
Abstract
Study Design:
Retrospective cohort study.
Objectives:
Chronic steroid therapy is used in the treatment of various inflammatory and autoimmune conditions, but it is known to be associated with adverse effects. There remains a gap in the literature regarding the role of chronic steroid therapy in predisposing patients to perioperative complications following elective posterior lumbar fusion (PLF). We aimed to identify the effects of chronic preoperative steroid therapy on 30-day perioperative complications in patients undergoing PLF.
Methods:
A retrospective analysis was performed using the 2011-2014 American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database. We identified 22 903 patients who underwent elective PLF. There were 849 patients (3.7%) who received chronic preoperative steroid therapy. Univariate and multivariate analyses were performed to examine steroid therapy as an independent risk factor for 30-day perioperative complications. A subgroup analysis of patients on chronic steroid therapy was then performed to identify additional patient characteristics that further increased the risk for perioperative complications.
Results:
Chronic preoperative steroid therapy was an independent risk factor for 7 perioperative complications, including superficial surgical site infection (SSI), deep SSI, wound dehiscence, urinary tract infection, pulmonary embolism, nonhome discharge, and readmission. Subgroup analysis demonstrated that morbid obesity further predisposed patients on chronic steroid therapy to an increased risk of superficial SSI and wound dehiscence.
Conclusions:
Patients on chronic preoperative steroid therapy are at increased risk of multiple perioperative complications following elective PLF, particularly surgical site complications and venous thromboembolic events. This risk is further elevated in patients who are morbidly obese.
Keywords
Introduction
Corticosteroids are commonly used in the treatment and symptomatic management of various inflammatory and autoimmune conditions. 1 -3 Despite demonstrated beneficial effects, existing literature suggests that a strong correlation exists between chronic steroid use and surgical complications. 4 -7 To date, most studies have focused on the adverse effects of chronic steroid use following gastrointestinal surgery 5,8 -11 or neurosurgery. 12 -16 In comparison, relatively few studies have examined the effects of chronic steroid use in patients undergoing orthopedic procedures. 13,14,17,18 Furthermore, no studies have specifically addressed the effects of chronic steroid use in patients undergoing elective spine surgery.
Posterior lumbar fusion (PLF) is one of the most commonly performed surgical procedures in the treatment of spinal instability, spondylolisthesis, degenerative disc disease, and spinal trauma. 19,20 Despite generally good outcomes, PLF is an invasive procedure, often requiring extensive muscle dissection and prolonged hospital stays, with a high potential for postoperative complications. With more PLFs being performed every year, 19,21 it is becoming increasingly important to identify characteristics that predispose surgical candidates to a higher risk of complications. The primary objective of this study was to examine the effects of chronic preoperative steroid use on 30-day perioperative complications following elective PLF.
Materials and Methods
Data Source
This was a retrospective study of prospectively collected data from 2011 to 2014 in the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database. The ACS-NSQIP is a nationwide, multi-institutional database that collects more than 300 variables on patient demographics, comorbidities, perioperative characteristics, and 30-day postoperative complications from surgical procedures performed at more than 500 institutions. 22,23 Quality improvement studies using the ACS-NSQIP database have been shown to be successful in private sector hospitals, public academic institutions, and the Veterans Affairs (VA) Healthcare System. 24 -26
Cohort Selection
Adult patients aged 18 years or older undergoing elective PLF with or without an interbody fusion were identified based on the following Current Procedural Terminology (CPT) codes: 22 612, 22 630, and 22 633. Exclusion criteria included a diagnosis of pneumonia or sepsis, cardiopulmonary resuscitation prior to surgery, pregnancy, clean-contaminated surgical wound, contaminated surgical wound, dirty surgical wound, open wound, prior operation within 30 days, nonelective case, spinal trauma case, or neoplastic case. Cases with missing demographic, preoperative, intraoperative, or postoperative data were excluded.
Comparison Groups
Patients were divided into 2 groups. The steroid group included all patients who received regular administration of oral or parenteral steroids to treat a chronic condition for more than 10 days in the 30-day period prior to surgery. All other patients were included in the nonsteroid group.
Baseline Patient Characteristics
Patient demographics consisted of age, sex, and race. Age was defined as a dichotomous variable (ie, <65 years or ≥65 years). Race was divided into 4 categories (ie, white, black, Hispanic, or other).
Preoperative patient characteristics included medical comorbidities, functional status, and operative variables. Medical comorbidities included diabetes, smoking within 1 year of surgery, pulmonary comorbidity (chronic obstructive pulmonary disease or ventilator dependence within 48 hours prior to surgery), cardiac comorbidity (hypertensive medication use or chronic heart failure), renal comorbidity (dialysis within 2 weeks or acute renal failure within 24 hours prior to surgery), obesity classification (class I = body mass index [BMI] 30.0-34.9 kg/m2, class II = BMI 35.0-39.9 kg/m2, class III = BMI ≥40.0 kg/m2), and acute or chronic bleeding disorder. Functional status variables included American Society of Anesthesiologists (ASA) physical status classification ≥3, dyspnea at rest within 30 days prior to surgery, and partially or totally dependent functional status. Operative variables included length of the fusion (short fusion <4 levels or long fusion ≥4 levels), pelvic fixation, surgical setting (inpatient or outpatient), year of the operation (2011, 2012, 2013, or 2014) and prolonged operative time >4 hours.
Perioperative Complications
The primary outcomes were 30-day postoperative mortality and complications. Complications included reoperation, sepsis, superficial surgical site infection (SSI), deep SSI, organ space infection, wound dehiscence, pulmonary complications (pneumonia, postoperative reintubation, or failure to wean from a ventilator after 48 hours), renal complications (progressive renal insufficiency or acute renal failure), pulmonary embolism (PE), deep vein thrombosis (DVT), urinary tract infection (UTI), intra- or postoperative transfusion of packed red blood cells or whole blood, prolonged length of stay (LOS) ≥5 days, nonhome discharge to a care facility, and unplanned readmission. Further details about the definitions of variables and complications are provided by the ACS-NSQIP database. 22
Statistical Analysis
A univariate analysis was performed on patient demographics, preoperative, intraoperative, and postoperative characteristics in the 2 groups using Pearson’s chi-square test. Statistical significance was set at a level of P = .05. Characteristics that resulted in a P value <.20 on univariate analysis were included in a multivariate regression (MVR) analysis adjusting for patient demographics, comorbidities, preoperative and intraoperative variables.
A subgroup analysis was then performed on the steroid group. Patients were divided into subgroups based on whether or not they experienced at least one perioperative complication for which steroid use was found to be an independent risk factor. A univariate analysis was performed on patient demographics, preoperative, intraoperative, and postoperative characteristics between the 2 subgroups using Pearson’s chi-square test. Statistical significance was again set at a level of P = .05. Characteristics that resulted in a P value <.20 on univariate analysis were subsequently included in an MVR analysis adjusting for patient demographics, comorbidities, preoperative and intraoperative variables. MVR models were constructed for each of the complications previously determined to be independently associated with steroid use. All MVR models in both the primary and subgroup analyses used a stepwise entry and removal criteria set to a statistical significance level of P = .05. Odds ratios (ORs) and 95% confidence intervals (CIs) were reported. All statistical analyses were performed using SAS Studio Version 3.4 (SAS Institute Inc, Cary, NC, USA).
Results
Study Population
A total of 22 903 patients met the selection criteria and were included in our analysis. The steroid group included 849 patients (3.7%). As shown in Table 1, patients who received preoperative steroid therapy were more likely to be female (P < .001), age ≥65 years (P < .001), have an ASA classification ≥3 (P < .001), and be either partially or totally dependent on presentation to the hospital (P < .001). Additionally, patients on a steroid regimen were more likely to have dyspnea (P < .001), diabetes (P = .011), bleeding disorder (P < .001), pulmonary comorbidity (P < .001), or cardiac comorbidity (P < .001). Patients in the steroid cohort were less likely to be smokers (P < .001). Finally, the steroid group had a greater proportion of patients who underwent a long fusion (P = .038).
Baseline Patient Characteristics Including Medical Comorbidities at the Time of Surgery, Preoperative Condition, and Operative Variables.
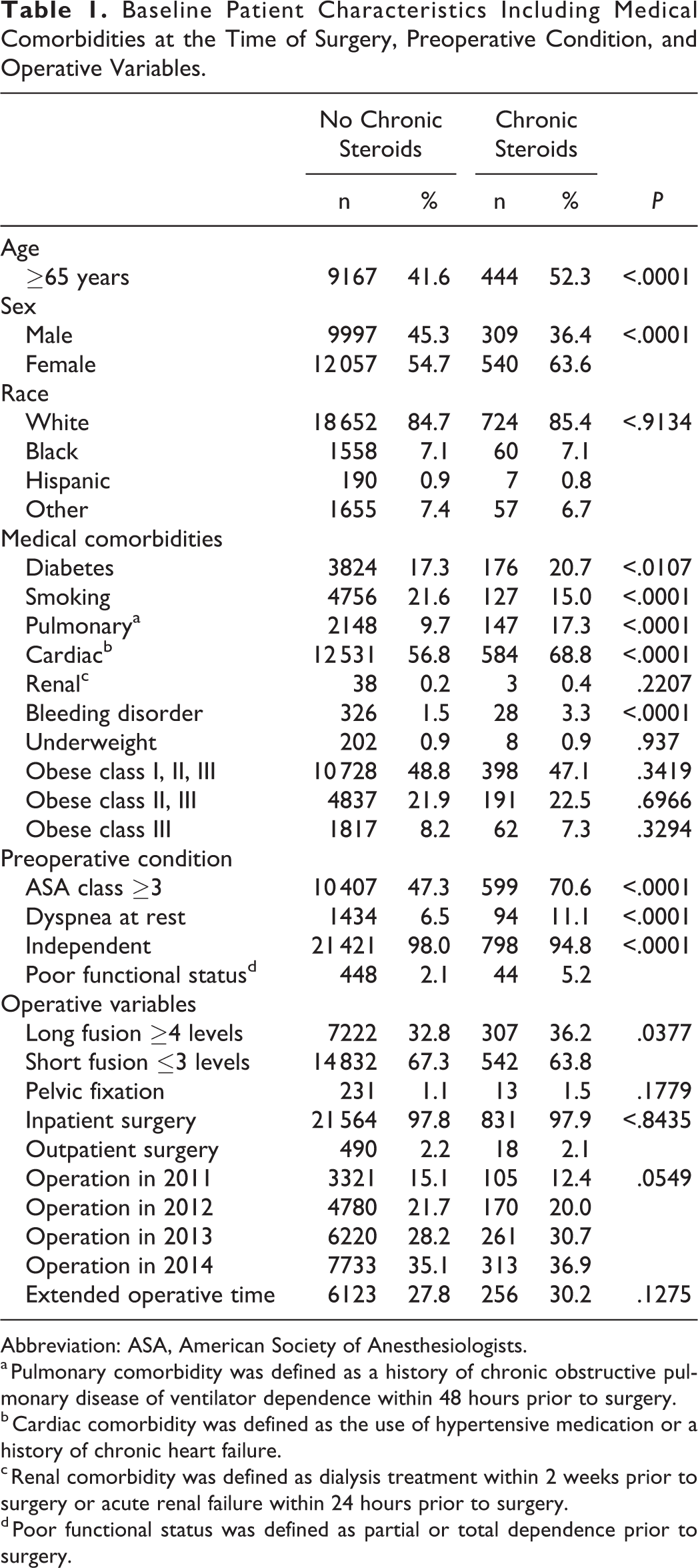
Abbreviation: ASA, American Society of Anesthesiologists. a Pulmonary comorbidity was defined as a history of chronic obstructive pulmonary disease of ventilator dependence within 48 hours prior to surgery.
b Cardiac comorbidity was defined as the use of hypertensive medication or a history of chronic heart failure.
c Renal comorbidity was defined as dialysis treatment within 2 weeks prior to surgery or acute renal failure within 24 hours prior to surgery.
d Poor functional status was defined as partial or total dependence prior to surgery.
Unadjusted Analysis
Results of the univariate analysis are summarized in Table 2. Chronic preoperative steroid use was significantly associated with prolonged LOS (nonsteroid, 21.6%; steroid, 26.5%; P < .001), superficial SSI (nonsteroid, 1.0%; steroid, 2.2%; P < .001), deep SSI (nonsteroid, 0.7%; steroid, 1.5%; P = .005), organ space SSI (nonsteroid, 0.2%; steroid, 0.7%; P = .007), wound dehiscence (nonsteroid, 0.3%; steroid, 0.7%; P = .016), PE (nonsteroid, 0.5%; steroid, 1.1%; P = .013), UTI (nonsteroid, 1.7%; steroid, 3.1%; P = .002), intra- or postoperative red blood cell transfusion (nonsteroid, 14.9%; steroid, 20.1%; P < .001), sepsis (nonsteroid, 0.9%; steroid, 1.5%; P = .043), nonhome discharge (nonsteroid, 17.5%; steroid, 26.9%; P < .001), and unplanned readmission (nonsteroid, 4.2%; steroid, 7.2%; P < .001). There was no significant difference in 30-day mortality between the 2 groups (P = .790).
Univariate Analysis of 30-day Perioperative Mortality and Complications in the No Chronic Steroid and Chronic Steroid Groups.
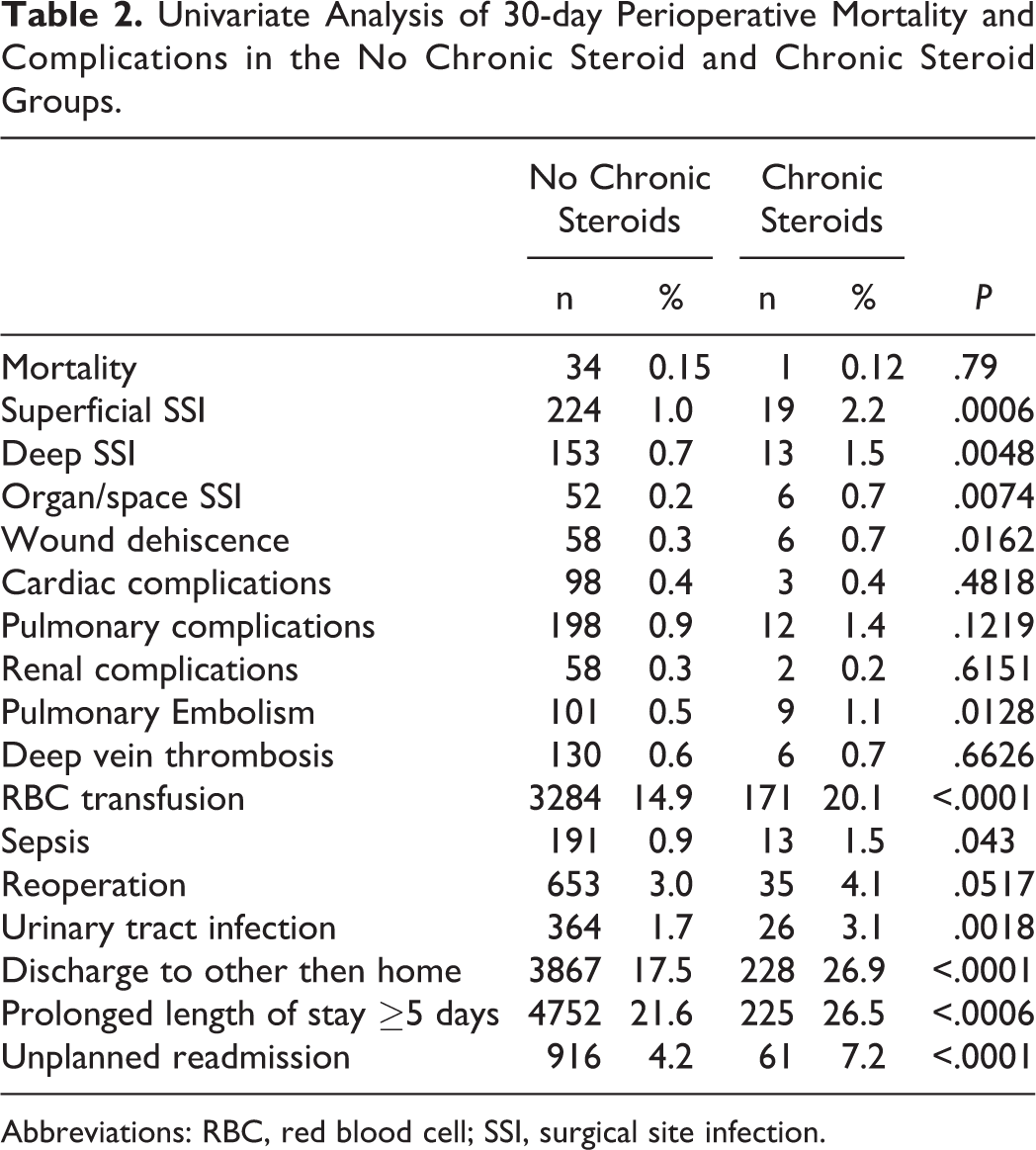
Abbreviations: RBC, red blood cell; SSI, surgical site infection.
Multivariate Analysis
MVR analysis demonstrated that chronic preoperative steroid use was independently associated with 7 perioperative complications (Table 3). Steroid use was independently associated with wound complications, including superficial SSI (OR, 2.38; 95% CI, 1.48-3.82; P < .001), deep SSI (OR, 1.90; 95% CI, 1.06-3.38; P = .029), and wound dehiscence (OR, 2.58; 95% CI, 1.10-6.01; P = .029). Additionally, steroid use was associated with an increased risk of PE (OR, 2.15; 95% CI, 1.08-4.27; P = .030), unplanned readmission (OR, 1.58; 95% CI, 1.20-2.08; P = .001), UTI (OR, 1.53; 95% CI, 1.01-2.30; P = .044), and nonhome discharge (OR, 1.23; 95% CI, 1.03-1.46; P = .019).
Multivariate Regression of Chronic Steroid Use as a Predictor of Perioperative Complications in all Patients Undergoing Elective PLF.
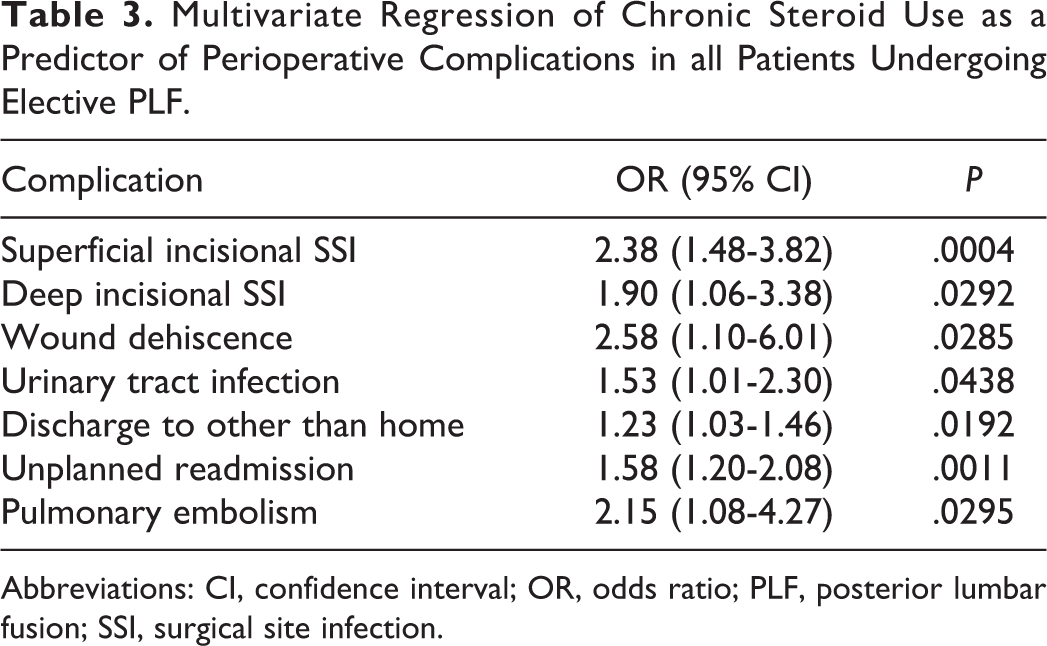
Abbreviations: CI, confidence interval; OR, odds ratio; PLF, posterior lumbar fusion; SSI, surgical site infection.
Subgroup Univariate Analysis
Results of the subgroup univariate analysis are outlined in Table 4. The no complication subgroup was significantly different from the ≥1 complication subgroup in terms of gender (P < .001), age (P < .001), diabetes (P = .005), dyspnea (P < .001), dependent functional status (P < .001), pulmonary comorbidity (P = .007), cardiac comorbidity (P < .001), underweight (P < .001), obesity class II or III (P = .048), obesity class III (P = .002), and ASA classification ≥3 (P < .001). Operative variables that were associated with a higher incidence of any perioperative complications were long fusion (no complication, 31.5%; ≥1 complication, 45.6%; P < .001), inpatient setting (no complication, 97.2%; ≥1 complication, 99.3%; P = .043), and prolonged operative time (no complication, 26.5%; ≥1 complication, 37.5%; P = .001). Smoking was associated with a lower incidence of any complication (no complication, 17.0%; ≥1 complication, 11.0%; P < .001).
Univariate Regression of Demographic, Preoperative and Intraoperative Characteristics for Chronic Steroid Users (subgroup) Undergoing Elective PLF.
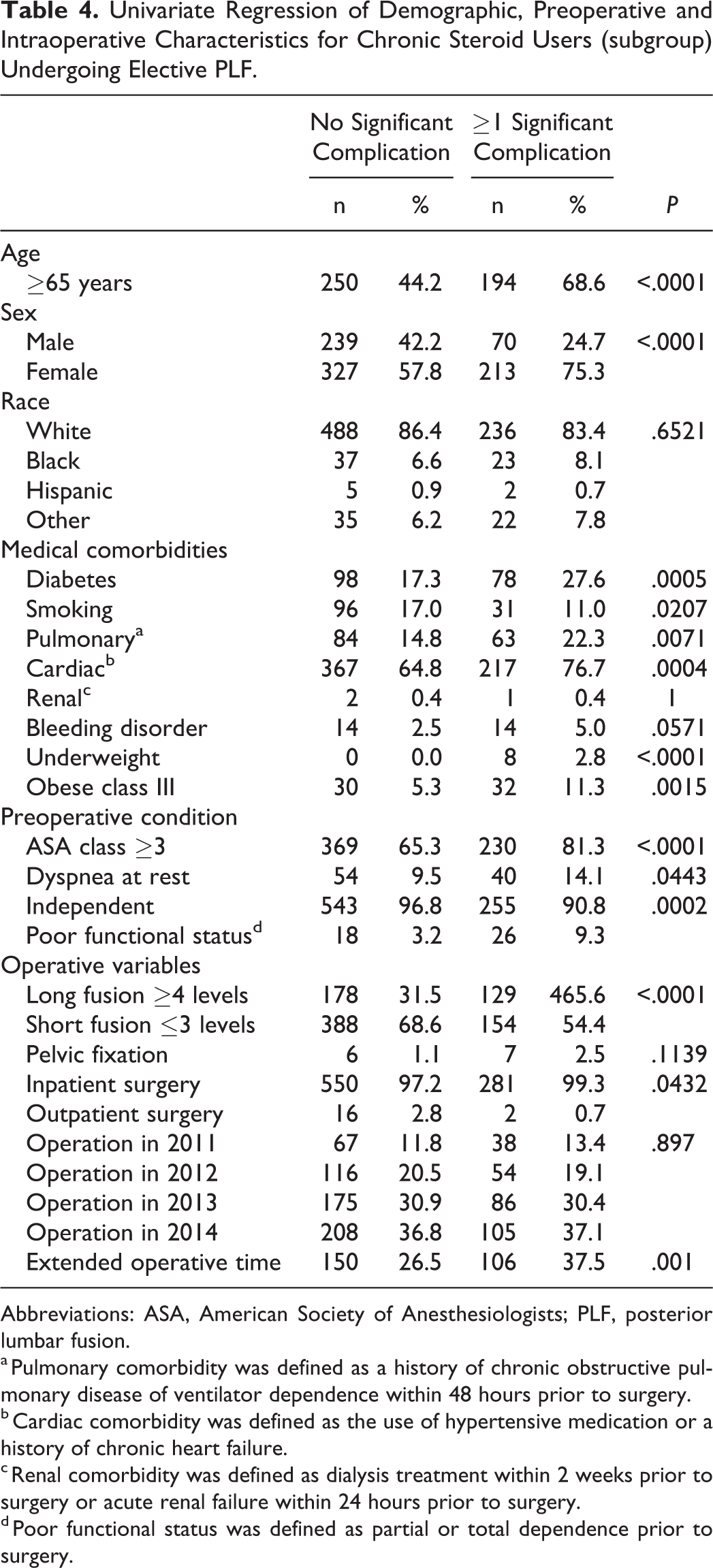
Abbreviations: ASA, American Society of Anesthesiologists; PLF, posterior lumbar fusion.
a Pulmonary comorbidity was defined as a history of chronic obstructive pulmonary disease of ventilator dependence within 48 hours prior to surgery.
b Cardiac comorbidity was defined as the use of hypertensive medication or a history of chronic heart failure.
c Renal comorbidity was defined as dialysis treatment within 2 weeks prior to surgery or acute renal failure within 24 hours prior to surgery.
d Poor functional status was defined as partial or total dependence prior to surgery.
Subgroup Multivariate Analysis
Results of the subgroup MVR analyses are outlined in Table 5. Morbid obesity was an independent risk factor for superficial SSI (OR, 8.13; 95% CI, 3.08-21.47; P < .001) and wound dehiscence (OR, 13.14; 95% CI, 2.59-66.51; P = .002). Bleeding disorder was predictive of deep SSI (OR, 5.83; 95% CI, 1.23-27.71; P = .027). Perioperative UTI was associated with age ≥65 years (OR, 4.61; 95% CI, 1.56-13.64; P = .006), pulmonary comorbidity (OR, 2.83; 95% CI, 1.23-6.51; P = .015), and prolonged operative time (OR, 3.35; 95% CI, 1.50-7.49; P = .003). Nonhome discharge was associated with many risk factors, including female sex (OR, 2.99; 95% CI, 2.02-4.42; P < .001), age ≥65 years (OR, 3.60; 95% CI, 2.49-5.21; P < .001), morbid obesity (OR, 2.97; 95% CI, 1.60-5.53; P < .001), diabetes (OR, 1.67; 95% CI, 1.12-2.51; P = .013), dependent functional status (OR, 4.02; 95% CI, 1.98-8.17; P < .001), long fusion (OR, 2.09; 95% CI, 1.46-2.98; P < .001), inpatient setting (OR, 8.58; 95% CI, 1.06-69.42; P = .044), prolonged operative time (OR, 1.61; 95% CI, 1.12-2.33; P = .011), and ASA classification ≥3 (OR, 1.82; 95% CI, 1.19-2.78; P = .006).
Multivariate Regressions (Grouped by Complication) Identifying Additional Patient Characteristics as Risk Factors for Perioperative Complications in Chronic Steroid Users Undergoing Elective PLF.
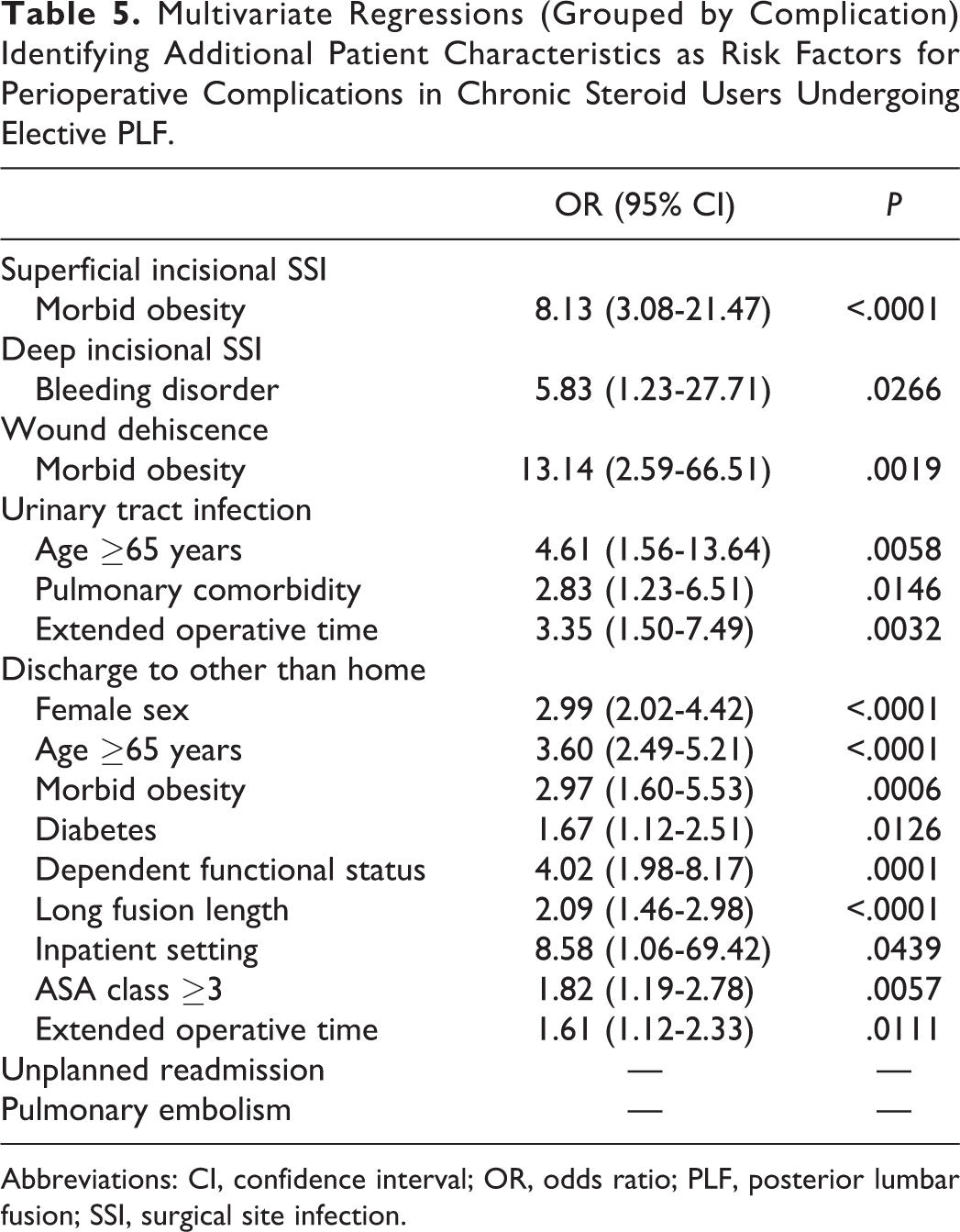
Abbreviations: CI, confidence interval; OR, odds ratio; PLF, posterior lumbar fusion; SSI, surgical site infection.
Discussion
In this ACS-NSQIP database study of patients undergoing PLF, we found that chronic preoperative steroid use was associated with an increased risk of 30-day perioperative complications, including superficial SSI, wound dehiscence, PE, deep SSI, unplanned readmission, UTI, and nonhome discharge. Subgroup analysis revealed additional risk factors for perioperative complications, including age ≥65 years, morbid obesity, bleeding disorder, pulmonary comorbidity, and prolonged operative time.
Chronic steroid use was associated with a 2 times increased risk of superficial SSI and deep SSI, as well as a 2.5 times increased risk of wound dehiscence. PLFs are lengthy and invasive procedures with extensive muscle dissection, high intraoperative blood loss, and urethral catheterization that contribute to a high risk of bacterial colonization and subsequent infection. 27 A well-understood anti-inflammatory effect of steroid therapy is achieved through immunosuppression. On absorption, steroids enter the cell nucleus and downregulate pro-inflammatory genes such as NF-κB and AP-1, 28,29 while upregulating anti-inflammatory genes such as IL-10 and GILZ. 30,31 This results in impaired leukocyte chemotaxis, adhesion, and phagocytosis, 32 leading to decreased ability to eliminate pathogens and increased risk of infection. 32 Additionally, given the established correlation between incision size and impaired wound healing, wound complications is also a significant concern with extensive PLF procedures. 33,34
Wound healing is a complex balance of many pro- and anti-inflammatory cytokines working in sequence to orchestrate interactions among various cell types. 35 -37 In particular, the pro-inflammatory cytokines interleukin 1 (IL-1) and tumor necrosis factor α (TNF-α) serve to regulate the effect of collagenase in scar formation and wound remodeling. 36 -38 The mechanism of wound dehiscence with chronic steroid use is likely 2-fold. First, glucocorticoids downregulate the activity of NF-κB, thereby decreasing the levels of circulating IL-1. 28,29 This, in turn, impairs collagen deposition and remodeling, which diminishes the tensile strength of the resulting scar and increasing the risk of wound dehiscence. 39,40 Second, downregulation of NF-κB impairs immune cell function, which increases the risk of infection. In turn, SSI has been shown to be an independent predictor of wound dehiscence. 34 Impaired wound healing associated with chronic steroid use, combined with long incisions that are often necessary for PLF procedures, leads to an increased risk of surgical site complications. 41
Chronic steroid use was also associated with a 2 times increased risk of PE. Steroids induce a hypercoagulable state by increasing levels of prothrombin and Von Willebrand factor, as well as decreasing levels of plasminogen. 42 Steroids may also cause endothelial damage and vascular wall dysfunction, further increasing the risk of a venous thromboembolic (VTE) event. 43 While the prothrombotic effects of steroids are understood at a molecular level, few studies have attempted to quantify the clinical risk of VTE events associated with steroid therapy. 42 -44 The increased risk of PE associated with chronic steroid use in this study highlights the importance of postoperative mechanical VTE prophylaxis and early mobilization.
Our subgroup analysis further identified morbid obesity as an additional risk factor for perioperative complications in patients on chronic steroid therapy following elective PLF. Specifically, morbid obesity was associated with an 8 times increased risk of superficial SSI and a 13 times increased risk of wound dehiscence. This is consistent with findings from prior studies, including a recent meta-analysis that reported a 21% increase in the risk of SSI following spine surgery for every 5 unit increase in BMI. 45
There is no general consensus about the mechanism of obesity’s effect on surgical site complications. One theory is that a thick subcutaneous layer of fat may decrease perfusion of the dead space, subsequently decreasing penetration of immune cells and local oxygen saturation at the surgical site. Prolonged hypoxia leads to local tissue necrosis, thereby increasing the risk of SSI and wound dehiscence. 46 -48 Alternatively, a thick subcutaneous layer of fat may increase tension along the surgical incision, potentially impairing myofibroblast-mediated wound contraction and contributing to subsequent wound complications. 49,50 Patients who are both morbidly obese and on chronic steroid therapy have a significantly elevated risk of wound complications following PLF. This is of particular significance in the United States where the prevalence of morbid obesity has reached 8.1% and is continuing to increase at an unprecedented rate. 51 For morbidly obese patients who are indicated for an elective PLF, preoperative weight loss should be strongly encouraged and spine surgeons may also consider referring patients for bariatric surgery prior to an elective PLF in order to reduce perioperative complications associated with morbid obesity.
Given the elevated risk for perioperative complications associated with steroid therapy, holding steroids preoperatively could theoretically minimize steroid-associated complications. However, completely stopping steroids may not be medically feasible for some patients. For example, in organ transplant recipients where the risks of organ rejection significantly outweigh the risks of steroid-associated surgical complications. 52 However, in those patients who are amenable to a brief period of being off steroids without significant complications or rebound symptoms, the exact timing of when to hold steroids preoperatively and when to resume steroids postoperatively must be addressed.
Chronic suppression of the hypothalamic-pituitary-adrenal (HPA) axis by exogenous steroids may cause adrenal atrophy and prevent endogenous production of cortisol, which may lead to circulatory collapse and death in the setting of increased stress from surgery. 53,54 Therefore, steroids should ideally be held far enough in advance of surgery in order to allow for immunosuppression to wane and endogenous steroid production to return to baseline levels. The adrenal glands recover at a highly variable rate, from as short as 48 hours to longer than a year after stopping steroid therapy depending on the dosing and length of steroid therapy. 55 Return of adrenal function can be confirmed with preoperative measurements of blood cortisol levels, cosyntropin stimulation test, or an insulin intolerance test. 56 The exact timing of stopping and resuming steroid therapy in the perioperative period should be determined on a case-by-case basis through an interdisciplinary approach with the patient’s medical providers.
This study has several limitations. First, the ACS-NSQIP database does not indicate the medical condition for which patients are on chronic steroid therapy. While the underlying condition is likely to have been included in one or more of the medical comorbidities that were adjusted for in our analyses, the lack of diagnostic data limits the ability of this study to fully control for potential confounding variables. Second, the data set does not include details on the specific type or dose of steroid used. Different types and doses of steroids may have a different impact on perioperative outcomes. Third, the ACS-NSQIP data is primarily collected by academic institutions, and therefore, our findings in this study may not reflect operative trends or outcomes in the community setting. Finally, the ACS-NSQIP database only reports complications within a 30-day postoperative period and thus, we were unable to assess the long-term outcomes associated with preoperative steroid use.
This study used the ACS-NSQIP database to identify 30-day complications following elective PLF that were associated with chronic preoperative steroid use. Complications that occurred more frequently in patients on chronic steroid therapy were—from most to least common—superficial SSI, wound dehiscence, PE, deep SSI, unplanned readmission, UTI, and nonhome discharge. Subgroup analysis demonstrated that morbid obesity conferred an additional increased risk for wound complications. While complete elimination of steroid administration in the preoperative period may not be possible for all patients undergoing elective PLF, interdisciplinary management of perioperative steroid regimens with the goal of reducing or holding preoperative steroids is critical in order to reduce steroid-associated perioperative complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.