
Abstract
Study Design:
Prospective cohort study.
Objectives:
To describe the rate of short-term complications following the posterior use of recombinant human bone morphogenetic protein–2 (rhBMP-2) in cervical deformity (CD) surgery.
Methods:
CD patients from 2013 to 2015 were enrolled in a prospective, multicenter database. Patients were divided into those receiving rhBMP-2 (BMP) and no rhBMP-2 (NOBMP). The relationship between BMP use, demographic variables surgical variables, radiographic parameters and complications was evaluated.
Results:
A total of 100 patients (47 BMP, 53 NOBMP) were included. Follow-up time averaged 7.6 months (range 3-12 months). An average of 13.6mg of BMP was used per person with 1.49 mg per level. Compared with the NOBMP group, patients in the BMP group were older (P = .03). BMP was more commonly used in patients that and had longer prior fusions (6.0 vs 2.5, P < .01). There were no differences between groups with regards to a history of surgery, Charlson Comorbidity Index, estimated blood loss, operation time, fusion levels, and surgical approach. The maintenance of radiographic parameters at 6-month follow-up was similar. There were no differences in terms of total complication incidence, total complications per person, major complications per person or any specific complication. Linear regression and Pearson correlation analysis did not reveal any strong r2 values (r2 = 0.09, 0.08, 0.06) between the use of BMP and complications (major or operative).
Conclusions:
BMP use was not directly associated with an increased incidence of early complications in this prospective cohort of operative adult CD patients. Its use was associated with increased number of levels instrumented and fused.
Keywords
Introduction
Recombinant human bone morphogenetic protein–2 (rhBMP-2) was first approved in 2002 for use in anterior lumbar interbody fusion (ALIF) surgery with a proprietary titanium interbody cage. 1 In subsequent years, rhBMP-2 has been used off label in all areas of the spine, including the cervical, thoracic, and lumbar spine. In 2006, it was estimated that bone morphogenetic protein (BMP) was used in 25% of all spinal fusions 2 and that 85% of this use was for off-label indications. 3 RhBMP-2 has been an attractive alternative to the traditional gold standard (autologous iliac crest bone graft [ICBG]) because it results in equivalent or slightly higher rate of radiographic fusion while avoiding donor site morbidity. 4 –6 This increase in fusion rates, however, has been accompanied by persistent concerns about the possibility of increased complications. 7,8
Specific to the cervical fusions, the use of BMP in anterior cervical fusions, in particular, has been shown to increase the risk of wound infection, dysphagia and retropharyngeal edema. 9 –12 The latter is a potentially life-threatening complication requiring emergent interventions such as intubation and surgical reexploration. 10 Recognition of this phenomenon led to a statement by the US Food and Drug Administration (FDA) recommending that practitioners avoid BMP use in the anterior cervical spine. 13
The use of BMP in the posterior cervical spine, however, has been recently examined in several retrospective studies without the airway complications reported with anterior use. 14 –18 These studies have shown rates of nonunion ranging from 0% to 10.3% with the majority showing an improvement fusion rates based on computed tomography imaging. Other authors, focusing on posterior BMP use at the cervicothoracic junction, found that the use of BMP did not result in a significantly different rate of symptomatic non-union requiring reoperation. 19
The existing literature on this topic is retrospective in nature, narrowly focused on radiographic outcomes and limited to patients with degenerative pathology. The rate of complications following BMP use in patients with cervical deformity is unknown. We chose to focus cervical deformity patients (as opposed to routine posterior cervical fusions) because the use of BMP in these patients is attractive because these patients are at high risk for pseudarthrosis. The risk of pseudarthrosis is higher in these patients because they are treated with long fusion constructs that frequently cross the cervicothoracic (and sometimes the thoracolumbar) junction. In addition, the instrumentation in this area is often thinner and smaller; this fact, combined with alignment correction can lead to higher rates of rod fractures and instrumentation failure if fusion is not achieved.
The objective of this study was to identify the short-term complications associated with BMP use in a prospective database comprised of adult cervical deformity patients. We sought to determine the impact of BMP use on short-term complications in adult cervical deformity surgery.
Methods
Subjects
This study was a retrospective review of a prospective multicenter database of cervical deformity patients. Cervical deformity was defined as one or more of the following criteria: cervical kyphosis >10°, cervical scoliosis >10°, C2-7 sagittal vertical axis (SVA) >4 cm, or horizontal gaze impairment (chin-brow vertical angle >25°). Eleven participating sites in the United States contributed patients to the data set. Patients were enrolled between January 2013 and October 2015. Institutional review board approval was obtained at all participating centers.
Patients were enrolled if the following inclusion criteria were met: age >18 years old, at least 1 posterior cervical surgery (ie, posterior only approaches or combined anterior and posterior surgery), full documentation of perioperative complications and a minimum 3 months of postoperative follow-up. Patients with cancer, infection and patients who were pregnant or planning to get pregnant during the study period were excluded from the study. Patients were divided into 2 treatment groups: those receiving rhBMP-2 (BMP) or no rhBMP-2 (NOBMP). All patients in the BMP group had BMP placed posteriorly, none of the patients in this cohort received BMP in anterior approaches.
Data Collection
Standardized data collection forms were used to collect demographic, surgical, radiographic, and complication data. Data collection forms were completed at the perioperative time point and at 3 months, 6 months, and 1 year postoperatively. Standing long-cassette radiographs were obtained preoperatively, immediately after surgery, and at 6-month follow-up. The last available time point was used for analysis of the radiographic and complication data.
Demographic data collected included age, body mass index (BMI), height, weight, gender, Charlson Comorbidities Index (CCI), and smoking history. Surgical data included the surgical approach, fusion levels, estimated blood loss (EBL), operation time, and rhBMP-2 use.
Complications were categorized as cardiopulmonary complications, dysphagia, dysphonia, electrolyte abnormalities, gastrointestinal complications, infections, instrumentation-related complications, musculoskeletal complications, neurological complications, operative complications, organ failure, radiographic complications, renal complications, vascular complications, wound complications, and other complications. Complications were also labeled major or minor based on consensus agreement of the study group surgeons. A complication that prolonged hospitalization or adversely affected the recovery of the patient was considered a major complication. A complication that was noted in the medical records but did not alter the patient’s recovery was considered a minor complication, as previously reported. 20 –22 Complications requiring revision surgery were also noted.
All spine radiographs were analyzed using validated software (SpineView; ENSAM Laboratory of Biomechanics, Paris, France) at a central location based on standard techniques. 23,24 The following postoperative cervical radiographic parameters were measured: cervical SVA (C2-C7 SVA: offset from the C2 plumb line and the posterosuperior corner of C7), C2-C7 lordosis (Cobb angle between C2 inferior endplate and C7 inferior endplate), fused cervical lordosis (Cobb angle between the fused cervical levels), unfused cervical lordosis (Cobb angle between the unfused cervical levels) and mismatch between T1 slope (TS) and C2-C7 angle (TS-CL).
Statistical Analysis
Descriptive, univariate analysis and multivariate regression were all performed using SPSS (version 22.0, IBM Corp, Armonk, NY, USA). Descriptive statistics were calculated for all study variables. Univariate analyses were used to determine the differences of variables between BMP and NOBMP groups. Regression analyses were performed to determine the risk factors for complications. The multivariate analysis included the following variables: age, gender, BMI, smoking history, previous cervical surgery history, numbers of previous cervical surgery, numbers of previous anterior cervical fusion, numbers of previous posterior cervical fusion, steroids use or not, intensive care unit stay or not, posterior BMP dose, number of posterior fusion levels, posterior BMP dose per level. P values of less than .05 were considered significant. The adjusted r2 statistic was used to assess the overall explanatory ability of the linear models.
Results
Demographic Variables
A total of 100 patients with cervical deformity were enrolled in the current study (53 BMP and 47 NOBMP). The mean age was 61.5 years. Follow-up averaged 7.6 months (3-12 months). BMP patients were significantly older (63.62 vs 59.15 years, P = .038). but had similar BMI, CCI, current smoking status, and past smoking history as NOBMP patients (Table 1).
Comparison Between BMP and NOBMP Patients Regarding Demographic, Surgical, and Radiographic Variables.a
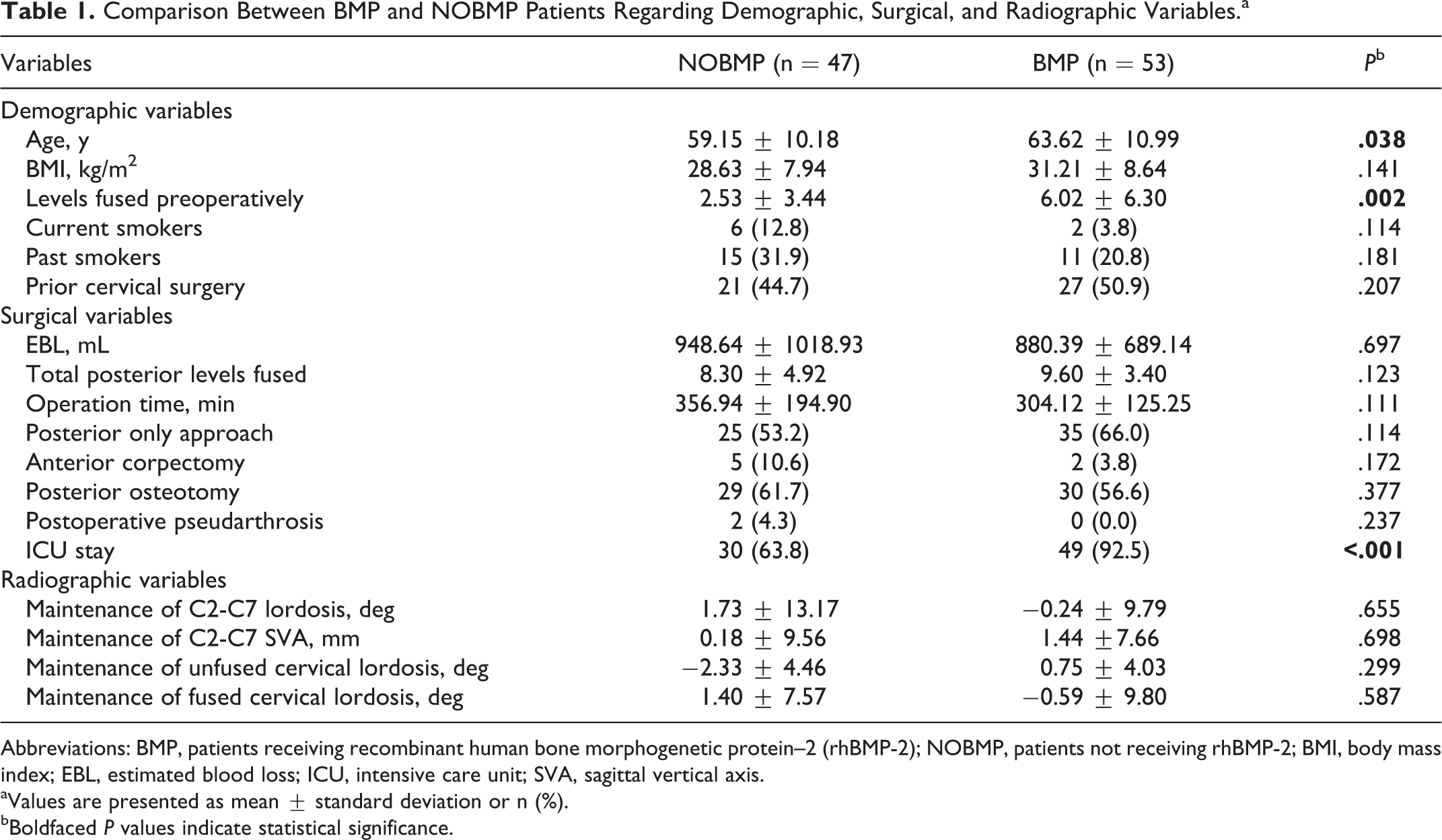
Abbreviations: BMP, patients receiving recombinant human bone morphogenetic protein–2 (rhBMP-2); NOBMP, patients not receiving rhBMP-2; BMI, body mass index; EBL, estimated blood loss; ICU, intensive care unit; SVA, sagittal vertical axis.
aValues are presented as mean ± standard deviation or n (%).
bBoldfaced P values indicate statistical significance.
Surgical Variables
The mean total rhBMP-2 dose for BMP patients was 13.58 mg (range: 1-60 mg). BMP patients had an average of 9.6 levels fused with a mean BMP dose of 1.49 mg/level (range: 0.13-8.57).
EBL, total posterior fusion levels and operative time were similar for BMP and NOBMP patients (Table 1). Surgical approaches (posterior only or combined anterior and posterior), anterior corpectomy, posterior osteotomy and postoperative pseudarthrosis were also comparable between the two groups (all P > .05, Table 1). Patients in the BMP and NOBMP cohort had undergone prior cervical surgery at similar rates. BMP was more commonly used in patients that had longer prior fusions compared to NOBMP patients (6.02 vs 2.53 levels, P = .002). In addition, BMP patients were more likely to stay in the surgical intensive care unit postoperatively (92.5% vs 63.8%, P < .001). Although the intensive care unit length of stay was recorded, the reason for this increased length (eg, prolonged intubation) was unknown.
Radiographic Variables
The maintenance of postoperative radiographic parameters at 6-month follow-up was similar in BMP and NOBMP patients, including C2-C7 SVA, C2-C7 lordosis, TS-CL, fused cervical lordosis and unfused cervical lordosis (all P > .05, Table 1).
Complications
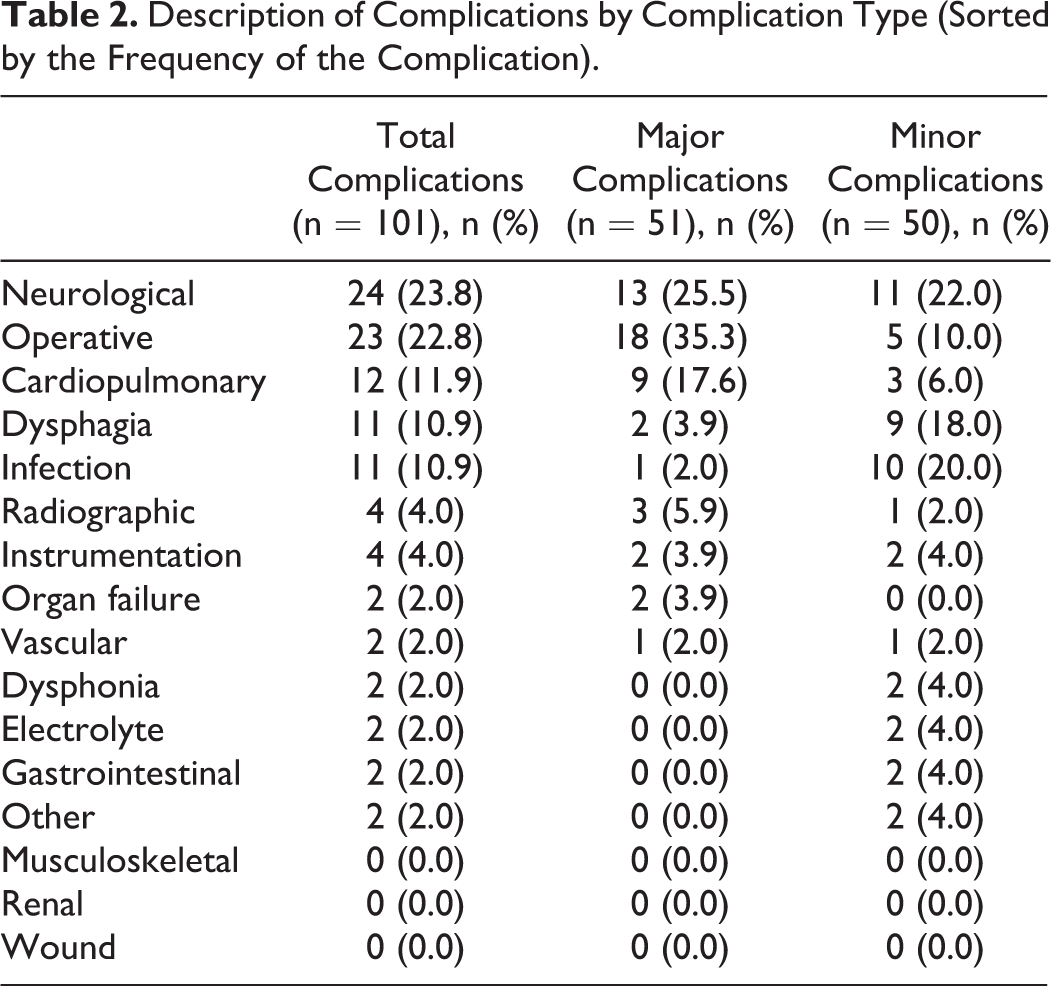
Five patients (1 BMP, 4 NOBMP) did not have any complications data recorded and were excluded from the complications analysis. Complications in the remaining 95 patients were analyzed. In these remaining 95 patients (52 BMP, 43 NOBMP) there were a total of 101 complications in 68 patients. 38 patients experienced at least 1 major complication and 30 patients had minor complications only (Table 2). 15 patients had complications requiring reoperation.
Description of Complications by Complication Type (Sorted by the Frequency of the Complication).
There were no significant differences between BMP and NOBMP patients with regard to any kind of complication incidence, including total complications, complications per patient, major complications per patient, minor complications per patient, and each specific complication (Table 3). There were also no differences between complication rates at 30 and 90 days after surgery.
Incidence of Complications in BMP and NOBMP Patients.
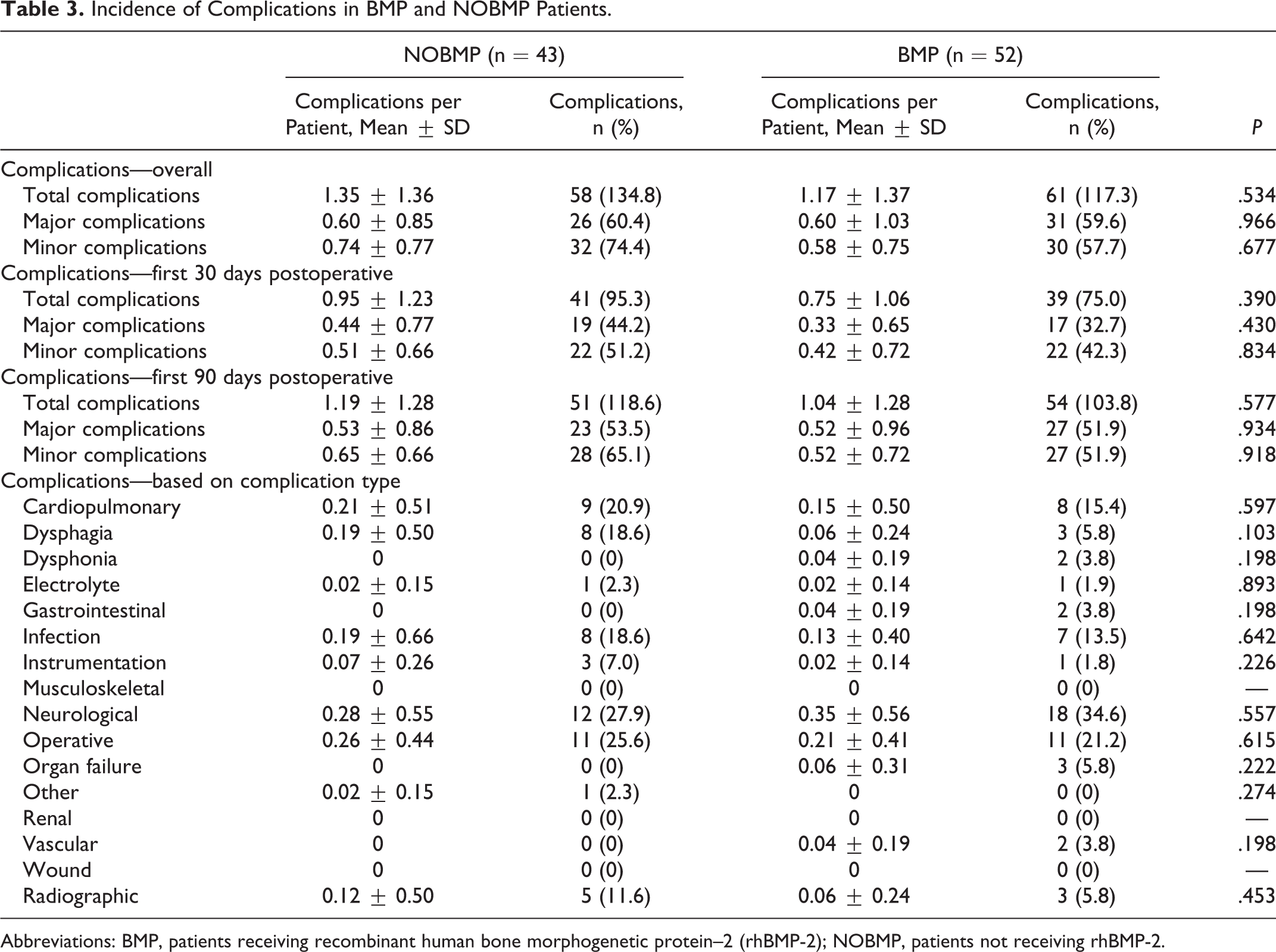
Abbreviations: BMP, patients receiving recombinant human bone morphogenetic protein–2 (rhBMP-2); NOBMP, patients not receiving rhBMP-2.
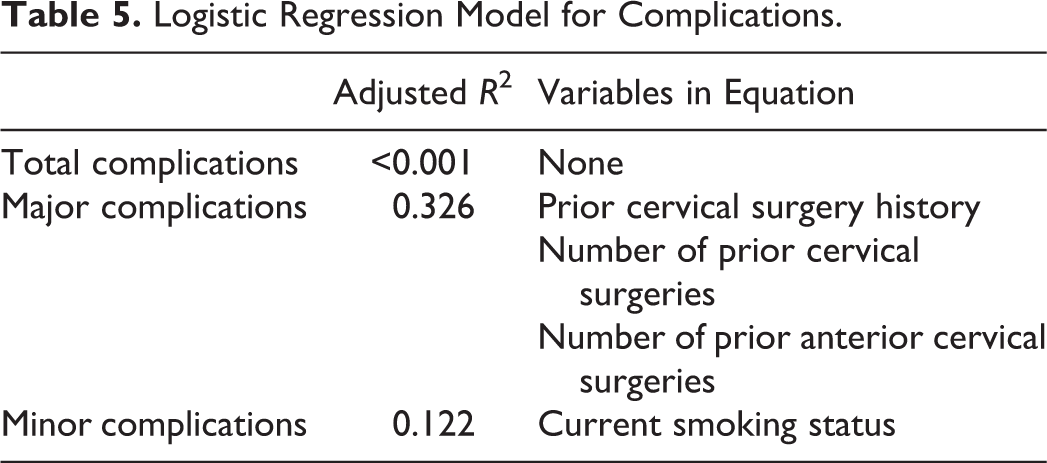
In BMP patients, a linear regression analysis revealed no relationship between rhBMP-2 dose and the number of total complications, minor complications, complications requiring re-operation, infections, neurological complications, dysphagia, dysphonia, and instrumentation related complications (Table 4). Linear regression also did not reveal any strong relationships between BMP dose and posterior fusion levels, major complications, and operative complications (r2 < 0.1 despite statistical significance, Table 4). Logistic regression also showed neither total BMP dose nor BMP dose per level could predict the total number of complications, major complications, or minor complications (Table 5). Finally, there were no differences in clinical outcomes between the BMP and NOBMP groups (Table 6).
Linear Regression Model Showing Relationship Between Total Bone Morphogenetic Protein Dose and Complications.
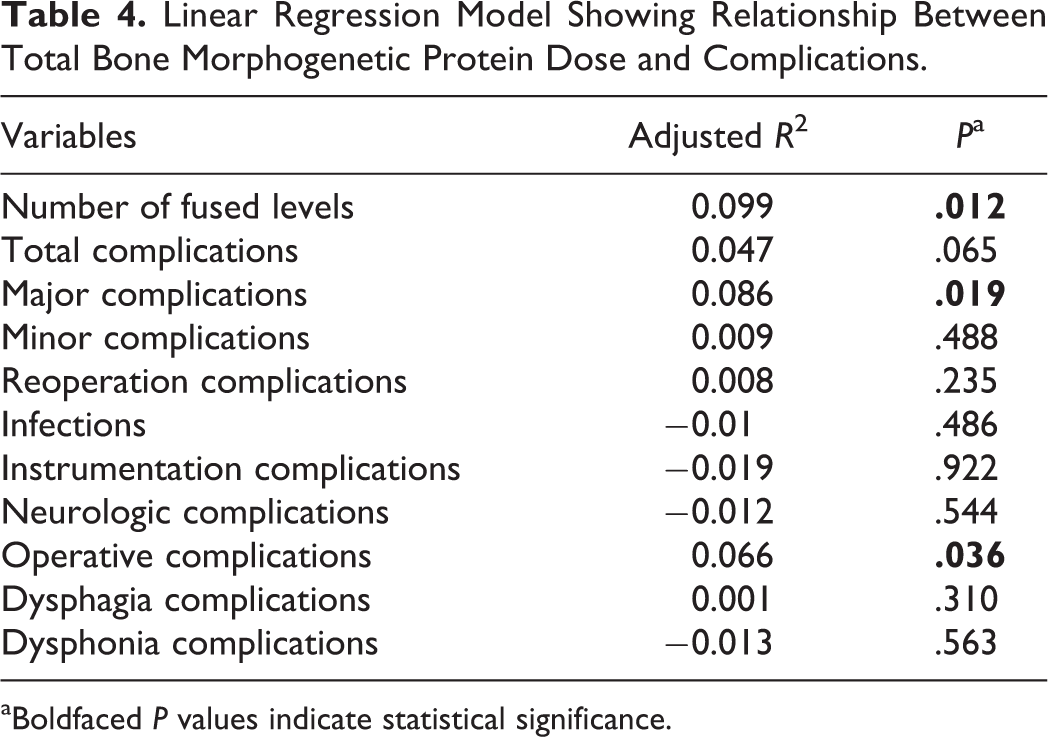
aBoldfaced P values indicate statistical significance.
Logistic Regression Model for Complications.
Health-Related Quality of Life Outcomes in Patients in the BMP and NOBMP Groups.
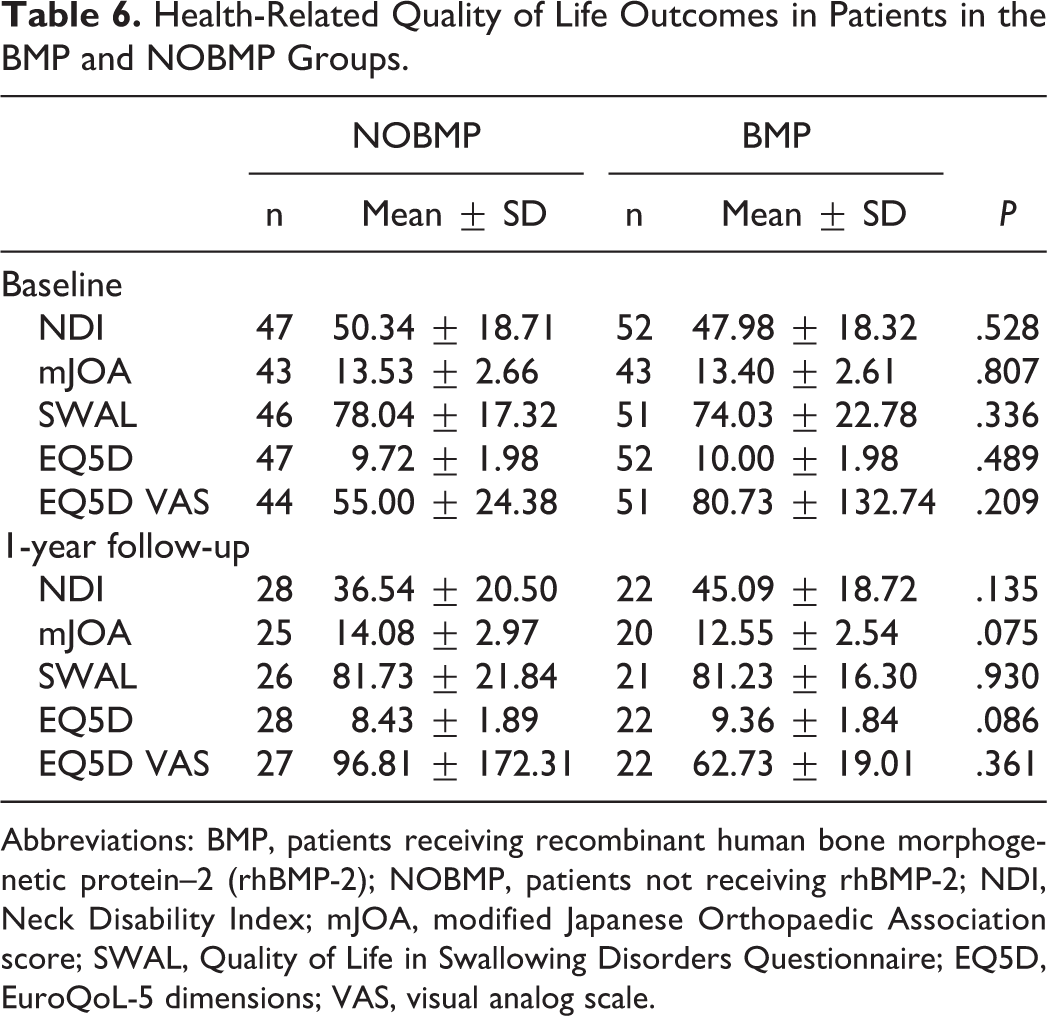
Abbreviations: BMP, patients receiving recombinant human bone morphogenetic protein–2 (rhBMP-2); NOBMP, patients not receiving rhBMP-2; NDI, Neck Disability Index; mJOA, modified Japanese Orthopaedic Association score; SWAL, Quality of Life in Swallowing Disorders Questionnaire; EQ5D, EuroQoL-5 dimensions; VAS, visual analog scale.
Discussion and Conclusions
Our data demonstrates that BMP can be used in the operative management of adult cervical deformity without an increase in early complications (Table 3). The use of BMP did not result in any increase in complications, including dysphagia, neurologic complications, and wound complications. These findings suggest that BMP may be safely used posteriorly in the setting of cervical deformity.
Most existing literature examining posterior BMP use in the cervical spine has focused on radiographic fusion as the outcome. 14,15,18,19,25 The majority of these studies report a higher radiographic fusion rate with BMP, but there may not be a substantial difference in clinically significant nonunion—defined as pseudarthrosis requiring revision—between these groups. 18,19,25 This question of clinical significance is important and is particularly relevant to the subject of BMP. The Yale Open Data Access (YODA) Project, for example, found that the use of BMP likely leads to an increased risk of complications. 7 Indeed, their work suggested that although the use of BMP results in marginally higher fusion rates, this may not be clinically significant in the face of a higher costs, complication rates and unchanged clinical outcomes. While the YODA project focused on BMP use in the lumbar spine, it is important that use of BMP in the cervical spine receive similar scrutiny that focuses on outcomes beyond radiographic healing.
To that end, there has been little work performed examining complication rates following BMP use in cervical spine surgery. 17,26 Xu et al 17 found that the use of BMP posteriorly in patients undergoing surgery for degenerative cervical conditions did not lead to an increase in complication rates and led to an increased rate of fusion based on computed tomography imaging and radiographs. Interestingly, these authors also noted an increased rate of neck pain in the BMP group. 17 More recently, Goode, et al 26 performed a registry study examining a large Claims and Encounters database. 26 They reported that patients receiving BMP were more likely to have a complication, undergo revision surgery and had a higher 30-day readmission rate. While Goode et al 26 considered both anterior and posterior BMP use in their analysis, their findings did not differ substantially based on approach.
Both these studies, however, were retrospective studies focused primarily on degenerative spine conditions. The cohort in Xu et al, 17 for example, was undergoing 5-level posterior cervical fusions. That cohort is significantly different from the patient population presented in our study. Patients with cervical deformity frequently need longer fusions (9 levels or more) that cross 1 or more spinal segments (occipotcervical and cervicothoracic junctions). Prior studies have shown that patients undergoing longer fusions are more likely to receive BMP. 26 To that end, it is crucial to define the rate of complications in this high-risk patient population.
The number of participants enrolled in this trial compares favorably to other investigations of BMP use in the cervical spine. 14,15,17 Additionally, we report data from a prospectively gathered database that allows for detailed documentation of complications and makes underreporting of complications less likely. To our knowledge, this is the first prospective study to report the effect of BMP in the cervical spine. This unique strength allows us to perform a detailed analysis of complications. We showed, for example, that the average dose of BMP (in cases where it was used) was 13.58 mg, or about 1.4 mg/level. While the dosing of BMP is not reported consistently in retrospective studies, 17 this dose of BMP is lower than that reported in previous trials. 14,15 This reduction in BMP dosing might explain the lack of complications seen in our patient cohort. Several studies, for example, suggest that the adverse effects related to BMP might be dose dependent. 9,27 While our analysis did reveal a significant but weak relationship between the dose of BMP and the rate of major complications and operative complications, this must be considered in the context of an overall lower dose of BMP used.
The lower dose of BMP used in this cohort makes it important to examine radiographic fusions and complications. However, we are limited by the relatively short follow-up period of our patient cohort and therefore cannot report on fusion rates. Fusion rates represent an important area of future investigation because patients in this cohort are undergoing longer fusions that cross the cervicothoracic junction and are therefore at higher risk for pseudarthrosis. We are actively collecting longer term follow-up data in this prospectively enrolled cohort so that we may be able to accurately report on fusion rates. While the current article establishes the safety of posterior BMP use, it will be important to establish its efficacy as well. There is debate, however, about the length of time required to diagnose pseudarthrosis and the most effective way to identify pseudarthrosis. 28 Additionally, there is some debate within the field about the significance of radiographic nonunions in the setting of unchanged clinical outcomes and rates of revision surgery. 7,25
Despite these limitations, we believe our study has significant value. We are able to show, through a variety of analyses, that BMP may be used in the setting of adult cervical deformity without an increase in short-term complications. This finding is of value to adult cervical deformity surgeons considering BMP use in patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was conducted with funding support provided to the International Spine Study Group Foundation (ISSGF) from DePuy Synthes Spine, K2M, NuVasive, Innovasis, Biomet, Orthofix, as well as individual donations.