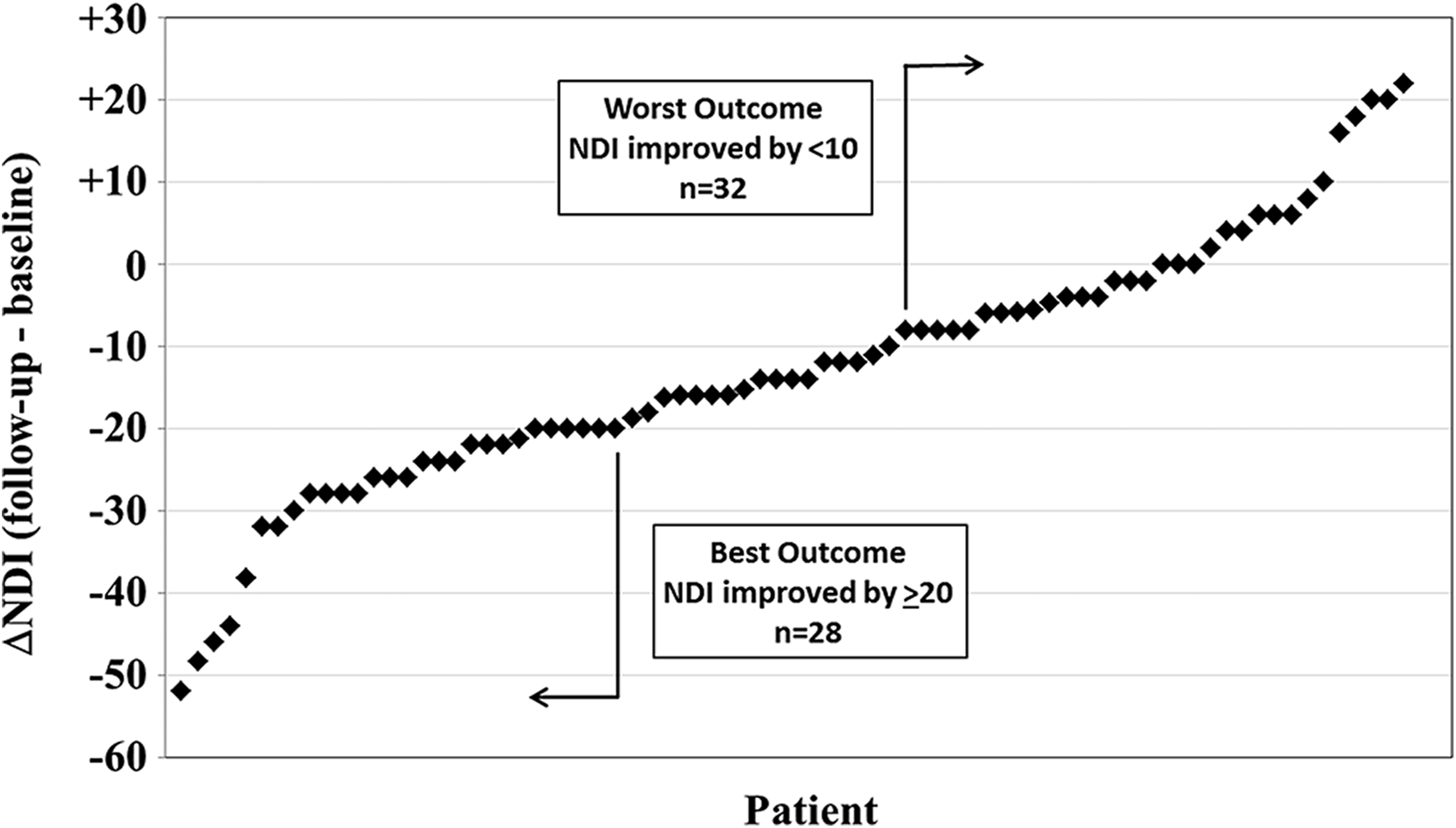
Change in Neck Disability Index (NDI) scores from preoperative baseline to minimum 1-year follow-up for 77 patients surgically treated for adult cervical deformity. Each patient had a preoperative baseline NDI score of at least 20 points. Cutoffs for best and worst outcomes are indicated.
Univariate assessments between the best and worst outcomes groups based on NDI are summarized in Table 3. Compared with best outcome patients, at baseline those with the worst outcomes had a higher comorbidity score (P = .009), lower PT (P = .003), and more negative PI-LL mismatch (P = .012). A significantly higher proportion of patients in the worst outcome group was treated with a posterior-only approach (P = .039), had a high-grade osteotomy (P = .004), and had a major complication (P = .004). At follow-up the worst outcome group based on NDI also had worse mJOA (P = .042) and NP-NRS (P < .001), had worse global sagittal alignment based on the C7-S1 SVA (P = .027), and had less increase in cervical lordosis (P = .041; Table 3).
Univariate Analysis of Baseline, Operative, and Follow-up Parameters Between Patients With the Best Versus Worst Outcomes Based on NDI Following Surgery for Adult Cervical Deformity.a
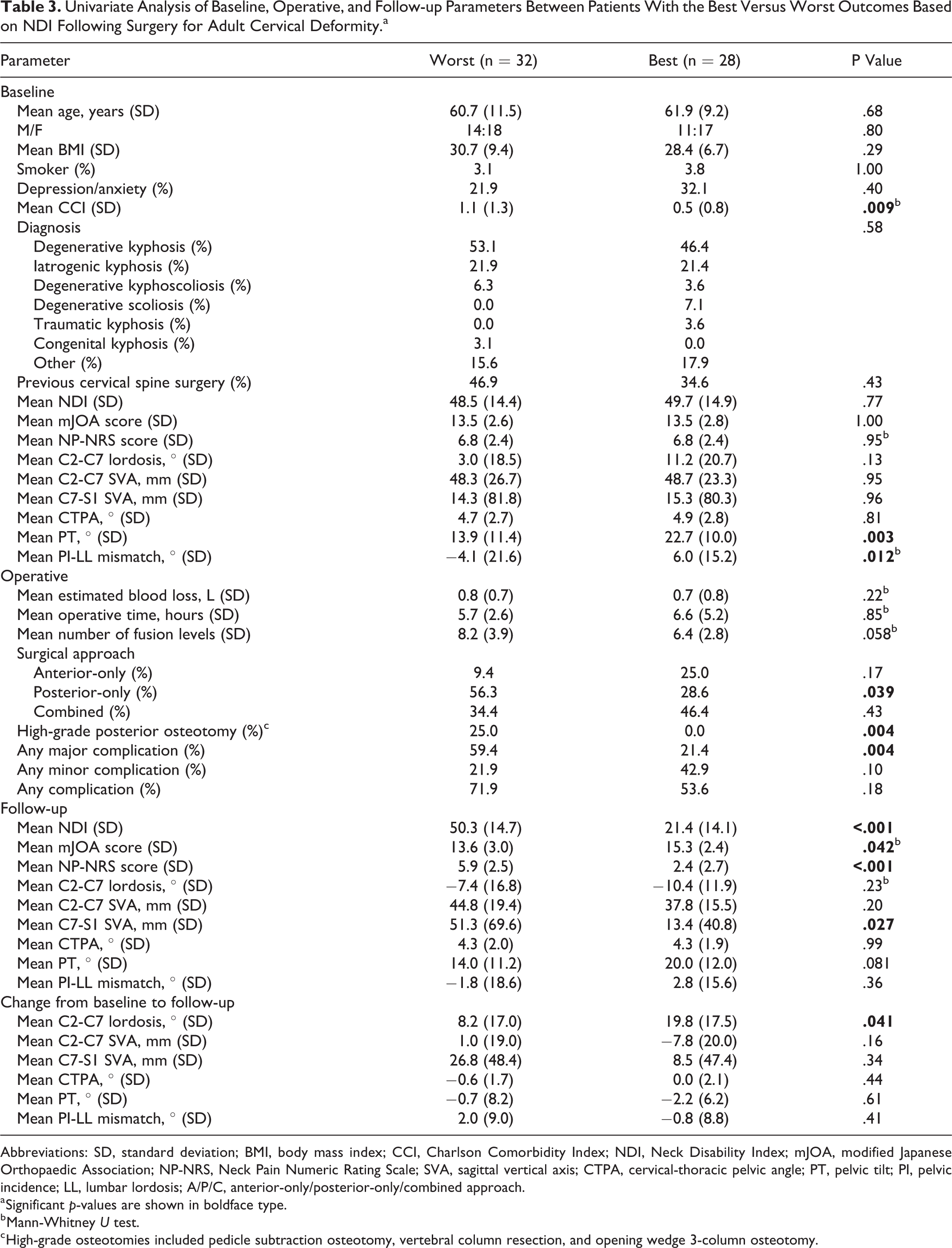
Abbreviations: SD, standard deviation; BMI, body mass index; CCI, Charlson Comorbidity Index; NDI, Neck Disability Index; mJOA, modified Japanese Orthopaedic Association; NP-NRS, Neck Pain Numeric Rating Scale; SVA, sagittal vertical axis; CTPA, cervical-thoracic pelvic angle; PT, pelvic tilt; PI, pelvic incidence; LL, lumbar lordosis; A/P/C, anterior-only/posterior-only/combined approach.
a Significant p-values are shown in boldface type.
b Mann-Whitney U test.
c High-grade osteotomies included pedicle subtraction osteotomy, vertebral column resection, and opening wedge 3-column osteotomy.
The best-fit model based on logistic regression analysis included 3 parameters: posterior-only approach (P = .006), occurrence of a major complication (P = .012), and C7-S1 SVA at last follow-up (P = .012; Table 4).
Multivariate Analysis of Factors Distinguishing Between Patients With the Best Versus Worst Outcomes Based on NDI Following Surgery for Adult Cervical Deformitya.
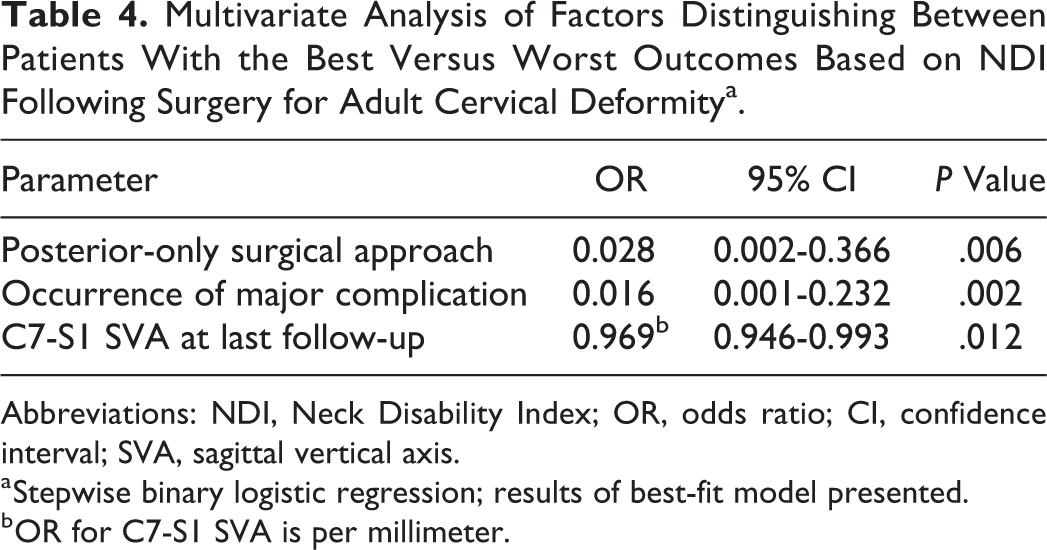
Abbreviations: NDI, Neck Disability Index; OR, odds ratio; CI, confidence interval; SVA, sagittal vertical axis.
a Stepwise binary logistic regression; results of best-fit model presented.
b OR for C7-S1 SVA is per millimeter.
Best and Worst Outcomes Based on NP-NRS
Of the 80 patients in the study cohort, 74 (92.5%) had NP-NRS ≥3. For these 74 patients, the mean baseline NP-NRS was 7.1 (SD = 1.8, range 3 to 10) and the mean follow-up NP-NRS was 4.2 (SD = 3.0, range 0 to 10.0; Figure 2). Based on the NP-NRS, the best outcome group (NP-NRS improved by ≥5 points) consisted of 26 patients, and the worst outcome group (NP-NRS without improvement or worsened) consisted of 18 patients (Figure 2). The best outcome group had a mean baseline NP-NRS of 7.6 (SD = 1.4) that improved to a mean of 1.3 (SD = 1.4) at follow-up. In contrast, the worst outcome group had a mean baseline NP-NRS of 6.3 (SD = 1.8) that increased to a mean follow-up NP-NRS of 7.6 (SD = 1.7).
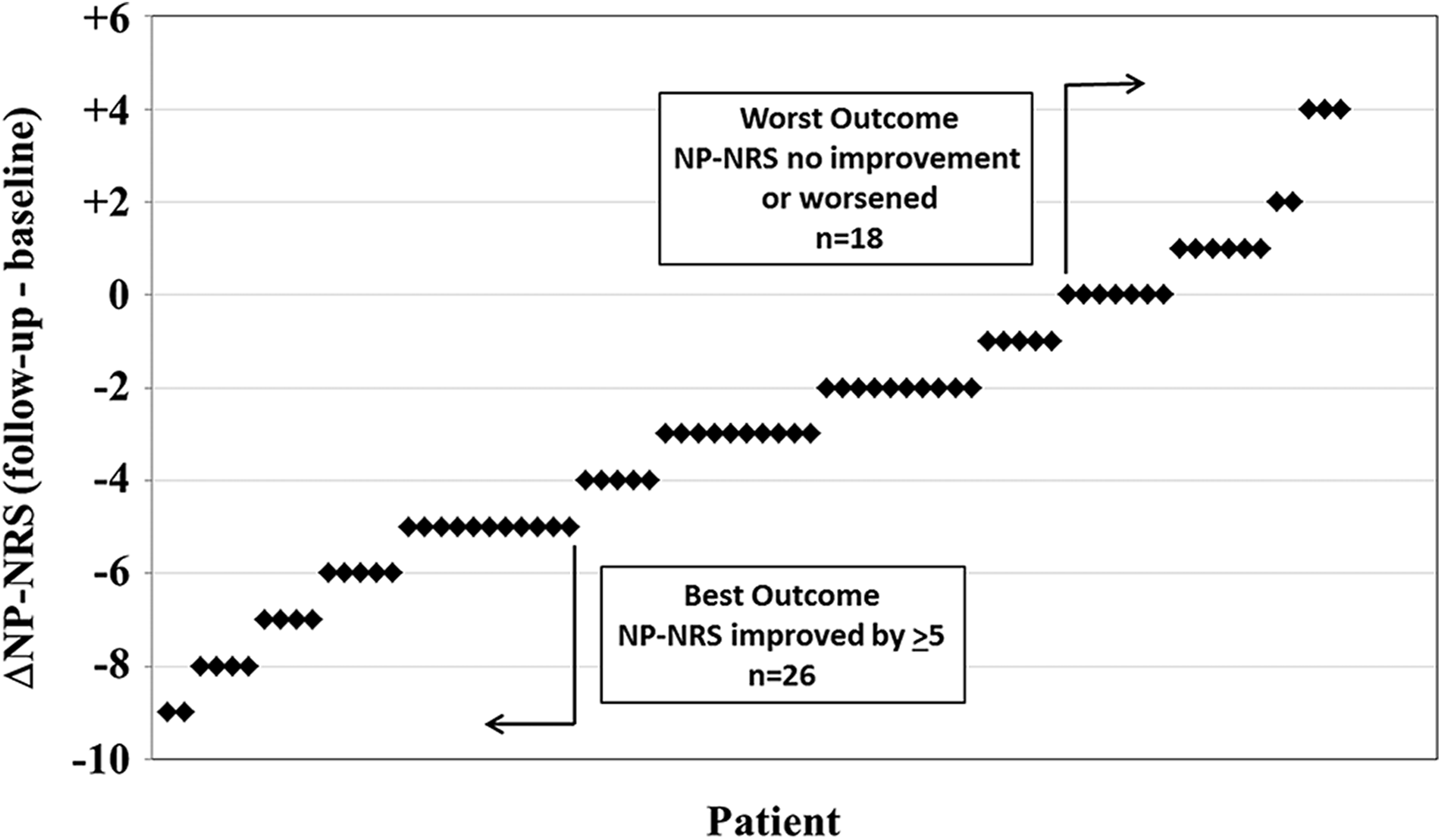
Change in Neck Pain Numeric Rating Scale (NP-NRS) scores from preoperative baseline to minimum 1-year follow-up for 74 patients surgically treated for adult cervical deformity. Each patient had a preoperative baseline NP-NRS score of at least 3. Cutoffs for best and worst outcomes are indicated.
Univariate assessments between the best and worst outcomes groups based on NP-NRS are summarized in Table 5. Compared with best outcome patients, at baseline those with the worst outcomes were younger (P = .045) and had lower NP-NRS (P = .034). Minor complications were more common among patients in the best outcome group (P = .03). At follow-up the worst outcome group had worse NDI (P < .001) and had a modestly but significantly lower CTPA (Table 5).
Univariate Analysis of Baseline, Operative, and Follow-up Parameters Between Patients With the Best Versus Worst Outcomes Based on NP-NRS Following Surgery for Adult Cervical Deformity.a
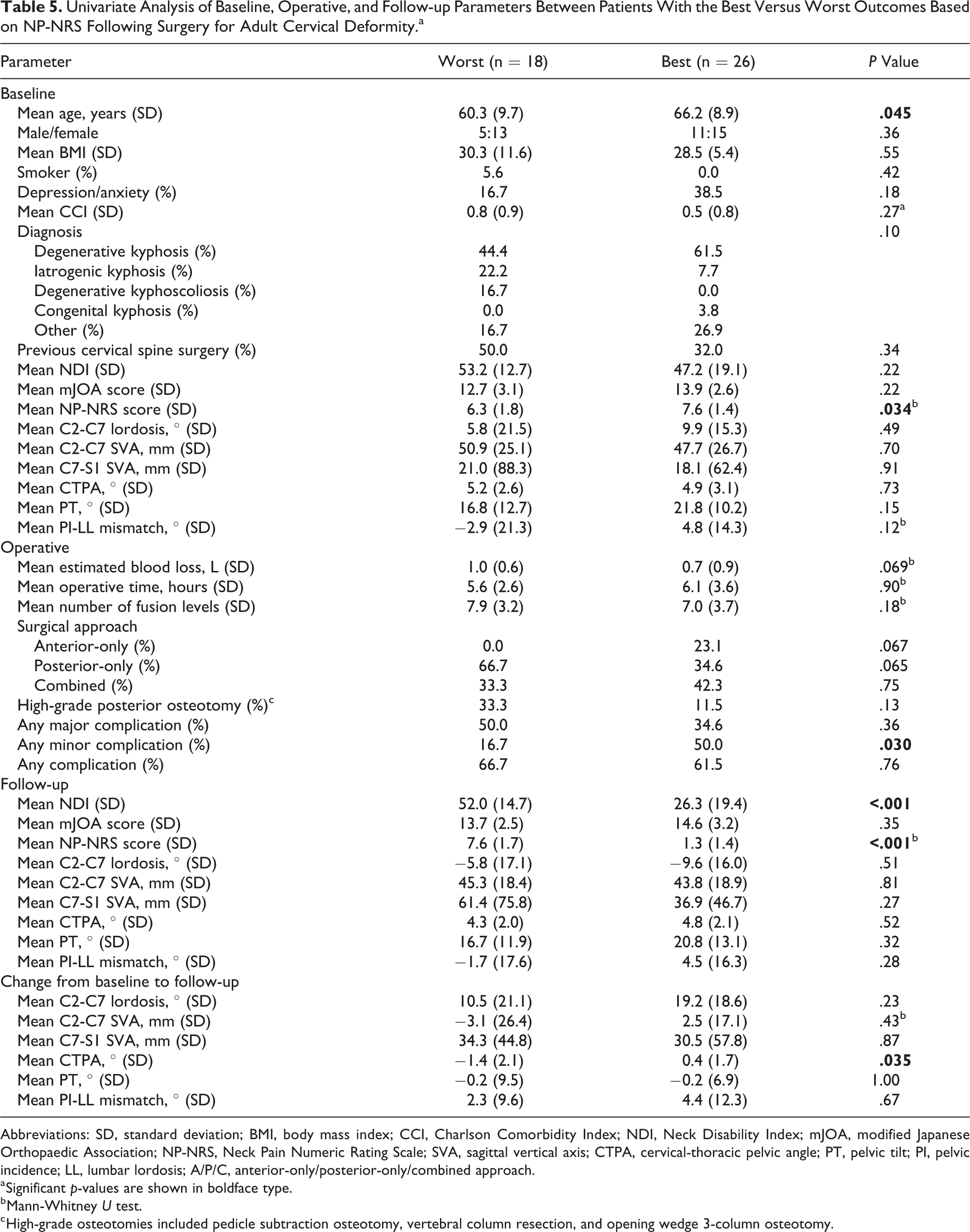
Abbreviations: SD, standard deviation; BMI, body mass index; CCI, Charlson Comorbidity Index; NDI, Neck Disability Index; mJOA, modified Japanese Orthopaedic Association; NP-NRS, Neck Pain Numeric Rating Scale; SVA, sagittal vertical axis; CTPA, cervical-thoracic pelvic angle; PT, pelvic tilt; PI, pelvic incidence; LL, lumbar lordosis; A/P/C, anterior-only/posterior-only/combined approach.
a Significant p-values are shown in boldface type.
b Mann-Whitney U test.
c High-grade osteotomies included pedicle subtraction osteotomy, vertebral column resection, and opening wedge 3-column osteotomy.
The best-fit model based on logistic regression analysis included 3 parameters: preoperative NP-NRS (P = .009), age (P = .017), and posterior-only approach (P = .038; Table 6).
Multivariate Analysis of Factors Distinguishing Between Patients With the Best Versus Worst Outcomes Based on NP-NRS Following Surgery for Adult Cervical Deformitya.
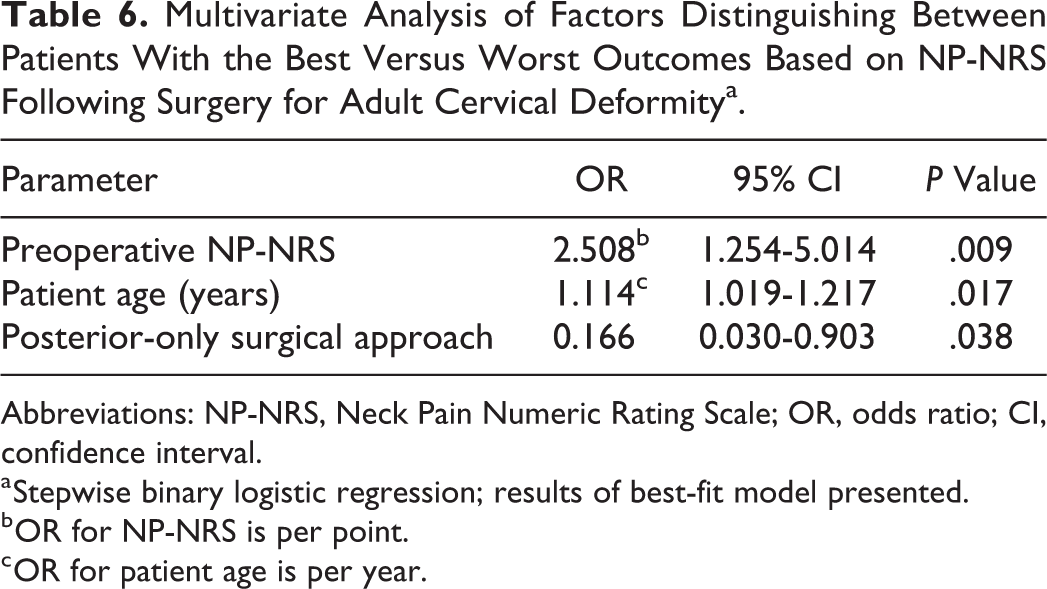
Abbreviations: NP-NRS, Neck Pain Numeric Rating Scale; OR, odds ratio; CI, confidence interval.
a Stepwise binary logistic regression; results of best-fit model presented.
b OR for NP-NRS is per point.
c OR for patient age is per year.
Best and Worst Outcomes Based on mJOA
Of the 80 patients in the study cohort, 64 (80.0%) had a baseline and follow-up mJOA documented. For these 64 patients, the mean mJOA was 13.6 (SD = 2.6) and the mean follow-up mJOA was 14.3 (SD = 2.7). Based on the mJOA, the best outcome group (mJOA score improved by ≥2 points) consisted of 16 patients, and the worst outcome group (mJOA worsened by ≥1 point) consisted of 18 patients (Figure 3). The best outcome group had a mean baseline mJOA of 12.3 (SD = 2.2) that improved to a mean of 16.4 (SD = 1.7) at follow-up. In contrast, the worst outcome group had a mean baseline mJOA of 14.1 (SD = 2.2) that worsened to a mean follow-up mJOA of 11.9 (SD = 1.8).
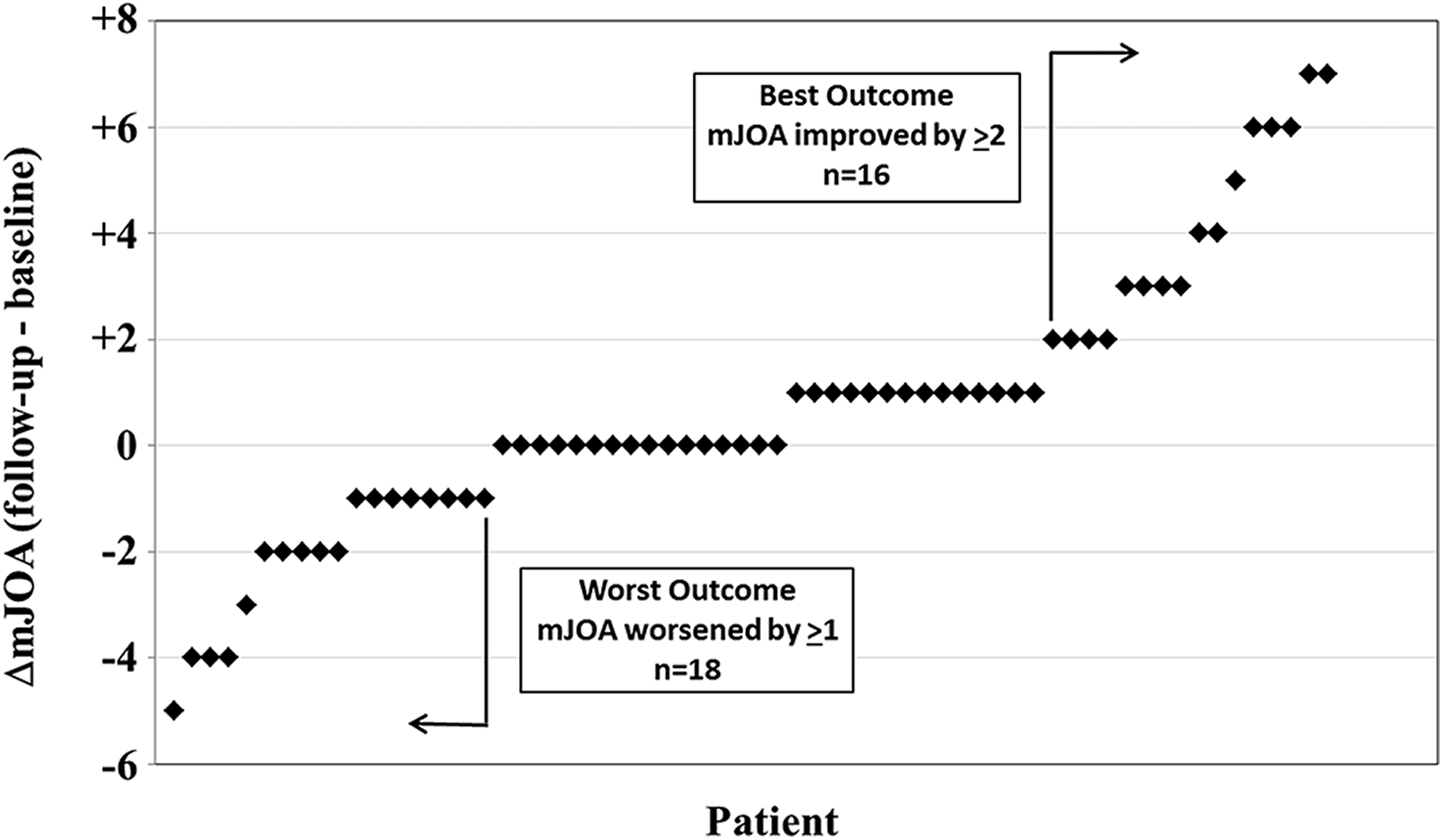
Change in modified Japanese Orthopaedic Association (mJOA) scores from preoperative baseline to minimum 1-year follow-up for 64 patients surgically treated for adult cervical deformity. Cutoffs for best and worst outcomes are indicated.
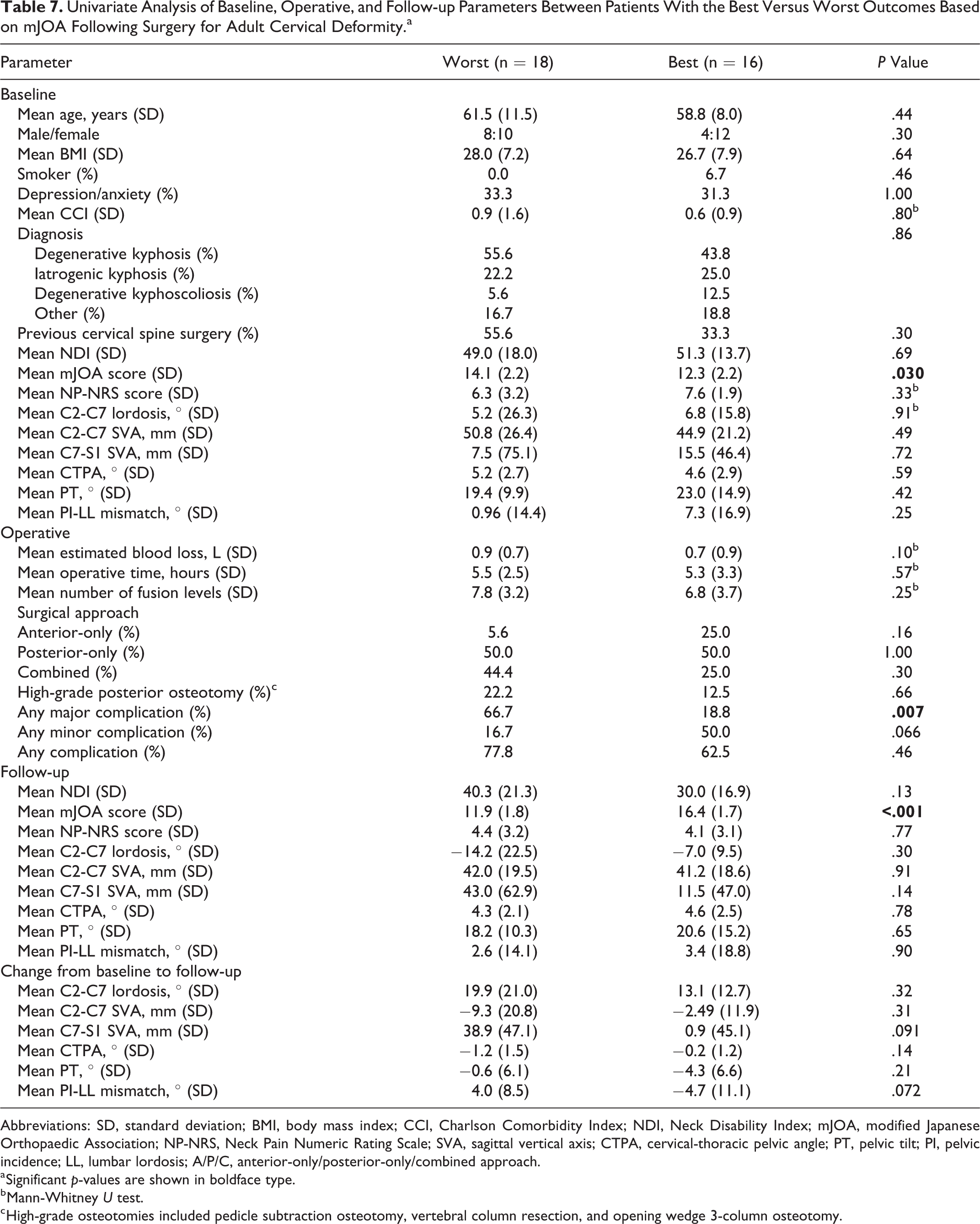
Univariate assessments between the best and worst outcomes groups based on mJOA are summarized in Table 7. Compared with best outcome patients, at baseline those with the worst outcomes had better mJOA (P = .030). The occurrence of major complications was more common among the patients with the worst outcomes (P = .007). Except for differences in mJOA, at follow-up the best and worst outcome groups did not differ based on radiographic measures or outcomes measures (Table 7 ).
Univariate Analysis of Baseline, Operative, and Follow-up Parameters Between Patients With the Best Versus Worst Outcomes Based on mJOA Following Surgery for Adult Cervical Deformity.a
Abbreviations: SD, standard deviation; BMI, body mass index; CCI, Charlson Comorbidity Index; NDI, Neck Disability Index; mJOA, modified Japanese Orthopaedic Association; NP-NRS, Neck Pain Numeric Rating Scale; SVA, sagittal vertical axis; CTPA, cervical-thoracic pelvic angle; PT, pelvic tilt; PI, pelvic incidence; LL, lumbar lordosis; A/P/C, anterior-only/posterior-only/combined approach.
a Significant p-values are shown in boldface type.
b Mann-Whitney U test.
c High-grade osteotomies included pedicle subtraction osteotomy, vertebral column resection, and opening wedge 3-column osteotomy.
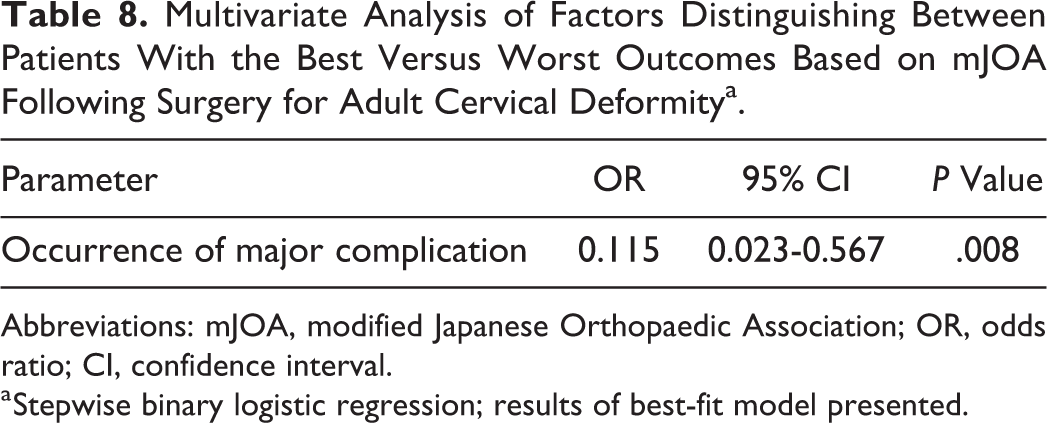
The best-fit model based on logistic regression analysis only included occurrence of a major complication (P = .008; Table 8).
Multivariate Analysis of Factors Distinguishing Between Patients With the Best Versus Worst Outcomes Based on mJOA Following Surgery for Adult Cervical Deformitya.
Abbreviations: mJOA, modified Japanese Orthopaedic Association; OR, odds ratio; CI, confidence interval.
a Stepwise binary logistic regression; results of best-fit model presented.
Discussion
The present study provides a prospective assessment of the clinical improvement following surgical treatment for 80 ACSD patients at a minimum 1-year follow-up based on standardized outcomes measures of disability (NDI), pain (NP-NRS), and myelopathy (mJOA). The overall patient cohort demonstrated significant improvement in pain and disability and had a modest improvement in myelopathy scores that bordered on statistical significance. Although the outcome score averages reflect overall improvement from the time of surgery to last follow-up, the amount of change in each measure at the individual patient level varied considerably. Comparing the best and worst outcomes groups demonstrated distinguishing factors that included a mix of patient (age, baseline NP-NRS, Charlson Comorbidity Index [CCI]), surgical (complications and surgical approach), and radiographic (follow-up C7-S1 SVA) parameters. Collectively, these findings demonstrate the broad range in outcomes following surgery for ACSD and suggest that the factors that may account for this variation are complex and multifactorial.
Predictors of the best versus worst outcomes varied based on the 3 different outcome metrics, likely due to differences in what the 3 metrics assess. The NP-NRS is a direct measure of pain, while the NDI assesses how neck pain affects a patient’s daily life and activities. 31,32 The mJOA provides a focused assessment of functional disability related to cervical myelopathy. 33
On univariate analysis, the occurrence of complications was a significant distinguishing factor between patients with the best and worst outcomes for all 3 measures assessed. For 2 of the measures (NDI and mJOA), the occurrence of a major complication was incorporated into the best-fit multivariate model. Although this association has not been previously reported for ACSD, authors have previously assessed the impact of complications on outcome for adult thoracolumbar deformity. Smith and colleagues performed a risk-benefit assessment of surgery for adult thoracolumbar deformity with stratification based on age. 34 They reported that, despite having a 4-fold higher complication rate compared with the young patient group, the elderly had greater magnitudes of improvement for pain and disability, suggesting that globally the impact of complications may not preclude significant clinical improvement following surgery. Bridwell and colleagues also reported outcomes for adult thoracolumbar deformity surgery and noted that there was a trend toward a smaller incremental improvement at 2-year follow-up in those patients who had a major complication. 35 With 3- to 5-year follow-up of the same patient population, these authors reported a significant impact of complications on outcome. 36 The present study, in combination with the findings of Bridwell and colleagues, suggests that complications do have the potential to significantly impact patient outcome, especially when comparing patients at the extremes (best versus worst outcomes). It must be recognized that, despite the best of care, there are inherent risks of complications associated with these often complex procedures. Nevertheless, these findings further emphasize that efforts to reduce complications associated with these procedures are warranted.
Posterior-only surgical approach was found to be significantly more common among patients with the worst outcomes. This association was apparent in the multivariate modeling for 2 of the outcomes measures (NDI and NP-NRS). There are many potential explanations for these associations. High-grade osteotomies are typically performed through a posterior-only approach. 16 These osteotomies are often reserved for the most severe deformities and are among the most aggressive of correction techniques. It is possible that the posterior-only approach may be disproportionately represented among the patients with the worst outcomes due to its favored use in the most severe and extensive of deformities, especially those requiring a 3-column osteotomy. Notably, for the univariate assessment of factors associated with best versus worst outcomes based on NDI, use of a high-grade osteotomy was significantly associated with the worst outcomes. The substantially greater muscle disruption associated with a posterior approach, compared with an anterior approach, may also partially account for the posterior approach being associated with poorer outcomes based on neck pain and disability. In addition, the posterior approaches used for some patients for deformity correction were extensive, with some necessitating extension of instrumentation and arthrodesis into the lower thoracic or lumbar spine, which could also affect clinical outcomes. These findings certainly do not suggest that the posterior-only approach is always associated with poor outcomes or that it should be abandoned. Selection of surgical approach is often driven by deformity type, history of previous procedures, and the goals of correction. For treatment of many cervical deformities, an anterior-only approach may not be feasible.
On both univariate and multivariate analysis, residual global sagittal malalignment (C7-S1 SVA) was significantly associated with the worst outcome group based on the NDI. The negative impact of positive global sagittal malalignment on pain and disability is well recognized for thoracolumbar deformity. 37,38 Although the C7-S1 SVA did not differ preoperatively between the patients that would ultimately have the best and worst outcomes, it is possible that changes in alignment induced by the cervical deformity correction may have altered the global alignment through changes in compensatory measures. 39,40
Patient age was a significant distinguishing factor between the best and worst outcomes based on the NP-NRS univariate and multivariate analyses. This association may seem counterintuitive, since the older patients were favored to have the best outcome. The reason for this association is unclear but may relate to unaccounted for differences in deformity types and differences in baseline pain and disability across age groups.
Smith and colleagues have assessed best versus worst outcomes for adult thoracolumbar deformity surgery based on the Oswestry Disability Index and Scoliosis Research Society 22r (SRS-r). Similar to the present study, they reported that the factors that distinguished the best and worst outcomes were a mix of patient factors (baseline depression, BMI, comorbidities, and disability), radiographic factors (residual global sagittal malalignment as assessed by the C7-S1 SVA), and the occurrence of complications. 20,21 Although baseline depression and BMI were not distinguishing factors in the present study, it is notable that the remaining factors overlap between the 2 studies and suggest that the factors that affect outcomes of adult thoracolumbar and cervical deformity surgeries may have more similarities than differences.
The primary strength of the present study is the prospective multicenter design with standardized data collection. In addition, the patient cohort is heterogeneous and represents a broad spectrum of cervical deformities treated by multiple surgeons across multiple institutions, which enhances the generalizability of the findings. The primary limitation of the present study relates to the number of patients. Although 80 is a relatively large number of patients for ACSD, the limited numbers of patients, especially when focusing on those at the extreme ends of the outcomes spectrum, does impact the ability to perform granular assessments of factors associated with outcomes. In addition, although multiple statistical comparisons were performed in the present study, we intentionally did not perform a Bonferroni correction, since we would rather commit a Type I error than miss potentially important associations, especially in the setting of limited numbers of patients. Another limitation of the present study relates to the distribution of the patient population enrolled in the database. Since the mean patient age was 62 years and the youngest patient was 36.5 years, the findings of the present study may be most relevant to the older ACSD patient population. Last, there remains no ACSD-specific outcome measure, which necessitated the use of more generalized outcomes measures that cover neck disability, neck pain, and cervical myelopathy.
Conclusions
Based on a prospectively collected multicenter series of ACSD patients, this study provides assessment of the clinical improvement following surgical treatment for 80 ACSD patients at a minimum 1-year follow-up based on standardized outcomes measures of disability, pain, and myelopathy. Although the overall patient cohort demonstrated significant improvement in outcomes, there was substantial variation at the individual patient level. The factors that distinguished between the best and worst outcomes groups included a mix of patient (age, baseline NP-NRS, CCI), surgical (complications and surgical approach), and radiographic (follow-up C7-S1 SVA) parameters. Collectively, these findings demonstrate the broad range in outcomes following surgery for ACSD and suggest that the factors that may account for this variation are complex and multifactorial. These findings suggest areas that may warrant greater awareness to help optimize patient selection, treatment strategies, and preoperative patient counseling.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The International Spine Study Group (ISSG) is funded through research grants from DePuy Synthes and individual donations.