
Abstract
Study Design:
Retrospective cohort study.
Objectives:
The prevalence of obesity-related low back pain and degenerative disc disease is on the rise. Past studies have demonstrated that obesity is associated with higher perioperative complication rates, but there remains a gap in the literature regarding additional risk factors that further predispose this already high-risk patient population to poor surgical outcomes following elective posterior lumbar fusion (PLF). The aim of the study is to identify independent risk factors for poor 30-day perioperative outcomes in morbidly obese patients undergoing elective PLF.
Methods:
We identified 22 909 patients in the American College of Surgeons National Surgical Quality Improvement Program database who underwent elective PLF. There were 1861 morbidly obese patients. Baseline patient demographics and medical comorbidities were collected. Univariate analysis was performed to compare perioperative complication rates between non-morbidly obese and morbidly obese patients. The 5 most common complications in the morbidly obese group were then selected for multivariate regression analysis to identify independent risk factors for poor 30-day outcomes.
Results:
Morbidly obese patients had a higher perioperative complication rate. The 5 most common complications were prolonged hospitalization, blood transfusion, readmission, wound complications, and reoperation. Independent risk factors for these complications were age ≥65 years, super obesity (ie, BMI > 48.6), chronic steroid use, American Society of Anesthesiology classification ≥3, poor functional status, long length of fusion ≥4 levels, and extended operative time (ie, operative time ≥318 minutes).
Conclusions:
Morbidly obese patients are at higher risk of perioperative complications following elective PLF. Modifiable risk factors for the most common complications are obesity and preoperative steroid use.
Keywords
Introduction
According to recent data from the 2013-2014 National Health and Nutrition Examination Survey, the obesity rate in the United States continues to rise, with 38.2% of the population over 20 years of age now considered obese. 1 Even more startling is the rate of morbid obesity (ie, body mass index [BMI] ≥40 kg/m2), which has reached 8.1%, an increase of over 3 million individuals in just 2 years. 1 This rising prevalence of morbid obesity has led to increasing rates of obesity-related low back pain and degenerative disc disease, for which patients may eventually seek surgical intervention. 2 –8
Posterior lumbar fusion (PLF) is routinely utilized to treat a variety of spinal pathologies, including degenerative disc disease, instability, spondylolisthesis, deformity, and trauma. 9,10 The recent increase in the number of PLF surgeries performed in patients over 40 years of age is thought to be primarily attributable to degenerative disc disease. 11,12 With an aging population and a worsening obesity epidemic in the United States, spine surgeons will likely see an increasing number of morbidly obese patients who are surgical candidates for PLF, and they must be prepared to address the unique challenges that come with treating and operating on this population. 13 –17
Obese patients have a significantly higher comorbidity burden, with overwhelming data now pointing to an association between obesity and hypertension, coronary artery disease, congestive heart failure, and diabetes mellitus. 17 –23 Furthermore, morbidly obese patients tend to have poorer quality of preoperative imaging, increased difficulty during the surgical approach due to excess subcutaneous fat deposits, and enhanced difficulty in intraoperative anesthetic management. 14,24,25 Not surprisingly, many studies have shown a significantly higher rate of perioperative complications in morbidly obese patients. 15,26,27
Recent advances in anesthetic and surgical management, however, have made PLF an increasingly viable and safe option for morbidly obese patients, and the rate of spinal surgery in this patient population has risen in recent years. 26,28 –30 Current data suggests that although morbid obesity is associated with higher perioperative complications, it is not a contraindication to PLF. 14 –16,27,31 However, there are currently no studies in the literature that examine patient characteristics and comorbidities that independently predict poor perioperative outcomes in the morbidly obese patient population. In this study, we aim to use a national surgical outcomes database to identify patient characteristics and comorbidities that independently predict perioperative complications following elective PLF in morbidly obese patients.
Materials and Methods
ACS-NSQIP Database
This was a retrospective study of prospectively collected data from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database. The ACS-NSQIP is a nationwide, multi-institutional database that collects more than 300 variables on patient demographics, comorbidities, perioperative characteristics, and 30-day postoperative complications and mortality from surgical procedures performed at over 500 institutions from 2011 to 2014. 32 –35 Quality improvement projects based on analysis of ACS-NSQIP data have been shown to be successful in the Veterans Affairs (VA) Healthcare System, private sector hospitals, and public academic institutions. 36 –38
Cohort Selection
Adult patients aged 18 years or older undergoing elective PLF with or without an interbody fusion were identified based on the following Current Procedural Terminology codes: 22 612, 22 630, and 22 633. Patients with pneumonia, sepsis, or cardiopulmonary resuscitation prior to surgery were excluded. Pregnant patients were also excluded. Patients with a clean-contaminated, contaminated, or dirty surgical wound (ie, surgical wound classes II, III, or IV) were excluded. Patients with an open wound or prior operation within 30 days were excluded. Additionally, cases that were nonelective or involved spinal trauma or neoplasm were excluded. Cases with missing demographic, preoperative, intraoperative, or postoperative data were excluded.
Comparison Groups
Patients were divided into 2 groups according to BMI. The morbidly obese group included patients with a BMI ≥40 and the non-morbidly obese group included patients with a BMI <40. Within the morbidly obese group, patients with a BMI greater than 1 standard deviation above the mean (ie, BMI >48.6) were further categorized into a super obese group.
Baseline Patient Characteristics
Patient demographics consisted of age, sex, and race. Age was defined as a dichotomous variable, with patients being divided into <65 years or ≥65 years of age. Race was divided into 4 categories (ie, white, black, Hispanic, or other), with the “other” group including American Indian or Alaskan Native, Asian, Native Hawaiian or Pacific Islander, or unknown. Preoperative patient characteristics included medical comorbidities, functional status, and intraoperative variables.
Medical comorbidities included diabetes, smoking within 1 year of surgery, chronic obstructive pulmonary disease or ventilator dependence within 48 hours prior to surgery, hypertensive medication use or chronic heart failure, dialysis within 2 weeks prior to surgery or acute renal failure within 24 hours prior to surgery, acute or chronic bleeding disorder, and steroid use for a chronic condition within 30 days prior to surgery. Functional status variables included American Society of Anesthesiology (ASA) physical status classification ≥3, dyspnea at rest within 30 days prior to surgery, and partially or totally dependent functional status. Operative variables included length of the fusion (short <4 levels or long ≥4 levels), pelvic fixation, surgical setting (inpatient or outpatient), year of the operation (2011, 2012, 2013, or 2014), and operative time. Extended operative time was defined as an operative time greater than 1 standard deviation above the mean in the morbidly obese group (ie, 318 minutes).
Perioperative Complications and Mortality
The primary outcomes were 30-day postoperative mortality and complications. Complications included reoperation, sepsis, wound complications (deep surgical site infection, organ space infection, wound dehiscence), cardiac complications (cardiac arrest requiring cardiopulmonary resuscitation, myocardial infarction), pulmonary complications (pneumonia, postoperative reintubation, failure to wean from a ventilator after 48 hours), renal complications (progressive renal insufficiency, acute renal failure), venous thromboembolism (pulmonary embolism, deep vein thrombosis), urinary tract infection (UTI), intra- or postoperative transfusion of packed red blood cells or whole blood, prolonged length of stay (LOS) ≥5 days, and unplanned readmission. Further details about the definitions of variables and perioperative complications are provided by the ACS-NSQIP database. 35
Statistical Analysis
A univariate analysis was performed on patient demographics and preoperative, intraoperative, and postoperative characteristics between the 2 comparison groups using Pearson’s χ2 test and Fischer’s exact test as appropriate. The 5 most common perioperative complications in the morbidly obese group were then selected for multivariate regression (MVR) analysis while adjusting for patient demographics, comorbidities, and preoperative and intraoperative variables. MVR models utilized a stepwise entry and removal criteria set to a statistical significance level of P = .05. An original statistical significance level of P = .05 was chosen, but utilization of the Bonferroni correction resulted in a statistical significance level of P = .01. Odds ratios (ORs) and 95% confidence intervals (CIs) were reported. All statistical analyses were performed using SAS Studio Version 3.4 (SAS Institute Inc, Cary, NC).
Results
Study Population
A total of 22 909 patients who underwent elective PLF from 2011 to 2014 met the inclusion criteria. There were 1881 patients (8.2%) with a BMI ≥40 in the morbidly obese group. Of the 1881 patients, 20 patients were missing baseline demographics and preoperative, intraoperative, and/or postoperative data, and they were excluded from subsequent analyses, resulting in a total of 1861 patients in the morbidly obese group. The mean BMI in the morbidly obese group was 44.2 ± 4.4. There were 237 patients (1.0%) with a BMI >48.6 in the super obese subgroup. Baseline patient characteristics in the non-morbidly obese and morbidly obese groups are summarized in Table 1. The incidence of at least one perioperative complication was significantly higher in the morbidly obese group (41.6% vs 33.6% in the non-morbidly obese group; P < .001).
Baseline Patient Characteristics Including Medical Comorbidities at the Time of Surgery, Preoperative Condition, and Operative Variables.
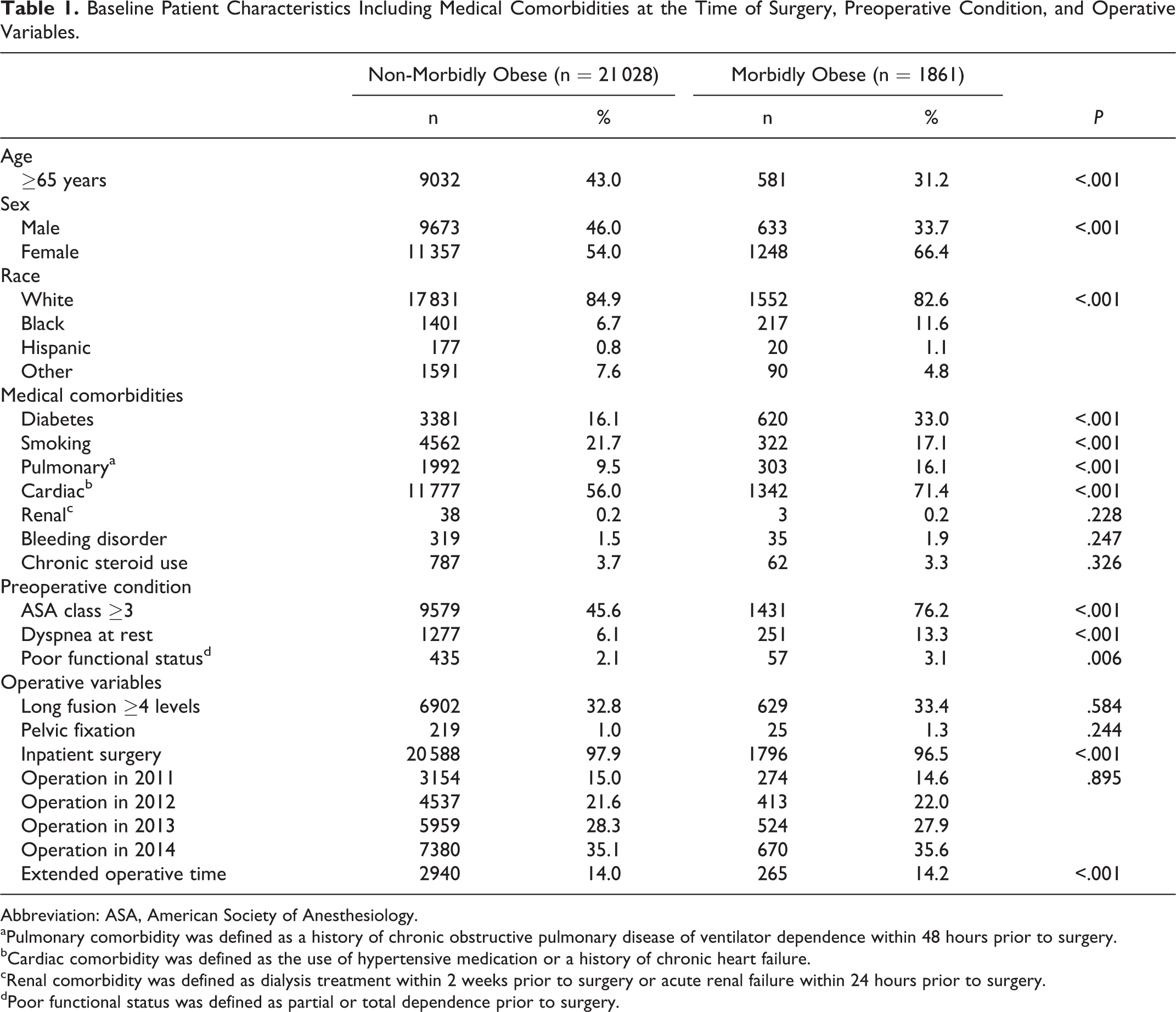
Abbreviation: ASA, American Society of Anesthesiology.
aPulmonary comorbidity was defined as a history of chronic obstructive pulmonary disease of ventilator dependence within 48 hours prior to surgery.
bCardiac comorbidity was defined as the use of hypertensive medication or a history of chronic heart failure.
cRenal comorbidity was defined as dialysis treatment within 2 weeks prior to surgery or acute renal failure within 24 hours prior to surgery.
dPoor functional status was defined as partial or total dependence prior to surgery.
Univariate Analysis
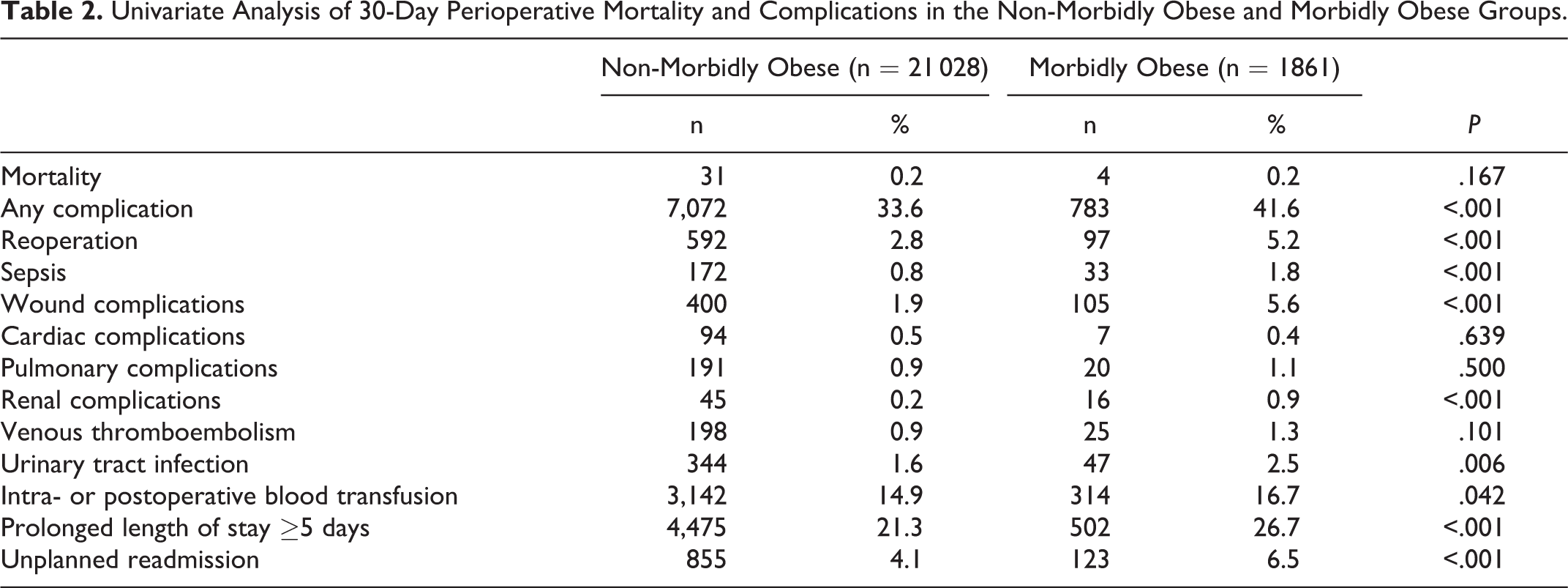
Results of the univariate analysis are summarized in Table 2. Morbid obesity was significantly associated with reoperation (non-morbidly obese, 2.8%; morbidly obese, 5.2%; P < .001), sepsis (non-morbidly obese, 0.8%; morbidly obese, 1.8%; P < .001), surgical site complications (non-morbidly obese, 1.9%; morbidly obese, 5.6%; P < .001), renal complications (non-morbidly obese, 0.2%; morbidly obese, 0.9%; P < .001), UTI (non-morbidly obese, 1.6%; morbidly obese, 2.5%; P = .006), intra- or postoperative blood transfusion (non-morbidly obese, 14.9%; morbidly obese, 16.7%; P = .042), prolonged LOS (non-morbidly obese, 21.3%; morbidly obese, 26.7%; P < .001), and unplanned readmission (non-morbidly obese, 4.1%; morbidly obese, 6.5%; P < .001). Of note, there was no significant difference in 30-day mortality between the 2 groups (P = .167).
Univariate Analysis of 30-Day Perioperative Mortality and Complications in the Non-Morbidly Obese and Morbidly Obese Groups.
Multivariate Regression Analysis
The 5 most common perioperative complications in the morbidly obese group—from most common to least common—were prolonged hospitalization (26.7%), intra- or postoperative blood transfusion (16.7%), unplanned readmission (6.5%), wound complications (5.6%), and reoperation (5.2%). Together, these 5 complications comprised 60.7% of all perioperative complications in the morbidly obese group. MVR analysis was independently performed on each of these 5 complications (Table 3).
Multivariate Regression Analysis to Identify Independent Risk Factors of the 5 Most Common Perioperative Complications in the Morbidly Obese Group.
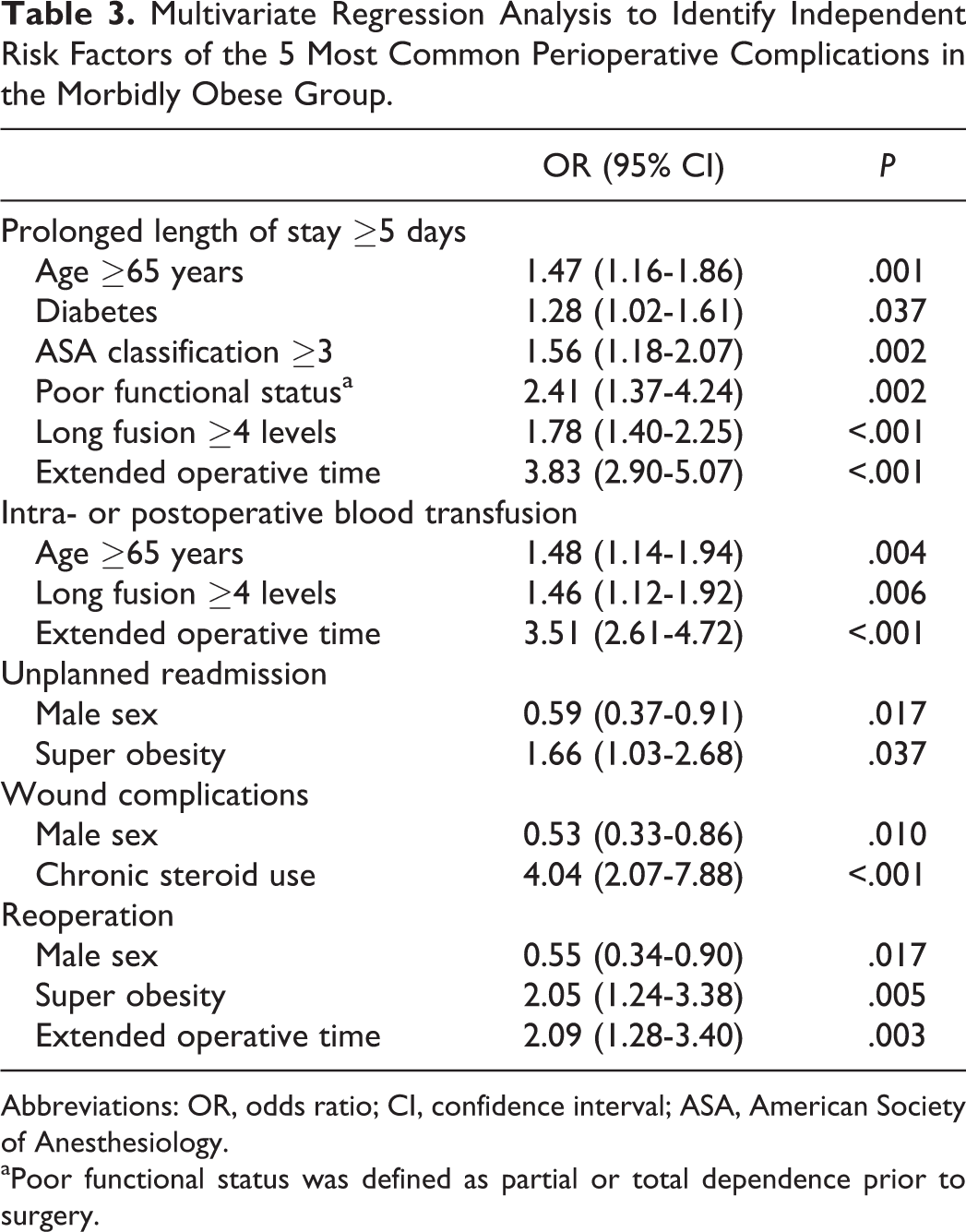
Abbreviations: OR, odds ratio; CI, confidence interval; ASA, American Society of Anesthesiology.
aPoor functional status was defined as partial or total dependence prior to surgery.
Independent risk factors for prolonged LOS in the morbidly obese group were age ≥65 years (OR = 1.47; 95% CI = 1.16-1.86; P = .001), ASA classification ≥3 (OR = 1.56; 95% CI = 1.18-2.07; P = .002), partially or totally dependent functional status (OR = 2.41; 95% CI = 1.37-4.24; P = .002), and long length of fusion (OR = 1.78; 95% CI = 1.40-2.25; P < .001). Diabetes was suggestive of an increased risk of prolonged LOS, but the association did not reach statistical significance after application of the Bonferroni correction (OR = 1.28; 95% CI = 1.02-1.61; P = .037).
An increased risk of intra- and postoperative blood transfusion in the morbidly obese group was associated with age ≥65 years (OR = 1.48; 95% CI = 1.14-1.94; P = .004), long length of fusion (OR = 1.46; 95% CI = 1.12-1.92; P = .006), and extended operative time (OR = 3.51; 95% CI = 2.61-4.72; P < .001).
Super obesity was suggestive of an increased risk of unplanned readmission in the morbidly obese group, but the association did not reach statistical significance after application of the Bonferroni correction (OR = 1.66; 95% CI = 1.03-2.68; P = .037). Male gender was suggestive of a decreased risk of unplanned readmission, but the association also did not reach statistical significance (OR = 0.59; 95% CI = 0.37-0.91; P = .017).
For operative site complications, steroid use for a chronic condition within 30 days prior to surgery was an independent risk factor in morbidly obese patients (OR = 4.04; 95% CI = 2.07-7.88; P < .001). Male gender was associated with a decreased risk of operative site complications (OR = 0.53; 95% CI = 0.33-0.86; P = .010).
Independent risk factors for reoperation in the morbidly obese group were super obesity (OR = 2.05; 95% CI = 1.24-3.38; P = .005) and extended operative time (OR = 2.09; 95% CI = 1.28-3.40; P = .003). Male gender was suggestive of a decreased risk of reoperation in morbidly obese patients, but the association did not reach statistical significance after applying the Bonferroni correction (OR = 0.55; 95% CI = 0.34-0.90; P = .017).
Discussion
Existing literature from a plethora of national and multi-institutional studies has demonstrated strong correlations between obesity and increased rates of perioperative complications following PLF. 14,15,26,27,31,39 –43 In a recent study of 24 196 patients in the ACS-NSQIP database, Marquez-Lara et al found that obese patients with a BMI ≥25 were at increased risk of perioperative wound complications, renal complications, UTI, and sepsis following spinal surgery. 41 However, they did not specifically examine the impact of morbid obesity with a BMI ≥40 on perioperative outcomes. There remains a gap in the literature regarding additional risk factors that further predispose this already high-risk obese population to adverse events in the perioperative period. 41 –45 To our knowledge, this is the first study utilizing a national database to identify independent risk factors for perioperative complications and mortality following elective PLF in the morbidly obese patient population.
Consistent with prior studies, we found that morbidly obese patients were at higher risk of perioperative complications compared to non-morbidly obese patients. The 5 most common complications in the morbidly obese group—from most common to least common—were prolonged hospitalization, intra- and postoperative blood transfusion, unplanned readmission, surgical site complications, and reoperation. Independent risk factors for one or more of these perioperative complications were age ≥65 years, super obesity (ie, BMI >48.6), steroid use for a chronic condition within 30 days prior to surgery, ASA classification ≥3, partially or totally dependent functional status, long fusion length ≥4 levels, and extended operative time. Of these variables, super obesity and steroid use are both modifiable risk factors that can be addressed prior to elective PLF surgery in order to optimize surgical outcomes.
In our morbidly obese group, super obesity was independently associated with increased rates of reoperation and trended toward an increased risk of unplanned readmission although the association did not reach statistical significance. Despite a wealth of studies in various orthopedic subspecialties investigating the effect of morbid obesity on surgical outcomes, few studies have further subdivided this cohort of patients into a super obese group to examine the effect of morbid obesity versus super obesity on perioperative outcomes. In one such study examining outcomes after unicompartmental knee replacements, Murray et al found that a BMI ≥45 was not associated with a higher failure rate compared to a BMI 40 to 45. 46 However, the spine surgery literature is currently lacking in terms of studies examining the relationship between super obesity and surgical outcomes.
Our results suggest that patients with a BMI ≥40 are not all at equal risk of perioperative complications. Super obesity—defined in this study as a BMI greater than 1 standard deviation above the mean in the morbidly obese group—was associated with a 2 times increased risk of reoperation and over a 1.5 times increased risk of unplanned readmission following PLF compared to morbid obesity. This supports a view that morbid obesity is not a single entity but rather a spectrum encompassing a range of different BMIs that likely have different effects on surgical outcomes. Further research to better understand the differing effects of morbid and super obesity on perioperative outcomes is warranted. However, given that obesity is a modifiable risk factor, patients with either morbid or super obesity should be encouraged to lose weight prior to undergoing elective PLF in order to reduce the risk of perioperative complications.
Another modifiable risk factor for poor perioperative outcomes in morbidly obese patients was preoperative steroid use. Oral or parenteral corticosteroid use for a chronic condition within 1 month prior to surgery was independently associated with approximately 4 times increased risk of surgical site complications in morbidly obese patients. Single-institution studies have found no association between preoperative steroid use and surgical site complications. 39,47,48 However, larger multi-institutional studies have demonstrated an increased risk of surgical site infections with preoperative steroid use in posterior thoracic or lumbar spinal surgery. 26,49
Chronic steroid therapy has a known immunosuppressive effect, which may allow for bacterial overgrowth leading to increased rates of hospital-acquired infections. 50,51 Chronic or high-dose steroid therapy can also cause adrenal suppression, which can result in patients requiring stress dose steroids in the perioperative period. This may then also have an effect on perioperative outcomes following PLF. Unfortunately, the ACS-NSQIP database does not include details regarding the dosing or frequency of steroid administration, nor does it include the specific indication for each patient’s steroid therapy. Therefore, we could not compare outcomes between patients who received chronic or high-dose steroid therapy for different indications. We also could not compare patients who received stress dose steroids from those who did not. Despite these limitations, however, our findings suggest that whenever possible, spine surgeons should consult with a patient’s multidisciplinary treatment team about the feasibility of discontinuing steroids in the immediate preoperative period in order to reduce the risk of surgical site complications.
Extended operative time was an independent risk factor for 30-day reoperation, intra- or postoperative blood transfusion, and prolonged LOS. In the morbidly obese group, 14.2% (n = 265/1861) of patients had an extended operative time, of which 60% (n = 159/265) of those patients experienced at least one adverse event in the perioperative period. Our finding that extended operative time increased the risk of perioperative complications is consistent with prior studies. 52 –55 Longer operative time allows for the potential for increased intraoperative blood loss, which may contribute to the increased risk of intra- or postoperative blood transfusion. Of note, high intraoperative blood loss >500 mL in instrumented spinal fusion procedures has been shown to be associated with increased risk of surgical site infections. 56 Morbidly obese patients with extended operative time also had a greater than 3 times increased risk of prolonged hospitalization. Operative time may be seen as a proxy indicator of the extent and/or complexity of the surgical procedure. More extensive and complex procedures with longer operative times likely require longer hospitalizations for adequate pain control, stabilization of postoperative laboratory results, and physical therapy clearance.
There are several limitations to this study. First, BMI is only one measure of obesity. Mehta et al recently reported that the thickness of subcutaneous fat at the surgical site might be more predictive of postoperative surgical site complications than a patient’s overall BMI. 57 Additionally, the ACS-NSQIP data is primarily collected from academic institutions, and thus our findings may not reflect operative trends or outcomes in the community setting. The ACS-NSQIP database is further limited in that it only collects data regarding complications occurring within 30 days following surgery. Therefore, we could not assess the impact of morbid obesity on long-term outcomes. Finally, because of the large number of covariates used in the regression analysis, it is possible that our model may have been overfitted.
In conclusion, we used the ACS-NSQIP database to identify independent risk factors for perioperative complications and mortality after elective PLF in morbidly obese patients. The 5 most common complications in the morbidly obese group—from most common to least common—were prolonged hospitalization, intra- and postoperative blood transfusion, unplanned readmission, surgical site complications, and reoperation. Independent risk factors for one or more of these perioperative complications were age ≥65 years, super obesity (ie, BMI >48.6), steroid use for a chronic condition within 30 days prior to surgery, ASA classification ≥3, partially or totally dependent functional status, long fusion length ≥4 levels, and extended operative time. Of these variables, obesity and steroid use are both modifiable risk factors that can be addressed prior to elective PLF surgery in order to optimize surgical outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.