
Abstract
Study Design:
Retrospective propensity score matched analysis.
Objective:
To compare the incidence of any 30-day perioperative complication following primary and revision discectomy for lumbar disc herniation.
Methods:
The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) was used to identify patients undergoing primary or revision lumbar discectomy from 2005 to 2012. Propensity score matching was performed to create matched pairs of primary and revision discectomy cases for analysis. Univariate analysis was then performed to compare 30-day morbidity and mortality between propensity score–matched pairs.
Results:
We identified 4730 cases of primary discectomy performed through a minimally invasive or open approach and 649 revision discectomy cases. Baseline patient characteristics and comorbidities were compared and then propensity score–matched adjustments were made to create 649 matched pairs of primary and revision cases. On univariate analysis, there were no significant differences in 30-day perioperative outcomes between the 2 groups.
Conclusion:
While there were no significant differences in 30-day perioperative complications between patients undergoing primary lumbar discectomy and those undergoing revision lumbar discectomy, this finding should be interpreted with caution since the ACS-NSQIP database lacks functional and pain outcomes, and also does not include dural tear or durotomy as a complication. Future large-scale and long-term prospective studies including these variables are needed to better understand the outcomes and complications following primary versus revision discectomy for lumbar disc herniation.
Keywords
Introduction
Intervertebral disc herniation is a common disorder of the spine, which in some cases is managed surgically. 1 -3 Several long-term studies have demonstrated support for surgical treatment for herniated discs, most notably the Spine Patient Outcome Research (SPORT) trial 3 that demonstrated encouraging 8-year outcomes following lumbar discectomy for disc herniation. However, despite good outcomes in general, a subgroup of patients have recurrent disc herniations after discectomy and require reoperation, with rates ranging from 3% to as high as 26%. 2 -7 Up to 85% of reoperations have been attributed to recurrent disc herniation at the same level as the index procedure. 3
Reoperations in spinal surgery have been associated with higher complication rates compared to primary surgeries. Cammisa et al reported an 8.1% incidence of durotomy in revision spinal procedures compared to 3.1% in primary procedures. 8 Ahn et al retrospectively compared primary versus revision single-level minimally invasive lumbar discectomy and found that revision lumbar discectomy is associated with increased procedural time, length of hospitalization, and postoperative narcotic utilization. 9 However, they found no differences in patient-reported functional outcomes. 9 In contrast, the prospective SPORT trial found significant differences between the revision versus primary groups in terms of operative duration, blood loss, dural tear, nerve root injury, and postoperative wound hematoma. 3 As such, there remains no general consensus in the literature regarding outcomes of patients undergoing revision lumbar discectomy. 10
There have been few studies in the current literature that have focused on comparing perioperative complications of primary versus revision discectomy using a validated national multicenter database. Our aim was to examine if revision discectomy is associated with higher 30-day perioperative complication rates than primary discectomy using the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database. We also aimed to identify patient characteristics and comorbidities that are risk factors for these perioperative complications. We hypothesized that 30-day perioperative complication rates would be higher after revision discectomy than primary discectomy.
Materials and Methods
Patient Selection and Data Collection
The ACS-NSQIP database was originally created as a quality improvement initiative for the Veteran’s Administration (VA) health system in 1994. It has since expanded to the private sector after its initial success in the VA system. 11,12 Details of the ACS-NSQIP database have been described earlier, and its use has been well established in the surgical literature. It is a validated outcomes registry that allows assessment of 30-day risk-adjusted surgical morbidity and mortality in order to provide feedback to participating hospitals. 13 Data is collected and validated for accuracy at each site by trained surgical clinical nurse coordinators. An interrater disagreement rate between the clinical abstractors >5% is investigated by the ACS-NSQIP team. 13 Random patient sampling is done in a standardized manner at all participating institutions.
The ACS-NSQIP participant files for the period 2005 through 2012 were used to identify patients undergoing posterior lumbar procedures. The data was obtained in compliance with the ACS-NSQIP data use agreement. The inclusion criteria were based on the Current Procedural Terminology (CPT) codes for primary discectomy (63 030) or revision discectomy (63 042) in adults with herniated nucleus pulposus (ICD-9: 722.10). Exclusion criteria included transpedicular approaches (CPT 63 056), nonelective procedures, pregnancy, ventilator dependence, underweight (body mass index [BMI] < 18.5 kg/m2), preoperative systemic sepsis, emergency operations, length of stay (LOS) >365 days, acute renal failure, central nervous system (CNS) tumor, disseminated cancer, chemotherapy for malignancy within 30 days before operation, and radiotherapy for malignancy within 90 days before operation.
Explanatory and Control Variables
Over 136 variables are collected at each participating site, including demographic characteristics, preoperative risk factors, intraoperative variables, and 30-day perioperative complications. 14 Recorded patient characteristics were classified into the following groups: baseline demographics, preoperative medical comorbidities, and operative variables. Patient demographics included age, gender, race (white, black, Hispanic, other), BMI class, American Society of Anesthesiologists class, diabetes, smoking (current smoker within 1 year of surgery), alcohol use, dyspnea (at rest, moderate exertion, or none), and functional dependence prior to surgery. “Other” race included American Indian, Alaska Native, Asian, Native Hawaiian, Pacific Islander. BMI was categorized according to the World Health Organization obesity classification: obese I (30.0-34.9 kg/m2), obese II (35.0-39.9 kg/m2), and obese III (≥40 kg/m2).
Medical comorbidities and operative variables included pulmonary comorbidity, cardiac comorbidity, peripheral vascular disease, neuromuscular injury, stroke, steroid use, recent weight loss, bleeding disorder, and operative time ≥4 hours. These medical comorbidities and operative variables were all treated as dichotomous variables. Cardiac comorbidity was defined as a history of congestive heart failure (within 30 days before surgery), myocardial infarction (within 6 months before surgery), percutaneous coronary intervention, cardiac surgery, angina (within 1 month before surgery), or use of hypertensive medication. Pulmonary comorbidity was defined as history of severe chronic obstructive pulmonary disease or current pneumonia. Peripheral vascular disease was defined as a history of revascularization or amputation for peripheral vascular conditions and rest pain. Chronic steroid use (regular use within 30 days before surgery) was also assessed.
Outcomes
The primary outcome variable was any postoperative complication within 30 days of surgery. These complications included mortality, wound complication (superficial wound infection, deep incisional surgical site infection, organ space surgical site infection, or wound dehiscence), pulmonary complication (pneumonia, intubation, or ventilator requirement), renal complication (progressive renal insufficiency or acute renal failure), CNS complication (stroke or coma), cardiac complication (cardiac arrest or myocardial infarction), pulmonary embolism, deep vein thrombosis, sepsis or septic shock, peripheral nerve injury, urinary tract infection, intraoperative or postoperative blood transfusion, reoperation for any reason, reoperation related to the index procedure, unplanned readmission (data only available from 2011 to 2012), and prolonged LOS ≥5 days.
Propensity Score Matching
Propensity score matching allowed us to reduce the risk of selection bias within our patient cohort. Propensity scores were assigned to patients in each cohort based on all preoperative factors including patient demographics and comorbidities. The process of matching was 1:1, with one patient from the primary surgery cohort being matched with a patient in the revision surgery cohort with the closest propensity score. Propensity score matching has been well-described in the literature. 15 -19 Matching was performed using R Software (Vienna, Austria; http://www.R-project.org/) package “MatchIt.” 20
Statistical Analysis
In the univariate analysis, categorical variables were assessed using Pearson’s χ2 or Fisher’s exact test where appropriate. Continuous variables were examined using a 1-way analysis of variance (ANOVA) test. For outcome variables that were significantly different between the primary and revision cohorts, a multivariate stepwise logistic regressions with propensity score adjustments would be performed to determine if revision surgery was an independent risk factor for perioperative complications compared to primary surgery after controlling for baseline differences between the 2 groups. A P value <.05 was considered significant. SAS software (Version 9.3, SAS Institute Inc, Cary, NC) was used for all statistical analyses.
Results
We identified 4730 cases of primary discectomy performed through a minimally invasive or open approach. We also identified 649 cases of revision discectomy. In the primary discectomy group, the median operative time was 77 minutes (standard deviation [SD], 49 minutes; interquartile range [IQR], 56-105 minutes). In the revision discectomy group, the median operative time was 101 minutes (SD, 74 minutes; IQR, 68-137 minutes).
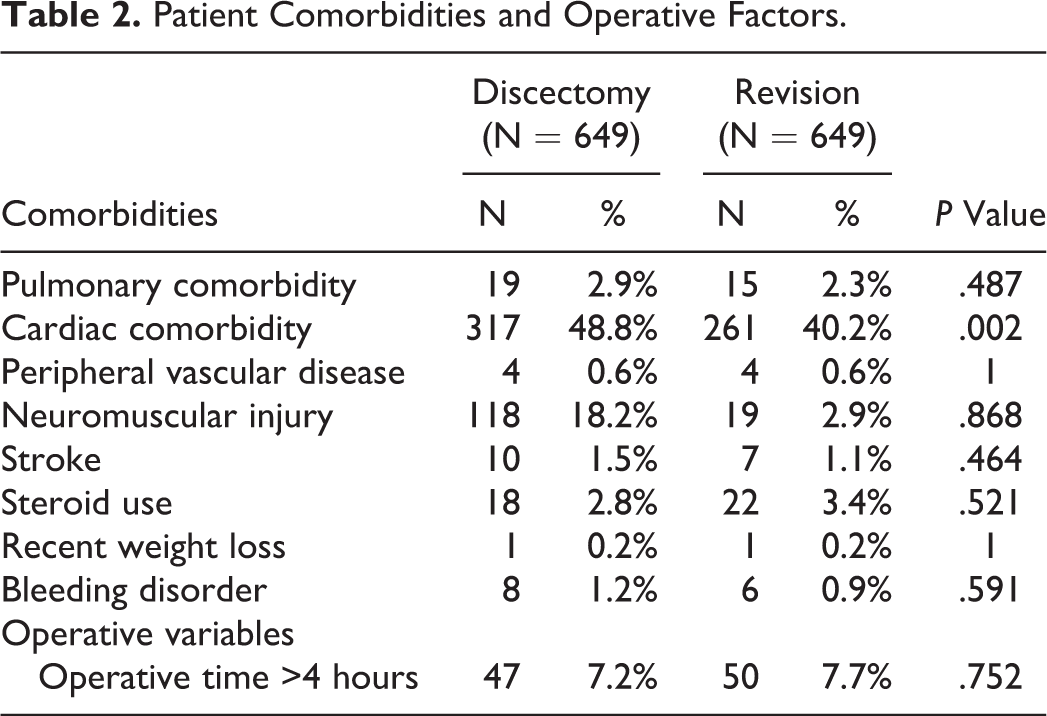
Propensity score–matched adjustments were used to create 649 matched pairs of primary and revision cases. After performing propensity score–matched adjustments, there remained significant differences between the 2 groups (Table 1). The revision discectomy group had significantly more females (32.5% vs 40.2%, P = .004), more outpatient procedures (20.2% vs 30.7%, P < .0001), and a lower proportion of patients with American Society of Anesthesiologists class ≥3 (35.6% vs 29.0%, P = .011). In terms of baseline medical comorbidities and operative variables, the only significant difference was a higher proportion of cardiac comorbidity in the primary discectomy group (48.8% vs 40.2%, P = .002). There were no significant differences between the 2 groups in terms of pulmonary comorbidity, peripheral vascular disease, neuromuscular injury, stroke, steroid use, recent weight loss, or bleeding disorder (Table 2).
Baseline Patient Demographics and Clinical Characteristics.
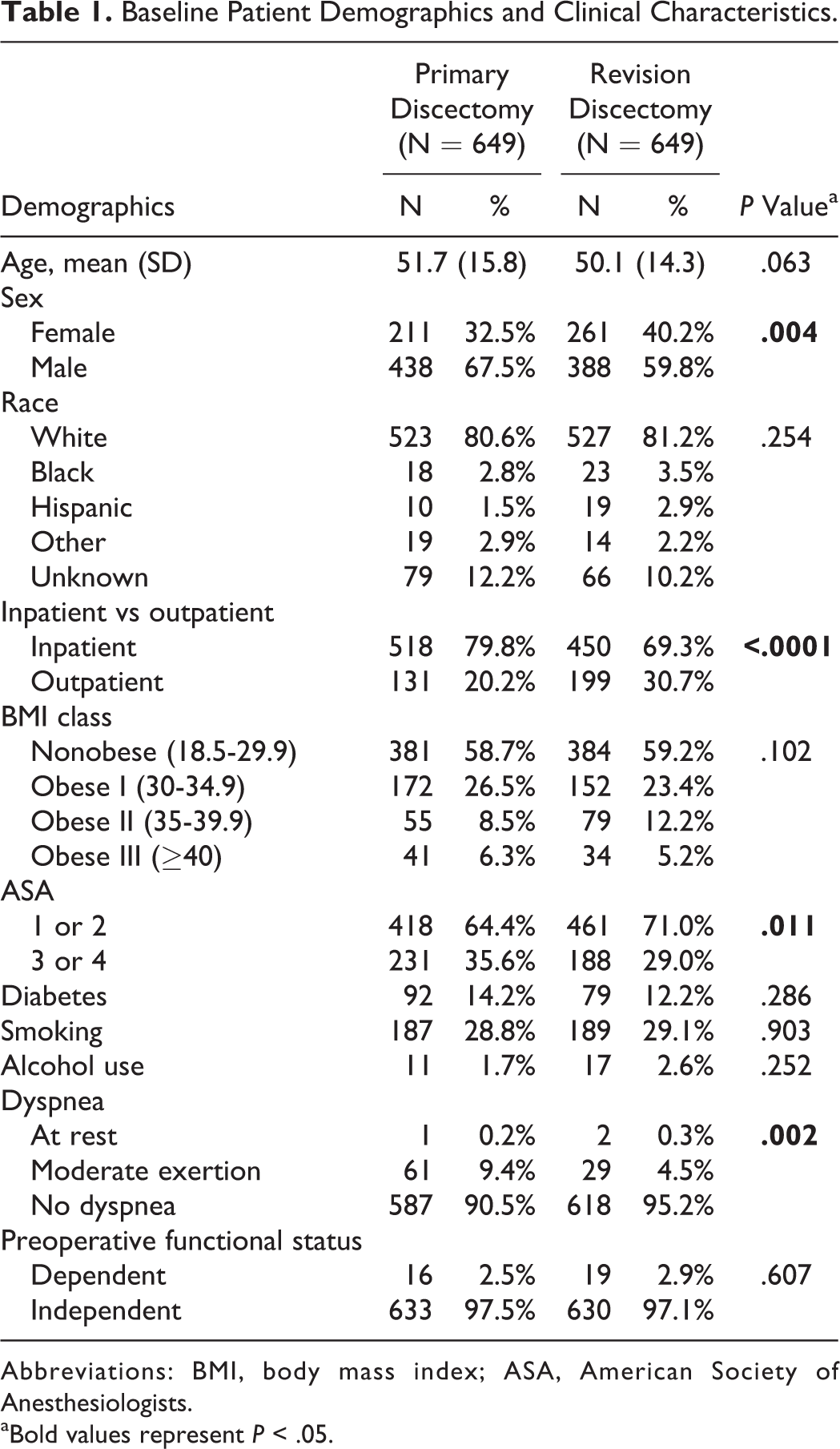
Abbreviations: BMI, body mass index; ASA, American Society of Anesthesiologists.
aBold values represent P < .05.
Patient Comorbidities and Operative Factors.
In our univariate analysis, there were no significant differences in 30-day perioperative complications between the propensity score–matched groups (Table 3). Of note, there were no deaths, cardiac complications, renal complications, CNS complications, or urinary tract infections in either the primary or revision surgery group. Additionally, there were no pulmonary complications in the revision surgery group. We did not perform a multivariate analysis since there were no significant differences in perioperative complications between the 2 groups in the univariate analysis.
Thirty-Day Perioperative Complications.
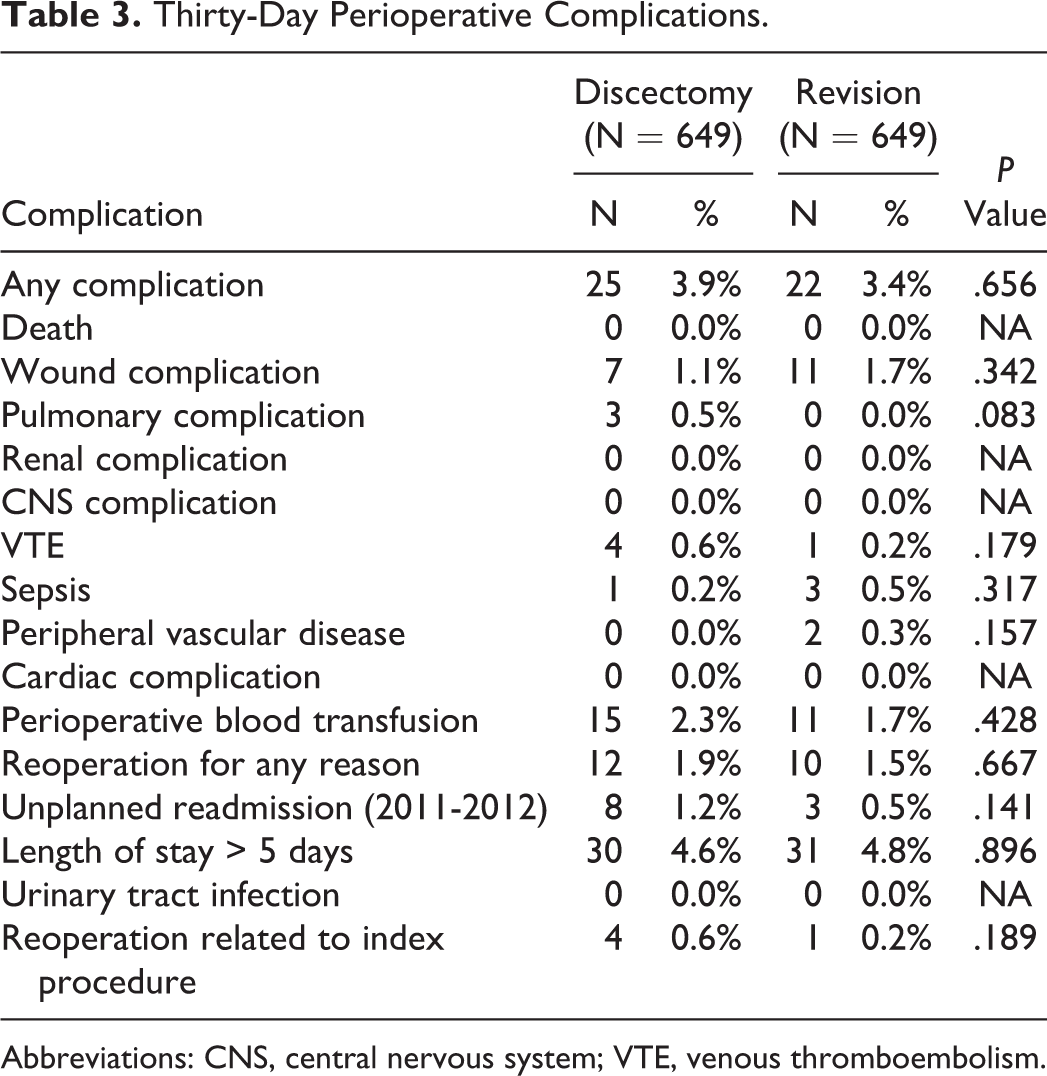
Abbreviations: CNS, central nervous system; VTE, venous thromboembolism.
Discussion
Intervertebral disc herniation is one of the most common reasons for lumbar spinal surgery, with discectomy being the mainstay of treatment. 21,22 However, reoperation rates after discectomy have ranged widely in the literature, which may be attributed to variations in surgical approach and technique, definitions of disc herniation recurrence, disease progression, or duration of follow-up. 23 -27 While few studies have directly compared primary and revision discectomy for lumbar disc herniation, studies of other spinal surgical procedures suggest that complication rates are significantly higher after revision surgery compared to the index procedure. 28
In this study, we utilized the ACS-NSQIP database to examine 5379 patients who underwent discectomy. The proportion of revision cases in this cohort was 12.1%, which is consistent with the revision discectomy rate of 13% reported by the SPORT trial. 3 Following propensity score–matched analysis, there were no significant differences in 30-day perioperative complications between the 649 matched pairs of primary and revision cases. This suggests that revision discectomy does not have a higher risk of short-term postoperative complications compared to primary discectomy.
This finding is in contrast to prior studies that have found over a 2 times increased rate of complications after revision surgery. 29 -31 This increased complication rate has been primarily attributed to the incidence of durotomy. For example, Morgan-Hough et al found a 14.3% incidence of durotomy after revision surgery compared to 5.5% after primary surgery. 29 Unfortunately, one of the main limitations of our study is that the ACS-NSQIP database does not collect data about the incidence of durotomy, and therefore, we could not assess whether there was a higher risk of durotomy after revision discectomy.
In past studies, complications other than durotomy that have also been associated with revision discectomy. Leven et al conducted a subgroup analysis of the SPORT trial in which they compared 691 patients who underwent primary discectomy without reoperation with 110 patients who underwent reoperation for recurrent lumbar disc herniation. 10 They found that the reoperation group had a significantly higher overall complication rate, as well longer LOS and a higher incidence of wound infections. 10 However, they found no significant differences in operative duration, blood loss, dural tears, nerve root injuries, or postoperative wound hematomas between the 2 groups. 10
Another study on outcomes following minimally invasive single-level discectomy by Ahn et al found comparable visual analogue scale scores between primary and revision discectomies at 6-month follow-up with no significant difference in 12-week postoperative complications. 9 Furthermore, there were no in-hospital complications and no 6-week postoperative complications reported in either group. 9 In contrast, our study of a large nationwide database—which included 649 revision cases—demonstrated that the rate of any 30-day complication was 3.9% and 3.4% following primary and revision discectomy, respectively. It is important to note, however, that Ahn et al’s study was a small study with only 41 revision cases. 9 Given that the complication rate associated with discectomies is fairly low, their small sample size may not have been adequately powered to capture the short-term occurrence of these infrequent complications.
Prolonged operative time ≥4 hours occurred significantly more often in the revision discectomy group compared to the primary discectomy group. This is consistent with our expectation that revision surgery is more complex and more technically challenging than primary surgery. One of the limitations of the ACS-NSQIP database is that it does not provide information regarding whether a revision discectomy was performed by the same surgeon as the primary discectomy or by a different surgeon. Therefore, this introduces bias into our data set, as we were unable to determine or control for differences in surgeons’ operative skills or surgical techniques within matched pairs.
Another limitation of the ACS-NSQIP database is the lack of information regarding the indication for revision discectomy. One of the known surgical indications for revision discectomy is recurrent disc herniation, and several risk factors have been proposed. These risk factors include young age, male sex, smoking, and prior trauma. 4,6,32,33 However, other studies suggest that recurrent disc herniation is more likely to occur in older patients with degenerative disc disease, as well as in patients with asymmetric motor weakness. 34,35 Therefore, there remains a lack of a general consensus in the literature regarding the risk factors that predispose toward recurrent disc herniation. In this study, patients in the revision discectomy group were more likely to have a cardiac comorbidity, but the clinical significance of this association in terms of identifying patients who are at risk for revision surgery is unclear.
In addition to the limitations discussed above, this study is also subject to potential selection bias due to the retrospective nature of our data set. We were also unable to examine longer term outcomes beyond 30 days following surgery. Notably, we were unable to assess the incidence of longer term instability and need for spinal fusion following primary or revision discectomy. Another major limitation is the lack of functional or pain outcome scores in the ACS-NSQIP database, which prevented us from examining patient satisfaction as a measure of whether the primary or revision discectomy was successful. Another potential limitation is that the ACS-NSQIP database does not differentiate between different types of disc herniations, that is, constrained, extruded, or sequestrated. Whether surgical outcomes and complications vary depending on the type of disc herniation requires further study. Last, the ACS-NSQIP database does not provide sufficient information to determine whether the revision surgery was performed on the same spinal level as the original surgery. With these limitations in mind, our finding that there is no significant difference in 30-day perioperative complications between primary and revision discectomy should be interpreted with caution, in particular as it does not include functional or pain outcomes, as well as dural tear or durotomy as a complication.
Conclusion
In this large retrospective cohort study of 649 propensity score–matched pairs of primary and revision discectomies, we found no significant difference in 30-day perioperative complications that are recorded in the ACS-NSQIP database. However, this finding should be interpreted with caution, as our data set did not include functional or pain outcomes. Additionally, dural tear or durotomy was not included as a complication, and this has been shown in past studies to be a major contributing factor to overall complication rates following discectomies. Future large-scale and long-term prospective studies including these variables are needed to better understand the outcomes and complications following primary versus revision discectomy for lumbar disc herniation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.