
Abstract
Study Design
Randomized controlled trial.
Objectives
To characterize postoperative C-reactive protein (CRP) trajectories as predictors of surgical site infection (SSI) following lumbar spine surgery, to determine optimal CRP thresholds, and to assess whether intrawound vancomycin powder affects postoperative CRP kinetics.
Methods
Data were drawn from a prospective randomized controlled trial enrolling 292 patients undergoing posterior lumbar interbody fusion. Patients received intrawound vancomycin powder (1 g) plus standard prophylaxis or standard prophylaxis alone. CRP was measured preoperatively and on days 1, 2, 3, 5, and 7. SSI was classified as overt (CDC criteria) or subclinical. ROC analysis evaluated prediction of any SSI at each time point.
Results
22 patients (7.5%) developed any SSI: 9 overt (3.1%) and 13 subclinical (4.5%). CRP peaked at day 5 in the overall cohort. SSI patients showed persistently elevated CRP through day 7, while uncomplicated patients declined after day 3. Day 7 CRP showed the highest discriminatory ability (AUC = 0.813; cutoff ≥79 mg/L; sensitivity 61.1%; specificity 91.4%; NPV 95.2%). Vancomycin did not alter CRP kinetics at any time point (all P > 0.08).
Conclusions
In 292 spine surgery patients, day 7 CRP (AUC = 0.813) was the strongest predictor of any SSI. A cutoff of 79 mg/L on day 7 provided NPV of 95.2%, supporting CRP as a rule-out biomarker. Day 3 CRP ≥92 mg/L (AUC = 0.761) offers early warning capability. CRP trajectories did not differ significantly between the vancomycin and control groups. ClinicalTrials.gov: NCT02631408; EudraCT: 2014-002096-29.
Keywords
Introduction
Surgical site infection (SSI) remains one of the most serious complications following spine surgery, with reported incidence rates of 0.7-12% depending on procedure type and SSI definition and a pooled incidence of approximately 3.1% in instrumented procedures.1–4 SSIs are associated with prolonged hospitalization, revision surgery, and significant health care costs.5,6 Early identification allows timely intervention and potentially improved outcomes.7,8
C-reactive protein (CRP) is an acute-phase reactant synthesized by hepatocytes in response to tissue injury and inflammation. 9 Following uncomplicated spine surgery, CRP typically peaks at 48-72 hours postoperatively (days 2-3) and declines toward baseline by day 7.10–13 A persistently elevated or secondary rising CRP may indicate an evolving infectious complication.14,15
Several studies have investigated CRP as a biomarker for SSI in orthopedic and spine surgery,16–19 but findings are inconsistent regarding optimal timing and cutoff values. Published thresholds range from 96 mg/L at day 5 to 150 mg/L at day 3.18,19 This heterogeneity reflects differences in patient populations, surgical procedures, and SSI definitions.
The present study reports a secondary analysis of the full cohort of a prospective randomized controlled trial, comprising both the control and vancomycin arms. Including both treatment arms and subclinical SSIs increases the study population and SSI event count, providing greater statistical power for threshold estimation.
We aimed to: (1) characterize postoperative CRP trajectories stratified by infection status; (2) determine optimal CRP thresholds for predicting any SSI (overt and subclinical combined); and (3) assess whether intraoperative vancomycin powder application affects CRP kinetics.
Materials and Methods
Study Design and Setting
This secondary analysis utilized data from both arms of a prospective, single-center, patient-blind randomized controlled trial conducted at our institution. The study was approved by the local ethics committee (approval no. 14-117-0814) and conducted in accordance with the 1964 Declaration of Helsinki and its later amendments. Trial registration: NCT02631408 (ClinicalTrials.gov); EudraCT 2014-002096-29. All patients provided written informed consent. Enrollment was conducted between August 2015 and April 2019.
Patient Population
Consecutive adult patients (≥18 years) undergoing elective posterior lumbar interbody fusion (PLIF; L1–S1; 1-2 fusion levels) were assessed for eligibility. Inclusion criteria required preoperative CRP ≤10 mg/L and written informed consent. Exclusion criteria included allergy to vancomycin or teicoplanin, prior spinal infection at the same level, immunosuppressive therapy, active malignancy, or refusal to participate. Of 308 randomized patients, 16 were excluded per protocol criteria, yielding 292 patients for the present analysis (control arm: n = 152, 52.1%; vancomycin arm: n = 140, 47.9%).
CRP Measurements
Serum CRP was measured by standard immunoturbidimetric assay at the following time points: preoperative baseline; postoperative days 1, 2, 3, 5, and 7. All patients received cefuroxime 3 g intravenously as standard perioperative antibiotic prophylaxis. Patients in the vancomycin arm additionally received 1 g of vancomycin powder applied directly to the surgical wound bed prior to fascial closure.
SSI definition and Surveillance
Overt SSI was defined per CDC/NHSN criteria, 20 classified as superficial incisional, deep incisional, or organ/space SSI. Subclinical SSI was defined as microbiological or clinical evidence of wound infection prompting antibiotic therapy but not meeting formal CDC/NHSN criteria. The primary outcome for ROC analysis was any SSI (overt + subclinical combined). Surveillance was conducted at hospital discharge, 6 weeks, and 1 year postoperatively.
Statistical Analysis
Continuous variables are reported as mean ± SD or median (interquartile range [IQR]). Group comparisons used the Mann–Whitney U test (two-sided). ROC curves were constructed for each postoperative time point; AUC was interpreted per established criteria: ≥0.90 excellent, 0.80-0.89 good, 0.70-0.79 fair, 0.60-0.69 poor. 21 Optimal cutoffs were determined by the Youden index (sensitivity + specificity −1). The significance level was set at α = 0.05. Separate ROC analyses were performed for overt SSI and subclinical SSI subgroups. Statistical analyses were performed using Python (version 3.x; pandas, SciPy, scikit-learn). Reporting followed STROBE guidelines. 22
Results
Patient Characteristics
Baseline Characteristics of the Study Cohort (N = 292). Data are presented as mean ± SD or n (%)

SSI Incidence
22 patients (7.5%) developed any SSI: 9 overt SSI (3.1%) and 13 subclinical SSI (4.5%). Among overt SSI cases: 3 superficial incisional, 2 deep incisional, 2 bone/joint infections, 1 discitis, and 1 spinal abscess. By treatment arm: overt SSI occurred in 6 control and 3 vancomycin patients (P = 0.50, Fisher exact test); subclinical SSI in 8 control and 5 vancomycin patients.
CRP Kinetics: Overall Cohort
CRP Kinetics in the Overall Cohort (N = 292)


Postoperative C-reactive protein trajectories in patients who developed any surgical site infection (SSI) versus those who did not. Overt SSI (n = 9, orange dashed line), subclinical SSI (n = 13, yellow dotted line), and no SSI (n = 270, blue solid line). Mean ± SEM. Asterisks indicate statistically significant differences between any SSI (n = 22) and no SSI (Mann–Whitney U test). Full cohort, N = 292
CRP Kinetics: Infection Status
Figure 1 shows CRP trajectories stratified by infection status. Patients who developed any SSI showed persistently elevated CRP at days 3 through 7. Uncomplicated patients reached their CRP peak at day 5 (mean 65.9 ± 44.7 mg/L) before declining toward day 7. The plateau between days 3 and 5 was statistically not different (Wilcoxon p = 0.40). Significant differences between any SSI and no SSI groups were observed at day 2 (P = 0.04), day 3 (P < 0.001), day 5 (P < 0.001), and day 7 (P < 0.001, Mann–Whitney U test). No significant differences were observed at preoperative or day 1 time points.
CRP Kinetics: Treatment Arm
CRP trajectories did not differ significantly between the vancomycin and control arms at any postoperative time point (Figure 2): preoperative P = 0.12; day 1 P = 0.64; day 2 P = 0.24; day 3 P = 0.09; day 5 P = 0.95; day 7 P = 0.47 (all Mann–Whitney U). The most pronounced between-group difference was observed on postoperative day 3 (P = 0.09), yet this did not reach statistical significance. Mean CRP values on day 3 were numerically lower in the vancomycin group, but the confidence intervals overlapped broadly. At all remaining time points, CRP levels were virtually identical between treatment arms. Intraoperative vancomycin powder application did not alter the systemic postoperative CRP response. Postoperative CRP trajectories by treatment arm: control (n = 152, blue) versus vancomycin (n = 140, purple). No statistically significant differences were observed at any time point (all p > 0.08). Mean ± SEM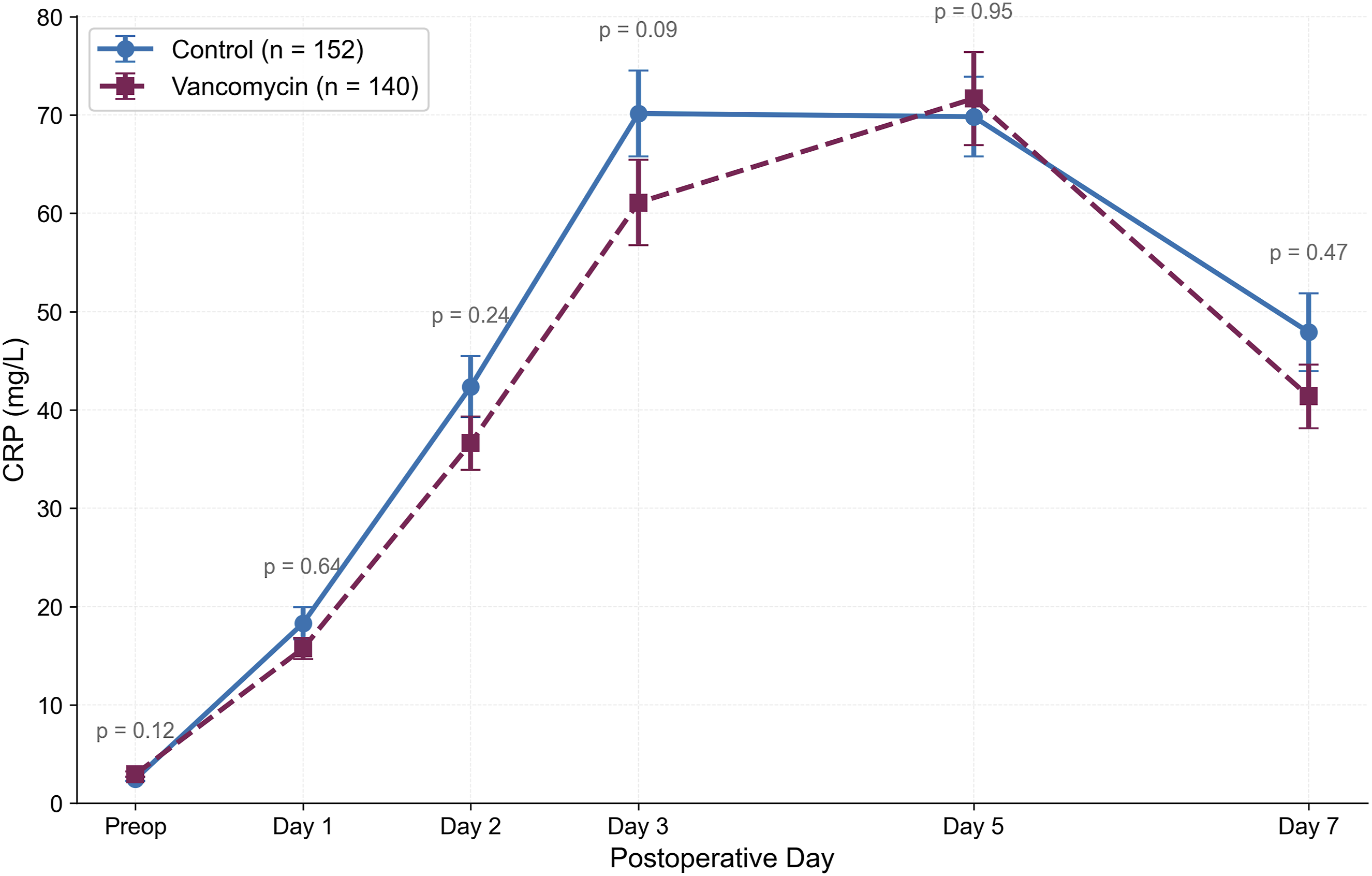
ROC Analysis and Diagnostic Performance
ROC curves are shown in Figure 3; diagnostic performance metrics are listed in Table 3. Day 7 CRP showed the highest discriminatory ability for any SSI (AUC = 0.813, P < 0.001) — in the ‘good’ range by standard criteria.
21
A cutoff of ≥79 mg/L on day 7 yielded 61.1% sensitivity, 91.4% specificity, PPV 45.8%, and NPV 95.2%. Day 3 CRP was the strongest early predictor (AUC = 0.761, P < 0.001; cutoff ≥92 mg/L: 66.7% sensitivity, 79.9% specificity, NPV 96.4%). Day 5 CRP also showed discriminatory ability (AUC = 0.757, P < 0.001; cutoff ≥124 mg/L). Early time points (preoperative, day 1) showed no clinically meaningful discriminatory ability (AUC <0.58). Receiver operating characteristic (ROC) curves for serum CRP at postoperative days 1, 2, 3, 5, and 7 for prediction of any SSI (overt + subclinical; n = 22 events). AUC values and optimal cutoffs (Youden index) shown for each time point. Day 7 CRP: AUC = 0.813 (highest discriminatory ability). Day 3 CRP: AUC = 0.761 (strongest early predictor). Dashed gray diagonal represents chance performance (AUC = 0.50) ROC Analysis — Any SSI (n = 22) vs No SSI (n = 270)

Discussion
In this secondary analysis of 292 lumbar spine surgery patients from a prospective RCT, day 7 CRP was the best-performing single biomarker for any SSI (AUC = 0.813) — a result in the ‘good’ range by standard criteria. 21 Including the vancomycin arm and subclinical SSI cases increased SSI events to 22, providing greater statistical precision for cutoff estimation.
SSI patients maintained elevated CRP through day 7 while uncomplicated patients showed progressive decline after day 5, consistent with established pathophysiology. The divergence between infected and uninfected patients became apparent from day 2 onward and reached statistical significance at days 3, 5, and 7. This trajectory pattern — rather than a single time-point measurement — may offer clinical utility for early SSI detection.
Our findings are in line with prior literature. Hoeller et al 13 identified day 7-8 CRP elevation as highly predictive of SSI after dorsal spondylodesis, reporting a sensitivity of 92.9% and specificity of 78.2% for a second CRP peak or failure to decline. Thelander and Larsson 19 proposed day 3 thresholds. Iwata et al 23 reported an AUC of 0.95 for a combined CRP and lymphocyte count model at day 7, though their analysis was limited to instrumented fusion cases and used a composite biomarker. Chen et al 24 identified day 7 CRP as the strongest single-marker predictor in a retrospective cohort (AUC = 0.908; cutoff ≥64.1 mg/L), corroborating day 7 as the optimal surveillance time point. A study on scoliosis correction surgery found limited diagnostic utility of early postoperative CRP (days 2-4), indicating that CRP’s predictive value depends on both procedure type and timing of measurement.25,26
In exploratory subgroup analysis, separate ROC analyses for overt SSI (n = 9) and subclinical SSI (n = 13) showed day 7 AUCs of 0.737 and 0.861, respectively. These subgroup analyses are limited by small event numbers and should be interpreted with caution.
Composite inflammatory indices may enhance SSI prediction beyond CRP alone. Pang et al 27 demonstrated that machine learning models integrating CRP-albumin-lymphocyte index and systemic immune-inflammatory biomarkers achieved high discrimination for SSI after posterior lumbar fusion. Salimi et al28–30 showed that the neutrophil-to-lymphocyte ratio carries diagnostic value for SSI prediction in spinal surgery. The preoperative CRP-to-albumin ratio has also been associated with SSI risk in spinal procedures.31,32 Future models may benefit from integrating CRP trajectories with such complementary markers.
Vancomycin powder prophylaxis did not significantly alter postoperative CRP trajectories compared to controls, with the most pronounced between-group difference observed on postoperative day 3 (P = 0.09). This finding is consistent with the pharmacological profile of locally applied vancomycin, which exerts predominantly topical antimicrobial activity with limited systemic absorption and, accordingly, minimal modulation of the systemic acute-phase response. The absence of a significant CRP difference between treatment arms carries a practical implication: postoperative CRP monitoring retains its diagnostic validity for SSI surveillance irrespective of whether vancomycin powder was used. Clinicians need not adjust CRP interpretation or thresholds based on intraoperative vancomycin application. 33
The high NPV (≥95% at days 3 and 7) supports the utility of CRP as a rule-out test. In the present cohort with 7.5% any-SSI prevalence (22/292), a CRP below threshold excluded SSI in over 95% of cases. This is relevant for antibiotic stewardship: CRP-guided decision support could help clinicians defer prolonged empiric antibiotics in patients with low postoperative CRP.34–36
Based on these findings, we propose a CRP monitoring algorithm: (1) routine CRP measurement on days 3 and 7; (2) day 7 CRP <79 mg/L as a low-risk threshold supporting continued observation or discharge; (3) day 7 CRP ≥79 mg/L prompting clinical reassessment and wound inspection; (4) day 3 CRP ≥92 mg/L as an early warning for heightened surveillance.
Limitations of this study include: moderate SSI sample size (n = 22) limiting power for subgroup analyses; single-center design limiting generalizability; incomplete CRP data at some time points due to early discharge (day 7 completeness 58.2%); and the retrospective nature of subclinical SSI classification. Future multi-center studies with prospective SSI classification and complementary biomarkers (neutrophil-to-lymphocyte ratio, procalcitonin, albumin) 37 are needed to validate these thresholds.
Conclusions
In this secondary analysis of a prospective RCT including 292 spine surgery patients, postoperative CRP trajectories discriminated between patients who developed any SSI and those who did not. Day 7 CRP (AUC = 0.813) was the strongest predictor. A cutoff of 79 mg/L on day 7 yielded NPV of 95.2%, supporting CRP as a rule-out biomarker. Day 3 CRP ≥92 mg/L (AUC = 0.761) provides early warning capability. CRP trajectories did not differ significantly between the vancomycin and control groups, indicating that intraoperative vancomycin powder does not confound CRP-based SSI surveillance. These findings support integration of day 3 and day 7 CRP monitoring into postoperative surveillance protocols for lumbar spine surgery.
Footnotes
Ethical Considerations
This study was approved by the Ethics Committee of the City of Vienna (Ethikkommission der Stadt Wien; approval no. EK 14-117-0814) and conducted in accordance with the 1964 Declaration of Helsinki and its later amendments.
Consent to Participate
All participants provided written informed consent.
Consent for Publication
Not applicable (no identifiable patient data presented).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a research grant from the German Spine Society (Deutsche Wirbelsäulengesellschaft, DWG; grant amount €18,000). The funding body had no role in study design, data collection, analysis, interpretation, or reporting.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
De-identified data from this study may be requested from the corresponding author, subject to institutional data sharing policies and patient privacy regulations.
Trial Registration
ClinicalTrials.gov: NCT02631408; EudraCT: 2014-002096-29
Artificial Intelligence Usage
Artificial intelligence tools were used to assist with manuscript preparation, statistical visualization, and language editing. All scientific content, data analysis, interpretation, and conclusions were reviewed, verified, and approved by the authors.