
Abstract
Study Design:
Retrospective cohort study.
Objective:
To investigate radiological differences in lumbar disc herniations (herniated nucleus pulposus [HNP]) between patients receiving microscopic lumbar discectomy (MLD) and nonoperative patients.
Methods:
Patients with primary treatment for an HNP at a single academic institution between November 2012 to March 2017 were divided into MLD and nonoperative treatment groups. Using magnetic resonance imaging (MRI), axial HNP area; axial canal area; HNP canal compromise; HNP cephalad/caudal migration and HNP MRI signal (black, gray, or mixed) were measured. T test and chi-square analyses compared differences in the groups, binary logistic regression analysis determined odds ratios (ORs), and decision tree analysis compared the cutoff values for risk factors.
Results:
A total of 285 patients (78 MLD, 207 nonoperative) were included. Risk factors for MLD treatment included larger axial HNP area (P < .01, OR = 1.01), caudal migration, and migration magnitude (P < .05, OR = 1.90; P < .01, OR = 1.14), and gray HNP MRI signal (P < .01, OR = 5.42). Cutoff values for risks included axial HNP area (70.52 mm2, OR = 2.66, P < .01), HNP canal compromise (20.0%, OR = 3.29, P < .01), and cephalad/caudal migration (6.8 mm, OR = 2.43, P < .01). MLD risk for those with gray HNP MRI signal (67.6% alone) increased when combined with axial HNP area >70.52 mm2 (75.5%, P = .01) and HNP canal compromise >20.0% (71.1%, P = .05) cutoffs. MLD risk in patients with cephalad/caudal migration >6.8 mm (40.5% alone) increased when combined with axial HNP area and HNP canal compromise (52.4%, 50%; P < .01).
Conclusion:
Patients who underwent MLD treatment had significantly different axial HNP area, frequency of caudal migration, magnitude of cephalad/caudal migration, and disc herniation MRI signal compared to patients with nonoperative treatment.
Introduction
Lumbar disc herniation (herniated nucleus pulposus [HNP]), or an extrusion of the nucleus pulposus intruding into the lumbar spinal canal, has been proposed as the most frequent cause of lower back pain. 1 Herniation magnitude can vary from small protrusion to complete annular tear and disc sequestration. 2 Herniations can cause spinal stenosis and nerve root compression, producing a variety of symptoms such as sciatica, radiculopathy, and lower extremity pain. 3 With symptom presentation, magnetic resonance imaging (MRI) can be used to help physicians confirm the diagnosis and to classify disc morphology. 4,5
Physicians can implement operative or nonoperative treatment for HNPs. There is mounting evidence that surgical treatment, specifically microscopic lumbar discectomy (MLD), is a cost-effective method of providing rapid relief, improved quality of life, and lower reherniation rates, especially in patients with severe symptoms. 6 -9 On the contrary, conservative nonoperative treatment is a noninvasive, low-risk option. 10 -13 In reality, in the era of shared decision making, patient decision to undergo MLD depends on severity and duration of symptoms, presence of neurologic compromise, and psychologic and socioeconomic factors. Although both modes of treatment yield positive outcomes, it is of utmost importance for physicians to provide the correct and optimal care for their patients.
Because of the complex association between disc morphology and symptom onset, there is ambiguity regarding which baseline factors indicate high likelihood for surgical treatment. 14 Prior studies have reported that clinical and symptomatic variables do not have strong predictability for MLD treatment success. Radiographic parameters pertaining to disc morphology, however, can more accurately predict success of surgical treatment. 15,16 Therefore, our study aimed to comprehensively analyze radiographic disc morphology parameters, and then identify predictors of requiring microlumbar discectomy.
Methods
Study Design
This study was an institutional review board–approved retrospective review of consecutive patients presenting to a single academic center from November 2012 to March 2017.
Patient Population
Inclusion criteria consisted of patients included presentation with symptoms, examination and imaging consistent with primary lumbar disc herniation (HNP). Patients were classified into either operative (MLD) or nonoperative treatment groups. Indication for surgery was based on shared decision making between surgeon and patient, based on the presence and duration of symptoms, having failed conservative treatment for more than 6 weeks, or in the presence of progressive neurological decline. Unless there was evidence of progressive neurological decline, patients in the operative group experienced an average of 413.0 ± 307.1 days of conservative treatment before undergoing MLD treatment. Operations were performed as outpatient surgeries after patients had been seen in the surgeon’s office/clinic. Patients were excluded if they received prior MLD or underwent surgical treatment other than MLD for their presentation, which would indicate a secondary diagnosis such as degenerative lumbar stenosis or instability.
Data Collection and Radiographic Analysis
Collected demographic data included age, gender, and body mass index (BMI). For patients receiving MLD treatment, date of surgery and level of operation were recorded. Radiographic analysis was performed on T2-weighted MRI images accessed via PACS (picture archiving and communication system) imaging software. The Carragee et al 17 study on MRI analysis in patients with lumbar disc herniation was used as a model for disc and canal measurement techniques. Using axial imaging, vertical and horizontal diameters of the herniation and the entire spinal canal were measured to calculate dimensions and area of the herniation and the spinal canal (Figure 1). A ratio of the axial vertical diameters (HNP canal compromise) was calculated to derive the magnitude to which the herniation intruded into the canal. Sagittal imaging was used to measure cephalad and caudal migration of the herniation, with the superior and inferior endplates as the starting point for each measure, respectively (Figure 2). Disc hydration was classified into either black, gray, or mixed (black and gray) color categories.
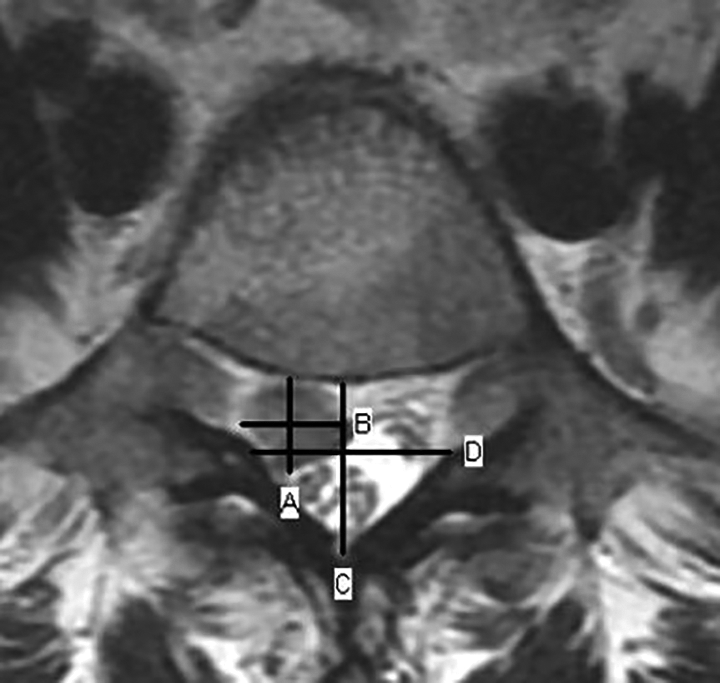
Axial diameter measurements of the herniation (vertical = A, horizontal = B) and the spinal canal (vertical = C, horizontal = D).

Sagittal canal migration in the cephalad or caudal direction. Cephalad herniations (line E) were measured using the inferior endplate of the upper vertebra as the starting point. Caudal herniations were measured using the superior endplate of lower vertebra as the starting point (line F).
Statistical Analysis
Statistical analysis was performed using R version 3.3 (The R Foundation for Statistical Computing, Vienna, Austria) and IBM SPSS version 23.0 (IBM Corp, Armonk, NY, USA) were utilized for preprocessing and analysis of the data. After classifying patients into MLD and nonoperative (non-MLD) groups, univariate analyses of primary demographic and radiographic variables were computed using independent t tests and chi-square tests, with means being compared with a significance threshold of P < .05. Odds ratios (ORs) analysis determined to what extent radiographic characteristics could significantly increase susceptibility of requiring MLD treatment. ORs were calculated for radiographic variables, with reporting of significance and confidence intervals for each variable. Random forest analysis utilized a set of 2000 conditional inference trees (subsampling without replacement) to determine ORs for each radiographic measurement with corresponding cutoff thresholds. Variables were then compounded in the decision tree to quantify the extent to which combined determinants increased susceptibility of MLD treatment.
Results
Demographic Assessment
Within our patient cohort, 285 patients receiving treatment from 1 of 16 included surgeons were classified into MLD (78) and non-MLD (207) groups. Patients in the MLD group had a mean age of 48.54 years and mean BMI of 26.91 kg/m2. In the MLD group, 46.2% of patients were male, and 53.8% of patients were female. Patients in the non-MLD group had a mean age of 49.41 and mean BMI of 27.65. In the non-MLD group, 51.7% of patients were male, and 48.3% of patients were female. There was no significant difference in demographic variables between the 2 groups (P > 0.05) (Table 1).
Demographic and Baseline Radiographic Characteristics.
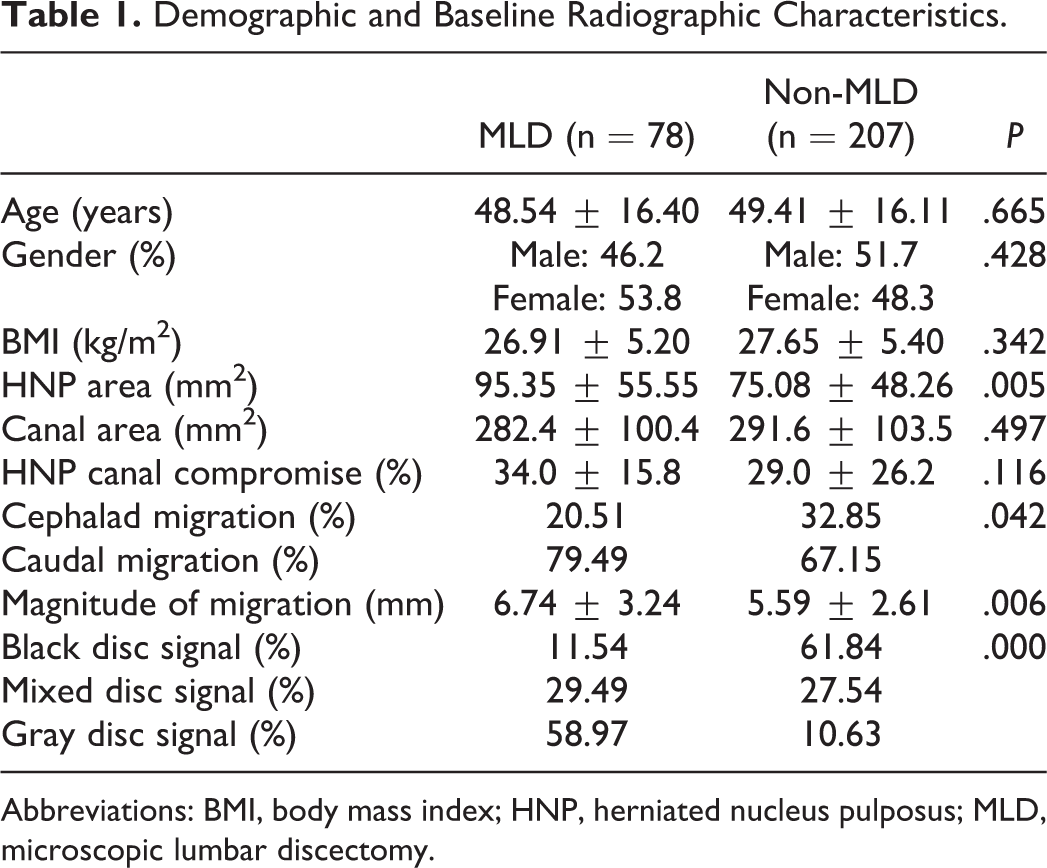
Abbreviations: BMI, body mass index; HNP, herniated nucleus pulposus; MLD, microscopic lumbar discectomy.
Primary Radiographic Analysis
Patients receiving MLD had a significantly larger axial HNP area (95.35 ± 55.55 vs 75.08 ± 48.26 mm2, P < .01). MLD patients’ HNPs were more likely to migrate caudally in the spinal canal (79.49% vs 20.51%, P = .042), and had a larger canal migration magnitude (6.74 ± 3.24 vs 5.59 ± 2.61 mm, P < .01) compared with non-MLD patients. Between the 2 groups, MLD patients had significantly higher frequency of a gray MRI disc signal (58.97% vs 10.63%) and lower frequency of black MRI disc signal (11.54% vs 61.84%) (both P < .01) (Table 1).
Decision Tree Analysis
In terms of clinical relevance, our results showed that patients with a herniated disc with caudal migration were almost twice as likely to require MLD treatment (OR = 1.90, P = .04, 95% CI 1.02-3.53). The strongest radiographic predictor of MLD treatment was MRI disc signal. Patients with a gray MRI disc signal were over 5 times more likely to undergo MLD (OR = 5.42, P < .01, 95% CI 3.58-8.20) (Table 2).
Decision Tree Analysis of Radiographic Metrics.
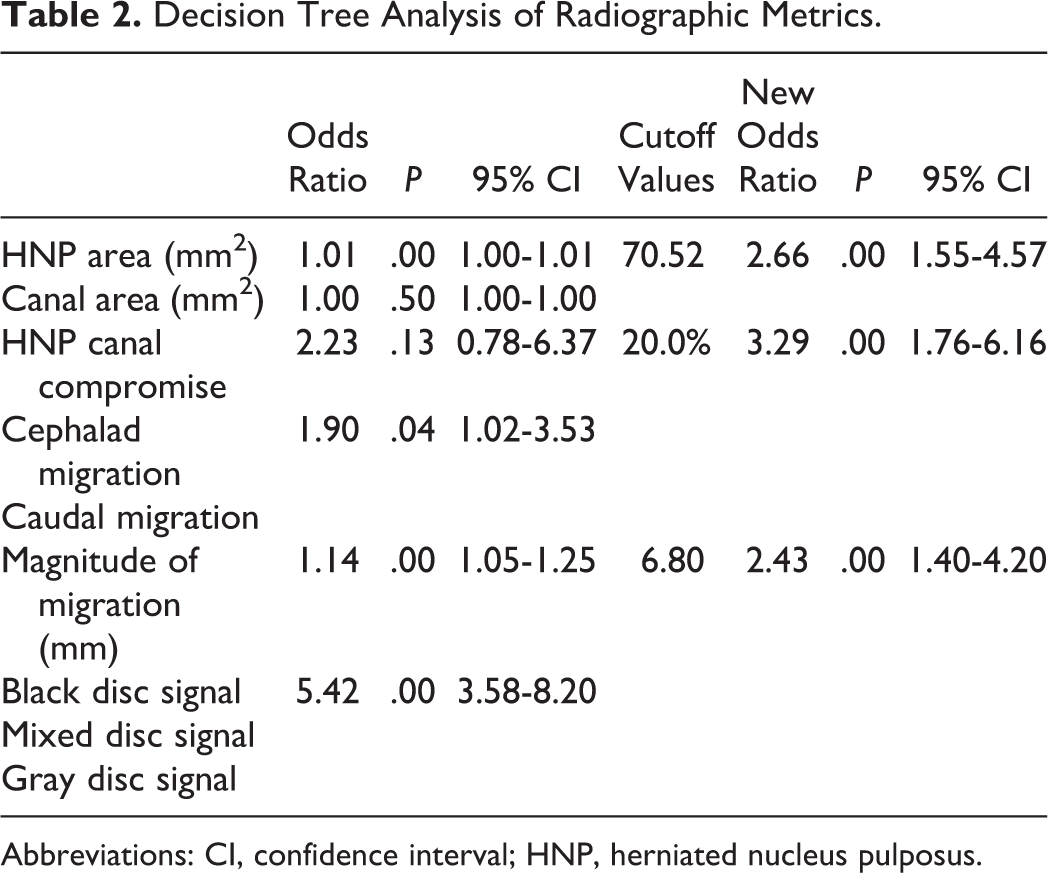
Abbreviations: CI, confidence interval; HNP, herniated nucleus pulposus.
Patients with an HNP area greater than or equal to 70.52 mm2 were over 2 times more likely to require MLD treatment (OR = 2.66, P < .01, 95% CI 1.55-4.57). Patients with an HNP canal compromise of greater than or equal to 20.0% were over 3 times more likely to require MLD treatment (OR = 3.29, P < .01, 95% CI 1.76-6.16). HNPs with a cephalad/caudal canal migration greater than or equal to 6.80 mm were over 2 times more likely to undergo MLD (OR = 2.43, P < .01, 95% CI 1.40-4.20) (Table 2).
Decision Tree Analysis With Compounded Variables
Within the group of patients with a gray MRI disc signal, 67.6% of patients received MLD treatment. However, when these patients also had an HNP area >70.52 mm2, probability of MLD rose to 75.5% (P = .01). Patients with either gray or mixed MRI disc signal had a 46.6% probability of undergoing MLD treatment, but when these patients also had an HNP canal compromise >20%, this probability rose to 51.8% (P = .02). Patients with a magnitude of cephalad/caudal canal migration greater than 6.80 mm had a 40.5% probability of receiving MLD. However, if patients also had an HNP area >70.52 mm2, probability of undergoing MLD treatment rose to 52.4% (P < .01). Similarly, if patients met the cephalad/caudal migration threshold along with having an HNP canal compromise >20%, risk of receiving MLD increased to 50.0% (P < .01) (Table 3).
Decision Tree Analysis With Compounded Variables.
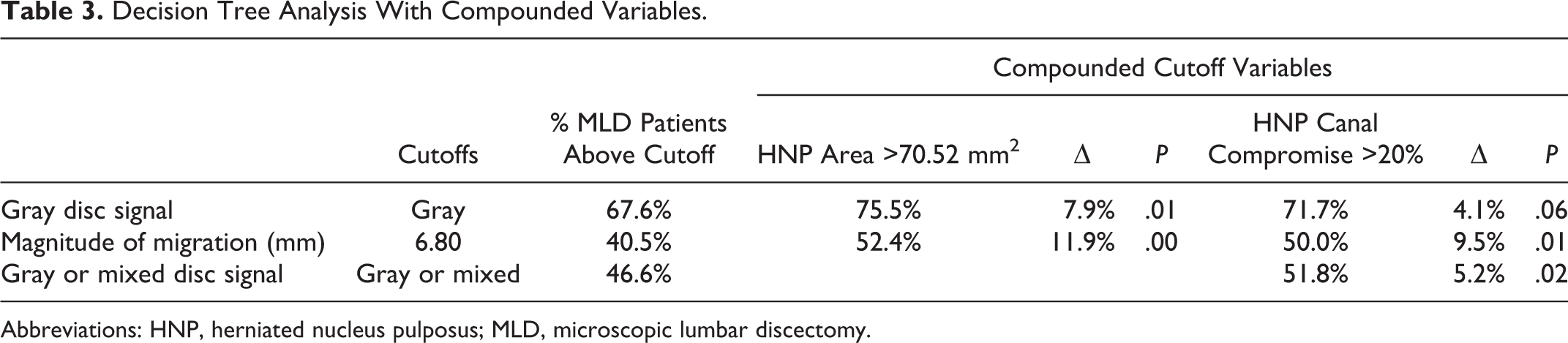
Abbreviations: HNP, herniated nucleus pulposus; MLD, microscopic lumbar discectomy.
Discussion
Recent literature has often reported ambiguity regarding predictive variables for operative and nonoperative HNP treatment. Occasionally, a patient can have a radiographically noticeable HNP that does not present any symptomatic pain or discomfort. 18 There is also other evidence noting the association between successful surgical outcomes and other clinical factors besides disc morphology. 19 Although numerous studies outline irresolute evidence behind identifying HNP predictors, the results from this study reaffirm the substantiated importance of predicting HNP treatment through radiographic analysis of disc morphology. A prospective study conducted by Carragee et al 17 analyzed MRI in 188 patients with sciatica and lumbar HNPs to test disc and canal morphology as correlated with outcomes. The study results indicated that MRI morphometric features of HNP and spinal canal were strong predictors of surgical outcomes. Specifically, larger anteroposterior disc diameter, canal area, and canal compromise all correlated with improved outcomes as a result of surgical treatment. 17 A later prospective study conducted by Carragee et al 15 investigated clinical outcomes after lumbar discectomy for sciatica to determine the effect of fragment morphology and annular competence on these outcomes. It was determined that intraoperative radiographic findings, opposed to demographic, socioeconomic, or clinical variables, were most clearly associated with outcomes. Within the 187-patient cohort, degree of annular competence after surgery and type of herniation (fragment-fissure, fragment-defect, fragment-contained, and no fragment-contained) were most predictive of surgical treatment success. 15 Pople et al 20 confirmed these findings, as surgical outcomes were significantly better in patients with extruded HNPs, with more canal compromise. All of these studies outline the significance of radiographic disc properties as a predictor for surgical success.
The results presented in the current study align with these findings, as similar morphometric HNP parameters were predictive of surgical treatment. However, the current study’s OR analysis advance previous study results. This study descriptively outlines patients’ likelihood of undergoing microdiscectomy treatment using individual and combined radiographic variables as predictors. The most substantial radiographic predictor found in this study was MRI disc signal. These results are consistent with previous studies that analyzed the success of different modes of treatment as a function of disc hydration status. The Butterman 21 study found that epidural steroid injections (nondiscectomy treatment) were effective in regressing symptoms in patients who presented low hydration HNPs. In this present study, just as high level of disc hydration correlated with high likelihood of discectomy treatment, the same was evident for HNPs with low hydration and low likelihood of MLD treatment.
Contrary to these findings, there have been numerous studies questioning the ability of radiographic disc morphology to predict necessity for operative treatment. Other studies and reviews have delved into finding other predictors, such as patient reported outcomes, physical, and psychometric variables in addition to radiographic variables. It is valid to believe that HNP treatment is multifactorial and is not solely determined by radiographic morphology, however, the results in these studies either contained very limited data, reported modest predictive value, or admitted to having ambiguous results and clinical implications. 22 -24
As with any study, this study has some limitations. First, this study was conducted at a single center using patients receiving treatment from 16 surgeons, which reduces generalizability of our findings toward other institutions with dissimilar practices. Second, since radiographic films were measured with limited imaging measuring technology, surface area measurements of the discs and canals were approximated using respective diameters of each area. However, these approximations were standardized by comparing relative sizes in a ratio calculation. Third, we only analyzed patients without coexisting stenosis, therefore the results may not be applicable to patients with preexisting stenosis and a lumbar disc herniation. Furthermore, the lack of postoperative health-related quality of life (HRQoL) outcomes does not confer success of the surgery performed, but merely confers that the patient elected to undergo MLD.
Ultimately, even though our study outlines the importance of radiological risk factors for requiring MLD treatment, presence of progressive neurological decline with a clinically relevant disc herniation, or failure of conservative treatments should still be indications for surgery regardless of size of the disc herniation. Cutoff values outlined in this study can be used as risk factors for requiring surgery and should be used in counseling patients as to the likelihood of requiring surgery but not necessarily as the primary indication.
Conclusion
Patients who underwent MLD treatment had significantly different radiographic measures of axial HNP area, frequency of caudal migration, magnitude of cephalad/caudal migration, and disc herniation MRI signal compared to patients with non-operative treatment. This suggests that a meticulous MRI analysis of HNPs could be utilized to effectively counsel patients as to the potential need for surgical methods despite nonoperative treatments.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.